“How much can you misbehave & get away with it?” I listened with fresh ears, as a practitioner asked my son this question recently. I use similar ones with my own patients but hearing it from someone else, I could sit back and appreciate its true purpose and how well it achieves this. Most of us adjust our behaviours, when we can, to ‘manage’ things that cause us problems.
Sure I can eat food I haven’t made myself
………..but once a week is my max. or ‘X’ flares
My energy is pretty good …… but 1 night of poor sleep & I’m back on ’empty’
No impaired alcohol tolerance
………I just never have more than 1
My [insert: gut, skin, energy, immunity, mood] is not a problem
………as long as I don’t miss a dose (of supplement/medication etc)
And sometimes this ‘adjustment’ (or avoidance) is unconscious. Hence the beauty of the question: How much can you get away with, coupled with our understanding of how much ‘room to move’ there should be in a patient who is truly well. So the teenage to early 20s patient sitting in front of us, theoretically, should be in their prime of wide mischief margins, and we are alerted to individuals in this age group who are having to live like an older person, needing to exhibit vigilance around early bedtimes and allowing themselves almost no indiscretions. In contrast, as we age, we understand too, the margin for mischief narrows. Our over-50s selves are unlikely to get away with half as much as did in years gone by but we shouldn’t require the stricter self-care hypervigilance of our senior selves.
And for the patient who answers ‘no’ to everything on your GIT or stress/mood screening questions, for clarification, follow them up with, “and how much can you get away with and still have no issues?”
You may very quickly get a different understanding of what lies beneath and how much ‘management’ is required to maintain ‘balance’ or ‘no symptoms’ or ‘health’ 🧐
The primary objective of MasterCourse I is to realise the true value we can extract from the most commonly performed labs (ELFTs, FBE, WCC, Lipids & Glucose) which constitute the largest biochemical dataset we have on almost every patient. By learning how to comprehensively interpret these labs in an integrated medical framework, using the very latest science, we can extract the gold often buried in this goldmine. Accordingly, we prove ourselves to be the greatest asset to our patients, to other health professionals we are sharing care of patients with and we cut the cost of additional expensive testing, that is less well understood and validated.
MasterCourse I will help you access that gold and has been intentionally designed to match each lesson with real learning– with the time spent in theory and in application. Delivered across 24+ hrs of streaming video sessions with bonus pre-sessions, audios, resources and tools – this MasterCourse is likely to be a genuine game-changer for the way you practise and the potency of your patient prescriptions.
Something’s just come up today again and I think we need to talk about it. A positive result on a stool PCR microbiome test for H. pylori, understandably, might be heard as a clear call to action to go in guns blazing with an eradication approach. But is it? Trust me, I’ve had more than my fair share of battles with this bug & can understand being keen to have it be gone BUT first things first, let’s be clear about what the result speaks to.
Does it say, “Here! Look over here! Here’s the source of your patient’s GIT distress,” or even, “Here’s a pathogen that has taken up residence in their GIT and is a risk for future dx!”
No, not necessarily. It speaks to its presence.
And that may be only fleetingly, as it passes through. I’ve seen it before and so have many other experienced practitioners: a positive stool PCR that is at odds with the results of gold standard H.pylori testing, the UBT, faecal antigens or blood serology, all freely available through the GP. And the reality is, if you have a negative UBT, there’s no urease production, the trademark trouble-making of this bug. If you have negative blood serology, your immune system has never ‘met’ this bug or, in the minority of cases, you’ve tested in that brief early exposure window prior to antibody production (2wks) so you should retest within the month, to confirm or refute. And if you don’t have any faecal antigen…it ain’t in da’ house…so to speak 😅 If there’s something new here, then have a quick read of Medscape’s great work-up summary. So, clearly we need to confirm before we open fire.
We (me included) have been so single-minded about increasing the ‘sensitivity’ with our testing methods, we may have left ‘specificity’, in broader sense, behind & that creates a new problem.
This leads us and the patient down the garden path of false attribution and time and money wasted ‘treating’ a ghost gut issue. And no one wants to be put on a pylori protocol when they really didn’t need to. Trust me 🙄 But if someone does come back confirmed, well then…
For a bacteria identified just a few decades ago as being a cause of chronic gastritis, atrophic gastritis and gastric carcinoma, the escalation of number of antibiotics used to eradicate it (4 at last count + PPI) has been nothing short of breath-taking. A management approach more consistent with both integrative medicine and with an improved understanding of the delicate microbiome focuses on changing the gastric environment to ‘remove the welcome mat’. What do we know about how to do this successfully? It turns out…quite a lot.
If I could be granted 1 wish regarding all health professionals, it would be that we were all competent in reading Iron Studies. Think that’s overstating the issue? Or not a bodacious enough way to ‘spend’ my wish? I don’t. Especially when you consider the impact of GPs in this space.
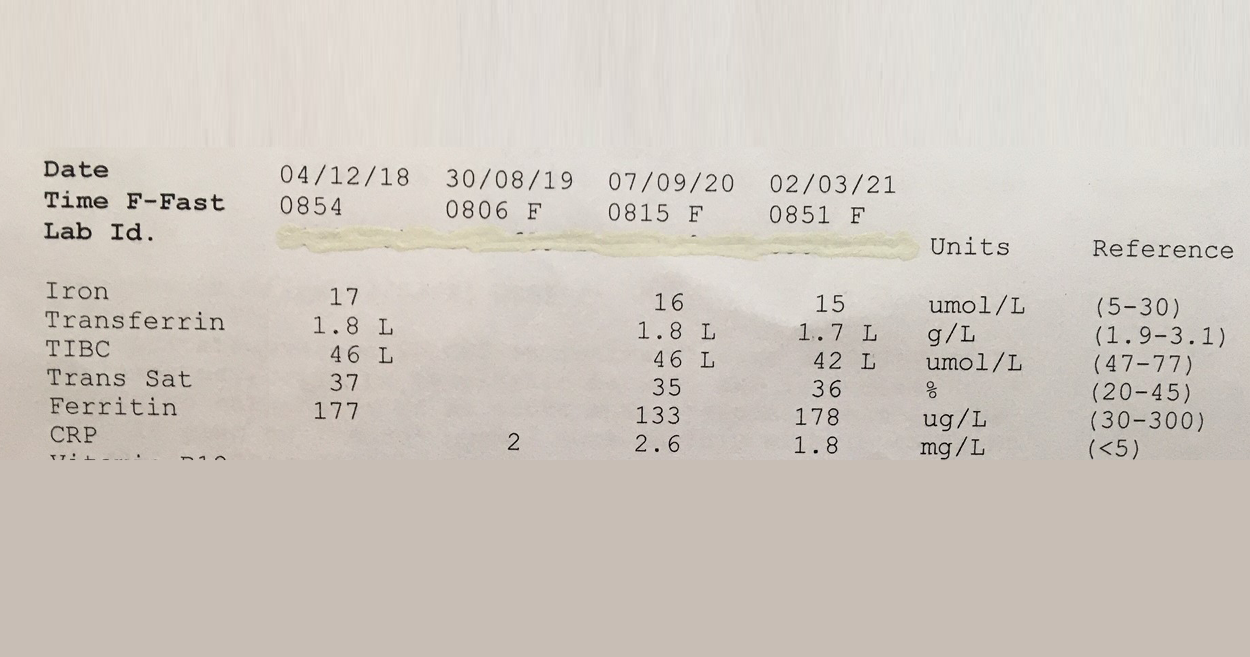
This 57Y male was asked to make a follow up appointment with his doctor, to discuss his ‘abnormal’ results which he was informed constitute Iron deficiency. Consequently he was was advised to start an iron supplement! #@!*
Your thoughts? Revoke this doctors medical licence? Insist on some very du jour ‘re-training’ at the very least? I mean, if you think this Iron pattern flags a deficiency or shortfall, then you’re as good as reading a map upside down and back to front…and written in a foreign language!! The ‘Ls’ in his latest labs flag he has suppressed transferrin, indicative of negative feedback inhibition of GIT uptake of this mineral, secondary to healthy stores or inflammation. And it’s not just that more iron is not indicated but that more iron in fact presents a patient like this with increased and unnecessary risk: to their microbiome, intestinal wall health, even according to the larger longer studies a potential correlation with colorectal cancer risk, if taken long term. Let alone the whole cardiovascular conundrum. Better still this same patient was told a few years back that he might have iron overload! Again the ‘map’ could only have been being read, upside down, back to front to reach such a conclusion!
