Wow, menopause is really having a moment, isn’t it? Or is that just me (and my mates who are all somewhere on that perimenopausal path)?! But seriously, medical perception of this reproductive transition is undergoing a revolution right now—widening the lens to take in more diverse potential presentations and lengthening the period of impact recognised both ‘before, during, and after’ that last, last…no hang on…last period. But I fear we are at a crucial crossroads. Anything could be related to (peri)menopause, but not everything is or should be.
There are several other conditions whose onset tends to rise or peak at the same age and stage for women, and due to their shared features, they get missed & misdiagnosed, misattributed to that!(more…)
Ever feel like the universe has been preparing you just for this moment? Me neither really…but in this one weird way – yes!
So hear me out.
Thyroid disease as a result of a viral infection was first described in 1902 by Dr Fritz De Quervain and of course he and his ego called it De Quervain’s subacute thyroiditis. For some historical context, this predates the recognised role of iodine deficiency in thyroid disease! Skip ahead almost a century to deep in the 1990s and mini-me was sitting in a uni lecture room [front row & wearing fluro of course🤣] and over hundreds of hours (no scrap that zillions*^# of hours) of lecture content I was exposed to, the description of De Quervain’s Subacute Thyroiditis stood out and stayed stuck to me. I’ve brought it out for a twirl from time to time in the interim with some of my patients & in particular in correspondence with their docs.Skip ahead to the 2020s when we had this thing called. ‘a global pandemic’, and now everyone wants to talk viruses and their broader health implications & as a result, good ol’ Fritz, me and our buddy, De Quervain’s subacute thyroiditis, are all having a moment.
But just to recap – this is (clearly) not new.
What is new is the way this ‘virus of the moment’ has brought this Thyroid V Virus battle to the forefront. We are living an important chapter in history where all the textbook entries on De Quervain’s Subacute Thyroiditis are madly being rewritten to reflect the veracity of this viral attack on the gland and the wide-scale & varied damage that ensues over the months and years that follow. And so many of our patients are the walking embodiment of it – whether that be in the form of low or high thyroid hormones, nefarious changes to gland anatomy only evidenced on US. So what do we need to know? in short, that pathogens as goitrogens have never been more of an issue than right now for ourselves and our patients. And that compared with just our usual desire for comprehensive investigation of the HPT, taking a complete look ‘under the hood’, not only by way of a full TFT and Ab titres but also, wherever there is an additional suspicion – by way of a thyroid US – has become non-negotiable. But regardless of what you find there, once you look, do you know what to do next?
Biopsies and autopsies of diseased thyroid glands alike reveal the prevalence of many common viruses within, setting the scene perfectly for the Thyroid V Virus battle. So, what happens when a virus takes a specific liking to this gland? While there are several different possibilities, one brought to the forefront in recent years is viral thyroiditis wherein stage 1 is ‘spill’, stage 2 constitutes a gland that is now ’empty’ and while stage 3 is reported to be ‘recovery’, this is increasingly scarce – replaced with chronic or recurrent thyroiditis, relapses of previously remitted GD and a doubling of new AITD diagnoses – not to mention the wide variety of unfavourable anatomical changes being found on ultrasound. Comes with a great desktop reference with prescription examples.
You can purchase ThyVIRoidhere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account. You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
The builder responsible for my reno arrived one day with a frown. When I asked him what was wrong – he said he’d just had his second high PSA result and now the doctor wants him to see a specialist. It was apparent that he felt this was a real cause for concern. Talk about raising a red flag to a bull 🚩🐂 Yes, of course you know what followed. I insisted on reviewing the results myself only to find the reference range provided on his report was not specific to his age – and if we adjusted up for this (as the science supports) his result is just 0.5 ng/mL above the expected value!
Now, remember he is a builder so, ‘0.5’ in his mind might well be on par with 5mm which apparently is a big deal…or so he keeps telling me every time I try asking for some weird unconventional thing for my roof, windows, walls, whatever!! So I still had to provide a little bit more detail for him to get perspective and to understand the true meaning (and lack of scary meaning) of his results.
This however is just a micro-illustration of a big problem in pathology – we all risk a lack of perspective but if we can get it back, aids us to see that seemingly ‘normal’ results are sometimes a concern, and so-called ‘concerning’ ones, non-significant. The incredible patient insights that can be gained from being able to measure & monitor actual quantities of things in our patients; nutrients to novel disease markers, precursors to end-products, all comes down to understanding how their values compare with…with what? With someone of a different sex and age? With ‘all adults 18-108!’? With any other pre-menopausal woman regardless of reproductive or cycle stage? With ‘the average’ adult given that this current definition is overweight & unwell? Who are we comparing ourselves and our patients to?
When I undertook my undergraduate training many moons ago – there was no education in blood test interpretation. But as soon as I got out into practice I found my patients had all these bits of paper filled with magic numbers that I felt certain might offer me insights and a deeper understanding of their whole health – and how to best help them.
I desperately wanted to decipher this foreign language and made it my mission to do so. I was lucky enough to meet and be paired with a kindred spirit, Dr Tini Gruner, who happened to be my supervisor when I returned to undertake my honours thesis. Together we pooled our knowledge, sought out & shared with each other yet more and found that, together with comprehensive case taking, it provided excellent scaffolding to our work-up of patient cases. Better than that, it created this baseline for patients, identified clear treatment objectives and we could measure the success of our interventions based on how their results did (or didn’t) respond to our interventions. It was (and still is) a totally thrilling way to practice.
We talk about there being both an art & science to medicine generally and certainly an integrative approach. Without the benefit of pathology interpretation, I felt too at sea at times, without quite enough of the science to check the accuracy of the ‘art’ and my speculation.
Being able to understand what each individual result represents and reflects, to know how to form meaningful comparisons – with external reference ranges that speak to healthy individuals of the same sex & life stage, derived from rigorous research – and also form a comparison with the patient themselves, to pick up on the most subtle and significant early alerts to an emerging pathophysiological or healing process – is the skill, I believe, we all need in health to complete the toolkit. That’s why I made it my mission to learn the language of labs, from a conventional & integrative interpretative perspective, and then to share this learning with everyone wanting and willing to take this baton from me (& Tini) and run with it 🏃♀️🏃
MasterCourse I: Comprehensive Diagnostics. Click here to read more and here to purchase it.
