You know when you learn about a ‘new’ dis-ease driver and then you actually have to stop yourself from diagnosing every patient with it? I’ve done this dance with Gilbert’s Syndrome for over a decade, so too maybe have some of you? And while there have been many, many occasions when I’ve been certain it’s Gilbert’s (clear robust & reproducible patterns of high bilirubin without other explanation) there are other times when I’ve been left wondering, and with questions. Like – what about a fluctuating pattern – sometimes ‘within range’ sometimes above or at least high-normal – with no other explanation? What about the patient whose symptom-story is a perfect fit – prone to nausea, early satiety, gut issues, food reactions and anxiety all worse for increased oestrogen…but the total serum bilirubin is 14 micromoles/L? I mean, 14, right? that’s well below the top of that range, but remarkably higher than the majority of women of the same age, eating the same diet. And you ask yourself…could it…be??
It could.
The latest UU30 offering on Gilbert’s Syndrome constitutes a complete overhaul of everything we’ve previously been told about how to recognise and diagnose this polymorphism & it’s going to answer a lot of those ‘could it be’ questions we’ve all had! Known also as familial non-haemolytic jaundice and episodic hyperbilirubinaemia under stress – is everyone with Gilbert’s prone to jaundice? Uh, no. Total bilirubin levels typically have to get to 45 micromoles/L to evoke this effect – many of our GS patients won’t ever get there, some will with increased illness or other stress and may yellow a tad (like a fading bruise), while other patients of mine routinely have a bilirubin at this level but won’t experience jaundice unless they impair their UGT further via doing what they know they shouldn’t: extreme exercise or excess alcohol. The latest deep dive into GS diagnostics
But as much as we don’t want to miss this diagnosis we don’t want to mis-diagnose patients with it either!
Can you spot the difference? Don’t forget total serum bilirubin levels are the net result of haem catabolism – so you need to account for rate of blood production, destruction and of course rule out any biliary dx before you can take a guess at Gilbert’s. Oh and watch out for expected high bilirubin values in the fasting fan(atic)s!
For those people living with Gilbert Syndrome at last the research world & the real one are uniting – with greater detailed documentation of how this very common polymorphism presents and the mark it may make in their health story. However, given only 1/5 with Gilbert’s syndrome actually know they have this condition, who are we missing? This latest instalment rewrites our diagnostic criteria and corrects our past misunderstandings based on the very latest science, while shedding further light on what it’s like to live in Gilbert St.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
“After our group session I suggested the low fat trial but she was ‘no, no, no….I can’t take anything more out of my diet’. It was at the beginning of lockdown & she had other stressors as well. So I asked her to be mindful of her fat intake & if one meal was higher in fat then go low fat for the rest of the day. I saw her last week & she did this & guess what her diarrhoea has dramatically improved. She is not experiencing watery diarrhoea nor the sense of urgency nor leakage. Mostly 4, sometimes 5 on Bristol Stool. She’s now happy to trial low fat (<40g/d)”
This is the story of a 50-something female who has battled IBS-D for over 30 years. Along the way she has diligently sought the help of so many health professionals and tried numerous ‘tried and true’ IBS approaches, like FODMAPS minimisation, gluten minimisation, dairy minimisation & joy minimisation with hardly any minimisation of her symptoms!Why? Because her loose stools and urgency were BAD. A very particular form of bile acid dysregulation that is present in almost half of IBS-D patients and responds best to low fat intake, together with a few other tricks.
And with the corresponding slowed transit time, we now can more clearly see if there are additional actual food reactions at play – without all the background BAD confounding and now that her gut has time at last to actually correctly absorb things that she couldn’t before due to inadequate time in contact with digestive enzymes and absorptive surfaces.
Ahhhhh we love a great ending – especially one that reminds us the most powerful prescription is getting to the root cause such that we can empower patients 💪🧐 This patient and her practitioner inspired the recent Update in Under 30 on how we can all learn to recognise….
This is not a trick question. Up to 50% of all patients diagnosed with IBS-D actually have bile acid diarrhoea (BAD) underpinning their digestive complaints as well as some patients with unresolving diarrhoea post-cholecystectomy and gastro. Knowing which ones do and how to manage this, which requires distinctly different approaches from our general management of IBS, is the key. As always, good lessons come from those we learn in the clinic and this story starts with a patient and how we came to recognise the BAD in her belly. Get this as a single download here.
No, this is not a trick question & it’s certainly not a silly one. IBS, as many of us know, has a very loose diagnostic criteria: visceral hypersensitivity coupled with altered motility in the absence of organic disease. Hence it tends to ‘loosely’ fit a vast number of patients struggling with GIT issues. The differential diagnostic algorithm all health professionals are encouraged to use for patients presenting with GIT issues leads us to this IBS label, just as soon as we’ve excluded the red flags. But this ‘early opt out’ according to many experts, including Schiller et al in the American Journal of Gastroenterology, tends to propagate the illusion we’ve reached our diagnostic destination: practitioners stop thinking about the ‘why’ & stop looking for the real drivers & causes, which is the key to shifting the refractory patient into remission.
For those presenting with chronic diarrhoea, Bile Acid Diarrhoea (BAD) is in the diagnostic algorithm & there is strong evidence it’s at play in almost half of these patients! It’s just that BAD, is the next station along the line after IBS-D, which means most clinicians have sadly disembarked already 🙁
Bile acids, as key biological agents, in both the behaviour & health of the gut & metabolic dx, are getting a lot of attention right now. While Bile acid malabsorption (BAM) in disorders of the small intestine such as Crohn’s & undiagnosed or refractory Coeliac dx, as well as other miscellaneous GIT disorders that clearly disrupt the bile acid balancing act of the gut-liver axis, have been known for a long time, there’s a new kid on the gut block, previously only known as the idiot, I mean, idiopathic BAD. But us idiots have finally worked it out! This is not about malabsorption but about excess production of bile acids and this pathophysiology is drastically over-represented in IBS-D patients.
And knowing if your IBS-D patient has a ‘BAD-thing’ going on, every researcher wants you to know, is game-changing. Explaining the strong heritability of this particular IBS subtype and the reason so many patients are refractory to standard IBS approaches.
We need to use distinctly different dietary strategies when IBS is BAD. Once again patients are our greatest teachers & I’ve relished the excuse one practitioner and her patient gave me to deep dive into the enormous body of BAD research, that is ‘so hot right now’! The way I look at, ask questions about and assess patients with chronic diarrhoea, especially IBS-D, is forever changed 💪🙏
When is I.B.S. B.A.D?
This is not a trick question. Up to 50% of all patients diagnosed with IBS-D actually have bile acid diarrhoea (BAD) underpinning their digestive complaints as well as some patients with unresolving diarrhoea post-cholecystectomy and gastro. Knowing which ones do and how to manage this, which requires distinctly different approaches from our general management of IBS, is the key. As always, good lessons come from those we learn in the clinic and this story starts with a patient and how we came to recognise the BAD in her belly.
I’m 100% confident that, as a professional group, among our highest values about healthy, preferable, food choices, would be characteristics like: ‘as close to nature as possible’, ‘unrefined’, ‘unprocessed’, ‘unadulterated’. Tell me I’m wrong.
So, when I keep hearing about NEW! “Never seen before” (read: never in nature) modified (read: more processed, adulterated) nutritional supplements: water soluble vitamin D, fat soluble C, bioflavonoids with unprecedented (read unnatural) bioavailability
I’m left wondering what these companies are missing about their customer group (because we are clear about our valuing of nature & what’s natural & have a desire to minimise exposures to things that are not, right?
or what are we missing here, in the clear conflict of our core values these constitute?