So the one patient in just a few years by 2 different doctors has been diagnosed incorrectly with 2 different iron issues. Yep.
And sadly I have sooooo many more cases of missed and mis-diagnoses with regard to this mineral. The latest RCPA Position Statement on the Use of Iron Studies, underscores that assessment of iron status and GPs competence in knowing when to do this and how to interpret, is an important part of core general practice. Given it “is the commonest nutritional deficiency state in Australia and is significantly under-diagnosed” This succinct document offers a quick crash course in Iron nutrition for doctors and it hits all the right marks with advice about not ordering ferritin as a stand-alone because “the interactive nature of the three components allows for more accurate interpretation”and this simple but sage advice:
“Transferrin, iron transport protein, tends to increase in ID… A better strategy (than being tricked by Serum Fe) is to report transferrin saturation. A low transferrin saturation in the setting of an equivocal ferritin level is suggestive of iron deficiency. An elevated transferrin saturation is the first manifestation of iron overload.“
I mean seriously, do doctors read these RAGCP resources & recommendations, or is it just me? 🤓😂
Need a rip-roaring review on how to really read iron studies? Or know another health professional who does?!! Consider this Easter Educational Gift Instead of Eggs!! So You Think You Know How To Read Iron Studies?
Overt Iron Deficiency Anaemia or Haemochromatosis aside…do you understand the critical insights markers like transferrin and its saturation reveal about your patients iron status? Most practitioners don’t and as a result give iron when they shouldn’t and fail to sometimes when they should. This audio complete with an amazing cheat sheet for interpreting your patients Iron Study results will sharpen your skills around iron assessment, enabling you to recognise the real story of your patients’ relationship with iron.
Don’t know this thrash anthem for all nutritional medicine practitioners written by Supernova about 20 years ago? Do yourself a favour and check it out!! It makes me laugh to the point of tears every time. What also got me giggling recently was a coffee catch-up with a fellow nat (relax, it was decaf people!) Both being active women approaching the half century we found common ground discussing our ‘war wounds’. She, an ankle injury, me, lax ligaments in my knee thanks to touch football minus any pre-season prep whatsoever. I was waxing lyrical about the wonders of swimming, which I’ve taken up to heal said gammy knee, at which point she asked, “What are you taking for it?”
My mouth dropped open & nothing came out…because the answer was *!NOTHING!*😂 At which point, she mentions a couple of supplements I have *!ON MY SHELF!* that really helped her ankle 😂😂
I text her 3 days later with, “Man, our medicines really work!!” You see, like the song says, I do ‘take my vitamins’ and ‘they’re good for you! Good for you!’ – just this physician health yourself thing can be a blinking full time occupation sometimes! Anyway, it got me thinking about how we choose the products we do. So turmeric caps are part of my new regime and they seem to be working a treat. I stock one brand only. Now how did I come to that decision amongst an ocean of options?! Well in this instance, I had asked a colleague who works OTC and dispenses a variety of turmeric products en masse – better still she sees those people come back either for more…or not. I’ve found asking my well-placed peers about these kind of products invaluable!! But there are so many different ways each and everyone of us may have made product choices – ethical concerns, personal experience, research, a teacher, mentor or rep’s influence. Anyone who has done the UTAS post-grad, of course, has exhaustively analysed the options, complete with comprehensive spreadsheets of all comparative products…god love these guys!! But for the rest of us mere mortals, how do we make such choices?
Let’s just talk turmeric for now, I’d love to know…
My gorgeous sister first brought this ditty to my attention & we’ve had a wonderful trip down memory lane today (with our elderly mother as our hostage as we both belt out the lyrics in laughter down the speaker phone)…she’d be cross if she didn’t get the credit here, rightly so 🤣
I’m gonna take my vitamins! (Vitamins! Vitamins!) You better take your vitamins! (They’re good for you! They’re good for you!)
You better take your vitamins, Two by two! Two by two!
I’ve seen two 20-year-old young men in my practice this last month who’ve already made a lasting impression on me. The first, is buff, full of cheek and humour while deeply engaged with his health, earnest in his desire to understand his 7 years of daily upper gastric pain, for which he has read much, changed his diet & given up what most 20 year olds would consider their rite of passage and right (late nights and alcohol). The second is pale, gaunt, neuro-atypical, full of tics and avoiding eye contact at the beginning of each consult, only to look me solidly in the eyes as he reveals incredible insight about ‘being different’ & his desire to be able to engage with something/anything so that he can live a more normal life, by the end. What do they have in common?
They’re 20 & trying to make their way in the world. Undertaking all these newly autonomous actions, previously taken care of by parents, including fronting up to a health professional with concerns, seeking understanding and support.
The first, in spite of 7 years of gastric pain and irritation (I can see mum took him to a GP with similar concerns at 13 years & again at 15!!), self-reported extreme worsening with gluten exposure and a family history of similar GIT issues, was not offered a single investigation by the GP they visited but was given a month long trial of a PPI. I caught him 3 days in. Was he feeling less pain? Yes? What does this mean? He has gastritis at best, something more sinister at worst? Does it reveal the cause? Not one iota. But tests for H.pylori, coeliac disease and a few other basic labs, might. Does it offer a long-term solution? Nope – even the GP said , ‘Now this will probably help but you won’t be able to stay on this too long!” While up to 80% reductions in gastric acid, will definitely lessen gastric irritation and pain for most, will a month ‘fix’ anything? Unlikely. Especially when the well-documented withdrawal rebound effect kicks in, once he stops! After a month of actual stomach repair work, he’s feeling dramatically better and yes, we’re still pushing for those test results.
The second 20yo, was seeking a mental health care plan from a GP he’d never seen before. He walked out after 15minutes instead with an SSRI.
