Ever been guilty of having a ‘man’s look’ for something? I have. Particularly when it comes to the online omniverse! I can be a bit flaky at finding things right there on the page…allegedly! So for those of you who have a similar experience with my website & endless educational offerings, I FEEL YOU! We do have a tonne of training options and a whole lot of (love 😉 couldn’t resist the Led Zepplin reference)… lab & diagnostics resources! This has come up in conversation a lot recently, following the release of our RAN Student Pathology Hub, for example: “I’ve done your MasterCourse in Diagnostics, does this cover something different?” or “LOVED😍 this new hub its *$@# incredible resources & extra training vids but I also wished it included your take on… [insert your pick from infinite list: thyroid, cortisol, zinc etc etc etc]
So here’s a Dummies Guide:
How to Find the Help you Need in Diagnostics
If you are just starting out on your path to pathology & true lab literacy & want an accelerated way to ensure you are starting this journey on solid ground and you have the most called-upon skills you’ll need in clinic today, then the RAN Student Pathology Hub is your perfect match. NOTE: this is not limited to actual students but anyone who considers themselves, like us, a life-long learner! This 12 part module includes some small core components of our MasterCourse, a few expanded episodes from our Update in Under 30, plus unique short training videos, covering tests and topics including: Iron studies, B12 assessment methods, Coeliac screening & much more
If you’re seeking the immersive experience – you want to maximise your competence and confidence & forge your path as a true Diagnostic Diva or Divo then look no further than our ‘mothership’, the MasterCourse in Comprehensive Diagnostics which now has a part payment option. This really is the most seminal training we offer, taking the time to dig deep into the science behind all the ‘signposts’ our patients’ results are pointing to. A big commitment for a big reward. It comprehensively covers all the routine labs you will see everyday: LFTs, Renal markers, Glucose and Lipids, FBE & WCCs & is loaded up with case illustrations for each key pathology pattern – that many practitioners say was an absolute highlight
Just have a specific question or need for upskilling in Cortisol assessment? Zinc or Zonulin? It’s probably in our vast Update in Under 30 library! Yes, with more than 100 episodes in there and my penchant for pathology…you’ll find something, if not in the UU30 episodes, then somewhere else on my website. You know how in pdfs ‘Control + F’ is a god! Ok on my site it is this fella 🔎 You can use this to search my whole site to find free information on the topic (blogs) or manifest the same magnifier🔎 magic once you have clicked ‘Catalogue’ on the top right of the tool bar on any page, to locate any specific educational offerings. Remember with the UU30, you can purchase single episodes or subscribe and get access to the whole shebang.
And for those of you primed praccies, patiently waiting for our MasterCourse II to land? Well about that…did we mention we got hit with a flood? Twice? And then got covid? Two of us? And have our beloved Nina about to depart to become a mumma!!! Yeah, so our plans to have this up and ready for May changed to Mayhem, real fast 🙄🤪 We will definitely keep you posted on any developments and new timeframes but for now we can only apologise for the delay and will do our best to get back on track with this, at the earliest opportunity. In the meantime maybe a little review of some of MasterCourse I is in order? I refer back and re-listen all the time, myself!!😂
Being a practitioner who is able to read labs will set you apart in practice. For your patients this flows from your ability to form a more sophisticated understanding of what’s happening for them, enabling you to better individualise treatment and deliver superior outcomes. Amongst other health professionals, it will attract positive regard and an increased willingness and enthusiasm for sharing the care of patients with you. Learning to be lab literate could take a lifetime…or you can enter the expressway from the very outset! We have curated the content to reflect the most essential elements, to help you hit the ground running in the shortest period of time. Spread across 12 modules which can be consumed as monthly instalments or, as an all-in-one experience for those wishing to waste no time. The teaching points, tips and tools make the complex simple, engaging, even fun!
Developed, designed and delivered with students of any health discipline in mind.
Burning, tingling, crawling, buzzing, humming, zapping, pins & needles, numbness: our patients often tell us about strange sensations they have in various parts of their body. It’s typically not their major concern, but they mention it as an aside, a curiosity, ‘another weird thing I get’. While they may have trivialised this, relative to their ‘real issues’ [insert gut, hormonal, mental health] we should do the opposite and bring this concern to top of the list to correctly identify the cause.
If bilateral sensory nerves are mis-messaging it typically means 1 of 2 things: 1. Nerve damage is occurring – and if allowed to progress this can become irreversible or extend to motor and central deficits 2. Nerves are irritated or impaired – and this tells you something ‘systemic’ is out of whack and these sensations are often the only alarm bell
The top cause of paraesthesia, falls into the first category and is of course diabetes – and yes even now diabetics will walk into your clinic not knowing they have this (a good old HbA1c should be routine to rule this out). Second on the list is alcohol dependence. The third most likely explanation for the patient with paraesthesia is nutritional. And in contrast to what many of us might incorrectly think, there is a long list of nutritional imbalances that can be responsible for either, nerve damage or irritation, and B12 deficiency is not in fact the most likely.
That’s right all you nutritional ninjas🐱👤 – that makes the correct identification of the cause & the solution our bag, right? I mean who else is going to do this, accurately?
Asking the right questions about these sensations helps you to quickly confirm when a nutritional cause is likely. From there we need to know how each single micronutrient excess or deficiency or in the case of some, ‘sort of single’ nutrients (we all know people who sit in this category, right?! So why not nutrients 😂) are likely to present, via ‘easy-to-spot’ key characteristics that cover: pattern of distribution, speed of onset and progression, risk factors, accompanying features etc. In our final New Graduate mentoring session for 2021, a practitioner presented her patient who rated her concerns as 1) Fatigue 2) PMS 3) GIT issues & 4) Tingling & crawling sensations across limbs, face, lips and tongue…and I was like, whoa stop right there, you might just have given us the answer to all of the above~!~! Seriously. Here’s a clue: it wasn’t oral allergy syndrome and it wasn’t B12. Can you pick it?🤓
The Patient with Paraesthesia – Part 1 Patients often mention experiencing peculiar sensations: crawling, tingling, burning, as an aside, as a ‘oh and by the way’. But while it may not be their top priority – it should be ours. That’s because nutritional imbalances are the 3rd most common cause of these and timely treatment is essential to prevent progression to more serious issues. The list of potential nutrient deficiencies and excesses behind these, is long, but this recording, the first part of 2, will help you narrow the differentials, nail the diagnosis & the solution.
The Patient with Paraesthesia – Part 2 In this continuation of this topic, we discuss several less talked about nutrients whose deficiencies drive potent pathology for the nervous system & move onto a cluster group of minerals, whose imbalances create functional irritation rather than organic change. This episode includes a range of excellent resources from videos demonstrating in-house tests you can perform to aid diagnosis, as well as our own Ready Reference which assists correctly categorising the different paraesthesia patterns and the nutrient issues behind them
You can purchase The Patient with Paraesthesia Part 1here and Part 2here.