I think if we find ourselves forsaking this core value & prescribing highly modified, unnatural supps, it’s the result of both hype & fear. The hype is self-explanatory and I’ve written recently on how modifications exponentially increase profit margins for companies, all the while possibly reducing ours because patients are spending more on product and therefore there is less left over for the practitioner fees 🙁 [The ones spending hours with them face to face, not to mention years & thousands on our training] The fear is perhaps less apparent, more insidious. The fear is that we’re not using the best, being the most effective, and deeper still, inevitably that we will fail to action our patients return to health. This is a big one. I think it’s pervasive, if not omnipresent, and works as a motivator for many positive actions by practitioners – like engaging in further education, reading that latest journal edition on your lonesome laptop when you could be streaming some series on a shared sofa. But this same fear can also undermine us, overwhelm us and shake our tree of trust, that we believe to be so firmly rooted within us, of the healing power of nature.
So while my position sometimes makes me feel very ‘old school’, I’m not suggesting we return to nutritional prescriptions composed exclusively of bee pollen & brewer’s yeast and I absolutely recognise and respond to an individual who has very specific barriers to benefiting from nutrients in their natural normal forms. But let’s be clear, they are a minority.
Some of you will know naturopath Dawn Whitten & know that she is one of my mentors. I’ve had the benefit of speaking with her over the years about herbal prescriptions but also about the principles & philosophy behind our practice & in one of many conversations she told me that a key objective she has with her patients is to rebuild their trust in their body, their own biological resilience (I love this concept and that’s a talk for another time!) and ultimately in nature. Well jeepers Dawn – how did you get to be so wise so young? But isn’t that central to vis medicatrix naturae? Maybe that Naturopathic Nanna’s club isn’t so fuddy-duddy after all. Want to join us?
Speaking of using nutrients in their most natural state for the best health outcomes – the best B3 is probably not what you think!!…. The Balance of B3
Most of us have been taught to ‘balance the Bs’ when supplementing, which discourages the use of single B vitamins in case this interferes with the regulation and roles of others. In reality, outside of a couple of dynamic duos like B12 and folate, there is little concrete information & evidence of this. In the case specifically of B3, however, we now know, the risk of an excess of the most common B3 forms found in supplements and fortified foods, results not only in disruption of other nutrients but imbalanced B3 biochemistry itself. Given B3, in its coenzyme form NAD+, is regarded as highly valued currency in the prevention of many diseases, as well as the key to our optimal health and longevity, it’s critical to understand the different forms and functions of the various B3 sources.
I haven’t personally seen every medical condition known to occur, nor every micronutrient deficiency & toxicity picture in the flesh but that doesn’t mean I doubt their very existence. Sadly, it would seem some practitioners due to a) not knowing ‘where’ to look in terms of best assessment medium and/or b) not knowing ‘what’ they’re looking at, when faced with an actual Copper deficiency, have declared this uncommon, but certainly not unknown, nutritional issue to be a figment of others’ imagination!
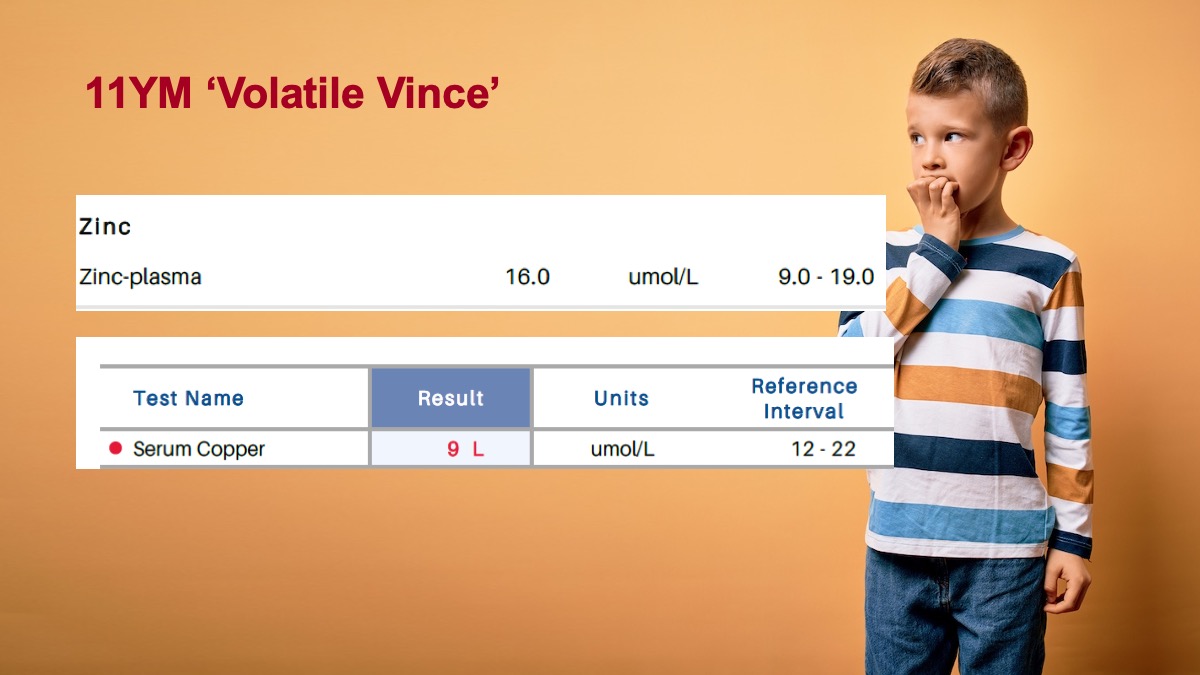
I know I’ve been fortunate to see more labs than most would want to in an entire lifetime , a collection of my own, my student’s & my mentee’s patients, so let me share just 3 sets of results from 3 different individuals: an 11Y boy, a male teenage athlete and a female in her early 20s with an eating disorder, all with Copper deficiency.
Don’t worry, I have more – just ask. What’s so dangerous about people spreading myths and misinformation in relation to copper in kids and teenagers specifically, is it shows complete disregard or ignorance of an understanding of how Copper is critical for development during these life-stages and how regardless of which developed country you live in Copper is expected to dominant over Zinc in blood, especially pre-puberty.
AM I SHOUTING???!!!
I’m sorry it’s just that my blood tends to hit boiling when exposed to the misinformed, misinforming others… and that can make one call out in pain 🤯
You see, I literally heard a practitioner in an “educational” webinar purport that
‘Copper Toxicity is so prevalent in kids in her clinic’ and I was like,
OH. EM. GEEE.