With a diagnosis of Asperger’s at 12, ADD at 13 and a series of high level neurocognitive assessments and stimulant trials – how could anyone make an informed decision about appropriate medication for this neurobiologically complex individual in 15mins, while simultaneously ignoring his request for hands-on psychological support? I was a bit stunned. He was too. How long, and how much effort and courage, will it take for him to make another appointment, get himself back to a medical clinic and ask again? He struggles to remember to eat. I’m glad he came. I can’t offer all of the services and support he needs, far from it, but I can listen long enough to ‘see him’, acknowledge that his personal priorities and values are valid and in turn, direct mine in terms of how best to support him. I can also try to encourage him not to give up on getting the support from others he desires and desperately needs. This is not gender specific of course – I’ve heard similar stories from young women. I remember being 20 – perhaps all health professionals need to take a moment to remember what that was like too? 🤔🤗
That’s not a word you hear often spoken by people practising nutritional medicine. Which is odd. I mean outside of the whole, ‘I’m not good with sulphites so I just have to add these magic drops into my glass of red so I can knock back my share,” often overheard at our conferences… it’s like this essential macromineral, pivotal to human health for things like barrier function, antioxidant defence and our basic ability to create the white cells for immune defence (for that matter), detoxification, musculoskeletal tissue integrity etc has just not received its due attention from us. Not entirely surprising given 1) there’s no RDI and 2) there’s no lab test to assess an individual’s status and how about 3) because we were never taught about it!
But the biggest ‘call to action’ here is that, in spite of items 1, 2 & 3, we’re ‘prescribing’ Sulphur Strategies all the time!
Take one of my favourite examples;GAGs. Glycosaminoglycans like Glucosamine sulphate (not the crappy, found to be not as effective, other forms that we now see more commonly) hit the headlines back in the noughties as an effective arthritis remedy. This is one of the 100s of our body’s ‘end products’ of its endogenous Sulphur Stream. We naturally make this in adequate amounts to ensure the integrity of our joints (and many other tissues of course!) when we have enough Sulphur in the ‘top pool’ (organic Sulphur) to trickle down to the 2nd pool (Inorganic Sulphur), therefore creating a constant essential supply of something known as ‘the universal Sulphur donor’ – ‘PAPs’, to its friends 😉 Like a waterfall, it helps to have a good flow from the top to increase the likelihood we’ll have anything to ‘show’ at the bottom.
So when we give a patient Glucosamine Sulphate it may well help. Or not. But did we ‘treat the cause’ of their Sulphur problem? Should we have treated higher up, increasing the size of either the organic or inorganic pool to have improved and widened the benefits for their health? Or, as is equally common, actually identified why someone might need more Sulphur than most – due to increased demand and losses?
Herein lies my reason for liking this particular Sulphur story somuch. The common medication that places the highest ‘demand’ on Sulphur (due to its need for detoxification) is paracetamol. There’s no debate regarding this – just absolute scientific consensus. NSAIDs and steroids also negatively affect the Sulphur status of individuals, as does Vitamin D deficiency and chronic mild metabolic acidosis. Now how commonly are these phenomena co-occurring in our patients afflicted with arthritis? And traditionally of course, what was the remedy for arthritis? Sulphur springs.
Unseen Sulphur – Time To Take A Look If you don’t have a clear picture of the gross daily requirements, determinants of altered individual needs, sources, regulation & associated deficiency picture of Sulphur, you’re not alone. Turns out this essential macromineral remains ‘unseen’ by most, even though you’re probably writing prescriptions every day that have Sulphur as their key component. From the simple: Taurine, N-acetyl cysteine, Protein powders, to the sublime: Brassica extracts & concentrates, N-acetyl Glucosamine, Alpha Lipoic acid etc. In order to use these Sulphur strategies successfully and safely, however, we need to fill in the missing detail on its metabolism, the difference between the ‘organic’ and ‘inorganic pools’, how regulation regularly goes wrong even in those seemingly consuming enough and how to balance the risks of this reactive medicine with its substantial therapeutic value. This recording comes with a great clinical tool to help you, at last, see the Sulphur strategy most indicated for your patient.
You can purchase Unseen Sulphur – Time to Take a Lookhere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
28 years ago I was in the midst of my own mental health crisis
24 years ago I graduated 20 years ago I dipped my toe into first year uni psychology units 18 years ago I worked in psychoactive medicines with a pharmaceutical company 16 years ago I began combining all my learning (pharmaceutical, psychological, naturopathic) to truly reinvent & optimise my approach to supporting patients with mental health presentations …And every day since I’ve remained passionate that we can offer an important and potent contribution in the management of mental health, when we do it well, and I want all of us to do it well.
So 2 years ago I started the Mental Health Primer Mentoring, to do just that.
Every year I learn more about mental health (from patients, mentees, mentors and via my ongoing active research) and each year this learning is reflected back into the content for the Mental Health Primer. It’s an exciting dynamic process. I don’t share the same beliefs I did, 5 years ago on certain testing and a few treatments, the research has moved on and in the last year alone I have refined my models for CNS histamine imbalance, reacquainted myself with a couple of old forgotten friends prescription-wise, which are working well, and discovered a couple of totally new BFFs! In this group, we keep it real, nothing stayed and static, no questions unaskable. And by mapping out and really taking the time to learn a tried and true ‘process’ by which we can navigate our way with seeing, recognising and supporting each individual in front of you, we feel confident in designing truly individualised mental health management approaches
“Honestly, I have to say all of it was valuable. The info re neurotransmitters, pathology,
questionnaires – truly brilliant. Changed the way I practice!” – Chris, Naturopath
“Very relevant to myself and practice, as it will completely change some of my treatment methods and gave me more confidence.” – Di, Naturopath
The Mental Health Primer Group gives you all the other skills and knowledge needed to really help patients with their mental health…that are as a) important as anything in a bottle and b) help the ‘bottles’ work better and c) direct you to the best ‘bottle’ in the first place. Like understanding the trajectory of certain diagnoses, recognising red flags, the need to rewrite your regular consult for patients with primary mental health presentations to get the most important information and adjust your expectations: never setting them up to fail etc.
Our Mental Health Primer Mentoring Group is topic based and here are some of the ones we cover…
MH Safety – Keeping You and Your Patients with Mental Health Problems Safe Neurobiology in a Nutshell – Digging Deeper into the Diagnoses Questions and Case Taking Skills Mental Health Assessments – Learning How to Use the Best Tools Out There Interpretation of Pathology Markers Through a Mental Health Lens Referring & Referral Letters for Mental Health Case; Treatment Options in Mental Health Boundaries, Barriers & Behaviour Change in Mental Health Management
I hope you are as passionate as I am about the enormous contribution we can make here but we also agree that a) we are flying under the radar as significant contributors in mental health care with the rest of the providers unaware and b) our training might be falling short in preparing us for this kind of client base and important role. Now is the time to step up to that plate en masse as soon as we can.
If you’re interested in joining our Mental Health Primer Group for 2021
then email us at [email protected] to receive your application. For more information on Group Mentoring and the extra bonuses you have access to click here. APPLICATIONS CLOSE 22 NOVEMBER
Well that got tongues talking! We’ve cried, and we’ve laughed, hearing from practitioners about their ‘over-delivering donkey experiences’ for 2020. We’ve heard many memorable & relatable tales of either failures to set the best boundaries or even, in instances when we do, patients’ incredible dexterity to scale these in single leaps, ala James Bond style.
Practitioner: “On the very same day we talked about this important and ignored topic, I’d received an email at 9am from a patient asking for advice and a 2nd opinion about the prospect of surgery (first mention of this and clearly outside my scope!!!!), which they wanted before they saw the surgeon in 2 hours!!”