*Please note that this is the place to start for everyone wanting to add preventive diagnostics to their tool kit. It is also the pre-requisite for MasterCourse II, so make sure you have completed this before continuing with MasterCourse II: Thyroid and Adrenal Diagnostics.
MasterCourse II: Thyroid & Adrenal Diagnostics. Clickhereto read more and here to purchase it and sign up for the Free Watch Party commencing tomorrow, 3rd August 2023 with is included with each purchase of the MasterCourse II.
Rachel: And sometimes emails from practitioners provide me with both the question and their own answer to their question even!
Cameron Barker’s (Ex-student long-term learner & mentee)email arrives titled:Unexpected Source of Iodine in Placenta Caps?!
A 32 yo female with a 12-week-old daughter came to me as she was not feeling well, in particular, she reports fatigue, racing heartbeat, anxiety and loss of appetite. Previously, 2 years ago, I had helped her with her Hashimoto’s. I did not hear from her for a year or so and she fell pregnant and was recommended to take a well-known iodine-containing pregnancy multi.
Just as optimal integration of lab results into our patient work-ups makes ‘the invisible visible’ we thought we might make visible some of the everyday Q & A that we engage in with wonderful practitioners who are fast becoming Diagnostic Divas & Divos.
Praccie email arrives with subject header ‘Graves Help’ (or is that ‘Graves…HELP!’🤔)
Practitioner: I have a Grave’s patient who required Propylthiouracil (PTU) for a few months from late 2022 until Jan 2023 which obviously took her thyroid in the opposite direction (see labs). Following a miscarriage last year, she has conceived and is around 6/40 and her current TSH result has come in at 3.3mIU/L, her TPO Abs > 1000 and she also has low-level Tg Abs (TRAbs not measured this time) and this is what she just said to me:
“I just had my specialist session this morning – and she has put me on thyroxine (50mcg) as my thyroid is quite low. I also asked her about the prenatal vitamin and she said it was safe for me to be on iodine at this time, as the Graves isn’t present and baby needs it for the development of its own thyroid.”
Oh gawd! Preg? Iodine? Graves? Antibodies? Antenatal or postnatal aggravation?!
Is there an UU30 I can listen to to help me understand this?… sorry for the panicked email…
If I wrote down these 2 elements on a MindMap: Thyroid dysfunction and Adiposity, how would you connect them? Would you reflexively draw an arrow from the former to the latter to flag that the thyroid underpins the weight management issues? My arrow would be the other way around.
According to every scrap of data, the likelihood that someone’s subclinical or even frank hypothyroidism is the source of the excess weight is quite low, while the probability that their excess adiposity has had profound effects on both the anatomy of the gland and the physiology of the HPT is much higher.
And the change in the direction of this relationship – adiposity as the cause not the consequence – changes everything, from what we tell our patients, to what effective management, and success, in terms of follow-up TFT patterns, actually looks like. It’s far from semantics. Because while we may not encounter any cassava excesses in our practice, an established goitrogen with a long history, we do see unhealthy adiposity often and it is the ‘newest’ goitrogen on the block, so to speak.
The definition of a goitrogen is something that interferes with thyroid hormonogenesis and thyroid function in any way.
Abdominal adiposity, that is excessive for that individual, (I don’t believe this can be simply determined by BMI alone but requires us to apply a more sophisticated lens & metric) interferes in many many ways.
Aligned with this recognition is the seismic shift in understanding that we’ve undergone regarding ‘who or what’ is the boss of the thyroid. Hypothalamus & pituitary, I hear you say? Nope. These guys are just the middle managers – and the real bosses are a board of directors that includes adipose tissue. Stop and think about this – makes sense, right? The HPT is attributed with being the major endocrine axis that determines how much ‘energy’ we have to spend – so of course it’s taking direct messaging and direction from the adipocytes! Add to this, that excess energy consumption drives up TSH, a trophic agent for the gland – a stimulator of proliferation without differentiation and with no guarantee of an adequate supply of the greater requirements for micronutrients required to ‘grow a bigger gland’ without architectural or functional disturbance. These are just the 1st two stages of goitrogenic effect resulting from over-nutrition, that I refer to as The Over-Feed and The Under-Resourced Thyroid…
But what can follow are 2 more stages: ‘The Disturbed’ and finally, ‘The Diseased’ thyroid – which include pathophysiological processes such as adipocyte infiltration of the actual gland (akin to the liver infiltration in NAFLD) seronegative thyroiditis, as well as epigenetic changes impairing DNA correction etc etc all a consequence of weight gain…not the cause.
Thyroid dysfunction –> weight gain or Weight gain –> thyroid dysfunction…Time to rethink this relationship?
According to every scrap of research, the likelihood that someone’s subclinical or even frank hypothyroidism is the source of their excess weight is quite low, while the probability that their excess weight has had profound effects on both the anatomy of the gland and the physiology of the HPT is much higher. So rather than a reflexive assumption that someone who presents with weight gain or ongoing unhealthy weight should have their thyroid checked to see if that is the cause – the TFTs absolutely should be performed but instead to understand one of the key consequences of this excess adiposity. In this recording we highlight the 4 stages of impact, moving from: the ‘Overfed’ to the ‘Under-Resourced’, the ‘Disturbed’ and finally the ‘Diseased Thyroid’. The reversal of this relationship – adiposity as the cause not the consequence of thyroid dysfunction – changes everything, from what we tell our patients, to what effective management, and success, in terms of follow-up TFT patterns, actually looks like. We need to be alert and responsive to the most common and contemporary thyroid disruptor in our patients: fat is a goitrogen.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account. You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
Gone are the days, thankfully, when we could all easily identify any individual taking an antipsychotic 1) because they were the marginalised ‘mad’ and 2) stigma and shame were rife. With the seismic shift that has occurred both in psychiatry & society we now know so many of the people we live or work with just might be taking ‘something’ & under any number of diagnostic labels. And increasingly the ‘anti-psychotics’ are not reserved for the psychotic nor the ‘mood stabilisers’ for the manic. Which can complicate things – especially when it comes to their thyroid.