Because if you start with that misunderstanding, and are unclear about what constitutes an accurate Copper assessment and how to recognise the pattern that follows low serum levels (each of these patients above had abnormalities in their FBE consistent with Copper deficiency) you are not only going to miss the thing you need to make a priority to fix, you’re going to make it worse! Take ‘Volatile Vince’ the gorgeous sensitive 11Y boy I saw, whose increasing mood volatility had been misattributed to pyrroles and given large doses of Zinc! So, Copper Crimes are a thing. Guilty until proven innocent but in fact, never found innocent by some practitioners it would seem. The ramifications of unchecked Copper deficiency include negative effects on mood and cognition, immunity, and the balance of other nutrients and kids are going to feel this impact the most! What are the causes? Inadequate intake being uncommon outside of eating disorders, and excessive Zinc rarely the cause, we’re likely looking at a marker of malabsorption or a genetic issue. Don’t buy into the confirmatory bias many use when they choose which research to read (risk of excess) and which to ignore (Copper as an essential mineral, critical to kids) and let’s not discredit something as not being a thing because we haven’t seen it ourselves, yet, hey, anyway, at least, now we all have, right?!😵🥴😆
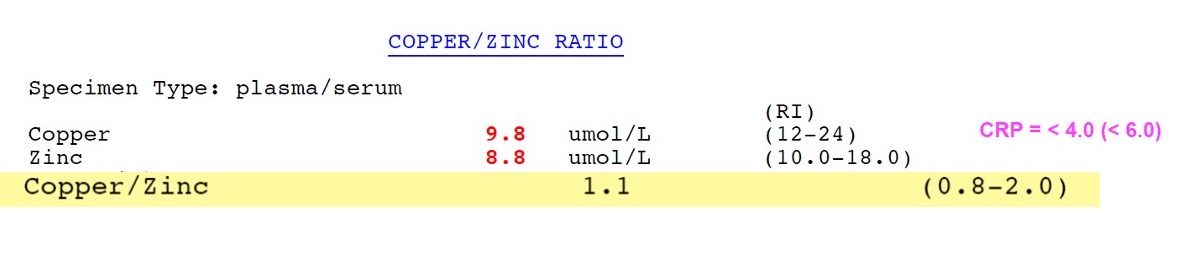
Copper, as a kingpin in angiogenesis, brain & bone building & iron regulation is a critical mineral during paediatric development. So much so, the kind of blood levels we see in a primary schooler might cause alarm if we saw them in an adult. So too their Zn:Cu. But higher blood Copper and more Copper than Zinc are not just healthy but perhaps necessary during certain paediatric periods. This recording redefines normal, low and high with a great clinical desktop tool to help you better interpret these labs, as well as reviewing the top causes and consequences of both types of Copper imbalance in kids.
Name a B vitamin. Hey, Bingo! It’s on the list! What list? The complete one from all the review papers & references to possible links between individual nutrient deficiencies & Angular Cheilitis – inflammation & cracking at the corners of the mouth. So does that mean more Bs are the answer for people presenting with this painful, recurring issue?…Ahhhhhh No. Yes, you heard me correctly, these deficiencies rarely cause the breakdown of the integrity of this very specific area of skin in the patients we see. So now we have a double ouch, right?
We might send patients away with a B complex and some lip balm and over a week the cheilitis resolves – which one was the most therapeutic? …I hate to tell you 👀
What is the underpinning cause(s) & the important message we are missing with this presentation? Well, it could be one or more of a long LONG list of differentials, ranging from anatomical, habitual, immune related to iatrogenic. And while many nutrient deficiency pictures can include this feature and therefore make the ‘possible’ list, only one makes the ‘probable’ list. And that’s iron but only in severe deficiency, aka anaemia and only affecting 1 in 5.
Me???
…Telling anyone to push the nutritional issues further down the list of differentials for any condition? Well, that’s unexpected
…possibly unprecedented
And no, antifungals aren’t the answer either. Yep, that might be worth a listen….👂
Just an annoying, embarrassing, cosmetic condition or could it be the clue that helps you ‘crack the case’? There is a surprisingly long list of differentials for this condition but most of us only know a few, reflexively reaching for either B vitamins or anti-fungal creams. Does either make sense? Does either address the cause(s) which we now recognise to be a unique series of risk factors in each individual? Or are we at risk of shooting the messenger and missing the message of Cracking Corners altogether?
You can purchase Cracking in the Corners – Angular Cheilitishere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
[Ahem] Ok let me explain…Several catch-cries from Australian ads have earnt themselves a lifelong place in my head and heart, taking up space where something more important should be, no doubt, but does anyone remember this SPC canned fruit (REALLY showing my age now!!) one, where the little boy chases the grape around the bowl and declares it a, ‘Slippery Little Sucker!’? Ok so this little boy is every one of us when we’re trying to ‘capture someone’s cortisol’ and just like the boy we will eventually achieve a ‘result’ – get a ‘number’ but what in fact does this mean in relation to your patient’s HPA axis, stress perception, responsivity, recovery etc etc?
Recently I was presented with 2 cortisol results for a patient taken within the same 24hrs – her blood am result was above range, while her 24hr urine flagged under-functioning of her HPA axis generally. Both were accurate.
Had I have only have seen one, I would have formed the wrong opinion and only gleaned part of her overall HPA story. Every different type of cortisol capture – from different mediums: blood, saliva & urine – to different collection conditions: time of day, fasting V fed, specific stressor exposure etc answers a different question about our patient’s HPA axis. So to use any form of cortisol assessment well we need to start with 2 understandings: 1) it is a slippery little sucker indeed and no one test can answer all our questions – or as Miller & colleagues more eloquently put it, “Remember, all models are wrong; the practical question is, how wrong do they have to be to not to be useful” and 2) be clear about the most important question you have about your patient you are trying to answer and that will make your choice of test (& timing & & &) patent. But do you know enough about cortisol regulation to be clear about the ‘sweet spot’ of each test?
The Cortisol Awakening Response has understandably attracted the bulk of the research focus over the last decade and accordingly has risen in popularity in practice & while it remains a very valuable way to answer certain questions about patients, our understanding of its limitations continue to grow. For example there is a disconnect between CAR & diurnal cortisol secretion – so in essence your CAR can look woke but your ‘Slope’ may be broke! If you’re a fan of this method, make sure you catch up on the CAR-Expert Consensus Guidelines by Stalder et aland if you’d like to get clear about which test and when, when it comes to all the key options for Cortisol Capture..
then let’s dive in together with my latest Update in Under 30 instalment
I have! And just recently a stark contrast between the results from 2 different methods of cortisol capture in the same patient illustrated just how likely this is. How do we ‘capture’ something so ‘dynamic’ and interpret anything of substance from a ‘static’ assessment technique? But rather than throw up our hands and throw out the whole attempt to measure cortisol, we can improve the rigor, reliability and real-world meaningfulness of our patients’ results by refining our timing of tests, choosing the medium wisely & manipulating test conditions to answer specific questions about their HPA function. Great desktop reference included!
You can purchase Cortisol – Have You Been Caught Out?here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
I’m experiencing some serious POTTS exhaustion – how about you? No, not POTS, POTTS: Preposterous Over The Top Selling of supplements, which seems to be at an all time high even amongst our practitioner brands. I saw a product name recently that included the word, ‘supreme’!*^# Is the choice of nutritional supplements now on par with selecting our pizza toppings?
When I previously delivered university lectures on population nutrition & the role of the food industry – we acknowledged that all the processing, packaging, and promoting the food industry invests in, creates a market and a source of competition that essentially doesn’t exist for their primary whole-food ingredients.
Take apples. How can we increase the profit margin on a humble apple? Aside from organic V conventional farming, the price that any of us would pay is pretty narrow and fixed. But send that apple to the factory to make juice (and chuck in some added vitamins to boot so you can feature this on the label!!), puree and package it in the most non-biodegradable way for kiddies, dice and stew the stuff and put it in little plastic tubs for the slightly older or throw in a long list of nasties with ‘essence of apple’ to make sauce for idk and suddenly you have the capacity for mark-up, an exponentially expanded profit margin & ‘something to say and something to sell’. In supplement companies, it’s not as far from this as you might imagine. Because nutrition (**WHAT A SURPRISE**) is a lot like primary whole-food ingredients – how does vitamin C compete with vitamin C? Hey, make it liposomal!! And the nanoparticles that we’re fearful of in our sunscreens and cosmetics..let’s use the same technology for our ingestives!! YES!!! Ummm any one recall, our fears re folic acid? Just asking…
I propose that ‘practitioner only supplements’ come under the same plain packaging restrictions placed on tobacco in Australia [I am joking but only just]. Remove the bright shiny distracting graphics and hyperbolic descriptors and only state the full ingredients and excipients list plus source where relevant. Let’s bring it back to simple(?) science, basic quality ingredients and affordable effective products for our patients. Then let’s see if we can spot the difference 🧐
Rachel loves nothing better than breaking through marketing babble and spin to get to the truth about supplements – their real strengths, niches, weaknesses, contraindications, therapeutic doses and best forms & therefore there is a dedicated section of her website with resources and recordings that do just this,here. These include reviews onB3, B12, Folate, Selenium, Zinc & Iron (of course!),Calcium D Glucurate,Co Q10, Quercetin, high doseVitamin DandFish oilsfor Mental health. These are a mix of Update in Under 30 recordings and longer presentations and her library is ever expanding! So, if you have a supplement you think needs some serious sleuthing on – send us an email…we’re always sniffing around for more!!
