Whenever I talk to practitioners about thyroid health, like I recently did at MINDD, I can guarantee I’m going to get 2 questions:
Shouldn’t we aim for the high iodine intake of Japanese?
Can we use the patch test for testing iodine levels in our patients?
I am so glad you asked. The answers are no and no.
I am a nutter for minerals and iodine just won’t go away right now. Too little = a problem, too much = often the same problems. To boot we are faced with radically contrasting views on assessment and dosage and just about everything iodine related. It’s not you – it’s iodine. Trust me it’s a complex little mineral that requires some extra thought and caution. If you imagine the Japanese have no thyroid problems – correct that big myth right now by reading this scientific paper that refers to health problems that result from too much dietary iodine. It also explains that the typical first step in treating hypothyroidism in Japan is to reduce their iodine intake!(more…)
Got any patients on Natural Thyroid Extracts (NTE)? Me too…and I am finding it’s on the increase. What’s the deal? What do we need to understand about this form of thyroid replacement therapy to best monitor and manage those patients already on it or contemplating taking it? Does it really offer advantages to all hypothyroid patients or just to a subset of those and how would we recognise these people who might benefit the most?
NTE are marketed as being superior to synthetic thyroxine primarily based on the fact that they provide the patient with some T3 as well as T4 and in addition to that, being extracts of pig thyroid glands, there are other thyroid and iodine based actives e.g. mono and diiodotyrosine, present in the extracts. So in essence this is giving us more iodine and more of the other ingredients we need to make our own thyroid hormones. Based on this, many proponents of NTE say this is a major advantage over synthetic thyroxine replacement because it is more ‘holistic’ and it supports the patient’s gland in its own hormonogenesis. (more…)
That’s the word on integrative medicine street. I had a sense this was coming, not just a tightening of our terminology but also a challenge of the very concept of ‘adrenal burnout’. Hear me out. (more…)
I just want to scream with joy…and then keep on screaming with utter frustration! Last week I presented the culmination of months of work looking into the extraordinary manifold relationships between thyroid health, fertility, pregnancy & post-partum health for mum and bub.
The findings are breathtaking: whether it’s about being able to put thyroid Abs firmly on the ‘Must Screen’ list for preconception care, given their ability to double-quadruple the rate of early miscarriage or their propensity for triggering post-partum thyroiditis in 50% of women who possess them or being able to state emphatically that maternal low iodine (prior to conception as well as during pregnancy) remains the number one risk for the thyroid’s healthy transition to pregnancy. The evidence is overwhelming that we need to pay very close attention to the thyroid.(more…)
Often we assume our patients know at least the basics about health – especially about things soooo seemingly basic…that we fear mentioning them would offend and make us look like someone trying to teach grandma anything! But there are some instances where I’ve found I have simply assumed too much.
I think the issue of what I affectionately call ‘Vag Care’, is right up there as an example.
Soapy water? Female deodorisers, daily panty liners, re-enacting bad movie scenes with soapy suds sex…what the??? It’s been my astonishing discovery that women of all ages, but especially a frightening majority of younger females (<30 yo), in this time of increasingly unreal ideas about sex and sexuality, feel inclined or pressured to adopt these practices in order to erase all trace of natural odour and healthy discharge. The abnormal has become normalised. (more…)
Back a few weeks ago I had the pleasure of presenting at the Integria Symposium and the even greater pleasure of listening to some of the fabulous speakers …you see I’ve heard my stuff before! 😉The ‘Mosaic of Autoimmunity’ was delivered by the very funny and knowledgeable Professor Yehuda Shoenfeld, who reiterated the sequence of events now well recognised to precede and precipitate autoimmunity: genetic susceptibility + endocrine context + environmental trigger –>autoimmunity.
Clinicians know that overwhelmingly women dominate when it comes to autoimmune disease epidemiology and most understand that this is a consequence of oestrogen’s immunostimulatory effects. Professor Shoenfeld, described the female, or E2 dominant, immune system as being ‘super charged’ and that increased rates of autoimmune diseases were a reflection of this. Sometimes practitioners do initially great work with a/immune clients – clearing up the diet & gut, ensuring vitamin D adequacy etc and then get ‘stuck’ or plateau with antibody levels that ‘won’t budge’. Going back and checking the hormonal contribution in the case is often indicated. If the patient has an unhealthy E2 dominance and /or impaired detoxification and clearance of this hormone then working on this aspect often kickstarts the next stage of improvement.