BUY PART 1 & PART 2 TOGETHER AND RECEIVE 10% DISCOUNT BY USING CODE BUNDLE12
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
There are some things we say so often to patients we could record them and just press <PLAY> Like this daily dogma: ‘When you’re under stress, your demand for Magnesium rises and then in turn that can make you more susceptible to further stress, so we’re going to give you some to support you’. But is this actually the whole story? You guessed it, no. (I know I am fairly predictable like that 😅)
Recently, a personal new record – a patient reported ongoing daily use of a very high dose Magnesium ‘practitioner only’ product 8 years after it was prescribed by her then naturopath – and guess what, the patient still hadn’t reached nirvana* not the band! – a transcendent state in which there is neither suffering, desire, nor sense of self
Jest as I may – I think this raises some serious questions. The pervasiveness of our prescriptions when patients are not given an end-date coupled with ongoing access. How (not) effective this intervention was if someone perceives ongoing undiminished dependency on it. And specifically with Magnesium – whether our prescriptions (form, dose, adjuvants, advice) are the problem? If stress is synonymous with a shortfall of this mineral then Magnesium is not a solution to stress itself but the amplified stress response and the stress still requires its own redress, right? But do our patients hear this as well when we press <PLAY>?
Likewise – the BIG doses per serve being recommended might make sense for the minority (seeking potential NMDA antagonism) but are a real mismatch with the majority, who are just stuck in the stress loop and weathering a perfect storm of Magnesium under-supply and increased demand.
I love my minerals as much as, ok more than, the next practitioner but I’m always keen to refine my repletion approaches and oh yes, by the way, there is good data, a meta-analysis in fact, examining how long it takes to achieve repletion using oral Magnesium – and guess what, it’s not 8 years! The latest Update in Under 30 goes into all this and much MuCh MUCH more…you’re welcome 😂
Practitioners working with nutrition appreciate that Magnesium is vulnerable to depletion by the stress response and that in turn, can make people more prone to stress & keep patients stuck in a so-called ‘stress loop’. But do we understand the intricacies of this and how we, as practitioners, can get stuck in another kind of loop – one of endless Magnesium prescribing without reaching repletion? We discuss ways to improve your Magnesium prescriptions – in particular, ‘doping Vs drip-feeding’ and other things to assess & address if the long road to repletion risks becoming an endless one!
You can purchase Magnesium – Stuck in the Stress Loophere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
An ideal T4 is 15
An ‘anti-aging’ DHEAs must be >7
A ferritin of 100 is optimal for women…
I’ve heard it all, probably you have too, and far too often & too recently from practitioners who should have rationalised & researched their way beyond these functional falsehoods, by now. I bought into these ‘optimal wellness truths’ hook line & sinker early in my career and proceeded to even propagate a few but with (not much) more experience in clinic, I had to seriously question this pursuit of ‘perfection’ & ‘perfect pathology’…in favour of reality & scientific evidence! They didn’t add up. Not with my patients – even the healthiest ones, in fact some of the really unwell ones occasionally had these kind of high-normal results and they were part of the problem!. ‘But that’s because no one is truly healthy outside of those seeing a functional medicine practitioner & supercharged on supplements & hormone replacements!!’ came the counter-argument. Ahhh, really?
How then do we reconcile this with the following: Individual genetics & biochemistry
Our biological resilience Healthy & appropriate senescence Large datasets of mixed race populations from other comparable first world countries…where these figures denote the statistical outliers?
I mean, if the 50th centile value for ferritin for actual living, breathing, bleeding, women in the US, Canada, Australia etc etc is 30-40 ng/mL and the 95th centile is 126 ng/mL and the WHO says that in fact, anyone menstruating with a ferritin > 150 ng/mL should attract suspicion for iron overload….but functional medicine men (mostly…sorry but it has to be said!) say 100 IS OPTIMAL FOR EVERY WOMAN #@^*…please tell me in which women, consuming what kind of diet, where in the world, & based on what improved or better health outcomes?
And while you’re there can someone please support this bold claim with a scrap of high quality evidence?? [Rant over🎤💧]
The falsehoods of functional medicine include the blanket belief, ‘more is better’ (ahhhhh not when it comes to many things, including iron where women’s lower levels have been found to be an evolutionary advantage…guys). But you know what, we’re better than that! We see each individual, recognising all the factors at play that make for their uniqueness, help to define what ‘healthy’ looks like for each person and don’t fall for one-size-fits-all claims without any evidence nor common sense even, to support them. What do you think?
Let’s make sense of the over-arching nutrition principles, that will profoundly change your understanding and application of this modality Truly understanding the ‘big’ concepts, so often overlooked, or incorrectly taught, ensures you get the critical ‘small’ detail in your nutritional prescriptions right. In this 4 hour recording, together with key clinical tools, we talk about the tough stuff: dose-response curves, active versus passive stores and excretory pathways and ooh lah lah…the myth of taking ‘activated vitamins’. Even those who feel satisfied with their original training – will find a lot in this critical review that is new, insightful and truly practise-changing!
And it will. It knocked again on a practitioner’s door last week. She in turn knocked on mine. It turned out to be a very familiar story:
Firstly:Patient presents distressed – recently a nurse applied the term ‘Chronic Kidney Disease’ to HER (note no one has ever mentioned this diagnosis) Secondly:She is in stage 3 of 5 Then: This practitioner is left to have ‘the conversation’ but wants to know where to start, ‘What do I say?’ Next up:And what else can I do for her – are we really able to make a difference?
Familiar to you too? So,1st & 2nd: Yes, this is not uncommon we would have to say and even with age-appropriate reference range adjustment, her GFR consistently in the 50s, flags premature decline. Then: What DO you say? Well this clearly is a delicate area, not only because of the level of patient distress and concern but because, at this stage the practitioner knows nothing more than what the patient tells her and her ELFTs over the last 2 years. This is not enough information, right? Chronic Kidney Disease is a heterogeneous condition, with many different causes, manifestations, comorbid conditions, and factors affecting prognosis (Levey et al., 2009) So while most individuals certainly progress from stage I to II and II to III the rate at which they do this differs dramatically.
Two years of data is not long enough for us to appreciate the trajectory of her CKD & means we are unable to provide the patient with any kind of perspective:
‘With no further decline in GFR or progression in stages over 5 years, you’re doing well, so keep doing what you’re doing!’ Vs ‘Ok, I can see what looks like a little period of accelerated decline – let’s review what’s been happening and how we can turn this around”
“Please sir can I have some more?’ Yes, back to her primary carers to request more information to fill in the gaps, and ideally more labs to calculate & observe the trajectory for yourself. Next Up: What do we have to offer the patient with CKD stage III? Soooooooooooooooooooooooooooooooooo much!! When is adequate hydration helpful? Always, except Stage V! (and these patients are not coming to see us) What are our treatment objectives & our evidence backed medicines to meet these? Hcy lowering (note often referred to as ‘folate refractory’ in renal dx), vitamin D adequacy, lowering the acid load, supporting the microbiome & in turn the Renal-GIT axis…hang on, got to go…someone’s knocking 😅 but hopefully we all can see, when they present to us, they are indeed knocking on the right door ✊
Nutritional or naturopathic support for the kidneys tends to have been over-looked in our training and yet research suggests there is much in our tool kit that can make an enormous difference to this system, in particular, slowing the progression of chronic kidney disease in patients. Rachel talks about what these key evidence based interventions are and also gives you the tools to identify the early pathology markers of renal impairment – the earlier the recognition, the earlier we can make a start on the remedy.