“How much can you misbehave & get away with it?” I listened with fresh ears, as a practitioner asked my son this question recently. I use similar ones with my own patients but hearing it from someone else, I could sit back and appreciate its true purpose and how well it achieves this. Most of us adjust our behaviours, when we can, to ‘manage’ things that cause us problems.
Sure I can eat food I haven’t made myself
………..but once a week is my max. or ‘X’ flares
My energy is pretty good …… but 1 night of poor sleep & I’m back on ’empty’
No impaired alcohol tolerance
………I just never have more than 1
My [insert: gut, skin, energy, immunity, mood] is not a problem
………as long as I don’t miss a dose (of supplement/medication etc)
And sometimes this ‘adjustment’ (or avoidance) is unconscious. Hence the beauty of the question: How much can you get away with, coupled with our understanding of how much ‘room to move’ there should be in a patient who is truly well. So the teenage to early 20s patient sitting in front of us, theoretically, should be in their prime of wide mischief margins, and we are alerted to individuals in this age group who are having to live like an older person, needing to exhibit vigilance around early bedtimes and allowing themselves almost no indiscretions. In contrast, as we age, we understand too, the margin for mischief narrows. Our over-50s selves are unlikely to get away with half as much as did in years gone by but we shouldn’t require the stricter self-care hypervigilance of our senior selves.
And for the patient who answers ‘no’ to everything on your GIT or stress/mood screening questions, for clarification, follow them up with, “and how much can you get away with and still have no issues?”
You may very quickly get a different understanding of what lies beneath and how much ‘management’ is required to maintain ‘balance’ or ‘no symptoms’ or ‘health’ 🧐
The primary objective of MasterCourse I is to realise the true value we can extract from the most commonly performed labs (ELFTs, FBE, WCC, Lipids & Glucose) which constitute the largest biochemical dataset we have on almost every patient. By learning how to comprehensively interpret these labs in an integrated medical framework, using the very latest science, we can extract the gold often buried in this goldmine. Accordingly, we prove ourselves to be the greatest asset to our patients, to other health professionals we are sharing care of patients with and we cut the cost of additional expensive testing, that is less well understood and validated.
MasterCourse I will help you access that gold and has been intentionally designed to match each lesson with real learning– with the time spent in theory and in application. Delivered across 24+ hrs of streaming video sessions with bonus pre-sessions, audios, resources and tools – this MasterCourse is likely to be a genuine game-changer for the way you practise and the potency of your patient prescriptions.
Is it just me or do you view everything with a trained eye? My son always laughed when I wrote him a shopping list: I would list items under each shop and I always wrote down our local supermarket the Independent Grocers Association, like this: IgA…you all see what I was doing, right?!! It’s actually known to everyone else as IGA…well truth be told, I didn’t until he pointed it out 😂 Then there’s this relic I regularly pass, as I walk through bushy parkland near my home, ‘Hmmmmmm, B12 hey?’, I’d muse. I’d be embarrassed to tell you exactly how long it was before I realised OMG it’s not a shrine to the vitamin but an old road sign telling you…Byron 12kms!!!
I preferred my take on it to be honest, because invariably once past this, the remainder of my walk was full of scintillating B12 banter. Just internally, people, no one panic, I don’t walk the streets of this town spouting out crazy random nutritional tidbits…although, let’s face it, I would be in good company in, the Byron Bay region!
I have a deep respect for B12 – weird but true. As a result of my clinical experiences helping patients who had a previously ‘unseen need’ for this nutrient and the significant improvements that come with its replenishment. Plus the deep dive I did into the science of the different forms and their actions last year. In particular, I now have 2 families where the TCNII SNP is evident in mum and all her children. No gene testing necessary, the pattern is self-evident once you know what to look for and the clear ‘call to action’ – more B12 please! And just this month, a fresh aspect has come to my attention in regard some brand spanking new research on B12 and IBD and the microbial (im)balance of this vitamin as a pivot point for the pathophysiology. Wowza! Early days, but I think we’re headed next level on this nutrient again! And I can’t say, I’m surprised. For while I don’t think the CHOICE of the supplemental form for B12 is complex at all (hence why we need to separate the B12 from the B*S#!) I recognise it is a complex character far beyond what regular dietetics has reduced it to.
B12 is a routinely under-rated and recognised micronutrient, which is in fact in high demand by many of our patients. As nutritional research pushes back against defining adequacy as simply the prevention of the deficiency-associated disease (macrocyctic anaemia, irreversible neurological damage) we enter a new landscape of more individualised approaches where we’re better able to recognise and treat those at risk of falling below ‘optimal’. But how do we accurately identify this and then choose the ‘best’ B12 (methyl- cyano- adenosyl- hyroxo-) supplement? Does it need to be this complex? Time to sort the B12 from the B*S#!! This recording comes with a bunch of great resources including a clever clinical tool.
Something’s just come up today again and I think we need to talk about it. A positive result on a stool PCR microbiome test for H. pylori, understandably, might be heard as a clear call to action to go in guns blazing with an eradication approach. But is it? Trust me, I’ve had more than my fair share of battles with this bug & can understand being keen to have it be gone BUT first things first, let’s be clear about what the result speaks to.
Does it say, “Here! Look over here! Here’s the source of your patient’s GIT distress,” or even, “Here’s a pathogen that has taken up residence in their GIT and is a risk for future dx!”
No, not necessarily. It speaks to its presence.
And that may be only fleetingly, as it passes through. I’ve seen it before and so have many other experienced practitioners: a positive stool PCR that is at odds with the results of gold standard H.pylori testing, the UBT, faecal antigens or blood serology, all freely available through the GP. And the reality is, if you have a negative UBT, there’s no urease production, the trademark trouble-making of this bug. If you have negative blood serology, your immune system has never ‘met’ this bug or, in the minority of cases, you’ve tested in that brief early exposure window prior to antibody production (2wks) so you should retest within the month, to confirm or refute. And if you don’t have any faecal antigen…it ain’t in da’ house…so to speak 😅 If there’s something new here, then have a quick read of Medscape’s great work-up summary. So, clearly we need to confirm before we open fire.
We (me included) have been so single-minded about increasing the ‘sensitivity’ with our testing methods, we may have left ‘specificity’, in broader sense, behind & that creates a new problem.
This leads us and the patient down the garden path of false attribution and time and money wasted ‘treating’ a ghost gut issue. And no one wants to be put on a pylori protocol when they really didn’t need to. Trust me 🙄 But if someone does come back confirmed, well then…
For a bacteria identified just a few decades ago as being a cause of chronic gastritis, atrophic gastritis and gastric carcinoma, the escalation of number of antibiotics used to eradicate it (4 at last count + PPI) has been nothing short of breath-taking. A management approach more consistent with both integrative medicine and with an improved understanding of the delicate microbiome focuses on changing the gastric environment to ‘remove the welcome mat’. What do we know about how to do this successfully? It turns out…quite a lot.
