I really enjoy mentoring practitioners in business – it’s a real privilege to be able to hear about each practitioners’ aspirations and challenges. A few weeks back I had the good fortune to speak with a fresh one! A practitioner who has only been in business for a short period of time. As always before our session, I looked over all aspects of her online presence from her website, to her practice newsletters, Facebook presence etc. Goodness how things have changed from when I graduated and you literally just hung out your shingle!! As much as the online world has created incredible opportunities for people working in integrative health and the public who use our services, I think it has also of course brought the ‘competition closer’.
Perhaps you’ve been keeping abreast of the bone broth debate? The practice of preparing broths made from slow boiled animal bones and made popular by the GAPS diet as well as many Paleo advocates, has come under scrutiny thanks to a small pilot study that evaluated the lead content of bone broths prepared from chicken. The likelihood of lead leaching out of the bones and into the broth after prolonged boiling is quite high of course, given that, just like us, animals are tricked into thinking it’s calcium, and accordingly store this heavy metal in their bones. This study by Monro et al and published in the journal Medical Hypothesis in 2013, suggests that regular bone broths could contribute significantly to the lead exposure of an individual given the lead content of the 4 samples they analysed:
(i) organic chicken-bone broth: 7.01 mcg/L
(ii) broth from organic chicken meat without bones: 2.3 mcg/L
(iii) broth made from skin and cartilage off the bone of organic chicken: 9.5 mcg/L
(iv) control (tap water): 0.89 mcg/L
How many of your clients are on a combination OCP?
Do you know the full extent of the physiological impact in each? Are you able to identify to key pathology indicators regarding the magnitude of that impact?
Like you I see a lot of clients who are on the COCP – whether it’s for contraception, skin, dysmenorrhoea or ‘hormonal balancing’ (interesting concept!!). It’s typically the case that these clients are aware that, beyond contraception, it’s not really a ‘solution’ & ‘isn’t ideal’. They have, as all patients (un)consciously do, carried out a little risk benefit analysis though and here they are. I really feel reluctant to make more difficult, an often already difficult decision for women, and I always want to respect people’s autonomy and choices, so whenever possible I simply go about my job, supporting them naturopathically in light of the impact it is likely to have on their nutrition & physiology.
However, there are occasions when I look at their pathology results and put it together with their symptoms and realise that the ‘danger signs’ are flashing & the COCP is not playing nicely with their unique biochemistry.
Women’s responses to the COCP are not one-size fits all. Apart from the fact that there are multiple combination OCPs available with varying ingredients and actions, we know that each individual can respond to the same formula differently based on a range of factors we might not completely be aware of until they start taking it. For example, all oestrogen (whether it’s yours, synthetic or bio-identical) causes mobilisation of copper from the liver. So when we see blood Copper levels rise following OCP initiation, it’s not because these women are suddenly absorbing or being exposed to more, rather it’s as a result of the liver mobilising a large proportion of the copper that it previously stored, for use by the [imaginary] foetus. The question is – how much does each woman have in the wings, ready to go? And does this result in a blood copper rise that’s mild (S Cu levels < 20 mmol/L) or severe (S Cu levels >20 or even > 30 umol/L). What would be the consequence of being someone in the last group? Apart from the significant increase in oxidative stress and the jump in glycosylated haemoglobin (a particular issue for those with pre-existing IR or T2DM) how would this disproportionately high copper impact your mental health in relation to its role in neurotransmitter synthesis? What about the COCP’s additional effects on each individual woman’s SHBG levels (and therefore available TT), HPA axis, glucuronidation etc. etc.?
We’ve all come across women who’ve stopped the OCP because ‘it didn’t agree with them’ but what about the ones whose biochemistry is really battling with the COCP but they’re none the wiser? We can identify this quickly via reviewing standard blood tests & help the client to understand their individualised reasons to be look for other alternatives.
Research continues to clarify the physiological impact of the combination OCP & individualised responses – we live in a world where the COCP will continue to dominate as a contraceptive choice but surely a step towards an individualised approach & improved patient education & informed decision making, are steps in the right direction?