It seems almost farcical to question the merits of hydration for our renal health but is this actually the truism we have been lead to believe? Where does the recommendation of ‘8 glasses a day’ come from and what is the level of evidence to support it and in whom? Or should we in fact be setting our sights on output ie. 24 hr urinary volume, over input. Do all kidneys love water – or does this relationship change with the progressive impairment seen in CKD which affects up to 30% of our middle-aged population? When does hydration become harassment?
Most practitioners graduated with not much more than a few ‘kidney’ herbs and an under-appreciation of the contribution renal health makes to wellbeing. It’s not just about waste and water. In reality, the kidneys are pivotal in just about every major element: blood, bones, pH balance, methylation, control of oxidative stress, the GIT microbiome and more! And we are seeing the impact of this in our patients in all sorts of subtle and not so subtle presentations. This new instalment in diagnostics, brings the renal system into the spotlight so we can confidently identify and better manage its critical contribution. In addition to this, just like with other routine labs such as LFTs, we unpack how these so-called ‘renal markers’ can flag a plethora of other insights into your patients, from reflecting (un)healthy muscle mass, to calculating individual dietary protein adequacy, from key ‘danger and distress’ signals in response to disturbed metabolism, oxidative stress to certain types of GIT dysbiosis! We call this Explained, Expanded and Exploded because these routine labs can deliver XXX sized insights into your patients.
And not in a good way, right. While we’ve known about the potential for peripheral neuropathy with excess B6 supplementation since the 1980s, currently there’s a seismic shift in our sense of safety even with previously regarded ‘safe’ levels. You may have heard individual whispers, or the chorus of voices coming together, both here and overseas, belonging to members of the public who report suffering sensory nerve impairment with as little as 2mg/d! Is this a mess of mis-diagnosis, false attribution & nocebo? Perhaps for some, but certainly not for all.
How could this be the case given the many RCTs employing hundreds of mgs per day over months, with no such events recorded? How could this be given, your (?), certainly my, high dose prescriptions, with only 1 case of quickly reversed, peripheral neuropathy in over 20 years, on my books? The pieces of this complex paradoxical pyridoxine puzzle are coming to light.
Is it the form?, the dose? the duration? individual differences in B6 metabolism & toxicity threshold? amplification of risk secondary to levels of other nutrients, or the use of certain medications? Yes. And we need to understand each element to better tailor every B6 prescription to the individual & mitigate risk. I have spent the best part of this month reading almost every paper on this from the 1970s to last month and I am now alarmed but more importantly, alert, to what prescription practice changes we can all make to lessen the risk, and control the power of B6. It’s been the most compelling deep-dive. Because in spite of a clear TGA warning issued last year that likely prompted the quiet removal of high dose products from market, it would seem none of the companies have the courage to have this difficult conversation with us 🙁 I invite you to ‘feel the fear & do it anyway’ & listen in to our latest Update in Under 30.
Haven’t we always known that nutritional medicine is a potent prescription? Now thanks to more sophisticated research we have a much greater understanding of this and of both the intended and unintended effects of micronutrient supplements that have the potential to achieve supra-physiological levels. B6 metabolism is arguably the most complex of the Bs – involving 6 different forms, at least 2 of which are active – and exhibiting some of the most complicated regulatory control designed to both harness the power & limit the accompanying risks. Excess B6 supplementation, however, has long been known to present as peripheral neuropathy in some individuals and case reports of this are growing, at lower and lower doses. New information has come to light to help us understand the why, the how and better still how to mitigate risk to our patients.
You can purchase Dynamics and Dangers of B6 – Controlling the Powerhere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
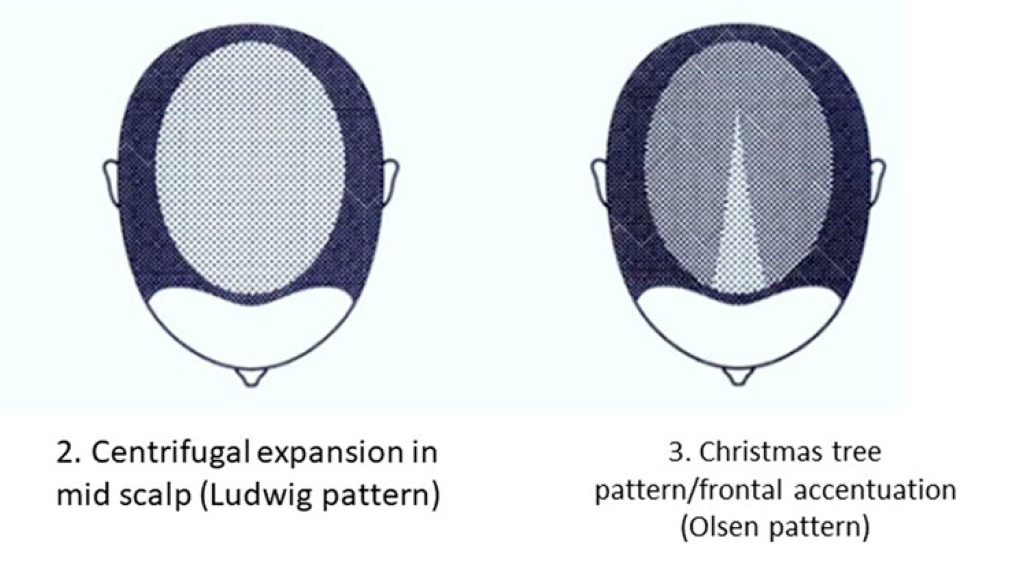
I’m intrigued by the silence. Hair loss in women is frighteningly common, following pregnancy, menopause & with extreme stress (wait is that a tautology? 🙄) In fact it can strike at any age and for a multitude of reasons. When it happened to me a few years back I also initially responded with silence, terrified that if I said it out loud it would make it real, but when my daughter suddenly asked, ‘Mum are you losing your hair?’ with her trademark attention to detail & exquisite empathy, she gave me the words & a good kick into gear, simultaneously. Now I am fascinated by women’s silence around this generally, how little we share our stories & forewarn others, & as practitioners, the lack of adequate training we’ve had identifying the different types (hint: it involves donning gloves or if restricted to online consulting, knowing how to organise correctly positioned pics) & from there finding the right solutions.
While Female Pattern Hair Loss (FPHL) is the dominant type in women – it only applies to the following pattern:
But alopecia due to stress, thyroid disorders, autoimmunity, contact dermatitis etc will affect different regions of the scalp and with a different onset & progression.
And remember, by the time YOU, the practitioner, can spot a patient is losing hair when they simply walk into the room, they have ALREADY LOST 50%😢 This is why I think we need to push back against the silence. The research is unflinching about the serious psychological impact this has on women – especially in cultures which place so much emphasis on looks generally, and hair, specifically as a commodity of very high value in women. The diagram above comes from a 2019 update on the phenomenon of FHPL and it’s a good articulation of the knowns and unknowns (pssst spoiler alert…it ain’t about androgens!) but let’s never forget the other causes and cures. So let’s make sure as the trusted practitioners women present to so often, we are sensitive enough to have this tricky conversation & skilled enough to help 💪
Stop Pulling Your Hair Out – The FPHL Answers You Need
Female Pattern Hair Loss (FPHL) is everywhere, perhaps you just haven’t been looking. As the leading cause of alopecia in women globally and with 1 in 5 women affected at any age, we’ve all got clients who have FPHL to different degrees. We need to be better able to recognise the early features of this condition which profoundly impairs quality of life and induces depression in its sufferers and that begins with validating patients’ concerns when they report “thinning” or “increased losses”. But what do we do from there? This recording talks you through the assessment, diagnosis and management of FPHL based on a combination of the most recent research and Rachel’s clinical experiences. Once you’ve ‘seen’ FPHL.., you won’t ever ‘unsee’ it and your patients will thank you.