If I could be granted 1 wish regarding all health professionals, it would be that we were all competent in reading Iron Studies. Think that’s overstating the issue? Or not a bodacious enough way to ‘spend’ my wish? I don’t. Especially when you consider the impact of GPs in this space.
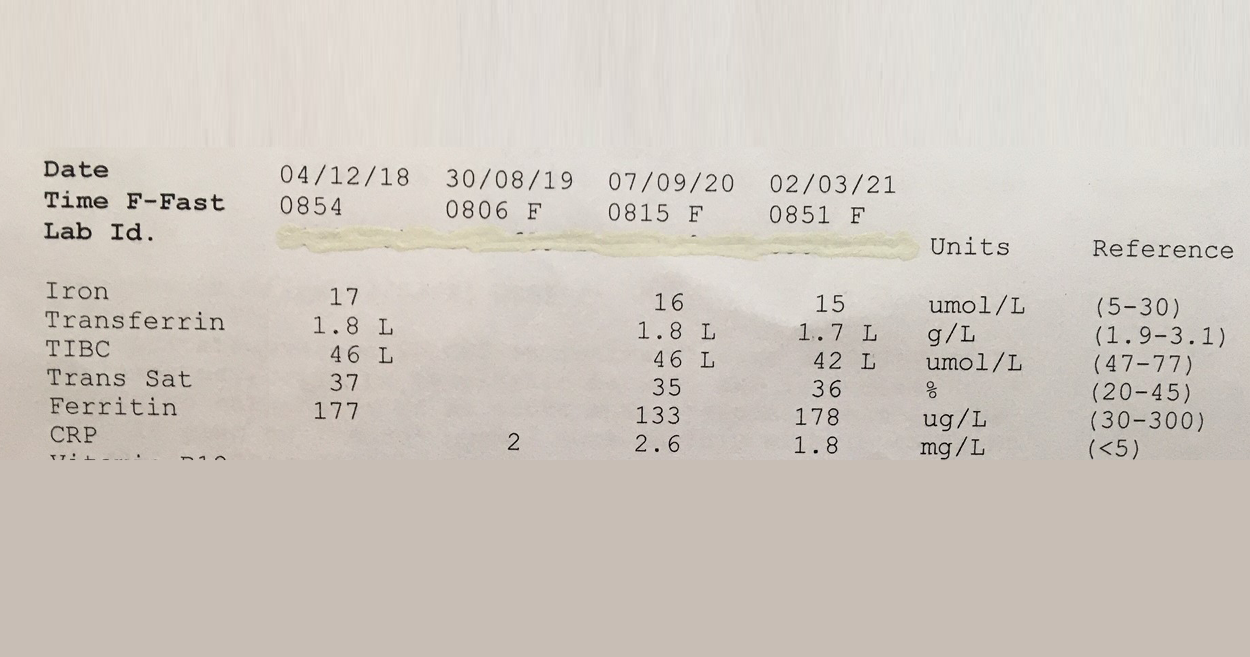
This 57Y male was asked to make a follow up appointment with his doctor, to discuss his ‘abnormal’ results which he was informed constitute Iron deficiency. Consequently he was was advised to start an iron supplement! #@!*
Your thoughts? Revoke this doctors medical licence? Insist on some very du jour ‘re-training’ at the very least? I mean, if you think this Iron pattern flags a deficiency or shortfall, then you’re as good as reading a map upside down and back to front…and written in a foreign language!! The ‘Ls’ in his latest labs flag he has suppressed transferrin, indicative of negative feedback inhibition of GIT uptake of this mineral, secondary to healthy stores or inflammation. And it’s not just that more iron is not indicated but that more iron in fact presents a patient like this with increased and unnecessary risk: to their microbiome, intestinal wall health, even according to the larger longer studies a potential correlation with colorectal cancer risk, if taken long term. Let alone the whole cardiovascular conundrum. Better still this same patient was told a few years back that he might have iron overload! Again the ‘map’ could only have been being read, upside down, back to front to reach such a conclusion!
So the one patient in just a few years by 2 different doctors has been diagnosed incorrectly with 2 different iron issues. Yep.
And sadly I have sooooo many more cases of missed and mis-diagnoses with regard to this mineral. The latest RCPA Position Statement on the Use of Iron Studies, underscores that assessment of iron status and GPs competence in knowing when to do this and how to interpret, is an important part of core general practice. Given it “is the commonest nutritional deficiency state in Australia and is significantly under-diagnosed” This succinct document offers a quick crash course in Iron nutrition for doctors and it hits all the right marks with advice about not ordering ferritin as a stand-alone because “the interactive nature of the three components allows for more accurate interpretation”and this simple but sage advice:
“Transferrin, iron transport protein, tends to increase in ID… A better strategy (than being tricked by Serum Fe) is to report transferrin saturation. A low transferrin saturation in the setting of an equivocal ferritin level is suggestive of iron deficiency. An elevated transferrin saturation is the first manifestation of iron overload.“
I mean seriously, do doctors read these RAGCP resources & recommendations, or is it just me? 🤓😂
Need a rip-roaring review on how to really read iron studies? Or know another health professional who does?!! Consider this Easter Educational Gift Instead of Eggs!! So You Think You Know How To Read Iron Studies?
Overt Iron Deficiency Anaemia or Haemochromatosis aside…do you understand the critical insights markers like transferrin and its saturation reveal about your patients iron status? Most practitioners don’t and as a result give iron when they shouldn’t and fail to sometimes when they should. This audio complete with an amazing cheat sheet for interpreting your patients Iron Study results will sharpen your skills around iron assessment, enabling you to recognise the real story of your patients’ relationship with iron.
Just like Kevin, ‘Niacin’ is profoundly misunderstood and consequently runs the risk of doing us harm. Unlike ‘Kevin’, we can’t watch the movie to see how this (our arguably excessive use of the wrong forms of B3 in supplements and fortified foods) is all going to play out, so that we can be suitably alarmed and start making some different choices. The risks that follow from our B3 ignorance are twofold:
One comes essentially from our gross under-estimation of this B vitamin – we’re stuck in the Pellagra Paradigm, believing that prevention of the 4 D’s is confirmation of adequacy.
The second, is our lack of discernment when it comes to the different forms or precursors of B3 & our unfamiliarity with their very specific physiological roles – good and bad.
In this regard we’re all likely to say, ‘Well back up there 1 second, we do know that Niacin (aka nicotinic acid) is different from the other forms!’ Producing flushing, yes. Used as a lipid lowering agent in pharmacological doses, yes. But can you tell me, which serious concerns and biochemical disruption is shared between both gram doses of niacin and everyday ‘routine’ mg doses of niacinamide? Yep, that one, the so-called ‘safe’ one. Better still, can we all list the various B3 forms in order from most to least potent, in regard to their capacity for NAD+ promotion in the human body?
Because this is now the definition of B3 ‘adequacy’ or ‘optimisation’ according to modern scientific understanding & it is a long long way from the absence of Diarrhoea, Dermatitis, Dementia and Death!
In fact, the boosting and optimisation of NAD+ pools in the human body is key to life – a long and healthy one according to the current research consensus – and its depletion is akin to ‘death’, or a faster one, anyway. From increased metabolic disorders, mitochondrial dysfunction, impaired gene stability (cancer, infertility etc) and higher rates of neurodegenerative disorders, just to start, these take up the lion’s share of our chronic health burden and battle that currently dominates the dis-ease landscape. And more niacinamide might just make that worse.