We’re all aware that in theory OCP use correlates with a range of elevated risks but in reality many females will make the decision that the pros, in terms of contraception or control of acne etc., outweigh the cons. What if we could provide more individualised advice by looking to their pathology results and identifying and quantifying specific danger signs for each individual? This approach enables us to better support patients who chose this form of contraception but accurately identify those that might want to consider safer or more suited options and equally reassure those for whom it remains a sensible choice.
I’ve been sick – real sick just for a couple of days…an acute exotic respiratory thing that the northern Rivers and specifically the period around Bluesfest (!) seems to specialise in. Anyway, apart from it being terrible timing (I ask my patients ‘when is it EVER good timing?’) it has been a quick gruesome but instructive reminder about what’s called ‘sickness related behaviour’. This is a cluster of behaviours that come as part of the package with being unwell. They’re usually short-lived as a result of acute infections like colds, flus, gastro. Trust me – you know them well 😉 they include: loss of appetite, social withdrawal, fatigue, amotivation, anhedonia or depression etc.
These behaviours are thought to be critical to our individual preservation and that of our community and at a physiological level are attributed primarily to the rise in pro-inflammatory cytokines (PICs) that are part of being ‘sick’. It makes sense right? If we’re sick we need to lie in bed, be still, rest up, stop working and most importantly, if it is contagious, stay away from everyone to prevent the spread! So really this sickness related behaviour is a very clever adaptation.(more…)
I was recently asked to speak at an ACNEM conference on ‘Clinical Pearls in Paediatric Practice’ and I talked about 3 key things that have proved to be absolute game-changers in my understanding and better management of children…and guess what one of my topics was…threadworm!!?? Yup. I am convinced some people who’ve heard me mention this before may start to think I have some sort of perverse interest in these little blighters because what could we possibly need to know about kids being infected with worms that we don’t already know? However the answer is….HEAPS!
I have spoken on this topic previously (basically when anyone will let me! ;)) and I can tell you that it’s this information specifically, what I’ve learnt about the myriad presentations, the individual susceptibility and fresh perspectives on treatment, that attracts the biggest ‘Wow!’, lightbulb moments and ‘oh my goodness you’ve just explained a riddle in half a dozen of my patients that I’ve been unable to solve’ kind of comments more than anything else. I just experienced this again at the ACNEM conference in NZ. It’s so wonderful to be able to spread the word! (no pun intended!)
Ok here’s a gripe I’m having currently. I have a number of patients who are taking anti-epileptic drugs (AEDs) and most of these are children who require them for seizure control. Naturally, working alongside such serious pathology and these critical medications requires a conservative and evidence based approach to ensure the safety of any added intervention. Fortunately, this is something I would like to think is one of my strengths. When these patients present seeking nutritional support, I typically refer them for investigations that can help to clarify what, if any, nutrients are imbalanced because of their long-term AED use or perhaps because of other independent reasons that may compromise they’re overall wellbeing. I feel that in such a vulnerable population I need to confirm nutritional deficiencies to check my assumptions, prove a need for supplementation and prevent against any excess or creation of further imbalance…and by doing so, I can adhere to my motto of least medicine, is best medicine.
The fact is AEDs are notoriously associated with a long list of potential negative nutrient interactions and the evidence to support this is extensive, this includes but is not limited to: folate, B12, B3, B6, zinc & vitamin D and the deficiencies potentially produced by the AEDs can be quite severe depending on a range of individual factors. For many of these nutrients, the research goes further and has shown that correction of the deficiency leads to better drug efficacy – therefore adjunctive nutritional monitoring and correction would seem like a real ‘win win’ situation.
(Stargrove,MB. et al. Herb, Nutrient & Drug Interactions – Clinical Implications & Therapeutic Strategies. 2008)(more…)
Have you ever wondered what is the best way to grow your business? Not a cardboard cut-out, off-the-shelf kind of business that every business coach talks to, or somebody else’s business, your business? Business advice like naturopathy, according to Rachel, is about taking an individualised approach.
The traditional model of a naturopath was based on a one on one clinical practice model, while potentially still a path to success and satisfaction, this requires a totally fresh and contemporary perspective on what works today. In addition to this, many naturopaths feel a need to diversify their revenue stream in order to work smarter not harder. The naturopathic path is not always conventional and rarely the same for any two practitioners depending on personality, location, skill sets (including non-naturopathic), passion etc.