I confess I was a chemistry nerd ‘way back when’, but my skill for stoichiometric calculations had sadly slipped by the time my kids needed help with high-school science & now my son, who’s about to graduate from chemical engineering, is my ‘chem-friend’ 🙄🧐 I suspect he feels FB messenger wasn’t intended for such use – or at least there should be some veneer of, ‘Hi darling how are you?’ before…’Need to talk through these pharmacokinetic datasets’ However, the one equation that was like turning a light on in my brain & therefore never forgotten was the Fenton reaction – basically metals’ MO for messing with our biology, especially iron. Turns out – it’s the most essential and helpful in understanding health & disease:
Endometriosis IBD Neurogenerative disorders: MS, PD, Alzheimer’s Higher than healthy GGT Impaired COMT or catechol excess for other reasons Cardiovascular disease & Diabetes Vitiligo Both the Big Cs Heavy metal burden Iron dysregulation (Obesity, HFE mutations, Thalassaemia) & Excess (IV or oral over-treatment etc)
(almost) All roads lead to radicals & reactive species…if you follow the Fenton pathway & iron leads us down this path more often than any other metal. Certainly sometimes for good: like protecting us against pathogens and destroying dodgy cells, but when it gets out of hand, a key pathophysiological process in a long list of disease. So understanding how to recognise patients prone to dysregulation of this mineral, avoiding iron over-treatment at all costs (I am seeing incorrect and excessive use of IV iron in many patients make it stop!) and identifying means to contain and control its movement, are important. Oh and in case the Fenton has faded in memory, it goes a little something like this:
While rates of iron deficiency and related anaemia continue to grow, the increase in prescriptions of IV Fe have expanded exponentially in western countries. What is behind this change in practice regarding how we treat iron deficiency and does it match with responsible prescribing? Do the benefits always outweigh the risks? And while we’re on the topic, who is most likely to benefit and what are all the risks? In light of a current class action in the US, relating to a lesser talked about adverse event associated with IV Fe and recent complaints here in Australia against GPs, allegedly due to inadequate information to enable informed patient consent…it’s time to answer these questions and more. When is IV Fe a means of rescue and when is it a risky repletion strategy with no evidence of advantage? Click here for this episode.
I’m 100% confident that, as a professional group, among our highest values about healthy, preferable, food choices, would be characteristics like: ‘as close to nature as possible’, ‘unrefined’, ‘unprocessed’, ‘unadulterated’. Tell me I’m wrong.
So, when I keep hearing about NEW! “Never seen before” (read: never in nature) modified (read: more processed, adulterated) nutritional supplements: water soluble vitamin D, fat soluble C, bioflavonoids with unprecedented (read unnatural) bioavailability
I’m left wondering what these companies are missing about their customer group (because we are clear about our valuing of nature & what’s natural & have a desire to minimise exposures to things that are not, right?
or what are we missing here, in the clear conflict of our core values these constitute?
I think if we find ourselves forsaking this core value & prescribing highly modified, unnatural supps, it’s the result of both hype & fear. The hype is self-explanatory and I’ve written recently on how modifications exponentially increase profit margins for companies, all the while possibly reducing ours because patients are spending more on product and therefore there is less left over for the practitioner fees 🙁 [The ones spending hours with them face to face, not to mention years & thousands on our training] The fear is perhaps less apparent, more insidious. The fear is that we’re not using the best, being the most effective, and deeper still, inevitably that we will fail to action our patients return to health. This is a big one. I think it’s pervasive, if not omnipresent, and works as a motivator for many positive actions by practitioners – like engaging in further education, reading that latest journal edition on your lonesome laptop when you could be streaming some series on a shared sofa. But this same fear can also undermine us, overwhelm us and shake our tree of trust, that we believe to be so firmly rooted within us, of the healing power of nature.
So while my position sometimes makes me feel very ‘old school’, I’m not suggesting we return to nutritional prescriptions composed exclusively of bee pollen & brewer’s yeast and I absolutely recognise and respond to an individual who has very specific barriers to benefiting from nutrients in their natural normal forms. But let’s be clear, they are a minority.
Some of you will know naturopath Dawn Whitten & know that she is one of my mentors. I’ve had the benefit of speaking with her over the years about herbal prescriptions but also about the principles & philosophy behind our practice & in one of many conversations she told me that a key objective she has with her patients is to rebuild their trust in their body, their own biological resilience (I love this concept and that’s a talk for another time!) and ultimately in nature. Well jeepers Dawn – how did you get to be so wise so young? But isn’t that central to vis medicatrix naturae? Maybe that Naturopathic Nanna’s club isn’t so fuddy-duddy after all. Want to join us?
Speaking of using nutrients in their most natural state for the best health outcomes – the best B3 is probably not what you think!!…. The Balance of B3
Most of us have been taught to ‘balance the Bs’ when supplementing, which discourages the use of single B vitamins in case this interferes with the regulation and roles of others. In reality, outside of a couple of dynamic duos like B12 and folate, there is little concrete information & evidence of this. In the case specifically of B3, however, we now know, the risk of an excess of the most common B3 forms found in supplements and fortified foods, results not only in disruption of other nutrients but imbalanced B3 biochemistry itself. Given B3, in its coenzyme form NAD+, is regarded as highly valued currency in the prevention of many diseases, as well as the key to our optimal health and longevity, it’s critical to understand the different forms and functions of the various B3 sources.
Name a B vitamin. Hey, Bingo! It’s on the list! What list? The complete one from all the review papers & references to possible links between individual nutrient deficiencies & Angular Cheilitis – inflammation & cracking at the corners of the mouth. So does that mean more Bs are the answer for people presenting with this painful, recurring issue?…Ahhhhhh No. Yes, you heard me correctly, these deficiencies rarely cause the breakdown of the integrity of this very specific area of skin in the patients we see. So now we have a double ouch, right?
We might send patients away with a B complex and some lip balm and over a week the cheilitis resolves – which one was the most therapeutic? …I hate to tell you 👀
What is the underpinning cause(s) & the important message we are missing with this presentation? Well, it could be one or more of a long LONG list of differentials, ranging from anatomical, habitual, immune related to iatrogenic. And while many nutrient deficiency pictures can include this feature and therefore make the ‘possible’ list, only one makes the ‘probable’ list. And that’s iron but only in severe deficiency, aka anaemia and only affecting 1 in 5.
Me???
…Telling anyone to push the nutritional issues further down the list of differentials for any condition? Well, that’s unexpected
…possibly unprecedented
And no, antifungals aren’t the answer either. Yep, that might be worth a listen….👂
Just an annoying, embarrassing, cosmetic condition or could it be the clue that helps you ‘crack the case’? There is a surprisingly long list of differentials for this condition but most of us only know a few, reflexively reaching for either B vitamins or anti-fungal creams. Does either make sense? Does either address the cause(s) which we now recognise to be a unique series of risk factors in each individual? Or are we at risk of shooting the messenger and missing the message of Cracking Corners altogether?