You see it’s a mistake to think that only Lithium spells trouble for thyroid function
The latest piece of evidence from a study of over 25K BPAD patients in the US tells us this common misunderstanding makes us prone to not recognise all the other patients in whom their psych meds are disrupting and in fact driving thyroid (dys)function. Though Lithium carbonate remains the most noxious goitrogen due to its multiple disruptive mechanisms – the rest of a large group of Psych meds (yes even antidepressants!) are impacting to the point of effecting the thyroid function test results you are likely to see in patients taking these. And this is something we need to be alert to – these medications are essential, non-negotiable in most scenarios, but a secondary hypothyroidism is not their intended goal and can make matters worse.
Cue our growing understand of psychoneuroendocrinology, of course. Your HPT is influenced by your mood & vice versa
I told you I’ve rekindled my love and passion for thyroid pathology and this is one of the many elements I got to include in our latest updated training * Advanced Thyroid Assessment* and the upcoming MasterCourse. But I just had to hit record on this one aspect immediately – because if we don’t recognise the cause we are likely to be throwing all the wrong things at the thyroid – to no avail. This kind of subclinical or overt hypothyroidism is not due to nutrition per se, or due to some other kind of HPT re-setting influence like inflammation…it’s the meds & that necessitates different solutions & a much bigger conversation…so join me…
Many of us recognise the bidirectionality between thyroid function and psychiatry wherein ‘stress’ and mental illness can produce a predictable pattern and shift in TFTs and vice versa but regarding the question of psych meds as potential goitrogens, many of us are mistaken in thinking this issue begins and ends with the use of Lithium carbonate. As it turns out, an increasing number of these pharmaceuticals are recognised to disrupt thyroid health & activity via a variety of mechanisms both centrally and peripherally & as a result many patients may get stuck in a vicious loop of worsening thyroid function and mental wellbeing. – until someone calls it – someone like us.
How much? How often? When is the best time & timing? do you know about friends, foes and frenemies? Which form, when? e.g. building blocks or bioactives? And for how long? aka are we there yet…?
These are the kind of questions that one would imagine nutritional prescribers can always answer – but can you? Yet this is the goal, right? So that with each and every unique individual who needs supplements – we have a clear, consistent go-to framework to guide & direct these prescriptions. One that makes scientific sense, offers optimal outcomes and removes the uncertainty.
From my interactions with thousands of practitioners, however, I know many of these key questions plague practitioners & they feel, at times, as if they’re flying without a net, or without a strong systematic approach, or at the very least without all the answers to these questions.
I’ve had so much good fortune & so many others to thank for providing me with this foundation. Fay Paxton – my nutrition lecturer in my under-grad who indoctrinated me with a systematic approach. Dr. Tini Gruner – my principal supervisor at SCU, who shared & further fuelled my passion for biochemistry and reading labs to extract insights into each individual. And thanks also to all the pharmacists I’ve delivered education to over the years, who, as a result of their grounding in the principles of pharmacokinetics, always ask the best questions – questions that if I don’t know the answer I know I need to know the answer! So I made it my mission to find out!
While we dip into these aspects of nutritional prescribing in our regular mentoring groups on an ‘as needs’ basis, I’ve decided the time has come to create a year-long program dedicated to sharing this information and building this skill-set in practitioners.
This monthly meet-up is delivered live (max 1.5hr) and runs from Feb to November with the following currently proposed format *subject to change dependent upon the needs of the group
Feb Factors Affecting: digestion, absorption (host, form, dose)
March What happens to what gets left behind? e.g. enhanced enterocyte micronutrient concentrations & their effects plus unabsorbed nutrients & their interactions with the colonic environment
April What happens to what’s absorbed e.g. distribution, hierarchy of needs, activation and deactivation
May The pharmacokinetics of prescribing
June Where do our ideas on dosing come from? e.g. Physiological Vs Pharmacological dosing & actions. The basis & believability of maximal intake boundaries?
July Bioefficacy V Bioequivalence. Beyond building block nutrients: Is ‘Bio’ (-active, -peptides, -materials) always better? e.g. GABA Vs Glycine, NAC Vs GSH, PLP Vs Pyridoxine, Niacin Vs Niacinamide riboside ——————————————————————Aug month off—————————————————————————
Sept How often & for how long? Are we there yet? And how would we know? Plus Fast Vs Slow Nutritional therapeutics
Oct Strategies for Supplement Success e.g. friends, foes and frenemies in nutrition underpinning principles with examples; compliance changers for clients
Nov Live attendance & opportunity to participate in a case-based mentoring session
This monthly ‘live’ meet up will be delivered as part of 2023 Group Mentoring as The Nutritional Prescribing Program Group Mentoring applications open 17 October 2022.
To join the waiting list and be notified when applications are open, email the team at [email protected]
Find out more about what groups are available for Group Mentoring in 2023 here.
Have you been told somewhere by someone that the ‘perfect’ TSH is 1.5 mIU/L? This is a wonderful, terrible & wonderfully terrible example of ‘magical numbers medicine’. As a push-back against the published reference ranges we’re given, that are so wide you could drive a truck through them, there has been an over-correction by some, leading to the myth of ‘magic numbers’. We can narrow the reference range substantially for many parameters with good rationale, make no mistake about that but once we start setting ‘aspirational goals’ that are explicitly rigid…well we’ve done 2 things 1) forgotten about the patient to whom this result belongs and 2) disregarded viewing each result as part of a ‘pattern’, that we must piece together and make sense of.
Back to TSH then… if my obese patient had a value of 1.5 mIU/L this in fact would be woefully inadequate – so too a child at any weight.
And we expect a higher value as well in our elderly clients too and this level there may be, in fact, increased mortality.
But the same result would be excessively & worringly high in my patient who’s undergone thyroidectomy.