Sometimes it’s not patients, but professional colleagues (& friends)! I personally took an urgent call on Sunday morning from one of my psych colleagues, only because she is a dear friend, only to discover she needed help regarding a friend with mental health escalation…ah…yup…nup. Her blurred boundaries breached mine and then I bugged another colleague out of hours for further assistance…bad boundary blurring behaviour all round! We’ve been talking about the uncomfortable truth that a lack of healthy boundaries is a fast track to burn out for health professionals in group mentoring and the end of the year is always…opportune!
Mentee:“I felt challenged in a way where I was reviewing my own boundaries from an overall perspective over a period of time. I’ve worked in retail for 15 years now (as a student nat initially and then as a qualified naturopath) and I still find myself questioning how far I will go in certain respects especially when it comes to mental health (or people who appear vulnerable). When I was initially in practice I found my boundaries challenged to another degree, where I would accept every person who came through the door, whether I felt ready or not, or willing to take on the case, which essentially led me to burning out.
Now as I get ready to start again in practice, I feel more prepared to set clear boundaries from the get go (give myself permission to do that) and check in with myself if I feel they are about to be crossed or not in alignment with me. It feels like an important and healthy assessment tool to utilise as a health care practitioner.”
As a profession we need to pool some solutions.
Instead of the reflexive, ‘Just pop me an email if you have any questions’, at the end of each consult which can constitute the equivalent of a blank cheque (!!), perhaps we can say, “If you need to clarify any advice I’ve given you today drop me an email and for any other questions that arise, we can decide whether we need to bring your next appt forward or schedule a between appointment phone consult” Or if you’re a practitioner who sees the value (and there is much research to support this) in increased touch points with patients, for better compliance and improved outcomes, then structure your billing accordingly. This from one of our cluey new grad mentees, ‘If you want to offer this add-on time as part of your service then you need to account for it e.g. shave 15 mins off the actual face to face time that they’ve been charged for, so as to have this ‘up your sleeve’ for this express purpose. They breed ’em smart these days! Love it!
The end of the year is such an important time for reflection. What have you learned this year about your professional boundaries? Got some tips you’d like to share?
I feel a bit Trumpy…because whenever someone says ‘N-acetyl cysteine’, I want to reply, “Big fan, I’m a big fan”. And yes that’s an uncomfortable awareness. But unlike he who shall not be mentioned, I can qualify my statement and provide supportive evidence, both of the research and real-world varieties. So, of course, can so many of you as well. I know of fertility specialists who place it in PCOS patients’ preconception prescriptions and respiratory specialists who regard it highly in COPD, CF and a range of other conditions. And I am a signed up supporter of its adjunctive use in many psychiatric conditions. Then there’s the biofilm-breaking buffs…
This is where non-believers might be tempted to call ‘Snake-oil!’
How can one very simple tricked-up amino acid possibly contribute to the health of so many systems? Oh, just via the chameleon qualities of its chemistry of course! As a rate limiting ingredient and precursor of GSH, as well as a potent mucolytic agent and and and…we get it. We surrender! But I want us all to back up here just a few steps. As a mucolytic agent…renowned for biofilm busting…hmmm. I prescribe a lot of NAC for a lot of people for a lot of days-weeks-months….because all the research in mental health points to it being a long-term intervention. I’ve heard Professor Michael Berk say, that patients still on it at 2 years had even more improvements than they had experienced at the 6 month mark and of course mental health, for most, is a chronic illness, so no one is surprised.
But we can’t contain its chameleon chemical qualities. Given orally, it will be having effects within the gut of these individuals on the way through…and not all biofilms should be busted, right?!
So what to do? Well thankfully, NAC is not something that patients rely on for short term acute effects, that would then make missing doses problematic – like pharmaceutical psychiatric medications, and some CAM options as well potentially, like SAMe and SJW. So a regular sNAC break is likely to be free from negative impact for those with mental health issues and in fact, beneficial long term. With all this in mind, we’re now using a dosing model of taking weekends off from this supplement – which works for most. Do we have any concrete research to say this makes sense and doesn’t compromise efficacy yet? Well no, and don’t hold your breath, because research can be very reductionistic (you heard it here first LOL) and there is a lack of consideration of the effects on an individual as a whole. The psych researchers are not measuring the impact of all interventions on the microbome of patients (yet!) and the gut researchers not always monitoring the mind. But we clinicians can pioneer the path, fuelled by two old buddies of mine: first do no harm & least medicine, best medicine, right?
Oh and has anyone managed to open a tub of NAC and not accidentally snort some?…I don’t have anything else to add or a solution, I am genuinely asking if this is humanly possible 😂
“There are few complementary medicines that come onto the market with such a bang, opening up genuinely new therapeutic options for the effective management of such a broad range of health complaints. N-acetyl cysteine stands out for this reason and has changed the way I practice” Rachel Arthur
Want to learn more about its diverse applications? Check this out
No, mastication. I’ve touched on this before but I believe we need regular reminders. Or maybe that’s just me? I am a fan of chewing. I don’t profess to be good at it (I am a wolfer of food tbh) but I see the enormous therapeutic benefits it has to offer. Seriously. Think I’m taking the mickey? Here are some tasty brain bytes for you!
Ancient Mayans – Chicle Ancient Greeks – Mastic Gum Native Americans -Sugar pine and Spruce sap Then there’s of course the Coca Leaves (South Americans) Betel Nut (Asians) etc
But putting aside those that come with a buzzy bonus🙄 …the tradition of chewing non-digestible substances between meals according to anthropologists and archaeological evidence dates back to the neolithic period. Nowadays, of course, we barely break from constant feasting…but perhaps when we do, we should maintain the mastication? There’s a lot to be said in favour of this. From brain benefits to dental deterrents against plaque but of course the main gain for many – is the potential for better digestion. For GORD it’s the oldest trick in the book, right? The increased saliva generated by the process neutralises any untoward excess acidity in both the oesphagus and also the pharynx. So naturally, not one to forget in Barrett’s oesophagus either and of course my beloved Silent reflux. While also producing greater amounts of salivary amylase to assist with CHO digestion and lingual lipase to kick off the first fat digesting process within the stomach. But could it help beyond this? Well, though the jury is out on this increasing the rate of actual gastric emptying (though still worth a crack in Gilbert’s Guts), it’s well regarded as being able to stimulate small and large bowel motility more generally. Some SIBO soothing in certain scenarios, perhaps? So much so, it has been recommended post almost all types of surgery (GIT, gyne, renal etc) to ‘get things going again’.
And while this doesn’t have the highest quality evidence to support efficacy…encouraging people to trial chewing a natural gum – no pretend sugars, no plastics & no PK for my patients (Sorry dad! ), is a recommendation that is accessible to just about everyone, easy to try and gives people a quick yes/no.
Yes I come from a long line of chewers. My dad chewed gum between meals and during them, he popped that piece behind his ear to ‘save for later’. I swore there and then, as an offended on-looker that I would never be so disgusting. Well… I’ve finally turned into him and I think he might have been onto something 😉 [except the behind the ear bit…ewwwwwwwwwwww]
Chronic dry coughs, rhinitis, postnasal drip, the sensation of ‘a lump in their throat’ or even asthma? Have you ruled out silent reflux aka laryngopharyngeal reflux? This UU30 helps you to better recognise the myriad presentations of this condition, understand the latest about why it occurs and is on the increase & finally outlines my top & somewhat unusual interventions for management of these presentations that have proved highly successful in my own clients. Up-skill on this sinister ‘silent’ one, here!~
We’ve been talking all about the dangers of excess fuel in our blood recently. You know, just like nature…too much fuel underfoot creates a fire hazard. So too in the bloods of our patients. The key fuels I am referring to, of course, are lipids (triglycerides & cholesterol) and glucose. Our tissues need ready access to both but Balanced Blood Supply & Mastery of Management is key.