You can purchase Cracking in the Corners – Angular Cheilitishere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
Last week I had my say about acknowledging our elders & mentors, this week I want to speak to the power of the young peeps. Just like a younger sibling, nipping at your heels can act as a great motivator to move faster, or having children can inspire us to do more to improve the ‘world’ we’re welcoming them into, my interactions with naturopaths, nutritionists & herbalists of the younger generations generally effect both responses in me! The best of these come from cluey ‘youngsters’ (mature-age-second-career-new-nats included!!) who ask the most difficult questions & show dogged determination in getting answers to these either via me or in spite of!
This is exactly what’s been in play over the last few years (yes, you heard me…years) while I’ve been under the watchful gaze of Jostling Josh Weymouth! He’s a youngun’ – it’s all relative right – who has kept us both on the straight and narrow writing:The accuracy and interpretation of plasma selenium in our patients: a literature review,which hasjust been published in the the Australian Journal of Herbal & Naturopathic Medicine.
At the outset I was able to hand over a substantial selenium research hoard I had obsessively compiled, Josh was able to build on this, refine some fledgling theories I had and then completely redefine my appreciation & understanding of how chronic over-treatment (not toxicity…) is so deleterious to human health. Check this out:
When Selenium (Se) saturation point occurs in plasma, there is a potential reduction in health protection… Se will progressively pool within plasma non-specifically as SeMet in lieu of regular, sulphur containing methionine, in albumin and other proteins…inducing oxidative stress via a complex disruption of cell reactions/signalling This is likely to be how Selenium over-treatment increases the risk of both CVD and T2DM
Many of you may ‘Know Your Numbers’ when it comes to Serum Se targets in thyroid health or just generally know how to Stay Safe with Selenium Supplementation because I’ve spoken extensively about these in the past and you will be relieved to know neither my ‘numbers nor my message’ have changed BUT I encourage everyone to read this new article because Josh has added so much more, including the interplay between our microbiota and our individual selenium needs, handling and tolerance and and and….I could go on but…what I really want to say is, thanks Josh for your academic rigor, your firm determination & diligence and for nipping at my heels all this time. This important piece of work just wouldn’t have happened without it 🐶
“How much can you misbehave & get away with it?” I listened with fresh ears, as a practitioner asked my son this question recently. I use similar ones with my own patients but hearing it from someone else, I could sit back and appreciate its true purpose and how well it achieves this. Most of us adjust our behaviours, when we can, to ‘manage’ things that cause us problems.
Sure I can eat food I haven’t made myself
………..but once a week is my max. or ‘X’ flares
My energy is pretty good …… but 1 night of poor sleep & I’m back on ’empty’
No impaired alcohol tolerance
………I just never have more than 1
My [insert: gut, skin, energy, immunity, mood] is not a problem
………as long as I don’t miss a dose (of supplement/medication etc)
And sometimes this ‘adjustment’ (or avoidance) is unconscious. Hence the beauty of the question: How much can you get away with, coupled with our understanding of how much ‘room to move’ there should be in a patient who is truly well. So the teenage to early 20s patient sitting in front of us, theoretically, should be in their prime of wide mischief margins, and we are alerted to individuals in this age group who are having to live like an older person, needing to exhibit vigilance around early bedtimes and allowing themselves almost no indiscretions. In contrast, as we age, we understand too, the margin for mischief narrows. Our over-50s selves are unlikely to get away with half as much as did in years gone by but we shouldn’t require the stricter self-care hypervigilance of our senior selves.
And for the patient who answers ‘no’ to everything on your GIT or stress/mood screening questions, for clarification, follow them up with, “and how much can you get away with and still have no issues?”
You may very quickly get a different understanding of what lies beneath and how much ‘management’ is required to maintain ‘balance’ or ‘no symptoms’ or ‘health’ 🧐
The primary objective of MasterCourse I is to realise the true value we can extract from the most commonly performed labs (ELFTs, FBE, WCC, Lipids & Glucose) which constitute the largest biochemical dataset we have on almost every patient. By learning how to comprehensively interpret these labs in an integrated medical framework, using the very latest science, we can extract the gold often buried in this goldmine. Accordingly, we prove ourselves to be the greatest asset to our patients, to other health professionals we are sharing care of patients with and we cut the cost of additional expensive testing, that is less well understood and validated.
MasterCourse I will help you access that gold and has been intentionally designed to match each lesson with real learning– with the time spent in theory and in application. Delivered across 24+ hrs of streaming video sessions with bonus pre-sessions, audios, resources and tools – this MasterCourse is likely to be a genuine game-changer for the way you practise and the potency of your patient prescriptions.
Just like Kevin, ‘Niacin’ is profoundly misunderstood and consequently runs the risk of doing us harm. Unlike ‘Kevin’, we can’t watch the movie to see how this (our arguably excessive use of the wrong forms of B3 in supplements and fortified foods) is all going to play out, so that we can be suitably alarmed and start making some different choices. The risks that follow from our B3 ignorance are twofold:
One comes essentially from our gross under-estimation of this B vitamin – we’re stuck in the Pellagra Paradigm, believing that prevention of the 4 D’s is confirmation of adequacy.
The second, is our lack of discernment when it comes to the different forms or precursors of B3 & our unfamiliarity with their very specific physiological roles – good and bad.
In this regard we’re all likely to say, ‘Well back up there 1 second, we do know that Niacin (aka nicotinic acid) is different from the other forms!’ Producing flushing, yes. Used as a lipid lowering agent in pharmacological doses, yes. But can you tell me, which serious concerns and biochemical disruption is shared between both gram doses of niacin and everyday ‘routine’ mg doses of niacinamide? Yep, that one, the so-called ‘safe’ one. Better still, can we all list the various B3 forms in order from most to least potent, in regard to their capacity for NAD+ promotion in the human body?
Because this is now the definition of B3 ‘adequacy’ or ‘optimisation’ according to modern scientific understanding & it is a long long way from the absence of Diarrhoea, Dermatitis, Dementia and Death!
In fact, the boosting and optimisation of NAD+ pools in the human body is key to life – a long and healthy one according to the current research consensus – and its depletion is akin to ‘death’, or a faster one, anyway. From increased metabolic disorders, mitochondrial dysfunction, impaired gene stability (cancer, infertility etc) and higher rates of neurodegenerative disorders, just to start, these take up the lion’s share of our chronic health burden and battle that currently dominates the dis-ease landscape. And more niacinamide might just make that worse.
I didn’t mean to to alarm you. I am alarmed. Want to deep dive into this yourself? Start with this older but still brilliant review article by Bogan & Brenner. Want me to hold your hand while we jump off the high platform diving board together into this vastly different and powerful new understanding of B3? Let’s do it!
Most of us have been taught to ‘balance the Bs’ when supplementing, which discourages the use of single B vitamins in case this interferes with the regulation and roles of others. In reality, outside of a couple of dynamic duos like B12 and folate, there is little concrete information & evidence of this. In the case specifically of B3, however, we now know, the risk of an excess of the most common B3 forms found in supplements and fortified foods, results not only in disruption of other nutrients but imbalanced B3 biochemistry itself. Given B3, in its coenzyme form NAD+, is regarded as highly valued currency in the prevention of many diseases, as well as the key to our optimal health and longevity, it’s critical to understand the different forms and functions of the various B3 sources.