Realising the full value of any test result in terms of what it reveals about the person sitting in front of you, requires these more thinking and more thoughtfulness. Unfortunately, a list of ‘magic numbers’ will often lead you astray. And building your scientific knowledge about labs will not only help you avoid the pitfalls of pathology but will strengthen your pathophysiology prowess in surprising ways, saving your patients a packet in terms of additional extraneous testing and help you truly personalise your prescriptions…because the ‘invisible (biochemical individuality, oxidative stress, genetic probabilities, subclinical states, imbalanced or burdened processes etc) just became visible’. I started requesting lab results early in my career and years later was lucky enough to be taken under the wing of Dr. Tini Gruner. I found some of our shared notes, from 10 years ago, scribbled all over patient results recently and I was struck by just how lucky I was to have her encouragement to really pursue my interest and how she was a guiding force about learning to recognise pathology patterns over single parameters. A decade on I can concede, much of my clinical and educative success has come off the back of this foundational skill-set and I know, this is true for so many I’ve taught too.
“The guidance I’ve received over the years from Rachel in relation to pathology interpretation has been one of the most valuable (and fascinating) investments I’ve made as a clinician. Her teachings have filled gaps in my knowledge base I never knew needed filling and have significantly enhanced my understanding of the inner workings of the body! Rachel has an incredible ability to make the numbers that patient’s so often present us with, both understandable and clinically meaningful. The knowledge I’ve gained by investing in this skillset has paid off in dividends and I’m certain will continue to do so into the future.”
Stacey Curcio – Cultivating Wellness
I hope you’ll join me for the most exciting up-skilling opportunity in learning labs yet. Oh…and all this talk about thyroid testing..this next MasterCourse series is focused on revolutionising your understanding of thyroid, adrenal, HPT & HPA markers based on the very latest research & findings & marry these together with everything you learned in MasterCourse I (ELFTs, FBE, Lipids & Glucose) to understand the ‘whole story’.
…an absolute treasure trove of free integrative health information about your patient!
DEEP DIVE INTO REAL CASE STUDIES TO DEMONSTRATE EACH PATHOLOGY PATTERN IN ACTION. ]\
There are limited places. To sign up for Rachel’s LIVE Series – MasterCourse II: Thyroid & Adrenal Diagnostics and for more information click here.
I’ve spent the best part of about 4 months recording my *NEW* Advanced Thyroid Assessment training. I told my team this would be easy and quick, given it was to be based on a great little 2-part, 2hr updated presentation I delivered just last year for ACNEM!! Sixteen weeks (like seriously…most of it) numerous rewrites and retakes later, our final product is 4 parts that goes for over 12hrs in total & has a bonus Adrenal recording! And yeah my team are impressed but unimpressed too if you know what I mean?!🙄🤪
Every time another, ‘Oh wow!’, or ‘No way!’, escaped my lips, it was a source of personal celebration, as another deeper layer of learning revealed itself.
But to the wonderful, somewhat weary and definitely wary Sally, who does all my powerpoints, it was met with, ‘Oh boy!’, because it meant many multiple new slides to build full of visual metaphors, animation acrobatics, if not an entire new Part!*#@^
Her sage advice along the infinite research road I’ve been travelling was : ‘Stop. You’re going to have to stop.’
So I didbut now I am this meme. Everything I see currently through the lens of thyroid health, I talk in tongues TFTs and my brain is one giant neural network of integrative endocrinological circuits! I have fallen in love with this topic, this neuroendocrine axis and its ‘first responder’ role all over again! Hence our little thyroid character below – all ‘antennaed’ up – is one of the many tools we’ve developed for this training, to teach us that ‘bad thyroids’ per se are extremely rare – but bad scenarios are common (too much or too little of any macronutrient, key micronutrients, a change in the internal or external environment etc etc) and this little fellow and his board of directors (no – not the hypothalamus or pituitary!) – well it’s their job to ‘read the room’, right?!
In the absence of this key understanding we risk: A lot of lazy labelling in thyroid health – ‘You have a bad thyroid – that’s why you…[can’t lose weight, feel tired, have SIBO etc]’ Misdirected treatment & especially a tendency to overload the butterfly with ‘thyroid’ nutrients – which can do more harm than good
I’ve said many times, ‘perfect number pathology is a myth’ but it runs rife in practitioners’ beliefs about TFT results with complete disregard of the person those labs belong too! Did you know, for example, that your TFTs should all be higher if your BMI is? That your T4:T3 ratio should never be 3:1 if you are on replacement, have hot nodules, are pregnant or are acutely unwell etc etc etc? How about how low your Selenium or Iron levels need to be before this factor will influence the actual levels of thyroid hormones measurable – & what the impact of these deficiencies are well before then that is far more sinister and serious? Yep…you see here I am, pouring just some of the tiny take-homes of Advanced Thyroid Assessment ALL over you!
Watch this space my new Thyroid training is just around the corner!
An increasing number of our patients have thyroid concerns but unbeknown to many of us the most likely explanation of all is thyroid nodules, whose incidence is on the rise globally. The development of nodules has always been primarily viewed as a nutritional disease. Traditionally attributed to chronic iodine deficiency but recently novel nutritional causes have emerged. Benign nodules come in 2 flavours: hot and cold and while patients can present with a mixture, it is the presence or absence of a hot nodule that radically changes what complementary medicines you can and can’t use and what an effective treatment plan looks like. The pointers, as is often the case, are there for us in the patient’s presentation and pathology, so knowing the difference is no longer a guessing game. This UU30 comes with a great visual clinical resource and includes key papers on the nutritional management of nodules.
Over years of delivering independent education in integrative health I have spoken to some diverse audiences. This has included health professionals from very different backgrounds: from hospital-based psychiatrists & mental health nurses, to whom I presented on site in hospitals both in Australia & NZ, to a national sparkle-arkle speaking tour, in front of large groups of aesthetic practitioners. They’re the doctors & nurses for whom botox and fillers are their tools of trade, and yes I got to see actual demonstrations of their work performed live!!!😶 More recently, I’ve had several opportunities to deliver evidence-based independent education on nutrition to pharmacists en masse – which I always enjoy because they ask some of the best questions!