I didn’t mean to to alarm you. I am alarmed. Want to deep dive into this yourself? Start with this older but still brilliant review article by Bogan & Brenner. Want me to hold your hand while we jump off the high platform diving board together into this vastly different and powerful new understanding of B3? Let’s do it!
Most of us have been taught to ‘balance the Bs’ when supplementing, which discourages the use of single B vitamins in case this interferes with the regulation and roles of others. In reality, outside of a couple of dynamic duos like B12 and folate, there is little concrete information & evidence of this. In the case specifically of B3, however, we now know, the risk of an excess of the most common B3 forms found in supplements and fortified foods, results not only in disruption of other nutrients but imbalanced B3 biochemistry itself. Given B3, in its coenzyme form NAD+, is regarded as highly valued currency in the prevention of many diseases, as well as the key to our optimal health and longevity, it’s critical to understand the different forms and functions of the various B3 sources.
There’s enormous potency in nutritional medicine for mental health but it ain’t in the form of a ‘dash of precursor here and a sprinkle of co-factor there’, like some may have you believe. Many nutritional prescriptions can look good on paper but that’s the extent of it, take the suggested use of glutamine for GABA production, for example. Sure it can be said to be a precursor (so is glucose!) – so will higher intake of this equate to higher production of this neurotransmitter? Ah, no. The reasons relate to distribution and hierarchy of use for this amino acid, as well as determinants of glutamatergic neuron activity.
Why would we limit our prescriptions to precursors, anyway, when we have 2 amino acids at our disposal, whose oral supplementation is known to translate to higher CNS levels and their actions and efficacy as major inhibitors of neuronal firing (akin to GABA), involves no modification nor maybes?!
Hello, Taurine & Glycine, where have you been all this time?
While, many of us may have been using taurine in combination formulas for mood, chances are you’re not entirely clear why sometimes those work and sometimes they don’t. The answer may be in the regulation of CNS taurine transfer & balance- sometimes the people who need it most, have the least capacity for its uptake across the BBB. This is well-established in neurobiology, but news to many nutritional and integrative health professionals, who have been using it in patients where Glycine, in fact, makes more sense. So while taurine has myriad impressive strings to its bow in relation to mood-modulation and powerful protection of brain structure & function, Glycine, has an extensive network of receptors throughout the brain and spinal chord, enabling it to exert inhibitory effects, second only to GABA itself. And, most importantly, BBB transfer of this amino is not subject to the same impediments that we see with taurine. These are two of my most frequent and favourite mood-modulators, affordable and accessible when used as single ingredients, for patients, with anxiety, addiction & sleep disorders etc but understanding how they work (and when they won’t) is essential in choosing which one to use, when.
For example, do you know the Tmax for either of these oral supplements? How long it takes, to create a spike in patients’ plasma, better still their CSF, and therefore speed of onset of action? What about their elimination half-lives to guide your understanding their duration of action and therefore the timing of follow-up doses?
When we’re trying to realise the full potency of our medicines – these are important details to know that convert our ‘prescription potential’ into something powerful. Just like die-hard herbalists will tell you, its an art and a science and this is true in nutritional medicine as well. Don’t skimp on the science!🤓
Both taurine & glycine have a claim-to-fame as amino acids that effectively calm an over-revving brain, via their net inhibitory actions within the CNS. They achieve this via different means and while in some circumstances, one, either or both will is the result of differences in the regulation of their BBB transfer, pharmacokinetics, as well as add-on benefits or detractors, unique to each. Learn how to use both of these powerful and affordable mood-modulators, to their fullest, and be more able to know ‘which one when’, by listening to this latest narrative review.
The latest Update in Under 30 has landed!!!
You can purchase Take A Fresh Look: Taurine & Glycine in the CNS here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
That’s not a word you hear often spoken by people practising nutritional medicine. Which is odd. I mean outside of the whole, ‘I’m not good with sulphites so I just have to add these magic drops into my glass of red so I can knock back my share,” often overheard at our conferences… it’s like this essential macromineral, pivotal to human health for things like barrier function, antioxidant defence and our basic ability to create the white cells for immune defence (for that matter), detoxification, musculoskeletal tissue integrity etc has just not received its due attention from us. Not entirely surprising given 1) there’s no RDI and 2) there’s no lab test to assess an individual’s status and how about 3) because we were never taught about it!
But the biggest ‘call to action’ here is that, in spite of items 1, 2 & 3, we’re ‘prescribing’ Sulphur Strategies all the time!
Take one of my favourite examples;GAGs. Glycosaminoglycans like Glucosamine sulphate (not the crappy, found to be not as effective, other forms that we now see more commonly) hit the headlines back in the noughties as an effective arthritis remedy. This is one of the 100s of our body’s ‘end products’ of its endogenous Sulphur Stream. We naturally make this in adequate amounts to ensure the integrity of our joints (and many other tissues of course!) when we have enough Sulphur in the ‘top pool’ (organic Sulphur) to trickle down to the 2nd pool (Inorganic Sulphur), therefore creating a constant essential supply of something known as ‘the universal Sulphur donor’ – ‘PAPs’, to its friends 😉 Like a waterfall, it helps to have a good flow from the top to increase the likelihood we’ll have anything to ‘show’ at the bottom.
So when we give a patient Glucosamine Sulphate it may well help. Or not. But did we ‘treat the cause’ of their Sulphur problem? Should we have treated higher up, increasing the size of either the organic or inorganic pool to have improved and widened the benefits for their health? Or, as is equally common, actually identified why someone might need more Sulphur than most – due to increased demand and losses?
Herein lies my reason for liking this particular Sulphur story somuch. The common medication that places the highest ‘demand’ on Sulphur (due to its need for detoxification) is paracetamol. There’s no debate regarding this – just absolute scientific consensus. NSAIDs and steroids also negatively affect the Sulphur status of individuals, as does Vitamin D deficiency and chronic mild metabolic acidosis. Now how commonly are these phenomena co-occurring in our patients afflicted with arthritis? And traditionally of course, what was the remedy for arthritis? Sulphur springs.
Unseen Sulphur – Time To Take A Look If you don’t have a clear picture of the gross daily requirements, determinants of altered individual needs, sources, regulation & associated deficiency picture of Sulphur, you’re not alone. Turns out this essential macromineral remains ‘unseen’ by most, even though you’re probably writing prescriptions every day that have Sulphur as their key component. From the simple: Taurine, N-acetyl cysteine, Protein powders, to the sublime: Brassica extracts & concentrates, N-acetyl Glucosamine, Alpha Lipoic acid etc. In order to use these Sulphur strategies successfully and safely, however, we need to fill in the missing detail on its metabolism, the difference between the ‘organic’ and ‘inorganic pools’, how regulation regularly goes wrong even in those seemingly consuming enough and how to balance the risks of this reactive medicine with its substantial therapeutic value. This recording comes with a great clinical tool to help you, at last, see the Sulphur strategy most indicated for your patient.
You can purchase Unseen Sulphur – Time to Take a Lookhere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
A few things really took up a disproportionate amount of our time & attention in 2020: Zoom, Mask Fashion & Gin based hand sanitiser.On a personal note I need to confess another: Iron. So while my one true (mineral) love remains zinc, iron answer hunting has infiltrated a lot of my days and some nights! There’s no hiding it…3 out of my 12 UU30 episodes this year have iron in the title 🙄 a sure sign its been on my and my mentees’ minds and sitting across the desk from a lot of health professionals in human form. And this affair I’ve been having, like most, started innocently… it started with a just a ‘quickie’, you know a quick question from a well meaning practitioner: “So, what’s expected in terms of ferritin levels across pregnancy?”