A new thing to me (I know I’m a bit slow sometimes 🙁 ) was his mention of the potential link also with high prolactin (PRL). The literature on this is extensive and hyperprolactinemia (HPRL), even just mild elevations, have been correlated with a very long list of both systemic and organ specific diseases including: (more…)
Most practitioners are pretty knowledgeable about Zinc and are quick to recognise a deficiency and the opportunities for zinc supplementation as an effective therapy and those same practitioners are often plagued by nagging questions that come up, in spite of loads of clinical experience, like:
Are plasma and serum zinc levels interchangeable?
What does zinc adequacy look like? Is it just a single number on a page or do we always have to factor in copper levels and get the ratio right as well?
What can I expect from zinc supplementation in terms of changes to the patient’s plasma zinc?
What should I do when a patient’s zinc marker is refractory to the intervention?
Is there really a significant difference between the different supplemental forms available?
I became interested in working in mental health not entirely of my own free will. I guess you could say, it had made it’s way into my world via family members and friends as well as my own problems when I was younger. So when I was at uni and I came across any information about mental illness, whether it was pathology or prescription, it was when I undoubtedly resonated most strongly with what I was learning. I’ve had some great opportunities throughout my career to feed my interest, met some wonderful mentors and some other powerful teachers who were often my patients. It’s now become a running joke among my teenage children that all my friends are either psychologists or have some sort of mental health diagnosis, ‘…and what does that say about you?’ they love to add teasingly. Well it says a lot probably: that I enjoy people who are comfortable talking about the psychology of our lives and ourselves, that I deeply appreciate that to be human is to suffer and we all suffer it’s just a question of degrees and the bravest of us share that with others. Lastly, I think it tells you that I live in the real world with real people 🙂(more…)
Recently, while I was touring around the country talking all things Acid Base (!), I spent a bit of time talking to practitioners about the limitations of our current protocols and assessment tools for detecting ‘Bad Bones’. I was surrounded by a sea of nodding heads and when I offered a solution in the form of additional bone health markers, I could see light bulbs going on all over the room 🙂
We all appreciate that osteoporosis develops over a lifetime not overnight, yet the current screening recommendation in most countries suggests that women at the ripe old age of > 65yrs and men >70yrs undergo their FIRST (!) BMD scan! The only exception to this rule is that they recommend an earlier scan in those individuals at high risk…ahem….does anyone here not have their hand up?? (more…)
“Access the Experts with Rachel Arthur” is a month long intensive webinar series focusing on the best of Mental Health Education. Every Thursday night for the month of July, Rachel will be interviewing a hand-picked guest speaker about a particular area of expertise in Mental Health.
Each speaker is a clinician with years of experience (from a psychologist, to a GP, to psychiatrists) who Rachel has worked with and/or been mentored by and she is thrilled that these interviews create an avenue to share their incredible & very practical knowledge with a wider audience.
Rachel’s role as the interviewer will be a feature of the webinar series – ensuring you get the best of each speaker; translating the complex into easy-to-understand concepts and clinically relevant content that you can start applying immediately. (more…)
Ok here’s a gripe I’m having currently. I have a number of patients who are taking anti-epileptic drugs (AEDs) and most of these are children who require them for seizure control. Naturally, working alongside such serious pathology and these critical medications requires a conservative and evidence based approach to ensure the safety of any added intervention. Fortunately, this is something I would like to think is one of my strengths. When these patients present seeking nutritional support, I typically refer them for investigations that can help to clarify what, if any, nutrients are imbalanced because of their long-term AED use or perhaps because of other independent reasons that may compromise they’re overall wellbeing. I feel that in such a vulnerable population I need to confirm nutritional deficiencies to check my assumptions, prove a need for supplementation and prevent against any excess or creation of further imbalance…and by doing so, I can adhere to my motto of least medicine, is best medicine.
The fact is AEDs are notoriously associated with a long list of potential negative nutrient interactions and the evidence to support this is extensive, this includes but is not limited to: folate, B12, B3, B6, zinc & vitamin D and the deficiencies potentially produced by the AEDs can be quite severe depending on a range of individual factors. For many of these nutrients, the research goes further and has shown that correction of the deficiency leads to better drug efficacy – therefore adjunctive nutritional monitoring and correction would seem like a real ‘win win’ situation.