It’s taken a little while for me to collect my thoughts on this one. Initially there was a little flash of anger, frustration and a good deal of huffing and puffing when I heard about the RACGP guidelines recommending GPs say no to any requests from naturopaths for further investigation of their shared patients… but I’m over that now. In an interview on 702 ABC Sydney radio last week, Stephen Eddy, the vice president of ATMS, responded to these guidelines by suggesting that a blanket directive for GPs to ignore all requests from all naturopaths about all testing didn’t really sound sensible or appropriate. Here here! Surely, in the pursuit of evidence based medicine and discerning practice decisions, each case should be considered on an individual basis. I think Stephen Eddy gives GPs more credit for being able to make these judgements than their own association! (more…)
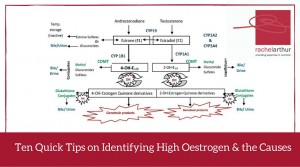
During mentoring sessions over the last week I’ve been prompted to ask a few practitioners if their patient had any signs, either clinically or in their pathology results, of high oestrogen.Each time it kind of caught the practitioner off guard because their patients weren’t presenting with conditions overtly related to an oestrogen excess and they hadn’t specifically ‘tested’ for this. However, in each instance the information was already there in the case, it was just a matter of knowing what markers to look for.
So some patients scream ‘high oestrogen’ right from the minute they enter the room? But often others present with health problems that don’t necessarily appear related at first glance. Regardless, their condition absolutely could be being compounded by this background imbalance – think thyroid & other autoimmune conditions for example.
There are plenty of patients who don’t have the exaggerated clinical presentation but still have this imbalance as a significant compounder or perpetuating issue in terms of their pathology.
Relax – I am not suggesting salivary hormones or any form of expensive testing all round (!) – in fact what I am saying is before you even consider yet another pay out of pocket test, costing your patient more time and money, we should look to the clues that are already there, in standard blood tests. Amazingly, you can infer a lot not just about the overall oestrogenic load but also pick up some clues as well about where the excess might be coming from.
In this Update Rachel brings together her 10 quick tips on how to recognise either high oestrogen and/or the potential underpinning reason behind the excess, in a range of easily accessible markers. A great refresher and synthesis of ideas on this important aspect of diagnosis and clinical management. This Update in Under 30 is now available to purchase as a download, click here to find out more or if you’re interested in a 12mo subscription click here
Howdy practitioners – I’ve had an inspiring month of clients. Not because I cured anyone, answered some major riddle previously unsolved by modern medicine or any of these enormous tasks we or our patients often set ourselves but rather because I got back to basics. Many of you will know that I spend most of my practice time working at the pointy end of complex chronic multi-system disease and while it is deeply satisfying when you have a breakthrough with someone’s health, it is challenging. Often I am the last bastion, my clients have been referred to me and therefore typically have already addressed their diet and other health behaviours to a certain extent. So unlike perhaps many naturopaths, I don’t spend most of my time in practice talking about food and doing the grassroots education that is at the core of naturopathic medicine (in my humble opinion) 😉
This month was different. I had a bunch of clients who, while they did have pointy end (that’s a technical term!) multi-system disease, e.g. one client alone had retinal detachment, coronary stents, a genetic bone disease, NAFLD and a liver abscess, they clearly hadn’t been educated about food in the way that we do so well and which can make such a huge impact on a person’s life and health.
Well here’s a thought…the ‘Superfood’ nutrition movement has just about eaten the South Americans out of quinoa and the Pacific Islanders out of coconuts..isn’t it time for a local hero? I get a bit despondent when any new food is touted as a ‘Superfood’ anyway for all the obvious reasons but this is heavily compounded when this so-called ‘Superfood’ and the bankable gross exploitation of this foodstuff comes at a huge cost: whether that be in terms of food-miles, another population’s access to their food staple or the radical change in land management in these countries that often follows, e.g. think palm oil plantations.
“I need a (Local) Hero!” – cue Bonnie Tyler soundtrack & wind machine 🙂
We kicked off mentoring this year with some great cases last week. One was a pregnant hyperthyroid client. During the session the wonderful practitioner mentions that the client is using Withania somnifera as required for anxiety.