Underpinning each decision to accept an invitation from a 3rd party, be that a company an organisation or an institution, to speak, is: 1.The realisation of an opportunity for nutritional medicine to reach more people, a wider audience, & ultimately expand the circle of influence amongst health professionals, who interact with & advise the public at all different levels 2. An agreement and/or contract that ensures my independence, the correct use of my materials, image, brand and IP & removes any expectation to promote their products/services etc
And my ‘door’ is open to any invitation which meets these 2 criteria. So you might have seen my name, previously associated with some brands or organisations, in the last few years disappear off their speaker announcements, or no longer connected, and in turn you might see my name pop up in new places! Like….Metagenics Congress on Autoimmune Disease!! After many invitations from this company, that I wasn’t able to previously accept, I am pleased to be speaking at this face to face event on the Gold Coast in August. What a novelty, hey? Face to face?! My talk is about the 4 Mistakes not to Make in Hashimoto’s and as always, I’ve completed a full mini-literature review in order to speak to the very latest on diagnostics and nutritional management, in this condition. Yes, to quote a Costanza, “We’re back baby, we’re back!” And to see my full current smorgasbord of speaking commitments & all the people I am ‘spreading the (nutritional) word’ to – just click here.
This previous training will take your understanding of the interplay between food, nutrition, environment and the thyroid several steps further. With more supportive research and a greater focus on the mechanisms behind the relationships between these macro- & micro nutrient & environmental factors, this presentation is for the true thyroid die-hard.
We love hearing from our fellow fearless friends on the frontline – working with lab results & pathology providers – everyday. We recently received an SOS! from the Francesca Naish over yet another iodine assessment issue that you may need to also be alert to:
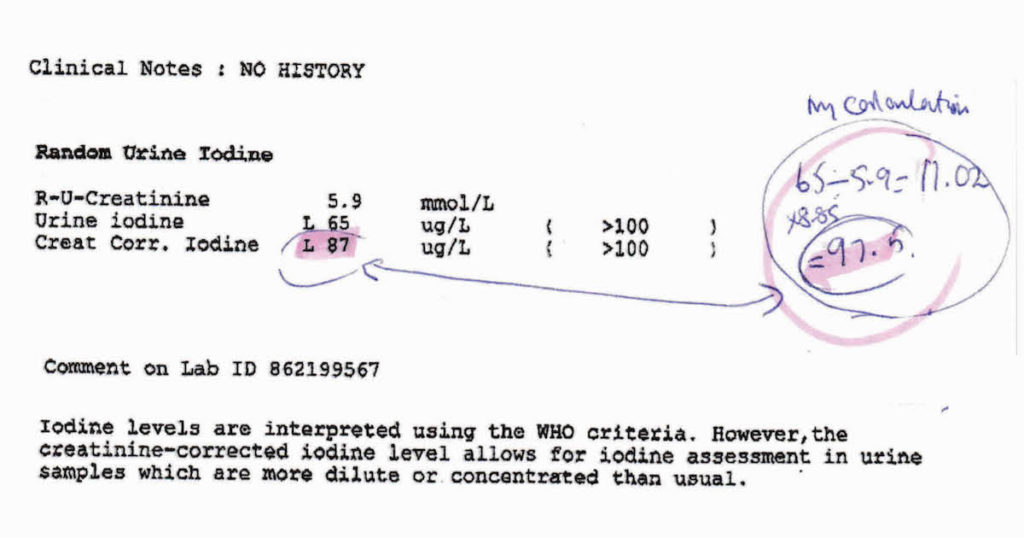
“Ever since you first drew our attention to the need to correct urinary iodine results, I have used your formula for all my patients’ results. Thank you for this. As most GPs don’t seem to be aware of the need to do this, I find it essential to warn my patients to wait for my interpretation before acting on their doctor’s advice! For a while now, Laverty have started giving the corrected result, which complies with the calculation you recommended. However, very recently Douglass Hanly Moir have started to give a corrected result on their result sheets, but it does not tally with the calculation I have been using (the one you recommended) and generally gives a lower figure.”
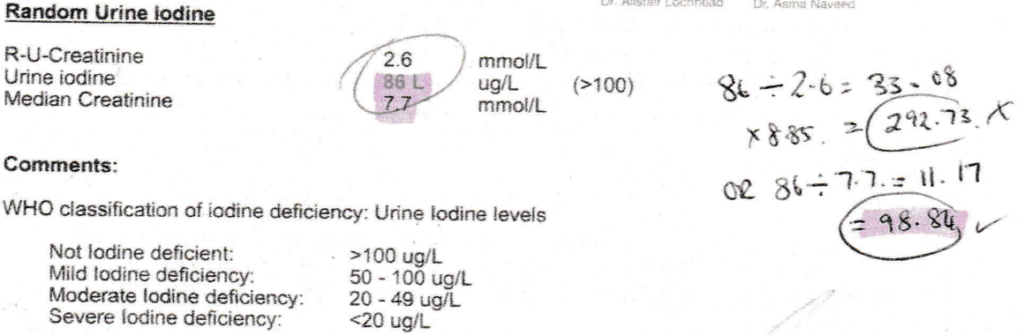
Well, as always, cluey people ask cluey questions…and this did take some back & forth with DHM to solve. Increasingly, all the major pathology companies are coming around to the essentiality of urinary iodine correction, something I’ve been banging the drum 🥁 about now for….yikes…7 years..no wonder I’m going grey! This is a mathematical formula applied to any raw score for urinary iodine to account for the dilution/concentration of the given sample, because, as we all know, hydration status varies widely between individuals and even within an individual at different times – and this is something that can wildly lead you astray in your thoughts about their iodine status, if not accounted for. Some companies are now employing the formula we use: Iodine (mcg) ÷ Creatinine (mmol) X 8.85 = Corrected Iodine in mcg/gCr which is wonderful to see. But DHM have taken a different path, strangely enough, using this formula BUT rather than using the patient’s own reported urinary creatinine they instead use a ‘median creatinine’
Which…I am going to say it… MAKES NO SENSE!^%@* aka we WILL correct this iodine for hydration status – but we’ll correct it for someone else’s no yours! – Ms/Mr average…ok? Ahhhh no. Just look at the difference this makes in a patient with very dilute urine, in example number 2 above!!
So Francesca & all of you on the frontline, can be assured, if you’re using the formula above – it is correct – keep up the great work and know that it is often better to do something yourself than blindly trust a 3rd party when it comes to pathology…unless that 3rd party is our RAN Patient Pathology Manager template which calculates this perfectly of course!