Don’t know why on earth I would be discussing ‘Glassing’?I have a hunch. I was supposed to be doing a deep dive into Taurine & Glycine & their CNS effects for the latest Update in Under 30 and due to a technical glitch we produced a software generated transcript from my first attempt at the audio recording. We’ve never done this before and it seems to suggest, I have an accent and I’m a little mortified. I wasn’t under some delusion that my utterance was universal…my speech narrows my origins to certainly the ‘bottom of the globe’, but, ‘Strewth Sheila, how does any of yous guys understand me??!’
So we’re giving away 3 free copies of this recording to the first 3 individuals who can correctly translate the following from that transcript!:
“In fact, if we go back to their chemistry, you might recall that Glassing, well I refer to it as the naked amino acid. It refers to the fact that Glassing is the amino acid in its most stripped back form. It actually doesn’t have a side chain, which of course all other aminos do. So therefore it doesn’t have eyes and ears. It doesn’t have an Alan O’Day form.”
🥴😵😬
What?! Yes it took me a while to work it out…and I WAS THE PERSON IT WAS QUOTING!! So while I am currently using a medium released from my regional rhino-challenged speech, let me tell you why I am right into ‘Glassing’ as CNS support and as a sleep aid for many patients. Ever listen to the long list of enviable actions Melatonin has on the brain and think…’gee I wish we had something that wasn’t a hormone that could do that?’…hello Glassing, I mean Glycine. SCN sensitising, circadian entrainment, sleep architecture improvement without being a sedative or hypnotic…just to name a few. And guess what? The overlap between these two even extends to their behaviour within the upper GIT! Both of course being shown to be helpful in aiding the healing and recovery of function and integrity in the stomach. What else dose it do and how can we use it to its fullest benefit? The answers are in our latest instalment, A Fresh Look: Taurine & Glycine In The CNS.
And you’ll be pleased to know, the transcript experience has certainly got me paying more attention to my enunciation than ever before. So you’ll understand every word!
Maybe my parents really were just being kind when they said, ‘Everyone sent their kids to elocution lessons back then, it wasn’t because we thought you specifically needed help” 🤣😂
Both taurine & glycine have a claim-to-fame as amino acids that effectively calm an over-revving brain, via their net inhibitory actions within the CNS. They achieve this via different means and while in some circumstances, one, either or both will is the result of differences in the regulation of their BBB transfer, pharmacokinetics, as well as add-on benefits or detractors, unique to each. Learn how to use both of these powerful and affordable mood-modulators, to their fullest, and be more able to know ‘which one when’, by listening to this latest narrative review.
The latest Update in Under 30 has landed!!!
You can purchase Take A Fresh Look: Taurine & Glycine in the CNS here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
That’s not a word you hear often spoken by people practising nutritional medicine. Which is odd. I mean outside of the whole, ‘I’m not good with sulphites so I just have to add these magic drops into my glass of red so I can knock back my share,” often overheard at our conferences… it’s like this essential macromineral, pivotal to human health for things like barrier function, antioxidant defence and our basic ability to create the white cells for immune defence (for that matter), detoxification, musculoskeletal tissue integrity etc has just not received its due attention from us. Not entirely surprising given 1) there’s no RDI and 2) there’s no lab test to assess an individual’s status and how about 3) because we were never taught about it!
But the biggest ‘call to action’ here is that, in spite of items 1, 2 & 3, we’re ‘prescribing’ Sulphur Strategies all the time!
Take one of my favourite examples;GAGs. Glycosaminoglycans like Glucosamine sulphate (not the crappy, found to be not as effective, other forms that we now see more commonly) hit the headlines back in the noughties as an effective arthritis remedy. This is one of the 100s of our body’s ‘end products’ of its endogenous Sulphur Stream. We naturally make this in adequate amounts to ensure the integrity of our joints (and many other tissues of course!) when we have enough Sulphur in the ‘top pool’ (organic Sulphur) to trickle down to the 2nd pool (Inorganic Sulphur), therefore creating a constant essential supply of something known as ‘the universal Sulphur donor’ – ‘PAPs’, to its friends 😉 Like a waterfall, it helps to have a good flow from the top to increase the likelihood we’ll have anything to ‘show’ at the bottom.
So when we give a patient Glucosamine Sulphate it may well help. Or not. But did we ‘treat the cause’ of their Sulphur problem? Should we have treated higher up, increasing the size of either the organic or inorganic pool to have improved and widened the benefits for their health? Or, as is equally common, actually identified why someone might need more Sulphur than most – due to increased demand and losses?
Herein lies my reason for liking this particular Sulphur story somuch. The common medication that places the highest ‘demand’ on Sulphur (due to its need for detoxification) is paracetamol. There’s no debate regarding this – just absolute scientific consensus. NSAIDs and steroids also negatively affect the Sulphur status of individuals, as does Vitamin D deficiency and chronic mild metabolic acidosis. Now how commonly are these phenomena co-occurring in our patients afflicted with arthritis? And traditionally of course, what was the remedy for arthritis? Sulphur springs.
Unseen Sulphur – Time To Take A Look If you don’t have a clear picture of the gross daily requirements, determinants of altered individual needs, sources, regulation & associated deficiency picture of Sulphur, you’re not alone. Turns out this essential macromineral remains ‘unseen’ by most, even though you’re probably writing prescriptions every day that have Sulphur as their key component. From the simple: Taurine, N-acetyl cysteine, Protein powders, to the sublime: Brassica extracts & concentrates, N-acetyl Glucosamine, Alpha Lipoic acid etc. In order to use these Sulphur strategies successfully and safely, however, we need to fill in the missing detail on its metabolism, the difference between the ‘organic’ and ‘inorganic pools’, how regulation regularly goes wrong even in those seemingly consuming enough and how to balance the risks of this reactive medicine with its substantial therapeutic value. This recording comes with a great clinical tool to help you, at last, see the Sulphur strategy most indicated for your patient.
You can purchase Unseen Sulphur – Time to Take a Lookhere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
I say: Biotin, Broccoli Sprouts & Bone Broth You say….?
If you said: ‘Sulphur’, go directly to the top of the class, passing ‘Go’ & collecting $200 on your way!🤓 If you nervously said…”I don’t know, they all start with ‘B’ ?”, you are not alone. In fact, most integrative health professionals aren’t aware of the Sulphur Strategies they’re using, probably, everyday. But it’s time we all were.
How about this list? Glycosaminoglycans (GAGs for joint, gut etc tissue integrity), Cerebroside Sulphate (Myelin), Metallothionein, Glutathione, Hydrogen Sulphide (H2S), Co-Enzyme A, Lipoic acid, SAMe, are just some things Sulphur is essential for.
I could go on…and on and on. You see Sulphur, in spite of being an essential macromineral (adult dietary requirements > 1g per day) and critical to health, remains largely unseen. Often we don’t know when we’re writing patient prescriptions that actually we’re using a particular vehicle for Sulphur and therefore we’re also not able to discern which, of the very long list of options (dietary and supplements), makes the most sense in this patient at this time. We’re not to blame, not many ‘possess the power’ to see it, it seems. Por old essential, irreplaceable Sulphur doesn’t even have an RDI. But the time has come to take a good look. We need to know how patients are able to meet their needs, who needs more and how, very commonly, someone who is seemingly ‘consuming enough’ may still exhibit a functional Sulphur deficiency with poor musculoskeletal tissue integrity, low white cell replication capacity or higher oxidative stress load etc and in those who do have a shortfall, how to treat successfully & safely. Who needs a top down approach (more protein, methionine, cysteine, bone broth) and in whom would that be a risky path and using ‘downstream’ Sulphur products instead would be a better balance of pros and cons?