Insert sound of brakes screeching to a dangerous squealing crash! Here’s a situation where I would give Withania a miss. (more…)
Low dopamine as an underpinning cause of depression, anxiety and even addiction (illicit drugs, sex, gambling) has been gaining increased recognition in research. In spite of this there are no antidepressants currently on the Australian market that address dopamine specifically and therefore patients with this pathophysiology often fall through the gaps, failing to get efficacy from pharmaceuticals. Many of these patients are subsequently diagnosed with ADHD as well, which has disordered dopamine as part of its aetiology, and are prescribed dexamethasone as well. The dexamethasone, being a stimulant that helps significantly to improve dopamine, is typically the drug that has more of a positive impact than the anti-depressants on these patients however, still fails to really solve the issue and can come with many side effects.
Since the 1990s the term ‘Reward Deficiency Syndrome’ was coined to describe a subset of these individuals whose brains are effectively under-equipped with dopaminergic activity in certain key areas. This is the result of a less common genotype coding for our D2 receptor in the brain. Far from being rare, this genotype is reported to be present in 30% of Americans, however, the magnitude of problems associated with it can vary from mild to severe depending on many other genetic and environmental factors.
There’s taking a break and then there’s taking a break.
For most of us Christmas does not fit the definition of a break but rather simply an altered version of our escalated pre-Christmas frenzy. The crazy end of year work wrap up replaced by the equally crazy Christmas to do list…the same underpinning mantra pervades both…” I must, I must”. But when all the pressies and eating is done the pace usually eases off a tad. I felt a wave of relief just having Christmas day behind me. Suddenly it seemed I was on holidays…still upright, still going through all the usual paces of looking after kids and elderly parents and occasionally attending to a work issue but the relative slowness was noticeable and welcome.
Then something radical happened. I went away.
I was already away, in the sense I was interstate at my parent’s house but we travelled just 30 mins further down the coast to an unknown little rental house by the Rye back beach just with my kids and one of my oldest nearest and dearest mates for a few days. Out of the familiar and all the ‘musts’, ‘shoulds’ and habituations that come with it, off the grid with no computer, no phone (by chance I had forgotten my charger) and to boot the clock in our little hideaway didn’t work! Aaahhhhhh timelessness found.
We sat, we lay, we read, we wandered the back beach for hours exploring rockpools and caves and I had a wonderful sensation as if my feet were sinking into something that I can only describe as the Awake Delta Wave Experience 🙂
I am reminded that of course taking a break is a bit like sleep, we need to progress through the more superficial stages where we remain semi-vigilant, always ready to jump up into action if necessary, until after staying with this slowed relatively restful state for long enough we can progress into deeper stages of relaxation and finally….ahhhhh… hit the delta wave experience of true restoration.
I am wishing you all a truly restorative Awake Delta Wave Experience this festive season and remember it’s not about how long you stay there, it’s just about having one at all 🙂
It is with great excitement & enthusiasm that today I can announce the launch of our crowdfunding campaign for the first independent Australian Naturopathic Summit to be held in Byron Bay on the 27-28th August 2016 (check out our campaign video below!).
This Summit is the creation of myself, Nirala Jacobi and Kathryn Simpson, who all individually noticed a big gap in the support available to Naturopaths striving to carve out their careers in a variety of areas (practice, education, medicinal herb growing and manufacture, corporate health, public health etc.). We’ve been working hard over the last few months to bring to fruition something that fills this gap & offers a truly unique educational experience and platform for our Naturopathic community. (more…)
Come along and be a part of the final case of the month session this Monday at 3.30pm AEDT.
A 47yo male initially presents with anxiety, panic and depression. He also has had chronic sleep disruption for 4 years due to vivid dreaming and nocturia and works in a high stress job. He has a BMI of 27 and in spite of a being a non-smoker, non-drinker & exercising regularly he has a high blood pressure. While he has marked psychosocial risk factors for mental health problems but what else are we missing or could we do to support?