Increasingly our patients are coming armed with lab results and this cumulative data helps us to clearly see their ‘norms’ (as opposed to textbook ones) and therefore be alert to any changes. However, results from different labs at different times, and even the same lab, are unlikely to be presented side by side for easy comparison. They certainly don’t come with all the important information about what was happening for that patient at each time point – important details pertaining to the blood collection itself (fasting, inflamed etc) which can profoundly alter results or the broader context: menstruating, breastfeeding, losing weight, on meds and supplements.
The Patient Pathology Manager retains all the results for you, including the critical contextual elements, helping you to keep more accurate records to make the most correct interpretation. It also assists you to monitor changes related to various interventions.
Previously, the RAN Patient Pathology Manager has only ever been available to clinicians who participate in Group Mentoring but due to frequent requests for access, we thought it was time to share this great tool for those wanting a foot up with some better systems in their practice.
This provides you with a template that can be used an infinite number of times plus a short training tutorial.
‘Hey Alexa, What’s that formula for correcting urinary iodine for hydration status?’ Oh yes, if only she could answer these kind of questions!
There’s no one here by that name but we get these kind of emails all the time [Oh and also for Freya who hasn’t worked here in like 5 years!!😂] But we love them because it means our blogs provide useful, sought after and (we like to think!) really really hard to get anywhere else answers . But hey try it, Ask Siri! We’re always forthcoming with references – not just citations but the full low down and dirty full texts (as long as we’ve managed to get our hands on it!!) and we know which topics particularly hit a spot across our professional group by not just the number of enquiries but how far the actual blog they’re referring to, dates back. So we’ve just received more comms regarding one that’s often on high rotation…a post I wrote on urinary Iodine Assessment & how and why we should adjust for hydration! That was 2014…what a vintage 🤩 Show’s though how topical and tricky this little test is.
The iodine landscape has undergone radical change recently. We’ve moved from recognising the resurfacing of a widespread deficiency, to large-scale food fortification that has failed to correct deficiency in most and produced excesses in a few. Parallel to this, we have the ever growing incidence of thyroid disorders and some radically contrasting ideas regarding iodine’s role in both aetiology and treatment. Micrograms V milligrams? Random urinary iodine or iodine loading test? Important new evidence and clinical experience helps us understand more about how to accurately assess patients’ need for iodine and know when & how to use it therapeutically & when not to!
What’s the most common thyroid disease you’re seeing in practice? Nope, try again. I’m serious. There would be very few of us who’d get this right without cheating. It’s nodules. Current figures suggest 1/2 of all us middle-agers have them and by the time we’re 80 that’s risen to 90%! There’s a school of thought that says these figures have jumped purely because of increased rates of thyroid imaging and we should stop sticking our nose in places it doesn’t belong. Just because they are there doesn’t mean we need to know about them or that they are causing trouble. All this is true and yet there is a percentage of patients for whom these nodules are a whole lot of trouble, in fact, that’s why they’re coming to see you…they (& possibly you!) just don’t know it yet.
Nodules, outside of radiation exposure, have always been primarily viewed as a nutritional deficiency disease: Iodine. While this was always a bit one-dimensional (poor selenium…when will you ever get your due?) it’s an explanation that no longer fits as well as it once did because even in populations who have addressed iodine deficiency, the incidence of nodules continues to rise.
So, what now?
New nutritional drivers have been identified but rather than being about our deficiencies they speak to our nutritional excesses. And while iodine is not totally out of a job here, some people of course are still experiencing long-term suboptimal iodine which can trigger nodule development, we now need to question if there is any therapeutic role for iodine once the nodules are established. Well the answer is both ‘yes, maybe’ and ‘absolutely not’. The determinant being whether we’re dealing with Hot or Cold. Unfortunately most patients and therefore their practitioners can’t tell the difference. But it is the presence or absence of a hot nodule that radically changes what complementary medicines you can and can’t use and what an effective treatment plan looks like.
I’ve seen a lot of thyroid nodule cases pop up in mentoring this year and it’s been a great learning opportunity for everyone to get comfortable with clues in both patients’ presentation & their pathology. While iodine deficiency no longer ‘fits’ like it did, nutritional medicine should arguably remain the primary approach to their management and the new research gives even more credence to this and identifies a far greater range of dietary and supplemental tools.
Thyroid nodules are going to explain a surprising number of our subclinical (hypo and hyper) thyroid patients and we already have a dispensary full of powerful interventions but we need to start by familiarising ourselves with their story: their why (they happen), their what (this means for patients) and their how (on earth are we going to address these effectively) Knowing your Hot from your Cold…is step one.
An increasing number of our patients have thyroid concerns but unbeknown to many of us the most likely explanation of all is thyroid nodules, whose incidence is on the rise globally.The development of nodules has always been primarily viewed as a nutritional disease. Traditionally attributed to chronic iodine deficiency but recently novel nutritional causes have emerged . Benign nodules come in 2 flavours: hot and cold and while patients can present with a mixture, it is the presence or absence of a hot nodule that radically changes what complementary medicines you can and can’t use and what an effective treatment plan looks like. The pointers, as is often the case, are there for us in the patient’s presentation and pathology, so knowing the difference is no longer a guessing game. This UU30 comes with a great visual clinical resource and includes key papers on the nutritional management of nodules.
You can purchase Are You Running Hot and Cold on Thyroid Nodules here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
*****Your RAN Online Account has a NEW LOOK!!*****
Next time your log in, you will experience a more user friendly way to search, view, listen and download your resources. Find out what’s new here.
I had to say to a mentee just yesterday, “You’re going to see the topic for the Update in Under 30 this month and think it’s inspired by your patient but it was actually about the 3 other cases I’d seen this month, before yours!” Yep…I’m talking about thyroid nodules, which happen to be hot (pardon the pun) right now. But they’re not always hot, right? I mean, they are always a good topic for discussion because so many of our clients thyroid issues are due to these but nodules come in 2 flavours: hot and cold. And knowing the difference is about as important as knowing your left from your right 🤲
“Oh Iodine the panacea of all things thyroid (tongue firmly in cheek) – can you fix nodules as well?” chorus the masses
Honest (salt of the earth!) Iodine Replies, “No & in fact I may make some nodules worse!”
