The debasing of BMI as a stand-alone assessment of weight is long overdue given its significant limitations and lack of meaningfulness with respect to overall health. This coincides with a bigger societal and cultural shift towards inclusivity which involves redressing bias against people with diverse body sizes and compositions.
And how do we, as integrative health professionals, continue to uphold our principles of prevention and treating the cause when excess adiposity may be a very real contributor? While ensuring we ‘see’ and treat each individual in front of us, not our assumptions about adiposity, not our body size bias nor blind spots?
One part of the answer: read and be led by their lab results – because pathology is nothing if not personalised.(more…)
The builder responsible for my reno arrived one day with a frown. When I asked him what was wrong – he said he’d just had his second high PSA result and now the doctor wants him to see a specialist. It was apparent that he felt this was a real cause for concern. Talk about raising a red flag to a bull 🚩🐂 Yes, of course you know what followed. I insisted on reviewing the results myself only to find the reference range provided on his report was not specific to his age – and if we adjusted up for this (as the science supports) his result is just 0.5 ng/mL above the expected value!
Now, remember he is a builder so, ‘0.5’ in his mind might well be on par with 5mm which apparently is a big deal…or so he keeps telling me every time I try asking for some weird unconventional thing for my roof, windows, walls, whatever!! So I still had to provide a little bit more detail for him to get perspective and to understand the true meaning (and lack of scary meaning) of his results.
This however is just a micro-illustration of a big problem in pathology – we all risk a lack of perspective but if we can get it back, aids us to see that seemingly ‘normal’ results are sometimes a concern, and so-called ‘concerning’ ones, non-significant. The incredible patient insights that can be gained from being able to measure & monitor actual quantities of things in our patients; nutrients to novel disease markers, precursors to end-products, all comes down to understanding how their values compare with…with what? With someone of a different sex and age? With ‘all adults 18-108!’? With any other pre-menopausal woman regardless of reproductive or cycle stage? With ‘the average’ adult given that this current definition is overweight & unwell? Who are we comparing ourselves and our patients to?
When I undertook my undergraduate training many moons ago – there was no education in blood test interpretation. But as soon as I got out into practice I found my patients had all these bits of paper filled with magic numbers that I felt certain might offer me insights and a deeper understanding of their whole health – and how to best help them.
I desperately wanted to decipher this foreign language and made it my mission to do so. I was lucky enough to meet and be paired with a kindred spirit, Dr Tini Gruner, who happened to be my supervisor when I returned to undertake my honours thesis. Together we pooled our knowledge, sought out & shared with each other yet more and found that, together with comprehensive case taking, it provided excellent scaffolding to our work-up of patient cases. Better than that, it created this baseline for patients, identified clear treatment objectives and we could measure the success of our interventions based on how their results did (or didn’t) respond to our interventions. It was (and still is) a totally thrilling way to practice.
We talk about there being both an art & science to medicine generally and certainly an integrative approach. Without the benefit of pathology interpretation, I felt too at sea at times, without quite enough of the science to check the accuracy of the ‘art’ and my speculation.
Being able to understand what each individual result represents and reflects, to know how to form meaningful comparisons – with external reference ranges that speak to healthy individuals of the same sex & life stage, derived from rigorous research – and also form a comparison with the patient themselves, to pick up on the most subtle and significant early alerts to an emerging pathophysiological or healing process – is the skill, I believe, we all need in health to complete the toolkit. That’s why I made it my mission to learn the language of labs, from a conventional & integrative interpretative perspective, and then to share this learning with everyone wanting and willing to take this baton from me (& Tini) and run with it 🏃♀️🏃
MasterCourse I: Comprehensive Diagnostics. Click here to read more and here to purchase it.
*Please note that this is the place to start for everyone wanting to add preventive diagnostics to their tool kit. It is also the pre-requisite for MasterCourse II, so make sure you have completed this before continuing with MasterCourse II: Thyroid and Adrenal Diagnostics.
MasterCourse II: Thyroid & Adrenal Diagnostics. Clickhereto read more and here to purchase it and sign up for the Free Watch Party commencing tomorrow, 3rd August 2023 with is included with each purchase of the MasterCourse II.
Just as optimal integration of lab results into our patient work-ups makes ‘the invisible visible’ we thought we might make visible some of the everyday Q & A that we engage in with wonderful practitioners who are fast becoming Diagnostic Divas & Divos.
Praccie email arrives with subject header ‘Graves Help’ (or is that ‘Graves…HELP!’🤔)
Practitioner: I have a Grave’s patient who required Propylthiouracil (PTU) for a few months from late 2022 until Jan 2023 which obviously took her thyroid in the opposite direction (see labs). Following a miscarriage last year, she has conceived and is around 6/40 and her current TSH result has come in at 3.3mIU/L, her TPO Abs > 1000 and she also has low-level Tg Abs (TRAbs not measured this time) and this is what she just said to me:
“I just had my specialist session this morning – and she has put me on thyroxine (50mcg) as my thyroid is quite low. I also asked her about the prenatal vitamin and she said it was safe for me to be on iodine at this time, as the Graves isn’t present and baby needs it for the development of its own thyroid.”
Oh gawd! Preg? Iodine? Graves? Antibodies? Antenatal or postnatal aggravation?!
Is there an UU30 I can listen to to help me understand this?… sorry for the panicked email…
This is not about body shaming nor body positivity. I understand the crudeness of the body mass index, as a measure of (un)healthy weight – let alone (un)healthy muscle mass, so I don’t use this as a stand-alone assessment of weight, nor rigidly adhere to the categories it allocates individuals. With only minor recognised racial adjustments for BMI, I also recognise our concept of ‘healthy weight’ is incredibly whitewashed with minimal regard and consideration for clear ethnic and racial differences in physique. Patient’s lab results tell the real story. It’s in their results that we can discover someone is thin-on-the-outside-fat-on-the-inside (TOFI) or FOTI. These are patients whose BMI, WC,WHR, Body fat% etc identify them as obese – yet there is not a whisper of what I call ‘Adiposity Patterns’: no subclinical inflammation, no reduced glucose tolerance or actual IR, no raised transaminases that we expect to correlate with girth and the corresponding fatty infiltration of their liver. In this, as in so many other aspects of clinical practice, we are reminded to see each individual, individually.
AND if we adhered to this always, listening unfiltered to the whole health story and letting the labs speak, we would not miss those patients in whom unhealthy weight really is the most important underpinning, & all impacting, issue. And we are not doing our job, when we don’t.
I mean – we all know the detrimental effects of excessive adiposity – that’s like Pathology Unit 1 topic 1, right? I know we know it. Yet there are so many reasons why we might down-play, step-around, or even ignore its enormous contribution in our patient work-up and certainly the discussion that follows with our patients. That too is a no-brainer. Who wants to say to someone whose come seeking your help, as an explanation for their complex health concerns, ‘There’s no zebras here just a horse – one really over-weight horse!’ Knowing too that unhealthy weight results from the most complex constellation of factors (biopsychosocial) unique to each individual and that change in this health determinant, is arguably the slowest and hardest to sustain. But how are we serving our patients if we don’t?.
A practitioner presented this case of a 48yo F seeking help with the work-up: Self-reported inability to lose weight after 1st pregnancy = ‘obesity’ ongoing – now BMI 33.1 –> 25yo Reflux & Hiatus hernia Tx Omeprazole initiated – ongoing –> 26yo Depression Tx Venlafaxine initiated – ongoing –> 30s Back and other musculoskeletal injuries Tx Surgery & Opiates – ongoing –> 40s Hypertension & elevated resting HR –> Last 12mo – changes in Mx cycles suggestive of perimenopause & substantial weight gain
This patient didn’t ‘have’ any lab results but I think I can make an educated guess about how they would look and in particular whether they show the characteristic ‘adiposity patterns’ I mentioned before. What was my first thought about the most impactful element of the case? Obesity. What was my second thought? Where is all the weight (diet & intervention) history that would help us to understand how she is where she is, right now? We didn’t have any. The practitioner informed me that the patient was ‘not very interested in talking about her weight’ – in fact, according to her, it didn’t seem like losing weight was one of her goals. Now this could be several things: the fear of judgement, even her own self-loathing, the paralysing awareness of the enormity of such a goal, the dashed hopes of the past, or it could just be that her weight, as the key negative determinant of the majority of her health concerns & quality of life, has just never been brought to her attention, nor the connections explained to her in simple accessible language. So over to us, right?