There are 2 answers to this. The first reflects the practice guidelines for GPs and obstetricians in most western countries: > 30 mcg/L regardless of trimester And then there’s another that is [ahem] evidence based, accounts for the essentiality of physiological anaemia in pregnancy &, naturally, trimester specific
There’s a big Fe-ar factor at play when it comes to answering the question, ‘Does this woman have enough iron for her and bub?’ Public health and practice guidelines appear to assume we are ‘guilty’ until proven innocent, patients are worried and health professionals are plagued with their own doubts about whether they’re ‘reading this right?!’ I’m sure we’ve all been in the situation where we feel our pregnant patient is doing well iron wise early in pregnancy, only for them to have that routine antenatal 28wk GP/Ob visit and discover a total panic has descended upon the patient and the rest of the health care team, with calls for ‘IV Iron STAT!’ But 28wks is the height of haemodilution right? You know, that time when ferritin, Hb and Hct should look at their lowest, right? There certainly is a limit to how low we want any pregnant woman to go – for her and her baby’s health but that limit is not the one routinely used and the truly evidenced based one is going to shock you. So what? What’s the issues if we are a little Fe-ar based about Fe, resulting in hypervigilance (calling a deficiency when there isn’t actually one) and giving them a ‘boost’ of more iron, surely this is good news ultimately for baby’s iron levels and for lactation and for…sorry what? No?
There’s a U shaped Curve for Iron supplementation & serum Ferritin levels in pregnant women?!!
It starts with a simple enough question: What should women’s ferritin levels be in pregnancy? But the answer will surprise many. There are in fact two. The first reflects the practice guidelines for GPs and obstetricians in most western countries regardless of trimester and then there’s another that is arguably more evidence based, accounts for the essentiality of physiological anaemia in pregnancy & is also, sensibly, trimester specific. To challenge the ‘noise’ and have the confidence that ‘normal’ is ‘enough’, we need to better understand the mother’s protective physiological adaptation of iron regulation and the intricate systems the foetus has to ensure its needs are met. This of course is not without limit, so we need to also be clear about the maternal serum ferritin threshold for negative impact on the foetus and newborn. Getting the balance or iron right in pregnancy for both mother and baby, is perhaps easier than we have been led to believe.
Well, obviously(!)…this has been a year heavy on pathology interpretation for me and the huge number of practitioners who’ve just spent the last 6 months taking that learning journey with me. I celebrate and congratulate them all for their commitment to their own professional development and also their investment, in what is arguably, the most potent yet overlooked set of skills of any health professional… the ability to read bloods. Basic bloods. Mainstream labs. No…but to really read them. Backed by all the scientific understanding about what these parameters actually are, how they perform and what they (dis)prove e.g. subclinical inflammation and ramped up oxidative stress – not an informed guess but mappable…right there but where no one else can apparently see it! But I digress!
Actually what I wanted to discuss was the whole erroneous notion of ‘normal’.
No, I am not speaking from the heart about my personal quirks, sense of humour or dress sense but rather the incorrect assumption that a reference range defines ‘normal’ and that our answer for each patient and each result is, a Yes or a No!
In this brilliant article by Whyte & Kelly published in the BMJ they spell out this falsehood succinctly. They note that the term ‘normal range’ has slipped into medical language from the misunderstanding that all lab results follow a Gaussian (aka bell shaped curve & later referred to as ‘normal distribution’) pattern but many simply don’t. So for some parameters a result near the ‘middle of the reference interval’ constitutes aspirational whereas for others it spells danger. Add to this, that these reference intervals are mathematically determined to reflect the expected values of 95% of your patient population (mean +/- 2 SD either side) so…that means the chance of a YES…”Your patient’s results are ABNORMAL!”… is just 5%. And hey…who said all the values within the reference range are all equally “normal” or better yet, healthy?! Not these authors, nor I, nor the praccies who’ve just done our course. So while, in many regards, these goalposts are too wide, they are also too narrow – typically only representing a subset of adults age-wise and Caucasians, yes they are both ageist and racist (yep, I said it!). And if our practitioners have learnt anything it’s about keeping an ol’ eagle eye on the sneaky intra-individual shift! Only spotted, of course, if you know your patient’s normal (not theirs compared to anyone else…just theirs) and then spot a shift. [I can hear they’re shushing 🤫me…they’ve got it already, alright!!]
So this is music 🎻to my ears, from Whyte & Kelly: “The intraindividual variation in laboratory values is usually much smaller than the interindividual variability (ie, the variation in the population). Variation in the concentration of an analyte, if significantly outside of a patient’s usual values (but still within the reference interval), could be a sign of early or latent disease”
So if you want to tap into the power of pathology…start with Whyte & Kelly, maybe even dip your pinky in the pool by checking out Accurate Pathology Results Interpretation Starts Here – an easy little 1.5hr kickstarter…or jump right in the deep end with the rest of us pathology reading polo players and sign up for the MasterCourse 1: Comprehensive Diagnostics for some DIY summer fun 🌊
ps I know your type and know that is EXACTLY the kind of weird nerdy thing you have planned for your break…you should see my summer fun list!!! 😅
MasterCourse 1: Comprehensive Diagnostics is a self-paced online program due for release in December. The course has pver 18 hours of video presentations plus 2 free bonus sessions 1) Accurate Pathology Interpretation Starts Here and 2) Patient Pathology Manager and access to resources and tools within, for your own use. This is a pre-requisite for MasterCourse II that will be delivered live in 2021.
This skillset has been found by many to be biggest ‘game-changer’ in Integrative Health You can view the full course outline here.
I talk so much about iron, I feel like I’m cheating on my life partner (Zinc)…but these two are arguably the main mineral deficiencies we encounter most consistently in our patients and, don’t tell Zn, but quite frankly, in terms of who’s more well recognised out there, Iron throws some serious shade! But the truth is they’re a ‘twofor’, as a result of their similar distribution in food, with both demonstrating significantly better bioavailability (read: virtually double) from flesh foods etc, ‘Watch out, she’s on the attack again!’ I can hear the V’s (vegetarians and vegans) say and yes I think you see this one coming…but I think it’s possible to be pro moderate meat, without being, antiV.
Ethical and environmental aspects aside (just momentarily) it is hard to argue against the nutritional benefits from moderate meat for most patients.
I tried, trust me. Put my own body on the line (and my babies) to be a vegetarian for over a decade. But as the wheels fell off for me, I noticed them falling off for so many others…and these were people who were educated, with a capital ‘E’ and putting serious ‘E for effort’ into substitution etc Not everyone of course – but a LOT of women and occasionally some men. There was no denying their ‘iron hunger’ (high serum transferrin), their movement towards microcytosis (however slight that ‘smallifying’ may be…we don’t wait for anaemia, right?), their poor zinc status and more importantly, the clinical chaos of impaired immunity, some cognitive or mood issues that presented, as a result. I went back to the mineral manual, back to all the science that helps us to understand these minerals especially in a modern dietary context.
Ah yes…meat has become marginalised in our diets compared to those of our yesteryear selves (ABS data) while our consumption of potential mineral inhibitors…you know, all the good, but bad, but good foods, like legumes and grains and green tea and and and…has risen…especially among the kind of clients who come to see us, right?
Which ultimately leads to a lower iron ‘income’ with the same outgoings, again especially for menstruating, pregnant & breastfeeding women.
The books don’t balance. (So then…IV Fe to the Rescue???)