Come along and see what we make of the case as we dig deep with detective work. What were the key questions we needed to know the answers to? What other investigations are relevant? What other treatment approaches might be effective? To get the answers and more book in via our mentoring calendar here. 🙂
We’re so excited to announce the new mentoring program for 2016, specifically designed to add more value and provide greater skills and knowledge acceleration to Integrative Nutrition Practitioners.
RAMP is Rachel’s first incubator 11-month program that focuses on providing integrative nutrition practitioners with the most accelerated form of post-graduate education and clinically relevant skill development. This personalised approach supports practitioners to ‘gap fill’ their underpinning knowledge & strengthen their clinical skills ‘Achilles’ while providing comprehensive support for all aspects of case analysis, client management & treatment. As usual, the sessions involve dynamic detective work and discussions lead by Rachel and contributed to by all mentees.
Some things have changed and some things remain the same.
All the good stuff remains (dynamic monthly group Skype sessions which are case based and run by Rachel) but our session times and the commitment we’re asking from practitioners has changed. In order to ensure the best outcomes for all practitioners via a constant and collegiate group we are asking for a year long commitment. All sessions will be recorded in case you are unable to attend some live and for established practitioners there will no longer be a ‘drop in’ or casual attendance option.
To read more about this truly one-of-a-kind new program that is stepping up practical post graduate education, head over to the RAMP page here.
If you’re interested in joining the program, make sure you apply quickly! The program is capped at 11 practitioners to ensure that all mentees present a case at least once in the year and all of our groups are already half full and we expect to fill them in the coming weeks pre Xmas.
Keep in mind, if the time is unsuitable for you we are collecting names and will potentially open a second RAMP group if there is sufficient demand.
New Practitioner Drop in Class
We will also be continuing Graduate Mentoring with the new name, new look, New Practitioner Drop in Class. This very affordable class is a monthly drop in class that focuses on providing newly graduated, or returning from break, integrative nutrition practitioners with the most accelerated form of post-graduate education and clinically relevant skill development.
Most of us know that measuring a fasting blood glucose to assess how well someone is managing their glucose levels is about as crude and insensitive as waiting for the smoke detector alarm to tell you your dinner is cooked! If we wait to see an abnormal result here we’ve missed a prime opportunity for patient education and prevention long ago. Much the same story if you’re looking at HbA1c results.
To explain this I always use the analogy of a duck. A duck will always be able to swim but the question is how much effort does it have to exert to swim the same distance? If your blood glucose is within range after an overnight fast that’s as good as saying, ‘this duck can swim the length of the pond’. What it doesn’t tell you is how fast its little legs are paddling in order to achieve that. Measuring a fasting insulin at the same time, however, tells us some additional important information. It tells you how fast the duck’s legs are paddling just to keep its head above water! The more insulin you’re having to secrete to just maintain normal blood glucose levels, the more alarmed we should be!(more…)
If you’re left wondering why on earth Rachel undertook the “Supersize Me Month” (see previous post here) then you may have missed her SAMe: Mental Health & Beyond tour. It’s funny really because one of the key areas Rachel discussed in this presentation is the significant therapeutic role for SAMe in a wide range of liver conditions including fatty liver, cholestasis, hepatotoxicity and even hepatitis. SAMe may even be considered an antidote to the Supersize Me lives many of our patients are living!
While many people are excited by what they’ve witnessed using SAMe for their mental health patients, Rachel’s insight into it’s numerous other actions and therefore indications came as a welcome surprise. Did you know it’s an anti-viral, anti-inflammatory and the key to improving the integrity of every cell membrane in your body via its production of phosphatidylcholine?(more…)
One thing that you need to know about me is that I consider myself pretty healthy…surprise! :0) As in, I wake with energy, I love exercising and on a typical day I am blissfully ignorant of my digestive system..as in it doesn’t speak to me via oohs aahs gripes and groans. I don’t experience unexplained headaches, body aches or anything else that a lot of people tend to consider ‘their lot’. I put this down to some genetic luck and of course to a diet, lifestyle & minor supplementation regime that on the whole works for me (late nights for 11th hour work deadlines aside!). The last month however has made me realise that this has probably lead me to grossly underestimate the power of those core diet and lifestyle choices that have become so automatic as to risk being forgotten. (more…)