In terms of excesses, lipids play the long-game…wreaking havoc over a long period primarily via their vulnerability to form peroxides, which in turn create a chain of oxidative stress and depletes our antioxidant artillery.
In contrast, even outside of insulin dependent diabetes, for the rest of our patients, glucose plays a fast and furious game, being a highly reactive substance capable of causing both glycation and oxidation. We describe even high-normal levels of glucose as something akin to the ‘Bull in the China Shop’, disrupting the function of the endothelial linings and damaging a variety of plasma proteins (not just haemoglobin) that float within them. But do we have a way to routinely measure the level of damage occurring in our non-diabetic but somewhat glucose intolerant patients? Sure! Just check the C-CCTV footage!
The extra C stands for ‘Carb’ and yes we can potentially check the Carb-Closed-Circuit-TV ‘tape’ in every patient.
It’s called HbA1c and measuring this provides us with an opportunity to review their personal ‘tape’ of the last 2-3 months for evidence of excesses.
Helpful, hey. But we actually have so many great tools through regular routine labs at our disposal to understand the glucose disposal or dys-disposal(!) at play in our patients! You’ve just got to know where to look (urate, triglycerides, insulin, HOMA-IR etc) and what each piece of information is telling you. We’ve had SO MUCH FUN with this particular topic in the MasterCourse this month…or is that just me 🙄 No, I know it was, because our live session chatbox was full of ‘blown brain emojis’!! 🤯🤯🤯 I can’t wait to share this course content far and wide at the end of year with those of you that missed out on attending live.
In the meantime if you want to learn more about glycation which is the new inflammation, out there in research-land, you know…the source of all evil including ageing itself(!!) then check this out…
Glycation is a normal physiological process that, just like inflammation and oxidative stress, can get out of hand, contributing to disease processes. Currently there is an explosion of correlational research suggesting relationships between higher levels of Advanced Glycation End-products (AGE) in individuals who have fertility problems, psychiatric conditions, osteoporosis, premature skin ageing, cancer…you name it! New research implicates diet heavily in the determination of individual’s levels of AGE but there is devil in the detail – there are ‘4 Ps’ of dietary AGE contribution that we need to be mindful of when we are giving dietary advice and trying to move patients towards wellness. This Update in Under 30 recording: Are You Feeling Your ‘AGE’ will open the lid on the ‘new black’ in chronic health & ageing.
Recently a mentee reported that when attending an in-person training event (remember those, everyone?!) she approached a sponsor’s stand, promoting practitioner training in the nutritional management of mental health, based on the pioneering work of American scientist, Carl Pfeiffer. But when she and her nat buddy started asking questions, those manning the stand asked whether they were doctors and then, upon finding out they were naturopaths, encouraged them ‘to move along – this information isn’t for you then’. Or something to that effect…Ouch!
While I know a little about the decision behind offering this training only to doctors and specialists at this time, and I do understand that organisation’s reasoning, I also want to reassure you, this doesn’t mean that Pfeiffer’s important work, and the efforts of those that have followed him, is out of bounds to others.
No one can copyright cortisol or TM TSH, right? Equally, Histamine is his own man. Carl Pfeiffer and others brought histamine, the neurotransmitter to centre stage and many of us working in mental health remain eternally grateful for this. But CNS histamine has come a long way since then…and is currently a very hot topic in modern molecular psychiatry where they are always looking for new drug targets, given shooting at the previous ones, risked taking ‘an eye out’! The recognition of histamine as a key player in mood, cognitive and behaviour has been long overdue but is absolutely here now! Just give this search term a whirl in PubMed: histamine AND psychiatry, and you’ll be hit with quite the crush of citations!
An abundance of important info at your fingertips…no secret handshake required.
It was, in part, this story that inspired me to record an Update in Under 30 on Histamine Imbalance in Mental Health. Just the proverbial straw on the proverbial camel really, after years of examining, experimenting and experiencing the incredible results some patients can achieve when this imbalance is identified and redressed. So I’ve done my darndest to pull together those years of hands-on helping histamine imbalanced patients with the latest literature in under 30 minutes!! Surprise! I failed!There is a lot to convey but you’ll also be surprised by what I don’t say…there’s no infinitely long list of personality peculiarities that fit with too much or too little. Nor is there a didactic discourse about absolute treatment dos and don’ts. I’m communicating the common ground between the original evidence, clinical empiricism and contemporary neuroscience. So this month, consider the ‘under 30’ bit, merely a ‘Serving suggestion’…which would necessitate you playing it 1.5 X speed…go on, I dare you!!😅
About 15 years ago I was introduced to Histamine as a neurotransmitter. Not the allergy mediator or the ‘basophil baddy’ but rather this prolific and potent neurochemical we all produce in our brains which, in the right amount, regulates almost every biological rhythm, helps with memory and mood & much more. Being able to recognise excesses or deficiencies of CNS histamine in mental health presentations and, ever since then, fine-tuning my ability to support patients with these, has changed my practise forever and has been the key to some of my patients’ greatest recovery stories. Forever grateful to the pioneers of this model, 70 years on, the model is ready for a mini-makeover, to bring it in line with the current scientific understanding of histamine, methylation, genes and much more. This recording, together with a hugely helpful clinical resource, will give you the confidence to recognise and remedy this important imbalance in mental health. If you want to download this recording click here.
Given1 in 8 Australians right now are taking an antidepressant, chances are you’re seeing a lot of clients on these, especially the SSRIs. Erica McIntyre (fellow naturopath) and colleagues, found that in fact, mental health diagnoses affect about 43% of individuals who choose to seek help from a naturopath or herbalist, so clearly this is across all of our waiting rooms. Accordingly, by this stage in your clinical career you’ve probably seen more than 1 patient taking the identical SSRI – e.g. Citalopram (aka Lexapro or Cipramil) Have you also by now, therefore come to ‘expect the unexpected’, when it comes to patients on the same prescription, in terms of ‘weight effects’? The majority not reporting this to be a major concern or issue but the occasional client, experiencing such significant weight gain, they may even have seen this as a reason to discontinue the medication. So what’s up with that then? Don’t we all wish we knew for certain! But getting our heads around the potential mechanisms is important for our patients, in terms of making more informed choices, as well as offering us insight perhaps into their neurobiological nuances.
Some of you will know, this used to be my place of business.
I have a background in the pharmaceutical industry, specifically psychiatric meds, more specifically SSRIs and even I find every time I duck-dive back into the literature I come up with more ‘fish’ – critical new information about mechanisms, secondary and unexpected actions, unforeseen benefits, barriers and yes, some sad or bad new detail. Consequently, I always field lots of questions about SSRIs in our mentoring sessions & one that often comes up is why some patients gain weight on SSRIs. What’s most curious to many, is how the weight effects of antidepressants can be hard to predict. There is not a consistent pattern across any specific antidepressant class, nor just 1 or 2 medications within a class, that will do it, while the others never will. This is in contrast to the many determinations and drivers for who will or won’t get discontinuation syndrome. So what mechanisms might be behind such an individualistic weight response and is there any way to predict or prevent this?