There were other health determinants at play in this patient but the centrality of the adiposity was undeniable & the practitioner said this was the greatest take-home. She’d been ready to don some jungle gear and go hunting some zebras – but there was a horse right here in front of her and that could not and should not, ever be ignored.
What else became apparent was the lack of knowledge & skills regarding how to take a comprehensive weight history & why this is crucial. Not only for this type of unhealthy weight, the underweight require exquisite attention, as do those with a more labile weight than expected as an adult. This brilliant article by Kushner et al from 2020 is a total gift in that regard and a must-read for every clinician. We feel uncomfortable asking about certain things when a) a patient feels uncomfortable which is usually because b) we are uncomfortable and this ultimately comes from not being clear about WHY this information is so important and HOW this will ultimately enable us to better help THEM.
This is the very latest, comprehensive review of the key aspects of thyroid assessment that will revolutionise your understanding of thyroid markers. Gain a clear understanding of how to provide the best, most individualised, thyroid management by learning to read the real story in each patient’s pathology patterns. Boost your knowledge and confidence looking at TFTs, rT3, thyroid antibodies & related nutrient patterns, as well as AITD, environmental EDCs, HPA driven HPT issues, thyroid nodules, the impact of dietary macro- & micro-nutrient imbalances and much more!
This 4 part series provides over 10 hours of the very latest research & findings, punctuated with real case studies, that will both contemporise and deepen your understanding of all things thyroid, with a bonus recording on Adrenal Assessment.
Any pathology test is only of value if the result produced is ‘real’, or, representative of that individual, right? So the timing of the test is a major pivot point then: do I tell my patient to present for the test, or collect the sample themselves, on their ‘best’, their ‘worst’ or their ‘average’ day? 🤷♀️ Well, that all depends on the question you are trying to answer.
Whenever we reach or refer for a test, we have a question in mind we’re seeking an answer to. But the question always comes in two parts, at least.
Part 1: How much progesterone is she making? Part 2: …When she’s ovulated & her corpus luteum should be most productive?
A third might refine the question you’re answering further by adding another contextual clarification
Part 3,4,5: …When she’s eating her regular diet, not exercising excessively or under extreme stress
Without these other parts – the answer to the first one: How much progesterone is she making (full stop), is hard to correctly interpret, right? By refining and expanding on the full extent of our question, we can be clear about which elements of this patient’s life the result likely reflects. We might say that for her, this time-point, or set of collection conditions, is a ‘real reflection’ of her generally and therefore, representative. But what if she does occasionally undertake a 5 day fast, or train for & compete in marathons? If we were to specifically test during these times, we answer a different question, right? Likewise every time we instruct a patient to present for their blood tests (routine or fancy schmancy): Fasted, Rested, Hydrated and off their supplements – is this sound advice or a misdirection? Well it depends on the individual in front of you and the real question you want answered about them 🤓
Ahhhhh I love rules: both the making of them and the subsequent breaking of them 🦜🏴☠️
The collection conditions for any pathology test – can refine or ruin the question you were hoping to have answered about your patient but is it always appropriate to ask everyone to ensure their preparation for the test was ‘ideal’? What if their real life is far from ‘ideal’ and contrasts dramatically with these ‘conditions’ e.g. they forget to drink water but never alcohol! Or do they run 20km every weekday and 40 on weekends? And why would we tell some patients to stop their supplements prior to a blood-test and not others? If our goal is to ensure any pathology test answers the question we need answered we need to know how to respond to these and other scenarios. This new update is all about keeping results ‘real’ & representative.
You can purchase Fasted, Rested, Hydrated & Unsupplemented? Exceptions to the Rulehere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
Are we doing ourselves out of a job? I’ve been talking treatment plans with my New Grads recently. Given, only recently these were major assessment items in their clinic units, they have been trained to create ALL-ENCOMPASSING (biopsychosocial) prescriptions and recommendations of utterly EPIC PROPORTIONS – to simply prove they know it all. Problem is this doesn’t work in the real world.
Emailing your client multiple pages of advice that covers: a whole sizeable supplement schedule that only a military-training could nail (2 tablets 1 XTID 1 X BID, a liquid, a powder, some with food, some definitely not with food) plus dietary advice, plus hyperlinks to exercise advice, mindfulness exercises and a request for follow up investigations before the next appointment…is…a L*O*T!!
It is also ineffectual – because it completely disregards the human on the other end. Let me ask you this, how much change are you capable of between a first and second appointment, roughly a period of 2-3 weeks? Personally, I gotta say not that much. It took my dentist years to get me just embrace flossing & I don’t think I am an exception! With all the knowledge we possess its hard not to see people as (a long list of) problems (& problematic behaviours) that we translate into, and solve via, a prescription.
Effectively we are saying to patients with this practice model, ‘Go change & come back when you’re done & then I’ll probably ask you to change some more!’ That’s both a big ask and a huge missed opportunity.
I hear from reliable sources over the ditch, that GPs are increasingly referring their patients to, or teaming up with health coaches, rather than naturopaths. Given what I’m observing, I get it. Doctors on the whole only have time (and barely then) for a finger-pointing prescription – certainly not the time and touch-points required to actually support patients with the very difficult thing that is, behaviour change. Nor the skills to truly facilitate patients making the necessary and desired changes – so they outsource this role. But we shouldn’t.
After all – I want to be on my patients’ support bench & health care team always – not a flash in the pan, that blinded them with science or my ‘smarts’ and proved to them in one over-stretching prescription – that naturopathy is not for them, or at least, they’re not fit for the task.
At the end of an information & insight heavy appointment, formulating a list of products and doses for our patients to take can feel like a bit of a ‘tada moment’, like a magician pulling a rabbit out of the hat. “Here is the solution – now off you go!” Research tells us, however, that treatment-plans that are a co-creation between you and your patient – evolving from a discussion that not only allows them a voice, but a major role in the decision making – are far more likely to succeed. While we are the authority on our medicines, our patients are the authority on what makes them tick & what’s likely to succeed, in terms of taste, texture, temperature & timing! This is called Patient Centred Prescribing and together with some other tips tricks and hacks I share with you in this episode, can really increase patient buy-in, compliance and therefore bring your treatment plan to fruition and fulfilment!
Maybe it’s tax-time, just my wintery whinge or a tirade triggered by missing my twins’ 21st birthday due to border restrictions 😶 butI’m sorry for all the shouting of late…about interpreting iron studies, about the copper misinformed etc etc. and my gorgeous new grad mentees copped a full monologue, with links to articles, recordings & the Coeliac Society, when they asked me to expand on why we must exclude coeliac disease before removing gluten from anyone’s diet. I was so glad they asked though! I’m now using my inside voice.
But I don’t want my message to be misdirected and I fear it might be. It’s not you and it’s not me
‘We’ are doing our best. We are working in a field that demands us to be across soooooo many domains of knowledge and information, from the basic & not-so-basic medical sciences, to pathology interpretation, nutrition, herbal medicine and beyond. It’s a lot. None of us are across it all. I’m certainly not. And I’m aware, that the frustration I feel at others’ misunderstandings sometimes is unfair, because I’ve benefited from excellent early teachers all the way through to having a job now, that keeps my head in the research daily. And even still, without a doubt, the gaps & shortfalls I observe and criticise in others, I could have made of myself, earlier in my career. We don’t know what we don’t know, until we know better, right.
It’s them
Who is this ‘them’ of which I speak? Well, 25 years ago when I completed my under-graduate (and walked 10 miles to school in the rain, without shoes or breakfast 👵) I believe I received the training required to be the naturopath that I needed to be. Safe, effective, knowing my scope – which was basically coughs. colds, atopy and risk mitigation for future chronic disease. I never saw a lab test during my under-grad. I would have read a set of iron studies badly and something like ELFTs, like it was Latin. I wasn’t made aware by my lecturers of the critical part I could play in my patients’ lives, either by advocating and advancing correct diagnosis or by obscuring, confounding and delaying it (sorry, still thinking about the gluten debate!). But back then, I think this was appropriate for the time, the state of play of our collective medical knowledge and for the role naturopaths were playing in the health landscape. Not any more.
If you haven’t had a chance to read the extensive research about ‘us’ (Australian nats, nuts & herbalists) published of late, who we are, what we do, how we are viewed and what our patients expect, then you could be in for a surprise.
We’re perceived by many, if not most, of our patients to be a primary health care provider – either flying solo or co-piloting with the patient’s GP (& no auto-pilot function!!!) and as clinicians for chronic comorbid cases not the acute cold. My how times have changed and the question is – has the knowledge and level of competency of those in educational roles & the quality of what they deliver a good fit? Sorry, but if the majority of a large new graduate cohort have left their training with a mantra of ‘we must not diagnose’ and INTSEAD are likely to advocate a gluten free diet RATHER THAN Coeliac testing with the patients doctor first – then we’re falling at the first: Primum non nocere. Sorry,I forgot, inside voice 🙄🤐
This Update in Under 30 recording speaks to the seriousness and primacy of identifying Coeliac Disease in any patient reporting a suspected reaction to gluten and takes you through the latest evidence on the best screening protocol. With an increased understanding about the strengths and limitations of gene testing, serology and biopsy, we have a clear map to follow now. Along the way Rachel outlines 3 additional potential mechanisms for ‘gluten’ reactions amongst our patients, what to look for and how to tell the difference.
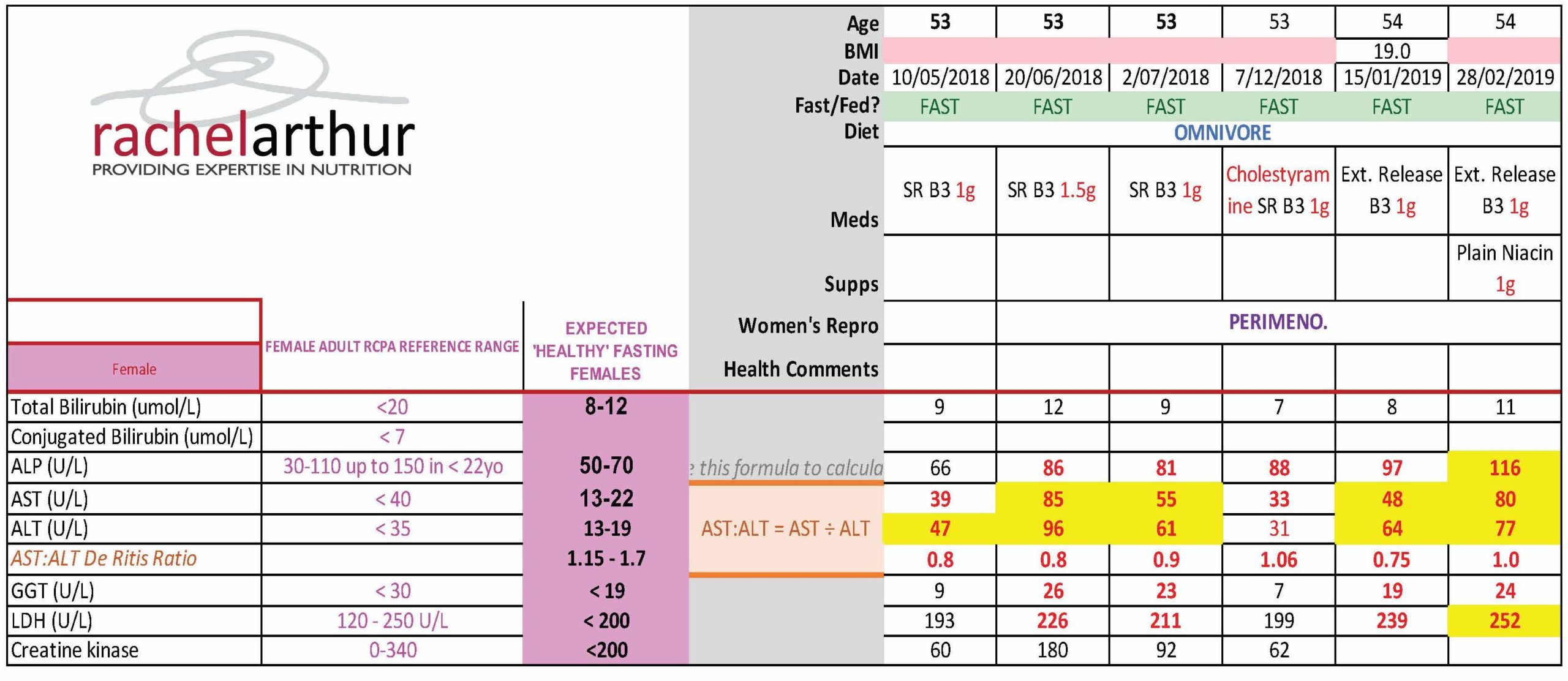
What’s your knee-jerk response to 52Y Lipids Lucy & Liver, whose ALT & AST suddenly jumped above range when she was put on statins? They’re damaging her liver? You’d be wrong. One of the practitioners who undertook the MasterCourse in Comprehensive Diagnostics just graduated with flying colours when she was able to correctly identify the true cause of this patient’s LFT abnormalities, can you?
[Cheeky hint: there is more than one explanation/process at play]
This naturopath now knows her pathology patterns. She knows the interpretation of any liver enzyme must also take into account the movement in other markers, to make meaning of the whole. Because so-called ‘liver enzymes’ are never exclusive to the liver. They are expressed in multiple other tissues and organs – sometimes at equal concentrations to their liver-level (e.g. ALP and bone). For some, even referring to them as a ‘liver enzyme’ is a mislabelling of sorts, with minimal expression in the liver itself compared with ubiquitous distribution all over the body (e.g. GGT & LDH). Of course this is both a blessing and a curse. A curse if you make the mistake of only interpreting their levels through a ‘liver lens’…a blessing if you know when they are flagging problems elsewhere through the specific pattern recognition. So back to Lucy – the statins had induced a rhabdomyolysis not hepatocellular damage. The clues? Significant AST dominance over ALT, above range CK and LDH.
So if the statins weren’t causing increased hepatocellular damage what is that increasingly high-normal ALP pattern all about?
Bones. And again, this practitioner picked it. And then got to win herself some pretty BIG credit and credibility points with all the other health professionals sharing care of this patient by suggesting that they clarify and confirm this by referring her for an ALP bone isoenzyme assay, which answers the question: is the elevated ALP originating from the liver, the intestines or from the bone? Bingo, bones it is! Or was, because this practitioner was able to alert not only the patient but all the other practitioners treating her to the increased bone remodelling taking place, independent of the statin reaction, but part of her perimenopause. Left unchecked this would escalate further of course at menopause and leave her bones in bad shape. This is just one illustration of how we can show ourselves the be the incredible one we are on the shared-care team.
Being lab literate and pathology proficient, sets you apart from the rest and enables you to practice truly preventative medicine. How else would we have known she was experiencing increased BMD loss that may be the start of something truly tragic?
Realise the true value you can extract from the most commonly performed labs. Join Rachel Arthur LIVE on the MasterCourse I: Comprehensive Diagnostics WATCH PARTY This skill is the biggest ‘game-changer’ in Integrative Medicine! Want to know more? Head over to my website here and check out more of the great benefits and bonuses of joining this program This course is a fantastic learning opportunity to identify the many intricacies in cases that have previously been missed.
If I could be granted 1 wish regarding all health professionals, it would be that we were all competent in reading Iron Studies. Think that’s overstating the issue? Or not a bodacious enough way to ‘spend’ my wish? I don’t. Especially when you consider the impact of GPs in this space.
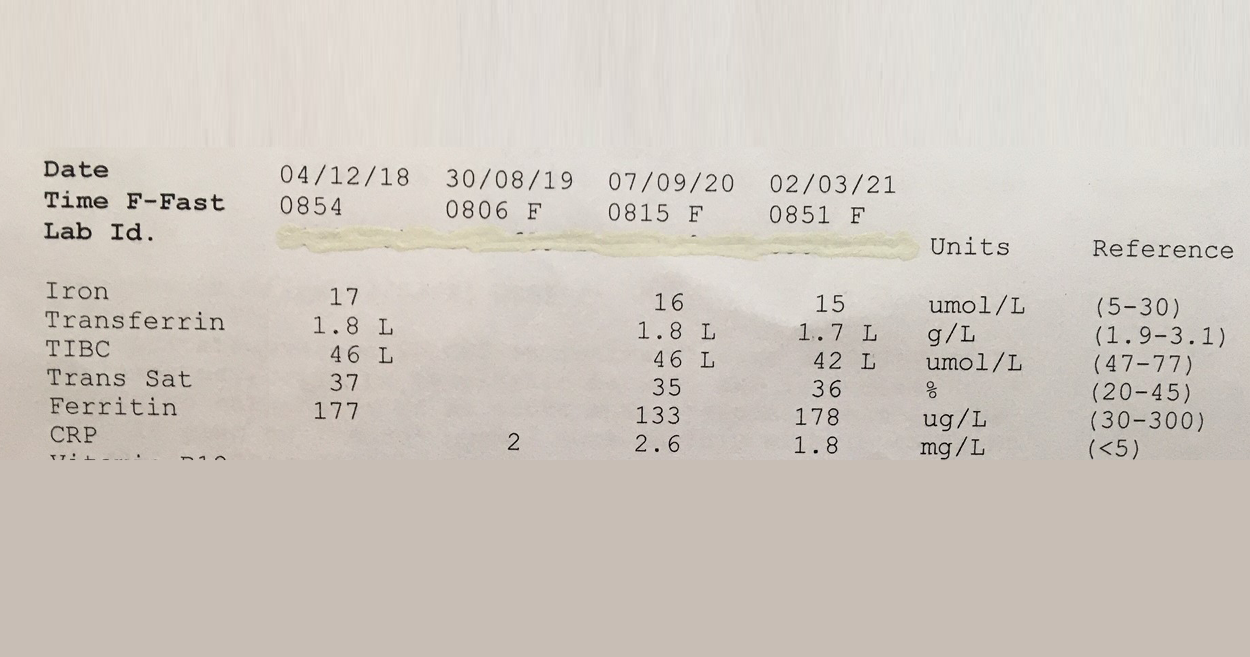
This 57Y male was asked to make a follow up appointment with his doctor, to discuss his ‘abnormal’ results which he was informed constitute Iron deficiency. Consequently he was was advised to start an iron supplement! #@!*
Your thoughts? Revoke this doctors medical licence? Insist on some very du jour ‘re-training’ at the very least? I mean, if you think this Iron pattern flags a deficiency or shortfall, then you’re as good as reading a map upside down and back to front…and written in a foreign language!! The ‘Ls’ in his latest labs flag he has suppressed transferrin, indicative of negative feedback inhibition of GIT uptake of this mineral, secondary to healthy stores or inflammation. And it’s not just that more iron is not indicated but that more iron in fact presents a patient like this with increased and unnecessary risk: to their microbiome, intestinal wall health, even according to the larger longer studies a potential correlation with colorectal cancer risk, if taken long term. Let alone the whole cardiovascular conundrum. Better still this same patient was told a few years back that he might have iron overload! Again the ‘map’ could only have been being read, upside down, back to front to reach such a conclusion!
So the one patient in just a few years by 2 different doctors has been diagnosed incorrectly with 2 different iron issues. Yep.
And sadly I have sooooo many more cases of missed and mis-diagnoses with regard to this mineral. The latest RCPA Position Statement on the Use of Iron Studies, underscores that assessment of iron status and GPs competence in knowing when to do this and how to interpret, is an important part of core general practice. Given it “is the commonest nutritional deficiency state in Australia and is significantly under-diagnosed” This succinct document offers a quick crash course in Iron nutrition for doctors and it hits all the right marks with advice about not ordering ferritin as a stand-alone because “the interactive nature of the three components allows for more accurate interpretation”and this simple but sage advice:
“Transferrin, iron transport protein, tends to increase in ID… A better strategy (than being tricked by Serum Fe) is to report transferrin saturation. A low transferrin saturation in the setting of an equivocal ferritin level is suggestive of iron deficiency. An elevated transferrin saturation is the first manifestation of iron overload.“
I mean seriously, do doctors read these RAGCP resources & recommendations, or is it just me? 🤓😂
Need a rip-roaring review on how to really read iron studies? Or know another health professional who does?!! Consider this Easter Educational Gift Instead of Eggs!! So You Think You Know How To Read Iron Studies?
Overt Iron Deficiency Anaemia or Haemochromatosis aside…do you understand the critical insights markers like transferrin and its saturation reveal about your patients iron status? Most practitioners don’t and as a result give iron when they shouldn’t and fail to sometimes when they should. This audio complete with an amazing cheat sheet for interpreting your patients Iron Study results will sharpen your skills around iron assessment, enabling you to recognise the real story of your patients’ relationship with iron.
The first time I saw a set of lab results was when a patient brought them in to her appointment. True. In spite of the comprehensive training I’d received in nutrition and biochemistry and pathophysiology my undergraduate did not include one single lesson on lab interpretation & now here I was faced with some badly formatted inkjet printed document full of numbers I was supposed to make sense of. Was the patient right to expect me to be lab literate?
We profess to be proficient in identifying and correcting nutritional deficiencies, as much as, cardiovascular risk, chronic inflammation, methylation imbalance etc etc so surely these ‘numbers’ are essential to informing our baseline understanding of & decision making regarding the management of our patients, as well as tools for monitoring their progress & safety.
Let alone the knowledge we need to work collaboratively with other health care professionals and show ourselves to be the asset that we are.
And herein lies the golden opportunity, I believe. Most of us do possess excellent foundational knowledge in nutritional biochemistry etc, much more so than other health professionals, who are ordering and seeing these results routinely, they will often tell you this themselves. And while more recent naturopathic, nutritional & herbal medicine graduates have had some basic orientation and education in pathology, are we really making the most of this powerful marriage of knowledge areas? What would we see, if we made it our business to view the same labs?So much more.
We can see warning signs well before the diagnosis, we can see the process behind the emerging or established pathology rather than simply a disease label, and accordingly, the individualisation of our patients’ presentations and their prescriptions.
But first we need to learn our labs.
That very first patient who turned up with results in her hot little hand started me on this path to lab literacy. Later, I was lucky enough to find a kindred spirit & mentor during my time at SCU, with Dr. Tini Gruner and then Dr. Michael Hayter, whom I co-presented my first diagnostics course with many years ago, and every day my patients and my mentees’ deepen my understanding. This path to lab literacy goes on forever I suspect, but with every new corner I turn, I am reminded of and rewarded by all that it has gifted me and my patients.
I’d like to share that gift with you through stories filled with new favourite characters, like ‘Mr More More More Monocyte’ above, engaging animations, loads of real cases, heaps of humour and plenty of practice in pattern-recognition, that make remembering, what can be very detailed content, doable.
In other words: The MasterCourse in Comprehensive Diagnostics I is finally here as a self-paced learning program you can undertake yourself. We know you’ll get as much out of it as those who attended live:
“I thought my pathology skills were pretty up there until I did Rachel’s Diagnostic MasterCourse! Nothing like being knocked off my perch by a literal avalanche of new information, especially when it comes from the most commonly tests that we all use so often. The course has beena fantastic learning opportunity for me, and has since helped me pick out many intricacies in cases that have previously been missed.”
– Rohan Smith | Clinical Nutritionist
MasterCourse 1: Comprehensive Diagnostics is a self-paced online program Gives you access to 24+ hours of streamed video presentations, 2 x Bonus Update in Under 30 episodes (The Calcium Conspiracy & Using Urea to Creatinine Values for Protein Adequacy) PLUS resources, a template and pdfs of all presentations. This package includes $200 worth of bonus material and remains forever in your online account. You will also receive access to any future updates of resources and our template. More information can be found here.
This is a pre-requisite for MasterCourse II that will be delivered live in 2021.
Key texts tell us, 2nd trimester Serum Ferritin may be between: 2……………………………………………………………………………………….and……………………………………………………………………………………….230 mcg/L But a 2nd trimester Ferritin even > 40 mcg/L is remarkable – and not in a good way🙄 So, ummmm what should it be and why?
Given all the attention iron gets from me alone, you would think we would be a lot clearer and a little ‘clueier’ regarding the answers to core questions like this. But we’re not. Correction, they’re not. Who is this ‘they’ of which I speak, um well, just the dudes in the top level office who write the practice guidelines for GPs, Obs, Midwives etc. Big call I know, but answer these to get my drift:
What is the average Serum Ferritin in healthy women with healthy pregnancies in the 2nd trimester? After all the routine Iron treatment given across numerous countries, in line with the WHO recommendations, is there any evidence that values higher than this have irrefutable benefits for mother or baby? Is there evidence to the contrary, that it can be harmful?
And while we’re busy asking questions that shake the flimsy foundations of the practice guidelines regarding monitoring and managing iron levels in mid-pregnancy – how about we get up to speed with the evidence that shows 1st trimester Serum Ferritin is in fact the most meaningful as an iron marker both in the short and long-run for any woman’s pregnancy. I know, right…this is all sounding very different from the, inappropriately named, ‘normal’, which is to test women at wk28, in the midst of peak haemodilution, and therefore physiological anaemia, and to then send that patient home often with a new diagnosis of iron deficiency and a sense of urgency to ‘fix this fast for you and baby’. In some instances this is appropriate and important, especially women who weren’t comprehensively cared for & whose iron status wasn’t monitored & well-managed in the first trimester. But for so many women, who are just riding the Ferritin-Fun-Bus…they are right on track with looking their very worst!
Couldn’t resist finishing this year of Update and Under 30s with a serious BANG! 🧨🧨🧨
In this continuation of our discussion about better iron balance for mum and baby we now map what is happening in each trimester with regard to requirements and regulation, and accordingly, what ‘healthy looks like’ in terms of both serum ferritin and transferrin, at every time point. This also gives us a clear practice protocol around when and how exactly to treat iron deficiency in pregnant women. Additionally, we review the risks of both under and over-treatment.
The latest Update in Under 30 has landed!!!
You can purchase Pregnancy Iron Balance Part 2 here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
A few things really took up a disproportionate amount of our time & attention in 2020: Zoom, Mask Fashion & Gin based hand sanitiser.On a personal note I need to confess another: Iron. So while my one true (mineral) love remains zinc, iron answer hunting has infiltrated a lot of my days and some nights! There’s no hiding it…3 out of my 12 UU30 episodes this year have iron in the title 🙄 a sure sign its been on my and my mentees’ minds and sitting across the desk from a lot of health professionals in human form. And this affair I’ve been having, like most, started innocently… it started with a just a ‘quickie’, you know a quick question from a well meaning practitioner: “So, what’s expected in terms of ferritin levels across pregnancy?”
There are 2 answers to this. The first reflects the practice guidelines for GPs and obstetricians in most western countries: > 30 mcg/L regardless of trimester And then there’s another that is [ahem] evidence based, accounts for the essentiality of physiological anaemia in pregnancy &, naturally, trimester specific
There’s a big Fe-ar factor at play when it comes to answering the question, ‘Does this woman have enough iron for her and bub?’ Public health and practice guidelines appear to assume we are ‘guilty’ until proven innocent, patients are worried and health professionals are plagued with their own doubts about whether they’re ‘reading this right?!’ I’m sure we’ve all been in the situation where we feel our pregnant patient is doing well iron wise early in pregnancy, only for them to have that routine antenatal 28wk GP/Ob visit and discover a total panic has descended upon the patient and the rest of the health care team, with calls for ‘IV Iron STAT!’ But 28wks is the height of haemodilution right? You know, that time when ferritin, Hb and Hct should look at their lowest, right? There certainly is a limit to how low we want any pregnant woman to go – for her and her baby’s health but that limit is not the one routinely used and the truly evidenced based one is going to shock you. So what? What’s the issues if we are a little Fe-ar based about Fe, resulting in hypervigilance (calling a deficiency when there isn’t actually one) and giving them a ‘boost’ of more iron, surely this is good news ultimately for baby’s iron levels and for lactation and for…sorry what? No?
There’s a U shaped Curve for Iron supplementation & serum Ferritin levels in pregnant women?!!
It starts with a simple enough question: What should women’s ferritin levels be in pregnancy? But the answer will surprise many. There are in fact two. The first reflects the practice guidelines for GPs and obstetricians in most western countries regardless of trimester and then there’s another that is arguably more evidence based, accounts for the essentiality of physiological anaemia in pregnancy & is also, sensibly, trimester specific. To challenge the ‘noise’ and have the confidence that ‘normal’ is ‘enough’, we need to better understand the mother’s protective physiological adaptation of iron regulation and the intricate systems the foetus has to ensure its needs are met. This of course is not without limit, so we need to also be clear about the maternal serum ferritin threshold for negative impact on the foetus and newborn. Getting the balance or iron right in pregnancy for both mother and baby, is perhaps easier than we have been led to believe.
When I deliver foundational nutrition training to GPs I talk tough. It’s a tough field, right? Compared with the relative certainty of pharmaceuticals, their established pharmacokinetics, their sophisticated delivery systems to ensure high bioavailability…trying to fix micronutrient deficiencies in patients can feel a lot like you’re trying to perform minor miracles. Take iron for something different, its homeostasis pivots on its tight regulation at the gut wall – and this is a wall that is very tight!! At best you get about 10% of a supplement taken up, at worst you get none and the harder you push & the higher you go with your dose…the lower the fractional uptake. Tough stuff, right?!
It’s about at this point in my talk I read their collective minds and say, “I know, you’re thinking, oral supplementation is for suckers – what about we bypass that road block and use IV?!” [Ok, I definitely use nicer words than this]
And then I put up a list of pros and cons about IV micronutrient repletion: ‘100% bioavailable’ & ‘Bypasses the body’s regulatory systems’, go on both! You see, time & time again we discover, when we think we’re outsmarting the body, it still manages to outsmart us. There are some exceptions to this – some nutrients (Vitamin C) and some contexts (late pregnancy iron deficiency) but the broader promise of ‘rapid replenishment’ for everyone, in your lunch break, via an IV infusion..is not realistic, responsible nor without risk. Don’t get me wrong, I am an advocate of appropriate IV Fe use and have encouraged a small fraction of my patients to take this path. However, given the dramatic rise in prescriptions for this since 2013, I think it’s time to stop and seriously review each element: In reality what does it achieve and in whom is it a responsible recommendation; Was a risk benefit analysis performed for & communicated to each individual & was the remaining risk mitigated?
Think anaphylaxis is the major concern? It might be the most lethal but there are more serious concerns due to higher incidence with newer preparations.
So, how well do you know your different IV iron forms, and their predilection for potential problems? And have your answers ready to all the questions raised above? In order for all involved to make an informed choice (both practitioners and patients), we must.
You’re welcome 😉 and hey welcome back to tough talkin’ Tuesday…
While rates of iron deficiency and related anaemia continue to grow, the increase in prescriptions of IV Fe have expanded exponentially in western countries. What is behind this change in practice regarding how we treat iron deficiency and does it match with responsible prescribing? Do the benefits always outweigh the risks? And while we’re on the topic, who is most likely to benefit and what are all the risks? In light of a current class action in the US, relating to a lesser talked about adverse event associated with IV Fe and recent complaints here in Australia against GPs, allegedly due to inadequate information to enable informed patient consent…it’s time to answer these questions and more. When is IV Fe a means of rescue and when is it a risky repletion strategy with no evidence of advantage?
Given1 in 8 Australians right now are taking an antidepressant, chances are you’re seeing a lot of clients on these, especially the SSRIs. Erica McIntyre (fellow naturopath) and colleagues, found that in fact, mental health diagnoses affect about 43% of individuals who choose to seek help from a naturopath or herbalist, so clearly this is across all of our waiting rooms. Accordingly, by this stage in your clinical career you’ve probably seen more than 1 patient taking the identical SSRI – e.g. Citalopram (aka Lexapro or Cipramil) Have you also by now, therefore come to ‘expect the unexpected’, when it comes to patients on the same prescription, in terms of ‘weight effects’? The majority not reporting this to be a major concern or issue but the occasional client, experiencing such significant weight gain, they may even have seen this as a reason to discontinue the medication. So what’s up with that then? Don’t we all wish we knew for certain! But getting our heads around the potential mechanisms is important for our patients, in terms of making more informed choices, as well as offering us insight perhaps into their neurobiological nuances.
Some of you will know, this used to be my place of business.
I have a background in the pharmaceutical industry, specifically psychiatric meds, more specifically SSRIs and even I find every time I duck-dive back into the literature I come up with more ‘fish’ – critical new information about mechanisms, secondary and unexpected actions, unforeseen benefits, barriers and yes, some sad or bad new detail. Consequently, I always field lots of questions about SSRIs in our mentoring sessions & one that often comes up is why some patients gain weight on SSRIs. What’s most curious to many, is how the weight effects of antidepressants can be hard to predict. There is not a consistent pattern across any specific antidepressant class, nor just 1 or 2 medications within a class, that will do it, while the others never will. This is in contrast to the many determinations and drivers for who will or won’t get discontinuation syndrome. So what mechanisms might be behind such an individualistic weight response and is there any way to predict or prevent this?
Here we find ourselves again with the question that keeps all IM practitioners awake at night: But why? But why?? But why???!
A worthy question indeed. According to comprehensive reviews of this issue: there are still multiple candidates – one is the incidental histamine blocking that some SSRIs exhibit (could this flag someone low in histamine to start with??), while others still hold some suspicion over an old foe, elevated prolactin, that we can see in a minority of patients on these meds…easy to measure and confirm or refute, right? But always ask your patients first, How has your diet changed over this same period? How has your activity changed? You may of course find, you need look no further. People can give you the answer on a platter with things like, “I just relaxed a lot more: about what I ate and my weight”…Bingo! As always, the patient in front of you is their own little ultimate black-box…🧐
Never our call to make, but with 1 in 8 Australians at any time taking antidepressants, playing a supportive role for patients wishing to discontinue their antidepressant medication is common. So what do we know, about how to really do this well, what to expect and how to perhaps mitigate some of the bumps that might lie ahead. What in our artillery should we go in armed with either during the discontinuation or, better still, beforehand? This Update in Under 30 outline the key principles of patient prescriptions in this context and may assist patients, in their desire to truly leave the antidepressants behind.
If you are an Update in Under 30 Subscriber, this is a previously release episode and you will need to search for it to find this in your library of UU30’s that are in your online account.
Not an Update in Under 30 Subscriber? To access this episode and the entire library of Update in Under 30 audio’s and resources become a subscriber here.
Have you been told somewhere by someone that the ‘perfect’ TSH is 1.5 mIU/L? This is a wonderful, terrible & wonderfully terrible example of ‘magical numbers medicine’. As a push-back against the published reference ranges we’re given, that are so wide you could drive a truck through them, there has been an over-correction by some, leading to the myth of ‘magic numbers’. We can narrow the reference range substantially for many parameters with good rationale, make no mistake about that but once we start setting ‘aspirational goals’ that are explicitly rigid…well we’ve done 2 things 1) forgotten about the patient to whom this result belongs and 2) disregarded viewing each result as part of a ‘pattern’, that we must piece together and make sense of.
Back to TSH then… if my obese patient had a value of 1.5 mIU/L this in fact would be woefully inadequate.
Also too low for any patient, no matter their size, if their T4 is low and we’d like a higher value as well for risk minimisation in our elderly clients too.
But the same result would be excessively & worringly high in my patient who’s undergone thyroidectomy.
Being given a list of ‘magic numbers’ will never replace learning labs correctly. When we do this, we come to truly know that meaning can only be made of the markers when you can answer the following questions:
What is this (metabolite, analyte, binding agent, plasma protein etc)?
What do I know about its physiological and biochemical context – what is its role and regulation in the blood, what moves it and to what magnitude?
How have the reference ranges been determined for this lab – who am I comparing my patient to?
Therefore, what is the significance of a result that is: ‘normal’, ‘low normal’, ‘high normal’, below or above the range?
Does this value ‘fit’ with my patient?
What else could explain an unexpected result?
How strong is my level of evidence?
What do I need to do from here to confirm or refute this?
And a few more 😉
Realising the full value of any test result in terms of what it reveals about the person sitting in front of you, requires these skills. Unfortunately, in contrast a list of magic numbers will often lead you astray. And building your scientific knowledge about labs will not only help you avoid the pitfalls of pathology but will strengthen your pathophysiology prowess in surprising ways, saving your patients a packet in terms of additional extraneous testing and help you truly personalise your prescriptions…because the ‘invisible (biochemical individuality, oxidative stress, genetic probabilities, subclinical states, imbalanced or burdened processes etc) just became visible’. I started requesting lab results early in my career and years later was lucky enough to be taken under the wing of Dr. Tini Gruner. I found some of our shared notes, from 10 years ago, scribbled all over patient results recently and I was struck by just how lucky I was to have her encouragement to really pursue my interest and how she was a guiding force about learning to recognise pathology patterns over single parameters. A decade on I can confess, much of clinical and educative success has come off the back of this foundational skill-set and I know, this is true for so many I’ve taught too.
“The guidance I’ve received over the years from Rachel in relation to pathology interpretation has been one of the most valuable (and fascinating) investments I’ve made as a clinician. Her teachings have filled gaps in my knowledge base I never knew needed filling and have significantly enhanced my understanding of the inner workings of the body! Rachel has an incredible ability to make the numbers that patient’s so often present us with, both understandable and clinically meaningful. The knowledge I’ve gained by investing in this skillset has paid off in dividends and I’m certain will continue to do so into the future.”
Stacey Curcio – Cultivating Wellness
I hope you’ll join me for the most exciting up-skilling opportunity in learning labs yet. Oh…and all this talk about thyroid testing..that’s just a serving suggestion 😉 this year my MasterCourse is focused on the most routine labs of all: ELFTs, FBE, WCC, Lipid and Glucose Panels…an absolute treasure trove of free integrative health information about your patient!
This skillset has been found by many to be biggest ‘game-changer’ in Integrative Medicine!
There are limited places. To sign up for the MasterCourse: Comprehensive Diagnostics click here. For more information about the program click here.
Assessing Adrenals can be hit and miss, especially given that even more so than other labs, timing is everything. That’s why endocrinologists typically won’t look at anything less than a 24hr urine collection. If the total output is deemed to be high = Cushing’s and if it’s low = Addison’s. Sounds simple right? But to say only values outside of this reference range flag a problem might just be a case of throwing the baby out with the bathwater (or urine in this case!). Especially given it has been established that humans frequently fail at correct & complete 24hr urine collection! Alternatively we can use saliva or blood assays and capture the cortisol at any given time point, comparing that to expectations based on diurnal rhythm – but again, how are the reference ranges for these ascertained and is there such as thing as low normal. high normal results for cortisol, that actually warrant follow up investigation? I’m so glad you asked.
I see a number of patients who present with possible indications of flagging adrenals: from some distinguishing, but far from definitive features, in the clinical picture, to secondary lab markers. However, when they ‘limp’ over the line with their morning blood cortisol result I am often left talking to myself in an echo chamber about the need for more follow up.
But with the RCPA a.m. reference range of 200-650 nmol/L (Some seriously wide goalposts!) and some labs even going down to 150 with their minimum acceptable level for morning cortisol…are we right to still flag hypocortisolism (for any reason) as a differential in patients with low normal results?
Well Medscape yet again delivered Christmas 🤶 early last week with the largest study to date of blood cortisol, that has narrowed what’s ‘normal’ significantly…at least in terms of how low you can go before warranting further investigation. In this study they tested blood cortisol in the morning and afternoon, in over 1200 individuals presenting at an endocrinology clinic to determine in real world terms how low is too low (and associated with an increased likelihood of genuine adrenal insufficiency). They then gave this new ‘minimum cortisol’ a bit of test-run in 2 other large cohorts of patients to check it really did work as an effective cut off and wham bang…we now have a fully validated bare minimum… and guess what…it’s 275 nmol/L in the morning and 250 nmol/L in the afternoon!
Let’s be clear, their cut-off has what’s called a low ‘positive predictive value’ – which means most people (approx 2/3) with cortisol under this cut-off, upon further investigation (typically the ACTH stimulation test) will be found to be fine. BUT the point of this study was to ensure we don’t miss patients with adrenal problems just because they have ‘within range’ cortisol…and this new cut-off delivers on that.
This is big helpful news actually. Previously with patients who had am cortisol between 150- 275 we tended to find ourselves in ‘no man’s land’ – unable to provide enough of an argument about why adrenal insufficiency should still be on the differential list but unable to abandon that suspicion entirely. Thanks Medscape! Now if all the labs, RCPA and the referring physicians can just read this study and shift their goal posts…🙄
Our Group Mentoring 2020 Doors are just…about…to…close!
TODAY!
So if you love labs (or want to learn to love them more), desire to be a better diagnostic detective than you already are and want truly independent mentoring in a collegiate and structured environment for next year and you haven’t applied yet…best shove your foot to hold that door open right now! We offer a range of different levels & types of special interest groups: from New Graduates & the Mental Health Primer group (for those wanting to upskill and focus on this area), from rotating case presentations in our regular groups which are a mix of funky similarly skilled clinicians, to our pure GP group…take our pick! But get in quick by emailing us right this very second: [email protected]
Our knowledge is subject to constant change, and it is oh so necessary to stay up to date in our field for a bazillion reasons, give or take a few 😉 So sometimes we can feel like we need eight arms (for the visual amongst us) to manage and keep up with it all. However, if we ‘use the force’ together we are stronger, learn faster and can stop with the whole ‘recreating the wheel thingo’ that so many practitioners find themselves doing out there in solo practice. Like, like…well, how confident do you feel about putting pen to paper? How good are you at your inter-professional communicating?
Referrals and inter-professional communication are just lightly touched on in the current undergraduate degrees (if at all!). But it’s actually such an important way to grow your own professional reputation while simultaneously the credibility of our whole profession. One might even argue, a pillar that stabilises the castle of shared patient-centred care & the future of true integrative health. I hear from my “New Graduates” as well as seasoned mentees about the unease that starts to creep in at the thought of writing the dreaded referral letter. I’ve been writing referral letters for 20+ years and it’s given me a lot of time to think!And refine. And refine again! To make inter-professional care a positive experience for everyone, we need to correct some misperceptions and ensure that our patients are everyone’s priority. And to fulfil our duty of care, communicating with the other practitioners on your patient’s healthcare team is fundamental. Sometimes, as you’ll learn, it’s about modelling the best kind of shared care to boot and being the bigger person 😉
Better still, positive experiences of inter-professional communication will bring collaborators out of the woodwork. Medicos and other allied health professionals you may never have been aware of otherwise, with a desire and openness to shared care tend to rise to the surface.
To get you even more excited about referral letters (you didn’t think that was going to be possible, right?!) and unlearn that Pavlovian procrastination you may have developed, Rachel has completely redesigned an older presentation to ensure it’s truly reflective of the contemporary healthcare landscape (oh yes, RACGP position statement included!). Expect to roll up your sleeves and get seriously practical advice with loads of examples about how to medico-speak naturopathic concepts, explain your role in the patient’s care, provide rationale for consideration of investigations and present ‘red flags’ with punch but minus the sensationalism. And above all else, reveal yourself as the asset you really are to the rest of the healthcare team.
“Thank you so much for a wonderful presentation yesterday, Rachel. It gave me a new perspective on how it must feel as a GP to receive incessant demands from Naturopaths/Nutritionists to order pathology for their clients. I am in awe of your integrity, desire for patient empowerment, humility and respect for other professionals in the mainstream health arena. I felt that every single naturopath and nutritionist out in the big wide world ought to have listened to your insightful words of wisdom when it comes to shared care of our clients. We are blessed to have you as our teacher.” – Michelle Blum (Mentee 2019)
If you know me, you may wonder if I’ve recently undergone a personality bypass. I am passionate about diagnostics, pride myself on ‘making the invisible visible’ through better understanding of pathology markers and confirming the true nature of the underpinning problem in order to be most effective in our management of every client. And I absolutely see that for the majority of patients ‘ knowledge is power’, so what on earth is this all about? Well, while I stand by my stubborn commitment to diagnostic sleuthing for ‘most patients most of the time’, there are occasions when I’m left wondering about the value and the likely outcome should we finally catch that elusive diagnosis by its tail…case in point:
Recently I’ve been aware of a bit of spike in ‘diagnosing’ Ehlers Danlos Syndrome for patients who present with myriad problems – from the text-book connective tissue issues (loose joints, hypermobility etc) to the seemingly more far flung like mast-cell activation syndrome and overactive pelvic floors.
Just so happens this ended up being a thought-provoking 3 way conversation. Got to love having so many wise women’s email ear..and especially such generous ones. First, I ran this case and the differential past the wisest dual qual physio/naturopath I know Alyssa Tait who specialises in pelvic conditions and any and every other bizarre – no-one-else-could-name-it, kind of conditions. And her response, breathtakingly comprehensive and punctuated by copious journal articles throughout as always, proceeded to flesh out the evidence for and against the more unusual patient features and the possibility of EDS from bladder irritability (maybe) to functional GIT disorders (definite maybe) to the dysautonomia link (patchy). But it was what she said next that struck a deep cord for me:
“This happened recently to me when I referred a very difficult Painful Bladder Syndrome (PBS) patient to a GP – suddenly she had EDS as the answer to all her problems. But we can’t change genetics. All we can change is the function, and I have seen a worrying pattern of blaming the unchangeable (EDS) at the expense of looking for the changeable (e.g. an EDS patient of mine who actually had low thyroid function which had been over-looked.)
My feeling is it’s better to evaluate and treat what we see. As soon as we start giving our patients a litany of all the possible horrible ways their health is/will be pervasively affected by a completely unchangeable genetic reality (EDS), it’s a major “thought virus” that can both reinforce the “sick person” self-image and negatively impact their health-seeking behaviour – either by making them give up, ‘cause it’s all too overwhelming, or to follow an infinite journey through rabbit holes that make health their hobby rather than experiencing their life and relationships to the full.”
So back I went to the original practitioner who was contemplating chasing this EDS diagnosis in her patient and she was not short on some of her own wisdom. Like many people who end up working in health Gabby battled her way out of her own ‘no-one-cold name-it’ health crisis before training to be a naturopath. So understandably she sees both sides:
“As a terrified 20 something who kept ending up in the emergency ward with flares – I desperately wanted to know what was wrong with me, why it was happening, why I was in so much pain and why at the time no-one could tell me. I remember being about 28 asking my Prof (of immunology) whether what I had was going to kill me. He said ‘If you want me to be honest I’m really not sure at the moment darling but I’ll do my absolute best to take care of you’. That answer changed my life. Now as a Nat with a history of chronic conditions – I can see managing the symptoms is probably really all you need plus regular monitoring. Which is what I do for myself and many of my clients. The hurdle is getting over the lack of trust these clients feel after years and YEARS of being misdiagnosed and fearing for their lives.”
So..I’m asking us all again..is a diagnosis always helpful? Perhaps with each patient we need to think this through afresh? Thanks wise women 😉
There’s a significant increase in the number of women in their 20s to 50s presenting with ‘atypical’ joint pain, that seems hard for specialists to diagnose and therefore, hard for any of us to know how best to treat. If we listen closely to these patients, however, they are often telling us that their, ‘gut isn’t right’. It doesn’t tend to grab so much attention but maybe it should! We examine 3 ‘atypical’ arthropathies that can have GIT symptoms and arguably may represent a key driver of their joint pain. The different clinical pictures & targeted investigations for these big 3 together with some key papers are covered in this audio.
With the increasing weight of evidence pointing to a potent pathogenic portal between our mouths and every other part of the body, whether that be in terms of cardiovascular disease, rheumatoid arthritis, appendicitis, even a growing case for Alzheimer’s disease, we need to ensure we’re not overlooking the condition of each patient’s oral cavity. I got very excited about the recent Medscape article: A rapid non-invasive tool for periodontitis screening in a medical care setting. It’s true, I live a quiet life 😉 But seriously, a validated tool for all non-dentists to accurately pick up on the likelihood of this condition would be a nifty little thing indeed, so we can narrow down just who we quick-march off the dentist as well as understand their whole health story. But then I read the 8 actual questions which included gems such as: Do you think you have gum disease? and Have you ever had treatment for gum disease such as scaling and root planing, sometimes called “deep cleaning”? I thought, ok, this is not rocket (dental) science.
But that’s the point, I guess, right?
So while I encourage you to check out & employ this screening tool by all means, we can also be reassured that just by ensuring that when we ask about someone’s digestion (and when don’t we?!) we start at the very top of the tube, we’re doing a good job!! As my new grad mentees learnt this year…following the patient’s GIT from mouth to south anatomically, is my rather simplistic way of guaranteeing I cover everything digestive..without using formal consultation script. So in the case of the mouth, my questions include things like: last trip to the dentist; any prior dental diagnoses, number of amalgams, implants, root canals etc & their routine dental care techniques, any signs of bleeding on brushing & all foods they avoid for dental or oral reasons? Look, it hasn’t undergone the rigorous validation that the Self-Reported Oral Health Questionnaire has..but I think it’s a good start.
Whether we’re being picky about pathogens and exactly how they got access to the rest of the body (and gums make a great entry point!!) or just concerned about chronic low level inflammation, a ‘gurgling’ CRP between 1-5 in an otherwise ‘healthy adult’, picking up on periodontitis is a pivotal.
Oh and if you’ve ever wondered about possible health implications from mouth metals other than amalgams…don’t worry, soon I’ll be getting to that with a forthcoming UU30.
Want to hear more about how certain microbiota (from the mouth to the south) are being implicated in joint diseases such as rheumatoid arthritis and ankylosing spondylitis and how we can investigate these individuals?Getting to the Guts of Women with Joint Pain is a recent UU30 instalment that gets down & dirty on the detail.
I’ve had a bit of ‘a bee in my bonnet’ this year. I heard that! Ok, arguably it extends a little further back…like my whole career! But if you’ve seen the topics I’ve been speaking on at conferences in recent months, you’ll know exactly the soapbox I’ve climbed up onto. Inter-professional communication & collaboration. My particular focus (naturally 😉 ) has been current issues regarding the sharing of, and access to, pathology results for our shared-care patients. However, in the face of several distinct threats to the practise of both naturopathy and medicine in Australia of late, especially in the form of anti-collaborative rhetoric/push affecting both professions right now (read PHI reforms, promptly followed by proposed MBA review..if you haven’t read this regressive and repressive set of recommendations you seriously must), the question of how to improve collaboration in order to ultimately serve our patients better, has never been more urgent.
Last week, at the ICCMR conference, I outlined the current barriers for naturopaths to accessing patients’ pathology results (current and historical) and the heightened risks that this results in, either because of incomplete information or because of the subsequent direct pathology referring by naturopaths. Yes, bypassing the GP and another set of trained eyes on your patients labs comes with risks. I also spoke to the opportunities that await us if we can overcome this: in terms of improved patient outcomes, reduced risk, more economically responsible public health budget spending etc. etc. need I go on?! In the Q & A following my presentation, a doctor in the audience made two very important contributions, which deserve some additional air…she said:
“Shouldn’t the patient ultimately own their own pathology results? Then it would be a case of them electing who has access to these: their GP, their naturopath, their osteopath. Rather than the other way around – after all, we are all supposed to be members of their health care team, right?”
She said it. Not me. But I applaud her. She’s right of course. Right now, under the current proposed changes, we and integrative health care delivery and patients’ right to choose and self-direct their healthcare and public health budgetary burden…are all under threat of de-evolving. Right at the time when, with the current chronic disease burden and predicted public health budget blowouts, it should be all hands to the pump! Who has ever conducted a cost-benefit analysis of what integrative health care (successful patient sharing between naturopaths and GPs /specialists) saves the government? No one is my guess and when I proposed I do exactly this for my PhD on a particular parameter some years back, I was not so subtly told, that in spite of a great application, given the primary funding of the research group was from government, and a clear conflict of interest with the head researcher who was also a government advisor, ” my proposal was not in line with the current directives”. Yep.
Last week, a dear mentee of mine mentioned that a GP one of her patients sees responded to her respectful correspondence regarding their shared patient with absolute terror, citing possible de-registration if they are seen to be collaborating or interacting with her in any way…assuming the MBA changes go through. This doctor then decided the lesser risk, was to cease communication with this other key member of the patient’s health care team, not refer the patient for any follow up investigations (including those representative of basic duty of care) and certainly not enable access to any pathology results for this patient from the past or in the future. My mentee’s exemplary response to this doctor:
“My apologies for placing you in an uncomfortable position. I do understand the restrictions and guidelines GPs must work within for Medicare and AHPRA and understand that as you are the requesting practitioner you are liable for any pathology referred for. I make this clear to all my patients and that my referrals are on a request base only and it is up to yourself or the requesting GP for the final decision. I only try and request pathology through a GP or other medical practitioner to try and minimise both risks (of only myself viewing these labs) and unnecessary costs to the patient.
…’X’ has currently been seeking medical and alternative treatment for over 2 years and yet has had no change, if not a worsening of his condition and when I saw them 2 weeks ago, it was my understanding that not even basic assessment of full blood count, liver function and other general health markers had been completed. I had advised X that not all pathology may be covered under Medicare, and to come back to me so I could send him privately for those tests not able to be completed under Medicare. My apologies this was not made clear to you at the time of his appointment.
I take pride in my evidence-based approach to nutritional health in my practice, and work frequently with other patients’ medical practitioners in supporting their health. Thank you for your time and I appreciate your thoughts on this matter”
If the patients’ best interests are no longer the primary goal, as decided by bureaucrats, both government and organisational, is it time to ask the actual health professionals to please stand up?! Is it tipi-talk time for practitioners from all disciplines? Growl over.
Want to ensure you are writing professionally to other health care practitioners? Then our recording and resource Dear Doctor, is for you!
In this 45min podcast Rachel succinctly covers the serious Do’s and Don’ts for your professional letter writing. Rachel gives step-by-step instructions and examples for key phrasing and clear medical justifications, what terms to use when in order to come across respectfully, and how to present urgent red flags without sensationalising. This podcast is will help your professional letters improve collaboration for you and your patients need.
 The debasing of BMI as a stand-alone assessment of weight is long overdue given its significant limitations and lack of meaningfulness with respect to overall health. This coincides with a bigger societal and cultural shift towards inclusivity which involves redressing bias against people with diverse body sizes and compositions.
The debasing of BMI as a stand-alone assessment of weight is long overdue given its significant limitations and lack of meaningfulness with respect to overall health. This coincides with a bigger societal and cultural shift towards inclusivity which involves redressing bias against people with diverse body sizes and compositions. 
 MasterCourse I: Comprehensive Diagnostics.
MasterCourse I: Comprehensive Diagnostics.