Sorry for the re-enactment of this little local theatre piece in my head…it’s been a big week. Hence the marionette…ah yes it’s all becoming clear now 🙄 But it seems this isn’t common knowledge because a mentee presented a case this week of a 39 year old female who has confirmed multiple thyroid nodules that had prior to seeing her, seen another practitioner who put her on high dose iodine with the reassurance “there’s nothing wrong with your gland that iodine can’t fix”..or something to that effect. Oh boy 🤨
“Tell us! Tell us what happened next!” the chorus chants
Well it looks like as a result of the iodine, her cold nodules just might have switched to hot…that’s bad news all round I am afraid 🙁 But if we all knew our nodule nutrition better, this wouldn’t happen.
Next week our October UU30 release becomes available: Can you tell you tell your Hot from your Cold in Thyroid Nodules?
Our Update in Under 30 Subscription allows access to the ENTIRE back catalogue of podcasts in addition to all podcasts released over the next 12 months. We are currently offering the Premium at a reduced SALE price of $239 (excluding GST) for 12 months. This Premium Subscription is worth its weight in gold! With a total value of over $1800, you receive each month a new podcast and access to the ENTIRE back catalogue to the value of $20/month (ex GST).
Stop press. No, seriously. This new research warrants the attention of every practitioner working with children & teenagers. In the largest paediatric study of its kind to date, which included 2,480 children aged 10-18yrs diagnosed with hyperthyroidism (Grave’s or otherwise), Zader & colleagues found
Double the rate of ADHD diagnoses
5 times the rate of Bipolar diagnoses (almost 7 times in males)
5 times the rate of suicidality
That’s what I said: in 10-18 year olds
What is most alarming of course is that these mental health diagnoses were made in half of these children >3 months prior to the diagnosis of hyperthyroidism. What does this mean? It means we are missing this critical biological driver in this patient group. We all recognise the potential for some psychological presentations people affected with thyroid conditions, however, perhaps we are more alert to this in adults and letting it slip off our radar in kids? There’s been renewed talk about the over- and mis-diagnosing of ADHD lately and given that research has found up to 80% of hyperthyroid children meet ADHD diagnostic criteria this is one of the 1st place arguably to look! It also means, as these researchers discuss in detail, these kids are being medicated with psychiatric meds that in fact may, at the least mask their abnormal thyroid, lead to the incorrect diagnosis of hypothyroidism (lithium & even stimulants for example) or exacerbate their hyperthyroidism (quetiapine). But wait there’s more and it’s essential to understand.
Zadar & colleagues note that while we can not be 100% clear about the direction of the relationship…e.g. were these children already at risk psychologically and the hyperthyroidism just exacerbated that, they note that correction of the TFTs does not always equate to ‘cure’ of the mental health issues. This is not entirely surprising of course. What the problem emerges via a combination of biology and psychology & we resolve or remedy the biology…guess what you have left? PLUS the learned behaviours etc from suffering from anxiety, impaired cognition, suicidality they’ve been battling at the hands of excess T3 and a subsequent tsunami of reactive oxygen species.
This is one of those papers we should all have to read top to toe and therefore ideally be able to access for free but alas 🙁 What you can read is the Medscape review of this, which is a reasonable summary but the full paper is worth it if you can. You know the other key take home here…the diagnosis of hyperthyroidism was only made with overt out of range TFTs… which begs the question what about all those subclinical hyperthyroid cases we know exist? Yes, no wonder this paper has RACHEL’ S FAVOURITE written all over it…paediatric thyroid assessment and missed biological drivers of mental health and the opportunity to get better at both…can my research reading get any better this week?!🤓
Currently in Australia there is limited use of age specific reference ranges for thyroid parameters in children & teenagers yet they are essential for correct interpretation and diagnosis. Even doctors & specialists seem to be at a loss with diagnosing thyroid problems in kids unless they are extreme presentations. Subclinical thyroid presentations, however, are increasing in both children and adults. Many practitioners competent in adult thyroid identification & management are less familiar and confident with knowing when why and how to test in this population. Make sure you’re not missing thyroid imbalance in your paediatric patients…early detection makes treatment easy.
Those ‘still-believers’ look away now. One of the great myths, misconceptions and misunderstandings in nutritional medicine is that supplementation with specific nutrients will produce change specifically in one system, or pathway, which just happens to be the one that the practitioner has determined would benefit most/is targeting. Let me explain myself a bit better. When we give patients any nutrient, in the cases where it’s not simply to correct a global deficiency & therefore improve levels all round, it’s typically on the basis of a specific desirable therapeutic benefit, e.g. some magnesium to help their GABA production…, additional B3 would improve their mitochondria. Beautiful on paper…but like sending a letter to Santa in reality (I did warn you!)
Truth Bomb No.1: There are nutrient distribution pecking orders that have nothing to do with who you ‘addressed’ it to
This dictates that when something is given orally, for most nutrients, the gut itself has first dibs. So the cells of your digestive tract meet their needs before any other part of your body gets a look in. Sometimes the digestive system’s needs can be quite substantial and leave little for any other part of the body…not mentioning any names (ahem) Glutamine!
Truth Bomb No.2: En route to the ‘target’, these nutrients get delivered and distributed to many other tissues – with possibly not so desirable or intended effects!