Because all Sulphur needs to be handled with care.
That’s right. Like other highly chemically reactive minerals, with reactivity comes risk – a great potency that requires careful consideration of both form and dose, so that we can harness this power for good not…well evil’s a bit strong…but how about, for not-good. I’m a bit of fan of Sulphur and using Sulphur strategies in my patients. I think it has interesting echoes with our past: the ‘healing’ waters of a Sulphur Spring and of course even further back the old ‘brimstone and treacle’ medicine of eons ago. This paper by Nimni in 2007: Are we getting enough sulfur in our diet? got me thinking about Sulphur again in a contemporary context, over a decade ago, I’ve done a lot more thinking, researching and prescribing since then but it seems that Sulphur still remains ‘unseen’ by most. But with the rise and rise and rise of popular Sulphur-based supplements (alpha lipoic acid, GSH, N-acetyl glucosamine, Brassica & Allium extracts and concentrates, N-acetyl-cysteine etc) I think it’s time to talk.
If you don’t have a clear picture of the gross daily requirements, determinants of altered individual needs, sources, regulation & associated deficiency picture of Sulphur, you’re not alone. Turns out this essential macromineral remains ‘unseen’ by most, even though you’re probably writing prescriptions everyday that have Sulphur as their key component. From the simple: Taurine, N-acetyl cysteine, Protein powders, to the sublime: Brassica extracts & concentrates, N-acetyl Glucosamine, Alpha Lipoic acid etc. In order to use these Sulphur strategies successfully and safely, however, we need to fill in the missing detail on its metabolism, the difference between the ‘organic’ and ‘inorganic pools’, how regulation regularly goes wrong, even in those seemingly consuming enough, and how to balance the risks of this reactive medicine with its substantial therapeutic value. This recording comes with a great clinical tool to help you at last see the Sulphur strategy most indicated for your patient.
The latest Update in Under 30 has landed!!!
You can purchase Unseen Sulphur – Time to Take a Lookhere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
The first time I saw a set of lab results was when a patient brought them in to her appointment. True. In spite of the comprehensive training I’d received in nutrition and biochemistry and pathophysiology my undergraduate did not include one single lesson on lab interpretation & now here I was faced with some badly formatted inkjet printed document full of numbers I was supposed to make sense of. Was the patient right to expect me to be lab literate?
We profess to be proficient in identifying and correcting nutritional deficiencies, as much as, cardiovascular risk, chronic inflammation, methylation imbalance etc etc so surely these ‘numbers’ are essential to informing our baseline understanding of & decision making regarding the management of our patients, as well as tools for monitoring their progress & safety.
Let alone the knowledge we need to work collaboratively with other health care professionals and show ourselves to be the asset that we are.
And herein lies the golden opportunity, I believe. Most of us do possess excellent foundational knowledge in nutritional biochemistry etc, much more so than other health professionals, who are ordering and seeing these results routinely, they will often tell you this themselves. And while more recent naturopathic, nutritional & herbal medicine graduates have had some basic orientation and education in pathology, are we really making the most of this powerful marriage of knowledge areas? What would we see, if we made it our business to view the same labs?So much more.
We can see warning signs well before the diagnosis, we can see the process behind the emerging or established pathology rather than simply a disease label, and accordingly, the individualisation of our patients’ presentations and their prescriptions.
But first we need to learn our labs.
That very first patient who turned up with results in her hot little hand started me on this path to lab literacy. Later, I was lucky enough to find a kindred spirit & mentor during my time at SCU, with Dr. Tini Gruner and then Dr. Michael Hayter, whom I co-presented my first diagnostics course with many years ago, and every day my patients and my mentees’ deepen my understanding. This path to lab literacy goes on forever I suspect, but with every new corner I turn, I am reminded of and rewarded by all that it has gifted me and my patients.
I’d like to share that gift with you through stories filled with new favourite characters, like ‘Mr More More More Monocyte’ above, engaging animations, loads of real cases, heaps of humour and plenty of practice in pattern-recognition, that make remembering, what can be very detailed content, doable.
In other words: The MasterCourse in Comprehensive Diagnostics I is finally here as a self-paced learning program you can undertake yourself. We know you’ll get as much out of it as those who attended live:
“I thought my pathology skills were pretty up there until I did Rachel’s Diagnostic MasterCourse! Nothing like being knocked off my perch by a literal avalanche of new information, especially when it comes from the most commonly tests that we all use so often. The course has beena fantastic learning opportunity for me, and has since helped me pick out many intricacies in cases that have previously been missed.”
– Rohan Smith | Clinical Nutritionist
MasterCourse 1: Comprehensive Diagnostics is a self-paced online program Gives you access to 24+ hours of streamed video presentations, 2 x Bonus Update in Under 30 episodes (The Calcium Conspiracy & Using Urea to Creatinine Values for Protein Adequacy) PLUS resources, a template and pdfs of all presentations. This package includes $200 worth of bonus material and remains forever in your online account. You will also receive access to any future updates of resources and our template. More information can be found here.
This is a pre-requisite for MasterCourse II that will be delivered live in 2021.
Well, obviously(!)…this has been a year heavy on pathology interpretation for me and the huge number of practitioners who’ve just spent the last 6 months taking that learning journey with me. I celebrate and congratulate them all for their commitment to their own professional development and also their investment, in what is arguably, the most potent yet overlooked set of skills of any health professional… the ability to read bloods. Basic bloods. Mainstream labs. No…but to really read them. Backed by all the scientific understanding about what these parameters actually are, how they perform and what they (dis)prove e.g. subclinical inflammation and ramped up oxidative stress – not an informed guess but mappable…right there but where no one else can apparently see it! But I digress!
Actually what I wanted to discuss was the whole erroneous notion of ‘normal’.
No, I am not speaking from the heart about my personal quirks, sense of humour or dress sense but rather the incorrect assumption that a reference range defines ‘normal’ and that our answer for each patient and each result is, a Yes or a No!
In this brilliant article by Whyte & Kelly published in the BMJ they spell out this falsehood succinctly. They note that the term ‘normal range’ has slipped into medical language from the misunderstanding that all lab results follow a Gaussian (aka bell shaped curve & later referred to as ‘normal distribution’) pattern but many simply don’t. So for some parameters a result near the ‘middle of the reference interval’ constitutes aspirational whereas for others it spells danger. Add to this, that these reference intervals are mathematically determined to reflect the expected values of 95% of your patient population (mean +/- 2 SD either side) so…that means the chance of a YES…”Your patient’s results are ABNORMAL!”… is just 5%. And hey…who said all the values within the reference range are all equally “normal” or better yet, healthy?! Not these authors, nor I, nor the praccies who’ve just done our course. So while, in many regards, these goalposts are too wide, they are also too narrow – typically only representing a subset of adults age-wise and Caucasians, yes they are both ageist and racist (yep, I said it!). And if our practitioners have learnt anything it’s about keeping an ol’ eagle eye on the sneaky intra-individual shift! Only spotted, of course, if you know your patient’s normal (not theirs compared to anyone else…just theirs) and then spot a shift. [I can hear they’re shushing 🤫me…they’ve got it already, alright!!]