Here we find ourselves again with the question that keeps all IM practitioners awake at night: But why? But why?? But why???!
A worthy question indeed. According to comprehensive reviews of this issue: there are still multiple candidates – one is the incidental histamine blocking that some SSRIs exhibit (could this flag someone low in histamine to start with??), while others still hold some suspicion over an old foe, elevated prolactin, that we can see in a minority of patients on these meds…easy to measure and confirm or refute, right? But always ask your patients first, How has your diet changed over this same period? How has your activity changed? You may of course find, you need look no further. People can give you the answer on a platter with things like, “I just relaxed a lot more: about what I ate and my weight”…Bingo! As always, the patient in front of you is their own little ultimate black-box…🧐
Never our call to make, but with 1 in 8 Australians at any time taking antidepressants, playing a supportive role for patients wishing to discontinue their antidepressant medication is common. So what do we know, about how to really do this well, what to expect and how to perhaps mitigate some of the bumps that might lie ahead. What in our artillery should we go in armed with either during the discontinuation or, better still, beforehand? This Update in Under 30 outline the key principles of patient prescriptions in this context and may assist patients, in their desire to truly leave the antidepressants behind.
If you are an Update in Under 30 Subscriber, this is a previously release episode and you will need to search for it to find this in your library of UU30’s that are in your online account.
Not an Update in Under 30 Subscriber? To access this episode and the entire library of Update in Under 30 audio’s and resources become a subscriber here.
Now find a comfy spot everyone & I’ll tell you a story…’Once upon a time, a long long time ago, we lived our days out in the dark, regarding potential calcium dysregulation!’But ever since serum Calcium has become a standard lab included in most routine screening tests (General Chemistry aka ELFTs) abnormal calcium handling is no longer an ambush for patients of ‘stones, moans and abdominal groans’, as the saying goes in hyperaparthyroidism. A diagnosis historically only mad, when someone presented with this constellation of rather advanced symptoms. But actually being able to identify your patients’ typical blood calcium levels offer us so much more than just a heads-up re parathyroid disease
It may tell us something about their Magnesium status, cardio cautions, be a bit of ‘bone barometer’ and probably most immediately important, flag their suitability for calcium supplementation!
Yep…rather than the current-criminally-crude-calcium-checklist: 1. Patient is female 2. Patient probably doesn’t consume enough calcium 3. Patient may be at risk of osteoporosis (yup…that accounts for practically every woman, right there!)
But seriously, if you just do a full review of the vast literature on this topic, what?! Not enough time?! How about then, just skim read a couple of key papers? Still baulking at that?…maybe just a wafer-thing editorial (??!) will tell you that, consuming elemental amounts of calcium (> 250mg), that are beyond even the biggest Dairy Diva’s Diet Diary, may be deeply problematic for many. And guess what…this doesn’t pertain to supplements alone…even calcium fortified foods are not free from concern! But let’s not let yet throw all our calcium fortified foods in the same bin as the folate ones we did a while ago!! Let’s step out of the dark and into the light that shines upon us, care of fasting serum Calcium measurements, to help us recognise whether Calcium is the cause, the consequence, a cure or a curse for person sitting in front of you 🧐
The Calcium ConspiracyControversy Continued
The Calcium Conspiracy arises primarily from misperceptions about it being ‘the boss of bones’ but becomes more of a controversy when in spite of ongoing advice for broad-scale use we review the evidence and have to acknowledge that the recommendation to supplement post-menopausal women with large doses of Calcium, not only lacks strong evidence but may cause harm to some. In this detailed discussion of the two schools of thought – Rachel finds a position somewhere in between. Reinforcing the need for an individualised approach and personalised risk benefit analysis while teaching you how to undertake this in every client.
The latest Update in Under 30 has landed!!!
You can purchase The Calcium Conspiracy Continued here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
Gotta love all the clever inquisitive minds among our integrative health practitioner community. I think each of us, as children may have been that one kid who just never stopped asking questions. What a great quality to have because it prompts us to think outside the box, then outside the triangle, then the hexagon and beyond! Simultaneously, busy minds that never stop questioning and never quiet down can also feel like a curse! None of us have the time to go find the answer independently to every single question that our patient, prescription & pathology encounters raise for us. We need to use the force. Our colleagues, our workmates, our informal and formal practitioner networks, our mentors, our associations, our educators etc.A lot of practitioners recently got some questions answered with the Update in Under 30: Separating the B12 from the B*S#!...and then guess what…they had some more B12 related questions 😂😂
Q: What might a normal or even high serum B12 together with low Active B12 combination flag in a patient?
A: Exclude COCP use, & gross liver pathology, refer for B12 antibodies if possible & review the case for other evidence of functional B12 deficiency, as TCII values are more specific and sensitive than serum
Q: What evidence do we have to use a higher cut-off value than the labs give us for Serum B12 (< 400 pmol/L), as a decision limit for follow-up investigation for B12 deficiency
A: Just the findings of some of the biggest studies on B12 assessment – correlating serum values and markers of functional deficiency such as Harrington et al 2017, Spence et al 2016, which flag that there is already metabolic impairment typically when serum values drop below 400, well before the classic features such as macrocytic anaemia
You’re welcome 🙂 It’s nice to be surrounded by like-minded curious kids (disguised in big people’s bodies!) I love playing my part in adding to the collective knowledge in different ways and for those of you who are our Update in Under 30 subscribers, and of course anyone that purchased this as a single download, well we’ve gone that extra step and put together a nice little pdf: A B 12 Assessment Decision Tree for you and added that in as a bonus to your Separating the B12 from the B*S#! episode. So go take a look now and hopefully that answers just a couple more questions and we can all have at least 1 good night’s sleep… before you come back with more 😉 🧐 😂
B12 is a routinely under-rated and recognised micronutrient, which is in fact in high demand by many of our patients. As nutritional research pushes back against defining adequacy as simply the prevention of the deficiency-associated disease (macrocyctic anaemia, irreversible neurological damage) we enter a new landscape of more individualised approaches where we’re better able to recognise and treat those at risk of falling below ‘optimal’. But how do we accurately identify this and then choose the ‘best’ B12 (methyl- cyano- adenosyl- hyroxo-) supplement? Does it need to be this complex? Time to sort the B12 from the B*S#!!
This recording comes with a bunch of great resources including a clever clinical tool.
And now a new one to boot!!
________
You can purchase Separating the B12 from the B*S#!here
If you are an Update in Under 30 Subscriber, you will find the new resource in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
You guys know I can’t help myself. For the last year or so I’ve been immersed in developing and redeveloping and redeveloping 🤓 [ahem apologies to my team!!] teaching tools for all practitioners to better understand what the routine renal markers can offer us in terms of understanding our patients…and it is far above and beyond renal function, promise. Just one example of this, is the sophisticated yet incredibly simple urea to creatinine ratio calculation that I was originally taught by Professor Mel Sydney-Smith. In adults with preserved renal function, this is the key to the kingdom, in terms of being able to objectively quantify whether patients are truly meeting their own individualised protein requirements. The Marvellous Mel (well he is, who can argue with that?!) added this one to my toolkit a long long time ago and in turn, I’ve been using it and spruiking it ever since.
In fact, I just lost 30 mins of my life listening to myself (ewww) in an old Update in Under 30 from 2013 that I recorded on this very topic.