Bite me…it’s just science. There have been some wonderfully thorough studies on this very issue and thoughtful discussions. This study in particular, by Reeves et al, of Australian women in their 20s followed for 6 years to 2009, argues that just a 1mg/d increase in heme iron from flesh foods could reduce susceptibility to the subsequent development of iron deficiency amongst omnivores. So while the median daily intake of fresh red meat in these women was just 39g/d, their analysis found that an additional 70g of lamb or 60g of beef…or about 140g of chicken and 250g of fish if you prefer white over red, appeared to be the positive tipping point for women and their ability to stay iron-replete. Well below ‘dietary guidelines’, nowhere near the scary cancer correlations (which of course may be more about fat or nitrates or ??). Moderate meat intake, right? Just saying. And don’t worry, I know. The only thing worse than an evangelical ex-smoker is a rambunctious reformed vegetarian 😂
Need A Manual on Minerals?
Minerals represent a critical tool in naturopathic nutrition and there has been an explosion of research in this area over the last 10 years. In order to optimise patient care, practitioners need to keep up with the constant stream of information, updating their previous beliefs and understanding in the process. This seminal 7hr seminar (!!)…yes…seriously..it’s THE MANUAL..is designed to facilitate and accelerate this process of review and re-evaluation via a fresh look at the key minerals iodine, selenium, iron, copper, zinc, calcium and magnesium.
When I deliver foundational nutrition training to GPs I talk tough. It’s a tough field, right? Compared with the relative certainty of pharmaceuticals, their established pharmacokinetics, their sophisticated delivery systems to ensure high bioavailability…trying to fix micronutrient deficiencies in patients can feel a lot like you’re trying to perform minor miracles. Take iron for something different, its homeostasis pivots on its tight regulation at the gut wall – and this is a wall that is very tight!! At best you get about 10% of a supplement taken up, at worst you get none and the harder you push & the higher you go with your dose…the lower the fractional uptake. Tough stuff, right?!
It’s about at this point in my talk I read their collective minds and say, “I know, you’re thinking, oral supplementation is for suckers – what about we bypass that road block and use IV?!” [Ok, I definitely use nicer words than this]
And then I put up a list of pros and cons about IV micronutrient repletion: ‘100% bioavailable’ & ‘Bypasses the body’s regulatory systems’, go on both! You see, time & time again we discover, when we think we’re outsmarting the body, it still manages to outsmart us. There are some exceptions to this – some nutrients (Vitamin C) and some contexts (late pregnancy iron deficiency) but the broader promise of ‘rapid replenishment’ for everyone, in your lunch break, via an IV infusion..is not realistic, responsible nor without risk. Don’t get me wrong, I am an advocate of appropriate IV Fe use and have encouraged a small fraction of my patients to take this path. However, given the dramatic rise in prescriptions for this since 2013, I think it’s time to stop and seriously review each element: In reality what does it achieve and in whom is it a responsible recommendation; Was a risk benefit analysis performed for & communicated to each individual & was the remaining risk mitigated?
Think anaphylaxis is the major concern? It might be the most lethal but there are more serious concerns due to higher incidence with newer preparations.
So, how well do you know your different IV iron forms, and their predilection for potential problems? And have your answers ready to all the questions raised above? In order for all involved to make an informed choice (both practitioners and patients), we must.
You’re welcome 😉 and hey welcome back to tough talkin’ Tuesday…
While rates of iron deficiency and related anaemia continue to grow, the increase in prescriptions of IV Fe have expanded exponentially in western countries. What is behind this change in practice regarding how we treat iron deficiency and does it match with responsible prescribing? Do the benefits always outweigh the risks? And while we’re on the topic, who is most likely to benefit and what are all the risks? In light of a current class action in the US, relating to a lesser talked about adverse event associated with IV Fe and recent complaints here in Australia against GPs, allegedly due to inadequate information to enable informed patient consent…it’s time to answer these questions and more. When is IV Fe a means of rescue and when is it a risky repletion strategy with no evidence of advantage?
Well that got tongues talking! We’ve cried, and we’ve laughed, hearing from practitioners about their ‘over-delivering donkey experiences’ for 2020. We’ve heard many memorable & relatable tales of either failures to set the best boundaries or even, in instances when we do, patients’ incredible dexterity to scale these in single leaps, ala James Bond style.
Practitioner: “On the very same day we talked about this important and ignored topic, I’d received an email at 9am from a patient asking for advice and a 2nd opinion about the prospect of surgery (first mention of this and clearly outside my scope!!!!), which they wanted before they saw the surgeon in 2 hours!!”
Sometimes it’s not patients, but professional colleagues (& friends)! I personally took an urgent call on Sunday morning from one of my psych colleagues, only because she is a dear friend, only to discover she needed help regarding a friend with mental health escalation…ah…yup…nup. Her blurred boundaries breached mine and then I bugged another colleague out of hours for further assistance…bad boundary blurring behaviour all round! We’ve been talking about the uncomfortable truth that a lack of healthy boundaries is a fast track to burn out for health professionals in group mentoring and the end of the year is always…opportune!
Mentee:“I felt challenged in a way where I was reviewing my own boundaries from an overall perspective over a period of time. I’ve worked in retail for 15 years now (as a student nat initially and then as a qualified naturopath) and I still find myself questioning how far I will go in certain respects especially when it comes to mental health (or people who appear vulnerable). When I was initially in practice I found my boundaries challenged to another degree, where I would accept every person who came through the door, whether I felt ready or not, or willing to take on the case, which essentially led me to burning out.
Now as I get ready to start again in practice, I feel more prepared to set clear boundaries from the get go (give myself permission to do that) and check in with myself if I feel they are about to be crossed or not in alignment with me. It feels like an important and healthy assessment tool to utilise as a health care practitioner.”
As a profession we need to pool some solutions.
Instead of the reflexive, ‘Just pop me an email if you have any questions’, at the end of each consult which can constitute the equivalent of a blank cheque (!!), perhaps we can say, “If you need to clarify any advice I’ve given you today drop me an email and for any other questions that arise, we can decide whether we need to bring your next appt forward or schedule a between appointment phone consult” Or if you’re a practitioner who sees the value (and there is much research to support this) in increased touch points with patients, for better compliance and improved outcomes, then structure your billing accordingly. This from one of our cluey new grad mentees, ‘If you want to offer this add-on time as part of your service then you need to account for it e.g. shave 15 mins off the actual face to face time that they’ve been charged for, so as to have this ‘up your sleeve’ for this express purpose. They breed ’em smart these days! Love it!
The end of the year is such an important time for reflection. What have you learned this year about your professional boundaries? Got some tips you’d like to share?





 I’m experiencing some serious POTTS exhaustion – how about you? No, not POTS, POTTS: Preposterous Over The Top Selling of supplements, which seems to be at an all time high even amongst our practitioner brands. I saw a product name recently that included the word, ‘supreme’!*^# Is the choice of nutritional supplements now on par with selecting our pizza toppings?
I’m experiencing some serious POTTS exhaustion – how about you? No, not POTS, POTTS: Preposterous Over The Top Selling of supplements, which seems to be at an all time high even amongst our practitioner brands. I saw a product name recently that included the word, ‘supreme’!*^# Is the choice of nutritional supplements now on par with selecting our pizza toppings?









 Well that got tongues talking! We’ve cried, and we’ve laughed, hearing from practitioners about their ‘over-delivering donkey experiences’ for 2020. We’ve heard many memorable & relatable tales of either failures to set the best boundaries or even, in instances when we do, patients’ incredible dexterity to scale these in single leaps, ala James Bond style.
Well that got tongues talking! We’ve cried, and we’ve laughed, hearing from practitioners about their ‘over-delivering donkey experiences’ for 2020. We’ve heard many memorable & relatable tales of either failures to set the best boundaries or even, in instances when we do, patients’ incredible dexterity to scale these in single leaps, ala James Bond style.