You may determine that a patient needs iron because their ferritin hasn’t got a pulse…so you keep giving them daily high dose oral iron to ‘fix’ this…not realising you’re making their GIT dysbiosis and gut inflammation worse in the process. Or you feel their mysterious ‘methylation cycle’, happening predominantly in the liver and kidneys, could do with a folate delivery…perhaps ignoring the very worrying fact that their colon may have already had a ‘gut full’. Literally. Hence the concerns and caution against supplementing with folate in patients with established colorectal cancer. So is bypassing the gut via IM or IV nutrients the answer…well yes and no…but mostly no. Read on…
Truth Bomb No.3: Those pathways that use the nutrient you’re supplementing, that are most active in the patient’s body currently – which is determined by many factors (genes, physiology, feedback circuits, pathophysiology) and rarely simply by the availability of nutrients – will take take the next lion’s share of that nutrient
Wanting to nutritionally support someone’s thyroid, you know tyrosine is the backbone of the thyroid hormones, so you include this in the hypothyroid prescription. Will it help? Who knows? Being a non-essential amino acid the body exhibits very complex regulation of its distribution and use – with thyroid precursor availability being only one job on a very long list! And if this was in a patient who is regularly smoking cannabis, due to upregulation of the tyrosine hydroxylase enzyme – there is likely to be more of the supplement headed for even more dopamine production and very little or none reaching in fact your intended target. And don’t get me (re)started on Glutamine – supplements of which in an anxious and glutamate dominated patient will make…G.L.U.T.A.M.A.T.E…right…not GABA! 🙁
Sorry, I know, it hurts right? But these are essential teachings, that tend to have been over-looked or under-played I find, in nutrition education, regardless of training: nutritionists, naturopaths, IM doctors, dual qualification practitioners remedial therapists. Nutritional medicine is a wonderful and potent modality when it’s done well…but we need to revisit some core truths and principles that many of us have missed out on, to ensure we’re not writing letters to Santa.
Let’s start with Micronutrients. Let’s talk make sense of the over-arching nutrition principles, that will profoundly change your understanding and application of this modality Truly understanding the ‘big’ concepts, so often overlooked, or incorrectly taught, ensures you get the critical ‘small’ detail in your nutritional prescriptions right. In this 4 hour recording, together with key clinical tools, we talk about the tough stuff: dose-response curves, active versus passive stores and excretory pathways and ooh lah lah…the myth of taking ‘activated vitamins’. Even those who felt well trained – will find a lot in this critical review that is new, insightful and truly practise-changing!
So we already know that thyroid problems can start in utero, right…but a recentMedscape review(the fountain of thyroid information that I frequently drinketh from 😉 ) on Hypothyroidism in childhood taught me a couple of big things I hadn’t known before!
The diagnostic criteria for subclinical hypothyroidism are raised TSH levels in combination with a normal concentration of free serum thyroxine (FT4) but because there are some differences between accepted ranges in TSH assays, high-risk groups should be screened, especially babies with malformations, whose mum received steroid treatment during pregnancy or in the neonatal period, or who had existing thyroid dysfunction, TFTs (or at the least TSH as part of what’s called the Neonatal Screening test) should be repeated 2 weeks later. But now comes the couple of big light-bulb moments: the incidence of eutopic thyroid in twin births is nearly double compared with singletons! As you know, I’m a mother of twins and I’m guessing at 18yrs old now (and multiple peachy TFTs 😉 ) the horse has well and truly bolted for my two but geez…I had no idea of the dramatic increase in risk. And it keeps going…monozygotic twins very commonly show a delayed TSH rise and those numbers are even more prominent in multiple births. The other not-so-fun-fact is the discovery that subclinical hypothyroidism in IVF babies is approx. 10% which is noteworthy considering none were observed in the control group.
This obviously left me thinking “W.H.Y?” And of course…the first place my head goes with the latter…is iodine.
The reasons behind our increasing rates of thyroid dysfunction across the life-stages are multifactorial (and don’t get me started on the very real contribution of EDCs!) and how, in spite of iodine adequacy being the first thing on the checklist for thyroid health, so many health professionals ignore this, at their patients’ peril… But now at least we know that patients with IVF babies, twins, and preterm bub, who are currently not included in the prioritised screening groups should be…and of course we should keep asking the questions, “what are the mechanisms behind this, why is it so?”
So if this has made you even more curious about the incredible butterflied-shaped gland and you’d like to go for a stroll on the vast plains of “thyroidisms” you can click on this link Thyroid Assessment in Kids and Teenagers and get completely “thyroided” up. There is always more research to come our way so keep your eyes and ears peeled.
That’s me…always questioning the ‘status quo’ and Iodine is the perfect example! The interview I did on this important subject with Andrew Whitfield-Cook from FxMedicine, covers a lot of key areas of confusion & underscores why it’s so critical all health practitioners get clarity on this topic. ‘It’s just a matter of geography’.
You know, I say to people, we can make vitamins ourselves, we can get all sorts of other organisms including animals, bacteria and plants to make vitamins for us, and then eat those…but minerals…our source of minerals…well it all comes down to the rocks and the soil our food itself is grown or fed on. And iodine is profoundly influenced by these factors.(more…)
“Researchers followed more than 500 women trying to conceive over about five years and found that, overall, those with moderate to severe iodine deficiency had 46% lower odds, per cycle, of becoming pregnant.”
All researchers dream of generating the kind of results that are ground-breaking but sometimes you read about the latest study’s findings and you think, ‘Really, you spent all your time & cleverness for years on this and that’s all you have to show for it!’ Like the study that finally confirmed dog’s can feel empathy (at last thank goodness …phew…cos I had my doubts until they crunched the numbers!)
So too a study published this month on the possibility that iodine deficiency is common in women trying to conceive in developed countries and may be connected to increasing fertility issues.
Stop press! I know…that made you spill your coffee!(more…)
 Wow, menopause is really having a moment, isn’t it? Or is that just me (and my mates who are all somewhere on that perimenopausal path)?! But seriously, medical perception of this reproductive transition is undergoing a revolution right now—widening the lens to take in more diverse potential presentations and lengthening the period of impact recognised both ‘before, during, and after’ that last, last…no hang on…last period. But I fear we are at a crucial crossroads. Anything could be related to (peri)menopause, but not everything is or should be.
Wow, menopause is really having a moment, isn’t it? Or is that just me (and my mates who are all somewhere on that perimenopausal path)?! But seriously, medical perception of this reproductive transition is undergoing a revolution right now—widening the lens to take in more diverse potential presentations and lengthening the period of impact recognised both ‘before, during, and after’ that last, last…no hang on…last period. But I fear we are at a crucial crossroads. Anything could be related to (peri)menopause, but not everything is or should be.
 You can purchase
You can purchase 
 MasterCourse I: Comprehensive Diagnostics.
MasterCourse I: Comprehensive Diagnostics.