[Sigh] I sounded so youthful…and…about 7 years younger too in terms of experience with this crafty calculation in the hundreds of labs I have encountered since!
My reliance on this ratio has remained but my wisdom regarding how to apply it has widened….and so, as I prepare to initiate another hundred or so practitioners into this secret sect 😉 via our current MasterCourse in Comprehensive Diagnostics, I couldn’t help myself and decided to re-record this UU30 episode: Using Urea & Creatinine as Markers of Protein Adequacy and also throw in a new pdf resource to boot [once again, ahem,apologies to my team!!] You see our ability to identify protein adequacy without this tool relies on the rather-rudimentary-‘rule’ that your protein requirements increase linearly with your weight…that’s the whole g/kg body weight thingo, right? But what if your weight gain is ‘all adipose’ Vs ‘mega muscle’ – are the protein requirements really the same for both people? Absolutely, not! This calculation enables us to step away from the rough approximation of the RDI and be able to determine if each individual is meeting their genuine requirements as driven by their own unique muscle mass hunger…oh and it reveals a few other very helpful things along the way to boot!
But this simple calculation comes with some caveats: 1. there are people and presentations in whom this calculation is not appropriate or accurate 2. because there are no magic numbers, right, it is about matching your labs with the patient in front of you and 3. looking (as always) for patterns.
…and a word of warning to the uninitiated: You’re going to love it!
So for those of you who are already Update in Under 30 Subscribers…happy Wednesday! Because you always benefit from any updated recordings etc. you’ll find this rejigged resource is already in your Active Content and for those of you who may have purchased this as an individual recording in the past, the same applies. And for anyone else keen to make some real meaning out of the most routine labs we see over and over again, and understand a whole world more about what they tell us about our patients’ muscle mass health, trajectory and the dietary protein piece of this puzzle…you might want to check this out too! And for those of you who think ‘total protein’ on a patient’s blood test results reflects ‘total protein’…boy have I got news for you!!
This comprehensive analysis of two standard indicators, urea and creatinine, that are often part of the patient’s standard blood chemistry tests. These commonly available results can provide insight into protein ingestion and uptake as well as muscle mass and, in extreme cases, kidney and liver function.
I don’t know about you but I don’t count myself among the conspiracy theorists. While I may have been partial to the occasional one over my lifetime, you have my word, I never inhaled. Or at least not since I learned the practise of scientific enquiry and the application of critical thinking to all evidence. The two together tend to put a dampener on the whole: earth is flat & the moon-landing was a hoax…kind of notions. But there is one conspiracy I think all of us in nutritional medicine have been the victim of: The Calcium Conspiracy.
Not in the vein of speculations regarding excessive lobbying & undue influence of the Dairy Corporation on dietary guidelines. Nor even arguments that this has gone so far as to inflate the RDIs for this nutrient. Nope, I am actually good with the RDIs for this mineral. High level evidence confirms that our intake of Calcium was enormous even before the Agricultural Revolution, and therefore BD (Before Dairy) 😂
Man, those roots and tubers and other bushfoods sure were nutrient dense, not like the stuff we consume these days!
No, the Calcium Conspiracy we’ve all been lead to believe is that it is the boss. The boss of bones. The boss of the parathyroid. The boss of the other minerals. And especially the boss of Magnesium. While you might have heard me describe Calcium as a ‘bully’ in the GIT (let’s call this the slide 😅) and I stand by that, it is far from being the boss of the rest of the playground! In fact its regulation is largely at the hands of other nutrients..not naming any names…[Magnesium😳] So while, all of us trained in nutrition have had the significance of the Calcium-Magnesium relationship & the mantra “2:1, 2:1, 2:1” drilled into us, which we repeat at night to get ourselves to sleep (or did they mean to take not just ‘talk’ these minerals, to help with sleep?!) Our teaching created this conspiracy – a misperception that Calcium is the boss and Magnesium its long-forgotten lackey. Well guess who’s really calling the shots and on whom?!
Have you ever heard the saying, ‘It can take Magnesium to fix a Calcium problem”? I’ve not just heard it but seen it many, many times in my patients.
But how do you tell which patients need both and which ones, just one? It comes down to understanding the exquisitely sophisticated way Magnesium lords it over Calcium – via the parathyroid and Vitamin D metabolism and how we can see this patently in the pathology (regular screening labs) of your clients. I think there is a bias in integrative nutrition – we favour Magnesium – it goes into our supplement recommendations for so many of our patients and while the rationale for this is valid – all dietary surveys show magnesium under-consumption to be rampant in the SAD – I don’t actually think all of us know 1) how much we should be giving (yes there is a limit) 2) how to discern who needs what, in spite of a lack of a good Magnesium assay and 3) the true potency in the prescription when we get these things right or wrong! This study by Sahota et al is so far my favourite for 2020..it’s 14 years old and the sample size is small but its methodology and examination of when Magnesium can fix a Calcium issue and when it can’t, is superb. Together with about 50 other papers I’ve just imbibed…they’ve refined my thinking, tremendously. There’s a Calcium Conspiracy, alright, but just throwing Magnesium at everyone in arbitrary doses is not the solution…. “2:1, 2:1, 2:1…..”😴
There’s a conspiracy going on regarding Calcium but it’s probably not the one you imagine. We have been lead to believe that Calcium is the boss: the boss of the bones, of the other minerals and certainly of its often over-looked lackey, Magnesium. But the truth is, we have it all the wrong way round. There is a sophisticated synergism between these two minerals but the brains and the brawn in this relationship are held by the latter and we need to understand how to recognise when Magnesium is ‘pulling the strings’, to produce low calcium, in our patients and how to find the sweet spot of their synergy. This recording comes with a great resource to use in your clinic, with explicit redefinition of ‘what healthy looks like’.
I used to all the time. Especially when I noticed the Niagara-falls-sized gap between the doses I was using compared with my mainstream medico mates. I thought, hang on, for a patient with a baseline blood level of 40nmol/L, they’re recommending <1000 IU per day, but I’m thinking 5000 IU…which one of us is wrong? Then again, we might both be right!
The sexily simple formula as cited byAussie researchersis: for every 1,000 IU of vitamin D a patient takes a day, their blood level is likely to rise approx. 17 nmol/L over 2 months, at which point it plateaus. So the medicos’ 1,000 IU supplement would bring our patient’s blood level up to 57 nmol/L which, as far as the medico might be concerned, is ‘job done’ 👍👏
My dose would be viewed as excessive but clearly I am aiming for a different set of goals (optimal rather than simple prevention of deficiency)…oh and I insist on follow up testing to know when we’ve made it!!
I encourage my patients to get their Vitamin D retested 2 months into treatment to confirm 1) they have responded and 2) their response is loosely within this predicted performance. And how many times is it not? Often. Which got me to readjust the formula I use to something more akin to: for every 10 nmol I want their blood levels to rise, I will need to increase their intake by a 1,000 IU. Now am I just making big sweeping inferences from empirical experiences of a few (hundred) patients without additional backing….well so what if I was...this is a branch of the EBM family tree! But no! I have also actually read enough studies clearly documenting the individualistic response to vitamin D, as a consequence of different adiposity levels, genes, magnesium status etc. to know that, while I am very grateful to have any kind of formula to start my thinking from…I treat individuals and goshdangit#@! they keep insisting on individualised medicine!