So this is music 🎻to my ears, from Whyte & Kelly: “The intraindividual variation in laboratory values is usually much smaller than the interindividual variability (ie, the variation in the population). Variation in the concentration of an analyte, if significantly outside of a patient’s usual values (but still within the reference interval), could be a sign of early or latent disease”
So if you want to tap into the power of pathology…start with Whyte & Kelly, maybe even dip your pinky in the pool by checking out Accurate Pathology Results Interpretation Starts Here – an easy little 1.5hr kickstarter…or jump right in the deep end with the rest of us pathology reading polo players and sign up for the MasterCourse 1: Comprehensive Diagnostics for some DIY summer fun 🌊
ps I know your type and know that is EXACTLY the kind of weird nerdy thing you have planned for your break…you should see my summer fun list!!! 😅
MasterCourse 1: Comprehensive Diagnostics is a self-paced online program due for release in December. The course has pver 18 hours of video presentations plus 2 free bonus sessions 1) Accurate Pathology Interpretation Starts Here and 2) Patient Pathology Manager and access to resources and tools within, for your own use. This is a pre-requisite for MasterCourse II that will be delivered live in 2021.
This skillset has been found by many to be biggest ‘game-changer’ in Integrative Health You can view the full course outline here.
I talk so much about iron, I feel like I’m cheating on my life partner (Zinc)…but these two are arguably the main mineral deficiencies we encounter most consistently in our patients and, don’t tell Zn, but quite frankly, in terms of who’s more well recognised out there, Iron throws some serious shade! But the truth is they’re a ‘twofor’, as a result of their similar distribution in food, with both demonstrating significantly better bioavailability (read: virtually double) from flesh foods etc, ‘Watch out, she’s on the attack again!’ I can hear the V’s (vegetarians and vegans) say and yes I think you see this one coming…but I think it’s possible to be pro moderate meat, without being, antiV.
Ethical and environmental aspects aside (just momentarily) it is hard to argue against the nutritional benefits from moderate meat for most patients.
I tried, trust me. Put my own body on the line (and my babies) to be a vegetarian for over a decade. But as the wheels fell off for me, I noticed them falling off for so many others…and these were people who were educated, with a capital ‘E’ and putting serious ‘E for effort’ into substitution etc Not everyone of course – but a LOT of women and occasionally some men. There was no denying their ‘iron hunger’ (high serum transferrin), their movement towards microcytosis (however slight that ‘smallifying’ may be…we don’t wait for anaemia, right?), their poor zinc status and more importantly, the clinical chaos of impaired immunity, some cognitive or mood issues that presented, as a result. I went back to the mineral manual, back to all the science that helps us to understand these minerals especially in a modern dietary context.
Ah yes…meat has become marginalised in our diets compared to those of our yesteryear selves (ABS data) while our consumption of potential mineral inhibitors…you know, all the good, but bad, but good foods, like legumes and grains and green tea and and and…has risen…especially among the kind of clients who come to see us, right?
Which ultimately leads to a lower iron ‘income’ with the same outgoings, again especially for menstruating, pregnant & breastfeeding women.
The books don’t balance. (So then…IV Fe to the Rescue???)
Bite me…it’s just science. There have been some wonderfully thorough studies on this very issue and thoughtful discussions. This study in particular, by Reeves et al, of Australian women in their 20s followed for 6 years to 2009, argues that just a 1mg/d increase in heme iron from flesh foods could reduce susceptibility to the subsequent development of iron deficiency amongst omnivores. So while the median daily intake of fresh red meat in these women was just 39g/d, their analysis found that an additional 70g of lamb or 60g of beef…or about 140g of chicken and 250g of fish if you prefer white over red, appeared to be the positive tipping point for women and their ability to stay iron-replete. Well below ‘dietary guidelines’, nowhere near the scary cancer correlations (which of course may be more about fat or nitrates or ??). Moderate meat intake, right? Just saying. And don’t worry, I know. The only thing worse than an evangelical ex-smoker is a rambunctious reformed vegetarian 😂
Need A Manual on Minerals?
Minerals represent a critical tool in naturopathic nutrition and there has been an explosion of research in this area over the last 10 years. In order to optimise patient care, practitioners need to keep up with the constant stream of information, updating their previous beliefs and understanding in the process. This seminal 7hr seminar (!!)…yes…seriously..it’s THE MANUAL..is designed to facilitate and accelerate this process of review and re-evaluation via a fresh look at the key minerals iodine, selenium, iron, copper, zinc, calcium and magnesium.
When I deliver foundational nutrition training to GPs I talk tough. It’s a tough field, right? Compared with the relative certainty of pharmaceuticals, their established pharmacokinetics, their sophisticated delivery systems to ensure high bioavailability…trying to fix micronutrient deficiencies in patients can feel a lot like you’re trying to perform minor miracles. Take iron for something different, its homeostasis pivots on its tight regulation at the gut wall – and this is a wall that is very tight!! At best you get about 10% of a supplement taken up, at worst you get none and the harder you push & the higher you go with your dose…the lower the fractional uptake. Tough stuff, right?!
It’s about at this point in my talk I read their collective minds and say, “I know, you’re thinking, oral supplementation is for suckers – what about we bypass that road block and use IV?!” [Ok, I definitely use nicer words than this]
And then I put up a list of pros and cons about IV micronutrient repletion: ‘100% bioavailable’ & ‘Bypasses the body’s regulatory systems’, go on both! You see, time & time again we discover, when we think we’re outsmarting the body, it still manages to outsmart us. There are some exceptions to this – some nutrients (Vitamin C) and some contexts (late pregnancy iron deficiency) but the broader promise of ‘rapid replenishment’ for everyone, in your lunch break, via an IV infusion..is not realistic, responsible nor without risk. Don’t get me wrong, I am an advocate of appropriate IV Fe use and have encouraged a small fraction of my patients to take this path. However, given the dramatic rise in prescriptions for this since 2013, I think it’s time to stop and seriously review each element: In reality what does it achieve and in whom is it a responsible recommendation; Was a risk benefit analysis performed for & communicated to each individual & was the remaining risk mitigated?
Think anaphylaxis is the major concern? It might be the most lethal but there are more serious concerns due to higher incidence with newer preparations.
So, how well do you know your different IV iron forms, and their predilection for potential problems? And have your answers ready to all the questions raised above? In order for all involved to make an informed choice (both practitioners and patients), we must.
You’re welcome 😉 and hey welcome back to tough talkin’ Tuesday…
While rates of iron deficiency and related anaemia continue to grow, the increase in prescriptions of IV Fe have expanded exponentially in western countries. What is behind this change in practice regarding how we treat iron deficiency and does it match with responsible prescribing? Do the benefits always outweigh the risks? And while we’re on the topic, who is most likely to benefit and what are all the risks? In light of a current class action in the US, relating to a lesser talked about adverse event associated with IV Fe and recent complaints here in Australia against GPs, allegedly due to inadequate information to enable informed patient consent…it’s time to answer these questions and more. When is IV Fe a means of rescue and when is it a risky repletion strategy with no evidence of advantage?


 Burning, tingling, crawling, buzzing, humming, zapping, pins & needles, numbness:
Burning, tingling, crawling, buzzing, humming, zapping, pins & needles, numbness: