Still. And yes – like you – I don’t see any slowing down any time soon in this extraordinary paradigm shift occurring in medicine and health. Which for us humans involves one humbling discovery after another.
Here we were thinking we made our dietary choices from a place of free will & individual preferences 🤣🦠
Thinking those microscopic mates, were making those B vitamins, and SCFAs and and and…for us & our benefit 🤣🤣🦠🦠
And while there’s a lotta love going on between our microbes and our micronutrients – in both directions – Pat Benatar said it best, “Love is a battlefield”
(sorry but I feel compelled to insert a link here for the youngsters – you’re welcome 😉)
The tussle over who gets to access those nutrients that are actually essential to both of us (the hostage and the microbiota) is an absolute turf war, peeps, and this battleground has seen some bloodshed! The new new question being raised is how the prescribing of nutrients, especially at the higher doses we tend to use, trickles down to influence and impact those microorganisms who reside in the bowel. Directly – as a selection pressure we have, likely unintentionally unknowingly, introduced. Which species do well when exposed to levels of a vitamin or a macro or trace mineral that are simply unobtainable in the diet? Yes – research answering these questions has begun in earnest revealing some positive ‘prebiotic-like actions’ of some but not of course for all nor in all scenarios. Want to learn more about this latest aspect we need to consider when formulating our nutrition prescriptions? You can either jump in and join us in the Nutrient Prescribers Program which kicks off next week to get across absolutely everything new in nutritional medicine or just dip your toe in here with our latest Update In Under 30: The Micronutrient Microbiota Universe
The world of health science went microbiota-mad a few turns back and there’s no sign of an end. Research continues to reveal the breadth of the GIT microbiota’s positive & negative reach, in particular, & with discovery upon discovery we’ve come to understand how often the microbiota are ‘managing us’. Both in terms of being integral to the success of our digestive, immunological, metabolic etc processes but also in a self-serving way, for example, directing our dietary preferences to satisfy their own needs. This has understandably prompted the question about the impact micronutrient supplementation is unintentionally having as a selection pressure on our gut microbes. Which bugs like which B vitamins when taken in excess of the amounts achievable in the diet? And which microbes flourish and which falter when we radically change their mineral exposure?
You can purchase The Micronutrient Microbiota Universehere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
I’m such a sucker for marketing!…ZoomZoom is from an old Australian car ad – an earworm clearly conveying ‘ the speed of something’, and let me tell you, totally fitting for this little Zinc tale I’m about to tell! Many years ago, I wrote a thesis on Zinc that necessitated me reading every research paper ever written (that’s how it felt anyway!🤪) on this trace mineral. Like everything in nutritional medicine, especially in the area of our burgeoning understanding of micronutrients, this is a highly dynamic space, so regular reviews of what’s new is essential and, since my thesis, part of my regular practice. Well, I just did my latest deep dive, and HELLOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO radical paradigm shift(s)…yep plural!
Zinc supplements should ideally be: Organic amino acid chelates Taken daily – due to the lack of Zinc stores in the body Taken fasting Taken in doses in excess of the RDI to compensate for the smaller % absorbed
Yep – nope. Or in true-blue Aussie: Yeah, nah. Can’t believe what you’re reading right now? Neither could I when I undertook this recent review but the studies are increasingly sophisticated and the resultant paradigm shifts are being echoed, reiterated & reinforced. And these have, in turn, challenged all those old ‘norms’ about how best to administer zinc for those patients with a shortfall. If you’d like to take this little journey for yourself…I suggest you start here! I immediately changed how I take it myself and now my mission is to both spread the word and get us all reflecting and reviewing our prescribing principles around Zinc…and tbh, around all micronutrients! After spending my ‘summer’ doing sufficient reading for a second thesis on everything new in micronutrients…I am armed and dangerously prepared for our upcoming *NEW* program: The Nutrient Prescriber’s Program which kicks off in late Feb for 5 months.
I truly believe that based on all this new information, we can now get so much more out of our medicines.
Nutrition represents such an extraordinary set of tools for us to work with, but it’s time to sharpen those tools in terms of how we apply them!
The Changing Zeitgeist Of Zinc Prescribing
Zinc research is a highly dynamic field and given its relative recency of discovery as being essential to humans, we’re still in the early days of truly getting to know this mineral. In just the last few years, enormous gaps have been filled-in regarding its regulation and roles that look to radically change our prescribing practices. Tune in to this essential update for some serious food for thought about doses and dosing frequency.
You can purchase The Changing Zeitgeist Of Zinc Prescribinghere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
How much? How often? When is the best time & timing? do you know about friends, foes and frenemies? Which form, when? e.g. building blocks or bioactives? And for how long? aka are we there yet…?
These are the kind of questions that one would imagine nutritional prescribers can always answer – but can you? Yet this is the goal, right? So that with each and every unique individual who needs supplements – we have a clear, consistent go-to framework to guide & direct these prescriptions. One that makes scientific sense, offers optimal outcomes and removes the uncertainty.
From my interactions with thousands of practitioners, however, I know many of these key questions plague practitioners & they feel, at times, as if they’re flying without a net, or without a strong systematic approach, or at the very least without all the answers to these questions.
I’ve had so much good fortune & so many others to thank for providing me with this foundation. Fay Paxton – my nutrition lecturer in my under-grad who indoctrinated me with a systematic approach. Dr. Tini Gruner – my principal supervisor at SCU, who shared & further fuelled my passion for biochemistry and reading labs to extract insights into each individual. And thanks also to all the pharmacists I’ve delivered education to over the years, who, as a result of their grounding in the principles of pharmacokinetics, always ask the best questions – questions that if I don’t know the answer I know I need to know the answer! So I made it my mission to find out!
While we dip into these aspects of nutritional prescribing in our regular mentoring groups on an ‘as needs’ basis, I’ve decided the time has come to create a year-long program dedicated to sharing this information and building this skill-set in practitioners.
This monthly meet-up is delivered live (max 1.5hr) and runs from Feb to November with the following currently proposed format *subject to change dependent upon the needs of the group
Feb Factors Affecting: digestion, absorption (host, form, dose)
March What happens to what gets left behind? e.g. enhanced enterocyte micronutrient concentrations & their effects plus unabsorbed nutrients & their interactions with the colonic environment
April What happens to what’s absorbed e.g. distribution, hierarchy of needs, activation and deactivation
May The pharmacokinetics of prescribing
June Where do our ideas on dosing come from? e.g. Physiological Vs Pharmacological dosing & actions. The basis & believability of maximal intake boundaries?
July Bioefficacy V Bioequivalence. Beyond building block nutrients: Is ‘Bio’ (-active, -peptides, -materials) always better? e.g. GABA Vs Glycine, NAC Vs GSH, PLP Vs Pyridoxine, Niacin Vs Niacinamide riboside ——————————————————————Aug month off—————————————————————————
Sept How often & for how long? Are we there yet? And how would we know? Plus Fast Vs Slow Nutritional therapeutics
Oct Strategies for Supplement Success e.g. friends, foes and frenemies in nutrition underpinning principles with examples; compliance changers for clients
Nov Live attendance & opportunity to participate in a case-based mentoring session
This monthly ‘live’ meet up will be delivered as part of 2023 Group Mentoring as The Nutritional Prescribing Program Group Mentoring applications open 17 October 2022.
To join the waiting list and be notified when applications are open, email the team at [email protected]
Find out more about what groups are available for Group Mentoring in 2023 here.
Have you been told somewhere by someone that the ‘perfect’ TSH is 1.5 mIU/L? This is a wonderful, terrible & wonderfully terrible example of ‘magical numbers medicine’. As a push-back against the published reference ranges we’re given, that are so wide you could drive a truck through them, there has been an over-correction by some, leading to the myth of ‘magic numbers’. We can narrow the reference range substantially for many parameters with good rationale, make no mistake about that but once we start setting ‘aspirational goals’ that are explicitly rigid…well we’ve done 2 things 1) forgotten about the patient to whom this result belongs and 2) disregarded viewing each result as part of a ‘pattern’, that we must piece together and make sense of.
Back to TSH then… if my obese patient had a value of 1.5 mIU/L this in fact would be woefully inadequate – so too a child at any weight.
And we expect a higher value as well in our elderly clients too and this level there may be, in fact, increased mortality.
But the same result would be excessively & worringly high in my patient who’s undergone thyroidectomy.
Realising the full value of any test result in terms of what it reveals about the person sitting in front of you, requires these more thinking and more thoughtfulness. Unfortunately, a list of ‘magic numbers’ will often lead you astray. And building your scientific knowledge about labs will not only help you avoid the pitfalls of pathology but will strengthen your pathophysiology prowess in surprising ways, saving your patients a packet in terms of additional extraneous testing and help you truly personalise your prescriptions…because the ‘invisible (biochemical individuality, oxidative stress, genetic probabilities, subclinical states, imbalanced or burdened processes etc) just became visible’. I started requesting lab results early in my career and years later was lucky enough to be taken under the wing of Dr. Tini Gruner. I found some of our shared notes, from 10 years ago, scribbled all over patient results recently and I was struck by just how lucky I was to have her encouragement to really pursue my interest and how she was a guiding force about learning to recognise pathology patterns over single parameters. A decade on I can concede, much of my clinical and educative success has come off the back of this foundational skill-set and I know, this is true for so many I’ve taught too.
“The guidance I’ve received over the years from Rachel in relation to pathology interpretation has been one of the most valuable (and fascinating) investments I’ve made as a clinician. Her teachings have filled gaps in my knowledge base I never knew needed filling and have significantly enhanced my understanding of the inner workings of the body! Rachel has an incredible ability to make the numbers that patient’s so often present us with, both understandable and clinically meaningful. The knowledge I’ve gained by investing in this skillset has paid off in dividends and I’m certain will continue to do so into the future.”
Stacey Curcio – Cultivating Wellness
I hope you’ll join me for the most exciting up-skilling opportunity in learning labs yet. Oh…and all this talk about thyroid testing..this next MasterCourse series is focused on revolutionising your understanding of thyroid, adrenal, HPT & HPA markers based on the very latest research & findings & marry these together with everything you learned in MasterCourse I (ELFTs, FBE, Lipids & Glucose) to understand the ‘whole story’.
…an absolute treasure trove of free integrative health information about your patient!
DEEP DIVE INTO REAL CASE STUDIES TO DEMONSTRATE EACH PATHOLOGY PATTERN IN ACTION. ]\
There are limited places. To sign up for Rachel’s LIVE Series – MasterCourse II: Thyroid & Adrenal Diagnostics and for more information click here.
I’ve spent the best part of about 4 months recording my *NEW* Advanced Thyroid Assessment training. I told my team this would be easy and quick, given it was to be based on a great little 2-part, 2hr updated presentation I delivered just last year for ACNEM!! Sixteen weeks (like seriously…most of it) numerous rewrites and retakes later, our final product is 4 parts that goes for over 12hrs in total & has a bonus Adrenal recording! And yeah my team are impressed but unimpressed too if you know what I mean?!🙄🤪
Every time another, ‘Oh wow!’, or ‘No way!’, escaped my lips, it was a source of personal celebration, as another deeper layer of learning revealed itself.
But to the wonderful, somewhat weary and definitely wary Sally, who does all my powerpoints, it was met with, ‘Oh boy!’, because it meant many multiple new slides to build full of visual metaphors, animation acrobatics, if not an entire new Part!*#@^
Her sage advice along the infinite research road I’ve been travelling was : ‘Stop. You’re going to have to stop.’
So I didbut now I am this meme. Everything I see currently through the lens of thyroid health, I talk in tongues TFTs and my brain is one giant neural network of integrative endocrinological circuits! I have fallen in love with this topic, this neuroendocrine axis and its ‘first responder’ role all over again! Hence our little thyroid character below – all ‘antennaed’ up – is one of the many tools we’ve developed for this training, to teach us that ‘bad thyroids’ per se are extremely rare – but bad scenarios are common (too much or too little of any macronutrient, key micronutrients, a change in the internal or external environment etc etc) and this little fellow and his board of directors (no – not the hypothalamus or pituitary!) – well it’s their job to ‘read the room’, right?!
In the absence of this key understanding we risk: A lot of lazy labelling in thyroid health – ‘You have a bad thyroid – that’s why you…[can’t lose weight, feel tired, have SIBO etc]’ Misdirected treatment & especially a tendency to overload the butterfly with ‘thyroid’ nutrients – which can do more harm than good
I’ve said many times, ‘perfect number pathology is a myth’ but it runs rife in practitioners’ beliefs about TFT results with complete disregard of the person those labs belong too! Did you know, for example, that your TFTs should all be higher if your BMI is? That your T4:T3 ratio should never be 3:1 if you are on replacement, have hot nodules, are pregnant or are acutely unwell etc etc etc? How about how low your Selenium or Iron levels need to be before this factor will influence the actual levels of thyroid hormones measurable – & what the impact of these deficiencies are well before then that is far more sinister and serious? Yep…you see here I am, pouring just some of the tiny take-homes of Advanced Thyroid Assessment ALL over you!
Watch this space my new Thyroid training is just around the corner!
An increasing number of our patients have thyroid concerns but unbeknown to many of us the most likely explanation of all is thyroid nodules, whose incidence is on the rise globally. The development of nodules has always been primarily viewed as a nutritional disease. Traditionally attributed to chronic iodine deficiency but recently novel nutritional causes have emerged. Benign nodules come in 2 flavours: hot and cold and while patients can present with a mixture, it is the presence or absence of a hot nodule that radically changes what complementary medicines you can and can’t use and what an effective treatment plan looks like. The pointers, as is often the case, are there for us in the patient’s presentation and pathology, so knowing the difference is no longer a guessing game. This UU30 comes with a great visual clinical resource and includes key papers on the nutritional management of nodules.
I’m intrigued by the silence. Hair loss in women is frighteningly common, following pregnancy, menopause & with extreme stress (wait is that a tautology? 🙄) In fact it can strike at any age and for a multitude of reasons. When it happened to me a few years back I also initially responded with silence, terrified that if I said it out loud it would make it real, but when my daughter suddenly asked, ‘Mum are you losing your hair?’ with her trademark attention to detail & exquisite empathy, she gave me the words & a good kick into gear, simultaneously. Now I am fascinated by women’s silence around this generally, how little we share our stories & forewarn others, & as practitioners, the lack of adequate training we’ve had identifying the different types (hint: it involves donning gloves or if restricted to online consulting, knowing how to organise correctly positioned pics) & from there finding the right solutions.
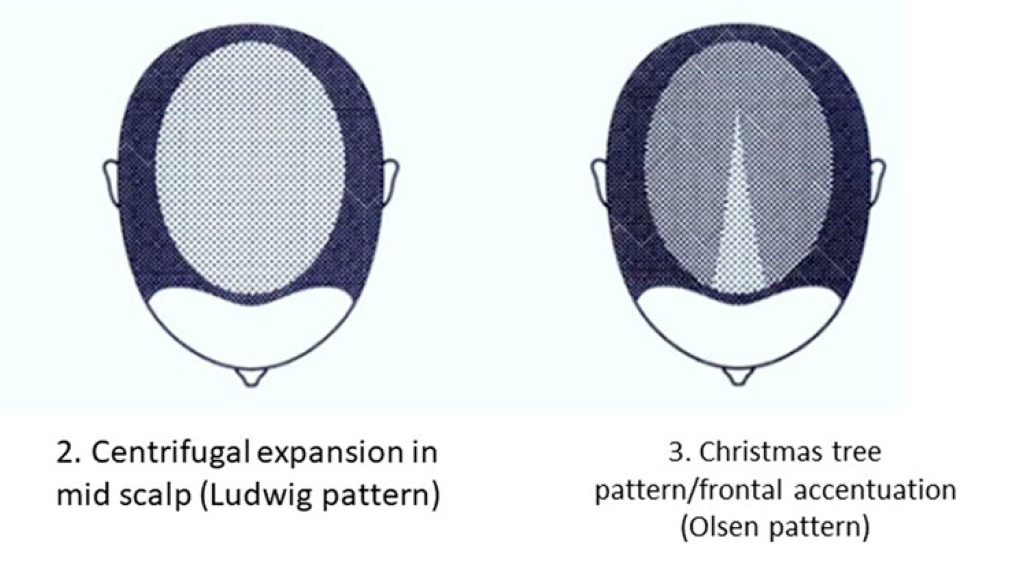
While Female Pattern Hair Loss (FPHL) is the dominant type in women – it only applies to the following pattern:
But alopecia due to stress, thyroid disorders, autoimmunity, contact dermatitis etc will affect different regions of the scalp and with a different onset & progression.
And remember, by the time YOU, the practitioner, can spot a patient is losing hair when they simply walk into the room, they have ALREADY LOST 50%😢 This is why I think we need to push back against the silence. The research is unflinching about the serious psychological impact this has on women – especially in cultures which place so much emphasis on looks generally, and hair, specifically as a commodity of very high value in women. The diagram above comes from a 2019 update on the phenomenon of FHPL and it’s a good articulation of the knowns and unknowns (pssst spoiler alert…it ain’t about androgens!) but let’s never forget the other causes and cures. So let’s make sure as the trusted practitioners women present to so often, we are sensitive enough to have this tricky conversation & skilled enough to help 💪
Stop Pulling Your Hair Out – The FPHL Answers You Need
Female Pattern Hair Loss (FPHL) is everywhere, perhaps you just haven’t been looking. As the leading cause of alopecia in women globally and with 1 in 5 women affected at any age, we’ve all got clients who have FPHL to different degrees. We need to be better able to recognise the early features of this condition which profoundly impairs quality of life and induces depression in its sufferers and that begins with validating patients’ concerns when they report “thinning” or “increased losses”. But what do we do from there? This recording talks you through the assessment, diagnosis and management of FPHL based on a combination of the most recent research and Rachel’s clinical experiences. Once you’ve ‘seen’ FPHL.., you won’t ever ‘unsee’ it and your patients will thank you.
I talk so much about iron, I feel like I’m cheating on my life partner (Zinc)…but these two are arguably the main mineral deficiencies we encounter most consistently in our patients and, don’t tell Zn, but quite frankly, in terms of who’s more well recognised out there, Iron throws some serious shade! But the truth is they’re a ‘twofor’, as a result of their similar distribution in food, with both demonstrating significantly better bioavailability (read: virtually double) from flesh foods etc, ‘Watch out, she’s on the attack again!’ I can hear the V’s (vegetarians and vegans) say and yes I think you see this one coming…but I think it’s possible to be pro moderate meat, without being, antiV.
Ethical and environmental aspects aside (just momentarily) it is hard to argue against the nutritional benefits from moderate meat for most patients.
I tried, trust me. Put my own body on the line (and my babies) to be a vegetarian for over a decade. But as the wheels fell off for me, I noticed them falling off for so many others…and these were people who were educated, with a capital ‘E’ and putting serious ‘E for effort’ into substitution etc Not everyone of course – but a LOT of women and occasionally some men. There was no denying their ‘iron hunger’ (high serum transferrin), their movement towards microcytosis (however slight that ‘smallifying’ may be…we don’t wait for anaemia, right?), their poor zinc status and more importantly, the clinical chaos of impaired immunity, some cognitive or mood issues that presented, as a result. I went back to the mineral manual, back to all the science that helps us to understand these minerals especially in a modern dietary context.
Ah yes…meat has become marginalised in our diets compared to those of our yesteryear selves (ABS data) while our consumption of potential mineral inhibitors…you know, all the good, but bad, but good foods, like legumes and grains and green tea and and and…has risen…especially among the kind of clients who come to see us, right?
Which ultimately leads to a lower iron ‘income’ with the same outgoings, again especially for menstruating, pregnant & breastfeeding women.
The books don’t balance. (So then…IV Fe to the Rescue???)
Bite me…it’s just science. There have been some wonderfully thorough studies on this very issue and thoughtful discussions. This study in particular, by Reeves et al, of Australian women in their 20s followed for 6 years to 2009, argues that just a 1mg/d increase in heme iron from flesh foods could reduce susceptibility to the subsequent development of iron deficiency amongst omnivores. So while the median daily intake of fresh red meat in these women was just 39g/d, their analysis found that an additional 70g of lamb or 60g of beef…or about 140g of chicken and 250g of fish if you prefer white over red, appeared to be the positive tipping point for women and their ability to stay iron-replete. Well below ‘dietary guidelines’, nowhere near the scary cancer correlations (which of course may be more about fat or nitrates or ??). Moderate meat intake, right? Just saying. And don’t worry, I know. The only thing worse than an evangelical ex-smoker is a rambunctious reformed vegetarian 😂
Need A Manual on Minerals?
Minerals represent a critical tool in naturopathic nutrition and there has been an explosion of research in this area over the last 10 years. In order to optimise patient care, practitioners need to keep up with the constant stream of information, updating their previous beliefs and understanding in the process. This seminal 7hr seminar (!!)…yes…seriously..it’s THE MANUAL..is designed to facilitate and accelerate this process of review and re-evaluation via a fresh look at the key minerals iodine, selenium, iron, copper, zinc, calcium and magnesium.
Sometimes I think I must be psychic..or is that psychotic? Don’t answer that, it’s a bad Byron Bay in-joke. I had literally just recorded my Update in Under 30 Copper in Kids and this excellent new study was published that same week, assessing and comparing trace minerals in age-matched ADHD and neurotypical kids. Snap! ✨ First, a moment of panic…because believe it or not, there are very few rigorous studies that have looked into this and so I had already read them all cover to cover and could confidently say, I had a grip on the literature. Gasp…’ will it have a different finding and challenge the much broader story about the excessive demonising of this mineral in kids health?’ Everyone take a big breath out…no.
But if you’re someone who thinks you’re seeing Copper toxicity in kids, you can keep taking a big breath in and while you’re at it a huge bit of new information:
Copper Excess is Normal in Children.
Every investigation of blood Copper levels in kids has reached the same conclusion and this latest one by a Russian group of researchers renowned for their work in Copper agrees. So the ideas that we have about optimal in terms of mineral balance for adults may stand, but can not and should not be applied to children. The elusive 1:1 relationship between Cu and Zn, for example, considered aspirational in optimising the mental health of big people, is absolutely not desirable or even healthy, in little ones. Why is it so? I hear you ask (…because you loved those old Cadbury chocolate ads with the crazy Professor as much as I did) Well, essentially because kids need more Copper than us, as a simple result of their increased growth requirements: blood vessels, bones, brains…Cu is a critical player in them all and more. And while we (and when I say ‘we’ I mean ‘I’) may be passionately passionate about Zinc’s importance, turns out, in paediatrics, it really does play second fiddle to Cu and should.
This new contribution to the Cu & Zn in ADHD kids debate did find that compared with neurotypical kids, their Cu:Zn was higher BUT – **and this is the really important bit **- as has been shown in a similar cohort before, the shift in relationship between the two was due in fact to lower Zinc levels NOT higher Copper.
So, I guess when you think about it…Zinc perhaps really does still deserve all our loving attention we give it 😂…we just need to rethink the whole negative attention we tend to mistakenly give Copper!
Copper, as a kingpin in angiogenesis, brain & bone building & iron regulation is a critical mineral during paediatric development. So much so, the kind of blood levels we see in a primary schooler might cause alarm if we saw them in an adult. So too their Zn:Cu. But higher blood Copper and more Copper than Zinc are not just healthy but perhaps necessary during certain paediatric periods. This recording redefines normal, low and high with a great clinical desktop tool to help you better interpret these labs, as well as reviewing the top causes and consequences of both types of Copper imbalance in kids.
The latest Update in Under 30 has landed. You can purchase January’s episode, Copper in Kids here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
-Your RAN Online Account has a NEW LOOK!!-
Next time your log in, you will experience a more user friendly way to search, view, listen and download your resources. Find out what’s new here.
What’s the most common thyroid disease you’re seeing in practice? Nope, try again. I’m serious. There would be very few of us who’d get this right without cheating. It’s nodules. Current figures suggest 1/2 of all us middle-agers have them and by the time we’re 80 that’s risen to 90%! There’s a school of thought that says these figures have jumped purely because of increased rates of thyroid imaging and we should stop sticking our nose in places it doesn’t belong. Just because they are there doesn’t mean we need to know about them or that they are causing trouble. All this is true and yet there is a percentage of patients for whom these nodules are a whole lot of trouble, in fact, that’s why they’re coming to see you…they (& possibly you!) just don’t know it yet.
Nodules, outside of radiation exposure, have always been primarily viewed as a nutritional deficiency disease: Iodine. While this was always a bit one-dimensional (poor selenium…when will you ever get your due?) it’s an explanation that no longer fits as well as it once did because even in populations who have addressed iodine deficiency, the incidence of nodules continues to rise.
So, what now?
New nutritional drivers have been identified but rather than being about our deficiencies they speak to our nutritional excesses. And while iodine is not totally out of a job here, some people of course are still experiencing long-term suboptimal iodine which can trigger nodule development, we now need to question if there is any therapeutic role for iodine once the nodules are established. Well the answer is both ‘yes, maybe’ and ‘absolutely not’. The determinant being whether we’re dealing with Hot or Cold. Unfortunately most patients and therefore their practitioners can’t tell the difference. But it is the presence or absence of a hot nodule that radically changes what complementary medicines you can and can’t use and what an effective treatment plan looks like.
I’ve seen a lot of thyroid nodule cases pop up in mentoring this year and it’s been a great learning opportunity for everyone to get comfortable with clues in both patients’ presentation & their pathology. While iodine deficiency no longer ‘fits’ like it did, nutritional medicine should arguably remain the primary approach to their management and the new research gives even more credence to this and identifies a far greater range of dietary and supplemental tools.
Thyroid nodules are going to explain a surprising number of our subclinical (hypo and hyper) thyroid patients and we already have a dispensary full of powerful interventions but we need to start by familiarising ourselves with their story: their why (they happen), their what (this means for patients) and their how (on earth are we going to address these effectively) Knowing your Hot from your Cold…is step one.
An increasing number of our patients have thyroid concerns but unbeknown to many of us the most likely explanation of all is thyroid nodules, whose incidence is on the rise globally.The development of nodules has always been primarily viewed as a nutritional disease. Traditionally attributed to chronic iodine deficiency but recently novel nutritional causes have emerged . Benign nodules come in 2 flavours: hot and cold and while patients can present with a mixture, it is the presence or absence of a hot nodule that radically changes what complementary medicines you can and can’t use and what an effective treatment plan looks like. The pointers, as is often the case, are there for us in the patient’s presentation and pathology, so knowing the difference is no longer a guessing game. This UU30 comes with a great visual clinical resource and includes key papers on the nutritional management of nodules.
You can purchase Are You Running Hot and Cold on Thyroid Nodules here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
*****Your RAN Online Account has a NEW LOOK!!*****
Next time your log in, you will experience a more user friendly way to search, view, listen and download your resources. Find out what’s new here.
There I said it. It was always going to happen. I’m ok, thanks for asking. This week we had a case of a woman diagnosed with MS in her late 20s. That was 5 years ago and she’s been medicated ever since with an immunosuppressant and she is understandably very nervous about taking any complementary medicine that would pull against this medication, interfering with its actions. Her concerns extended to zinc supplementation in spite of her plasma zinc being 7 umol/L. That’s right, 7. Zinc STAT, right? But slow up there everyone, her apprehension is not necessarily unfounded.
The top nutritional research topics in MS are: Vitamin D (for der…we all knew that, right?), Vitamin A and Zinc. The fan-mail for the first two, as key immuno-modulators in both prevention and in established conditions, is almost at stalker level.
In contrast Zinc attracts both fan and hate mail.
Although the jury is far from in, there’s growing concern that while extracellular levels of Zinc may appear low in MS (that includes of course plasma/serum values) the same individual may actually have elevated levels inside their cells and more specifically inside their CNS.Gulp. But wait there’s more. There is a hypothesis that Zinc dysregulation may be a pathophysiological driver in MS. Double Gulp. My (nutritional) soul mate has shown a potential dark side finally and is sitting under a cloud of suspicion. So what do we need to do differently?
If you’re seeing MS patients you need to be up on the sizeable pile of research into CM in this condition. A brilliant place to start is this very readable review of ‘Vitamins in MS’.
And specifically in regard to Zinc status in your MS patients? Well my advice is don’t rely on a plasma/serum Zinc alone – but couple this with an rbc Zn to ensure there is no sign of intracellular accumulation at play before you make a decision about treatment. Not a perfect solution, but while we’re unlikely outside of research to ever be able to measure CNS zinc concentrations, a reasonable approach. An unchecked zinc deficiency is in no-one’s interests either, including your MS patients – so it’s about gathering the best quality information you can to walk that fine line of adequacy not excess. And if you’re still reeling at the very thought that Zinc has a dark side – remember I did warn you…in Mastering Micronutrients – which is essentially a series of truth-bombs one of which, is every nutrient has a sting in its tail, a U-shaped dose response and a dark side. We need to get to know them all.
Let’s make sense of the over-arching nutrition principles, that will profoundly change your understanding and application of this modality Truly understanding the ‘big’ concepts, so often overlooked, or incorrectly taught, ensures you get the critical ‘small’ detail in your nutritional prescriptions right. In this 4 hour recording, together with key clinical tools, we talk about the tough stuff: dose-response curves, active versus passive stores and excretory pathways and ooh lah lah…the myth of taking ‘activated vitamins’. Even those who feel satisfied with their original training – will find a lot in this critical review that is new, insightful and truly practise-changing!
Integrative Psychiatry is an inspiring area to work in & its evidence base, acceptance and recognition of potency is rapidly growing & offering more patients, more. Going beyond the ‘neurotransmitter imbalance model’ for each presenting diagnosis helps us to see the unique mix of biological & psychological drivers in each individual who presents seeking our help. However sometimes I believe, we find ourselves falling into looking through the lens of just another short-list of alternate models:What kind of methylation imbalance does this person have? What sort of Zn, Cu issues?
While I am so grateful for having learned these tools and watched them be very successful in a portion of my mental health clients, they are simply not the answer for everyone. We need to keep our thinking and practices dynamic and up to date, to reflect the incredible increase in research in new areas of integrative psychiatry, such that more of our patients can benefit and that we can continue to think beyond the box…even if that box itself was originally so progressive!
What do you know, for example, about abnormal purine metabolism in mania and using serum urate as a BPAD prognostic marker in depressed patients? Think you can simply be guided by the reference range provided, think again. What could good old LFTs reveal about our patient’s mental health vulnerabilities and what have we potentially misunderstood about copper in this area, particularly in children?
I appreciate Zinc’s role in mental health as much as the next integrative practitioner. Okay, given my 20K word thesis manifesto, more. But increasingly I am seeing mental health patients who need treatment with different tools. This upcoming ACNEM Mental Health Module in Perth is on point: thinking outside of, outside the box!
While the above only speaks to what I’m presenting, I know Dr. Sanjeev Sharma will also be sharing his wealth of individualised management insights and he’s a big fan of addressing Chronic MIld Metabolic Acidosis as an early treatment objective. Maybe we all need to hear why? And I am so looking forward to getting a PTSD update from Christabelle and hear all about the research into therapeutic keto-diets in psychiatry from Cliff Harvey…haven’t read all those papers to know which conditions and when this approach shows merit? No, most of us haven’t. That’s the point of outsourcing our up-skilling to colleagues who we know are across these more than us and to boot have the clinical experience to ‘make real the research’. As I’ve said before, given the content of this upcoming ACNEM Mental Health program, I wish I wasn’t presenting really, so I could just kick back and take it all in, uninterrupted. But alas, I have some important new information on reading basic bloods through a mental health lens to share! I really hope to see you all there. Let’s get out of the rut of 3-4 nutritional approaches to mental health and make the most of the explosion of research and shared clinical experience.
ACNEM Face-to-Face Training Fremantle, 27-28 July 2019 at the Esplanade Hotel Fremantle by Rydges https://www.acnem.org/events/training
Oh and while you’re here…did you know the research into both beta-casomorphins and IgG casein reactions in relation to certain mental health diagnoses has taken some giant steps forward in the last couple of years? You should. Milk Madness is back and it’s via two distinct mechanisms – identifying which might be at play in your patients & correct management is now clearer than before. Want to get up to date in this area of mental health – check out our UU30 recordings: Milk Madness part 1 & part 2
Those ‘still-believers’ look away now. One of the great myths, misconceptions and misunderstandings in nutritional medicine is that supplementation with specific nutrients will produce change specifically in one system, or pathway, which just happens to be the one that the practitioner has determined would benefit most/is targeting. Let me explain myself a bit better. When we give patients any nutrient, in the cases where it’s not simply to correct a global deficiency & therefore improve levels all round, it’s typically on the basis of a specific desirable therapeutic benefit, e.g. some magnesium to help their GABA production…, additional B3 would improve their mitochondria. Beautiful on paper…but like sending a letter to Santa in reality (I did warn you!)
Truth Bomb No.1: There are nutrient distribution pecking orders that have nothing to do with who you ‘addressed’ it to
This dictates that when something is given orally, for most nutrients, the gut itself has first dibs. So the cells of your digestive tract meet their needs before any other part of your body gets a look in. Sometimes the digestive system’s needs can be quite substantial and leave little for any other part of the body…not mentioning any names (ahem) Glutamine!
Truth Bomb No.2: En route to the ‘target’, these nutrients get delivered and distributed to many other tissues – with possibly not so desirable or intended effects!
You may determine that a patient needs iron because their ferritin hasn’t got a pulse…so you keep giving them daily high dose oral iron to ‘fix’ this…not realising you’re making their GIT dysbiosis and gut inflammation worse in the process. Or you feel their mysterious ‘methylation cycle’, happening predominantly in the liver and kidneys, could do with a folate delivery…perhaps ignoring the very worrying fact that their colon may have already had a ‘gut full’. Literally. Hence the concerns and caution against supplementing with folate in patients with established colorectal cancer. So is bypassing the gut via IM or IV nutrients the answer…well yes and no…but mostly no. Read on…
Truth Bomb No.3: Those pathways that use the nutrient you’re supplementing, that are most active in the patient’s body currently – which is determined by many factors (genes, physiology, feedback circuits, pathophysiology) and rarely simply by the availability of nutrients – will take take the next lion’s share of that nutrient
Wanting to nutritionally support someone’s thyroid, you know tyrosine is the backbone of the thyroid hormones, so you include this in the hypothyroid prescription. Will it help? Who knows? Being a non-essential amino acid the body exhibits very complex regulation of its distribution and use – with thyroid precursor availability being only one job on a very long list! And if this was in a patient who is regularly smoking cannabis, due to upregulation of the tyrosine hydroxylase enzyme – there is likely to be more of the supplement headed for even more dopamine production and very little or none reaching in fact your intended target. And don’t get me (re)started on Glutamine – supplements of which in an anxious and glutamate dominated patient will make…G.L.U.T.A.M.A.T.E…right…not GABA! 🙁
Sorry, I know, it hurts right? But these are essential teachings, that tend to have been over-looked or under-played I find, in nutrition education, regardless of training: nutritionists, naturopaths, IM doctors, dual qualification practitioners remedial therapists. Nutritional medicine is a wonderful and potent modality when it’s done well…but we need to revisit some core truths and principles that many of us have missed out on, to ensure we’re not writing letters to Santa.
Let’s start with Micronutrients. Let’s talk make sense of the over-arching nutrition principles, that will profoundly change your understanding and application of this modality Truly understanding the ‘big’ concepts, so often overlooked, or incorrectly taught, ensures you get the critical ‘small’ detail in your nutritional prescriptions right. In this 4 hour recording, together with key clinical tools, we talk about the tough stuff: dose-response curves, active versus passive stores and excretory pathways and ooh lah lah…the myth of taking ‘activated vitamins’. Even those who felt well trained – will find a lot in this critical review that is new, insightful and truly practise-changing!
Standing at the podium, I looked down at my notes & slowly read out the title of my presentation to the hundreds of people attending, ‘Paediatric Digestive Issues & Neurocognitive Abnormalities’ and briefly froze thinking, Holy Heck (!) this is someone else’s presentation! Seriously. No, this is not one of my work stress dreams. This happened. I thought…oh my how am I going to deliver this, it sounds very complex and lofty and scary!!
Then I saw my scribbled hand notes on the page, the unofficial name I had affectionately given this presentation as I researched, compiled my case studies and brought it into being, months prior and I instantly relaxed…oh…Kids’ Guts Are Mental…now that I have some serious experience with and something to say about!(more…)
While we all know there can be a lack of specificity when it comes to some deficiency signs…like glossitis…eyeyiyi..naming a nutritional deficiency that doesn’t include this sign would be a tougher question 😉 but what a great reminder of some quirky things you may have forgotten or in fact deficiency features you may not have even known about.
A gem I love and apply frequently, is about zinc the ALP levels…watch out for the that later in the slideshow quiz.
Also note the distinct difference in opinion when it comes to vitamin D adequacy – with Medscape citing blood vitamin D result < 75 nmol/L unequivocally associated with osteoporotic change…in contrast to the …’anything over 50 nmol/L is a bonus’ line we’re being fed here in Aus and NZ! While we may not ever see some of these severe deficiency presentations walking through our doors – you can’t be so sure…given the reported resurfacing of scurvy in good ol’ Sydney just last year!
Is it just me? I love going back to nutrition 101. So tomorrow with your cuppa…test yourself and then let us know how you go 😉
Are you keen to keep developing your naturopathic knowledge in areas of diagnostics and nutrition? Rachel has a range of services that can help accelerate your learning. From the long list of great downloadable recordings in the store, that help fill your ‘knowledge potholes’ in a fun and engaging way that really brings these topics to life, to our Update in Under 30 Subscription: 30 mins of power-packed up-skilling delivered to your inbox every month, as well as our individual and group mentoring programs! There’s content galore and a delivery format to suit every clinician – come check out what’s on offer.
This year has been a steep learning curve but this is exactly as I had hoped and planned for. I strapped myself in for my roller-coaster ride, a series of intensive upskilling initiatives undertaken with mentors and experts in specialist areas, and I haven’t hurled yet or screamed loud enough to make the operator stop the ride (seriously this happened to me in about 1997 on a Pirate Ship in Rosebud!)…but I have come close 😉
One of the really big lessons has come from getting more into the science behind pyrroluria and urinary pyrrole testing again. What motivated me to tackle this spikey beast? Well, like many people who have been introduced to the concept of pyrrole testing and pyrrole driven mental health presentations – I had a lot of questions that hadn’t been adequately answered. Those gaps left me with some uncertainty about the validity of this investigation and about the interpretation of the results. I also have introduced this pyrrole theory to many naturopaths and hence feel a responsibility to polish up my knowledge on this and set the record straight.
Last but not least, in our local area we reputedly have a ‘pyrroluria plague’ at play – every man woman and their dog is getting this diagnosis and it had added not only to my misgivings about testing but also my concern about misdirected & unsafe treatment.(more…)
Most practitioners are pretty knowledgeable about Zinc and are quick to recognise a deficiency and the opportunities for zinc supplementation as an effective therapy and those same practitioners are often plagued by nagging questions that come up, in spite of loads of clinical experience, like:
Are plasma and serum zinc levels interchangeable?
What does zinc adequacy look like? Is it just a single number on a page or do we always have to factor in copper levels and get the ratio right as well?
What can I expect from zinc supplementation in terms of changes to the patient’s plasma zinc?
What should I do when a patient’s zinc marker is refractory to the intervention?
Is there really a significant difference between the different supplemental forms available?
We should all be as skilled in investigating & treating male hormone imbalances as we are female ones, yet this is often not the case. A lack of confidence in this area, which seems to be an issue for many, in particular will compromise our ability to question male clients comprehensively and effectively about their reproductive health and ultimately reduce our capacity for making good clinical decisions and achieving the best outcomes for them. If you’re female, how would you feel seeing a male practitioner who doesn’t ask you about your menstrual cycle in detail?
Many of us are at risk of committing similar crimes but we need not be.(more…)
As we head rapidly towards the change over of our calendars we would like to offer you a special on the very best educational recordings from 2014 – buy 2 CDs before Jan 31st and receive one complimentary Premium Audio Recording of your choice OR purchase 4 CDs and receive a 3 month Premium Audio subscription for free.
It’s been a busy year during which Rachel has delivered 7 very successful new seminars in the area of mental health and beyond, most notably fortifying her role as a leader in the field of diagnostics and pathology interpretation. This has included collaborations with ACNEM, Biomedica, Health Masters Live, MINDD and Nutrition Care, however, each recording is classic Rachel – full of fresh perspectives on diagnosis & treatment, colourful analogies & humour. In case you missed some of these this year or want a copy for keeps – here’s a quick summary of the 2014 recordings included in this end of year offer: (more…)
“Two great speakers – inspirational in the first half and bang on in the second – I now know how much I don’t know”
Just out now in time for Christmas…no seriously though… this year I had the good fortune to team up with Biomedica and in particular Rachel McDonald and we delivered a 3 hour seminar called Mental Health in Holistic Practice. The intention behind this collaboration was to shift the education focus for practitioners from a prescription based approach, to one really about the clinical reality of managing mental health clients. Probably most of you will agree that the ‘treatment’ counts for only a portion of the positive outcomes in your patients and this is particularly true in clients challenged with mental health issues. After more than 20 years in practice working in this area, I’m keen to share what I’ve learned so other practitioners can get there much much faster! (more…)
Just been speaking on the thyroid at ACNEM last week and am finding that practitioners across the board are getting more and more curly thyroid cases. One scenario that we increasingly see is something that might be described as ‘T3 resistance’, when your patient’s T3 value looks healthy but they continue to manifest the signs and symptoms of hypothyroidism. There are several differentials to consider of course (more…)