The whole practise of identifying a deficiency, ‘treating it’ and yet never following up with repeat labs to confirm that you actually have…BLOWS MY MIND🤯
That’s not EBM, let’s face it. Not even a distant demented cousin who has fallen from the dizzying heights of that family tree.
The one lesson I’ve learned, more than any other over 20 years in nutritional medicine, is that the more questions we ask and the more we challenge ‘established truths’, the more we uncover something much more personalised and potent about each and every nutrient …and now as the days continue to shorten into smaller and smaller slithers of sunlight between ‘bed-ends’, this is probably also a good time to ask ourselves…
Vitamin D deficiency has been associated with a long list of major health conditions: from autoimmunity to mental health & almost everything in between. This has lead to many of us recommending high dose vitamin D supplementation for a large proportion of our patients but do we understand everything we need to to be certain of the merits and safety of this? In this provocative episode Rachel outlines the key unresolved vitamin D dilemmas that should encourage us to exercise caution and outlines how adequate sun exposure is associated with improved health outcomes independent of the production & action of vitamin D.
You can purchase this UU30 episode individually here or become a subscriber and gain access to this and over 65+ episodes plus new monthly releases for 12 months here.
If you are already an Update in Under 30 Subscriber, you will have immediate access to this episode in the ‘active content’ of your online account.
🍌‘I think I am, B2! It’s time to separate the B12 from the B*S#!’
Ok, if you’re reading this and you’re not from around here you have reasonable grounds to conclude I’m the one who’s gone 🍌 but if you grew up with a show all about 2 adults dressed up as bananas and creatively known as B1 and B2, then we’re all good! Ok now for the next bit, you might need to sit down. Nothing not everything in the wildly popular, and dare I say it populist, doco The Game Changers was scientifically rigorous. I know, I’m loving the strike through a little too much today.
Goodness, when otherwise intelligent friends of mine forced me to watch this, they found the need for both restraints and duct tape over my mouth, to hear or see anything other than me jumping up and down, arms flapping, mouth yapping. People only tend to make this mistake with me once.
Among the many many dubious XXX was a terrible mis-truth about our ‘new modern reliance on animal food or supplements for B12’. Woah…back up there Game Changers Gang, say what?! Does anyone on their research team read any research? So that got me all motivated to go back to the books on our beloved B12, which is simply like no other micronutrient in human physiology or in nature, for many reasons…starting with 1) it contains a metal in the middle 2) it has dietary dopplegangers (plant forms that look just like it but actually are decoys that need to be actively removed from the body so as not to block its actions) and 3) has the most complex and sophisticated pathway for digestion and absorption, which surprising equates to brilliant average bioavailability (much better than most micronutrients)…until it doesn’t! And that’s when the trouble starts. Once you don’t have an intact IF absorption pathway, you’re down to picking up < 1% via simple diffusion, and suddenly we see why patients can be vulnerable to not meeting even the piddly required amount. Not to mention the vegans, of course.I’m on my best behaviour.
But the B*S#! about B12 is far from limited to the documentary. It’s in the words of the Methylation Mystics, making methylation sound like rocket science and in the supplements we’re being sold.
But don’t get me wrong…effective B12 treatment in the right patient is a total wow moment. I’ve literally seen all the lights go on⚡ in some . So what do we need to do to find our way out of the dark? Go back to the solid science. Come on. There’s nothing else you need to do and nowhere else you need to be… we all know it…so start by reading this and this. There’s plenty more of course but these are excellent appetisers. And if you want to cut to the chase and get the lowdown on what’s B*S#! versus what’s the real magic of B12, you can always settle in and listen to my latest Update in Under 30 – complete with a very cool clinical tool to help you choose the best B12 for each individual, but spoiler alert, it ain’t rocket science.🤫
B12 is a routinely under-rated and recognised micronutrient, which is in fact in high demand by many of our patients. As nutritional research pushes back against defining adequacy as simply the prevention of the deficiency-associated disease (macrocyctic anaemia, irreversible neurological damage) we enter a new landscape of more individualised approaches where we’re better able to recognise and treat those at risk of falling below ‘optimal’. But how do we accurately identify this and then choose the ‘best’ B12 (methyl- cyano- adenosyl- hyroxo-) supplement? Does it need to be this complex? Time to sort the B12 from the B*S#!! This recording comes with a bunch of great resources including a very handy clinical tool
The latest Update in Under 30 has landed!!!
You can purchase April’s episode, Separating the B12 from the B*S#! is here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
Me neither. I value transparency in all things impacting my health. So when the ‘Colonel’ tells us the magic is in not knowing…I think….hmmmmmmm, no thanks!
Similarly, when the provider of a test tells us, ‘We’d like to give you independent scientific support for our markers and our method but we just can’t because it’s patented!’…well that’s as good as the so-called ‘Colonel’ and his mysterious unidentified herbs and spices, as far as I’m concerned.
It’s effectively like they have created for themselves a ‘Get out of jail free card’ but unlike in Monopoly, they can play it over and over again. Trouble is, as the referring or just ‘reading’ practitioner (many of my patients present with results of these tests in hand) you have to practice either utter blind faith and believe every word that report tells you or you feel like you have to disregard the entire thing because you don’t have the time to sift through every parameter, searching out any independent scientific discussion of their markers, to distinguish fact from fiction. Utterly exasperating. Because of course, a test that offers a huge panel of results may consist of both – some of high value, some utter nonsense and some somewhere in between.
There’s one 24hr urine test from an OS company that I tend to see increasingly and it purports to be able to assess just about everything from gut health, to neurotransmitter levels, to your antioxidant capacity, mitochondrial health and beyond! How is this even possible in one 24 hr non-preserved urine sample that goes off-shore to be analysed? Well they can’t say…it’s a secret. 🤐 Pu-lease!
To boot all the lights and sirens are on for this patient who appears to have such little vitamin C in their urine, they’re at risk of scurvy! That is except for the fact that Vitamin C readily oxidises in urine only to turn into….wait for it….Oxalic acid! So, anyone surprised to hear she is also reported to have an exceptionally high oxalate load?!
Secret herbs and spices? No thanks, I’d prefer science. As the saying goes, “Keep an open mind but not so open your brain falls out!” Sorry but tough-talkin’ Tuesday is back and it’s gotten all toothy!
Update in Under 30: Oxalate Overload – Assessment and Management
Oxalates are present in many healthy foods and in all healthy people, but when ‘normal’ levels are exceeded they can spell trouble in a whole raft of different ways due to their extensive distribution across the body. Some tissues, however, have more problems than others, especially the urinary system and soft tissue and joints but now there are also questions about oxalates’ relationship with thyroid and breast issues. We review the latest evidence about the health consequences, blow the lid on accurate assessment for oxalate excess and talk management in this jam-packed update.




 Well that got tongues talking! We’ve cried, and we’ve laughed, hearing from practitioners about their ‘over-delivering donkey experiences’ for 2020. We’ve heard many memorable & relatable tales of either failures to set the best boundaries or even, in instances when we do, patients’ incredible dexterity to scale these in single leaps, ala James Bond style.
Well that got tongues talking! We’ve cried, and we’ve laughed, hearing from practitioners about their ‘over-delivering donkey experiences’ for 2020. We’ve heard many memorable & relatable tales of either failures to set the best boundaries or even, in instances when we do, patients’ incredible dexterity to scale these in single leaps, ala James Bond style.