(Stargrove,MB. et al. Herb, Nutrient & Drug Interactions – Clinical Implications & Therapeutic Strategies. 2008)(more…)
It’s taken a little while for me to collect my thoughts on this one. Initially there was a little flash of anger, frustration and a good deal of huffing and puffing when I heard about the RACGP guidelines recommending GPs say no to any requests from naturopaths for further investigation of their shared patients… but I’m over that now. In an interview on 702 ABC Sydney radio last week, Stephen Eddy, the vice president of ATMS, responded to these guidelines by suggesting that a blanket directive for GPs to ignore all requests from all naturopaths about all testing didn’t really sound sensible or appropriate. Here here! Surely, in the pursuit of evidence based medicine and discerning practice decisions, each case should be considered on an individual basis. I think Stephen Eddy gives GPs more credit for being able to make these judgements than their own association! (more…)
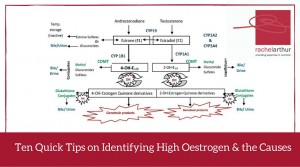
During mentoring sessions over the last week I’ve been prompted to ask a few practitioners if their patient had any signs, either clinically or in their pathology results, of high oestrogen.Each time it kind of caught the practitioner off guard because their patients weren’t presenting with conditions overtly related to an oestrogen excess and they hadn’t specifically ‘tested’ for this. However, in each instance the information was already there in the case, it was just a matter of knowing what markers to look for.
So some patients scream ‘high oestrogen’ right from the minute they enter the room? But often others present with health problems that don’t necessarily appear related at first glance. Regardless, their condition absolutely could be being compounded by this background imbalance – think thyroid & other autoimmune conditions for example.
There are plenty of patients who don’t have the exaggerated clinical presentation but still have this imbalance as a significant compounder or perpetuating issue in terms of their pathology.
Relax – I am not suggesting salivary hormones or any form of expensive testing all round (!) – in fact what I am saying is before you even consider yet another pay out of pocket test, costing your patient more time and money, we should look to the clues that are already there, in standard blood tests. Amazingly, you can infer a lot not just about the overall oestrogenic load but also pick up some clues as well about where the excess might be coming from.
In this Update Rachel brings together her 10 quick tips on how to recognise either high oestrogen and/or the potential underpinning reason behind the excess, in a range of easily accessible markers. A great refresher and synthesis of ideas on this important aspect of diagnosis and clinical management. This Update in Under 30 is now available to purchase as a download, click here to find out more or if you’re interested in a 12mo subscription click here
Most of us know that measuring a fasting blood glucose to assess how well someone is managing their glucose levels is about as crude and insensitive as waiting for the smoke detector alarm to tell you your dinner is cooked! If we wait to see an abnormal result here we’ve missed a prime opportunity for patient education and prevention long ago. Much the same story if you’re looking at HbA1c results.
To explain this I always use the analogy of a duck. A duck will always be able to swim but the question is how much effort does it have to exert to swim the same distance? If your blood glucose is within range after an overnight fast that’s as good as saying, ‘this duck can swim the length of the pond’. What it doesn’t tell you is how fast its little legs are paddling in order to achieve that. Measuring a fasting insulin at the same time, however, tells us some additional important information. It tells you how fast the duck’s legs are paddling just to keep its head above water! The more insulin you’re having to secrete to just maintain normal blood glucose levels, the more alarmed we should be!(more…)
Howdy hard working praccies 🙂 well I received a very interesting email this week from someone asking me if I thought her urinary iodine result was accurate or if, as I have written about previously (https://rachelarthur.com.au/concentrating-concentration-getting-urinary-iodine-right/), it needed to be corrected for the creatinine content of her urine. Her raw iodine result was 24ug/L which suggests severe iodine deficiency. Her referring doctor however had also asked for creatinine and applied the creatinine correction formula I have previously described:
Iodine (mcg) ÷ Creatinine (mmol) X 8.85 = Corrected Iodine –which changed her result to 265 mcg/gCR which suggests she is NOT iodine deficient at all
She then asked another doctor to review the result who had told her 24ug/L was correct in the first place as ‘pathology companies automatically correct for the concentration of the urine’. Naturally the individual found the difference in opinions and results absolutely striking and ultimately disconcerting so she thought she’d ask me.
It was good to get this email because it made me go and check my facts, get in touch with all the major mainstream pathology companies we deal with and ask their labs ‘Do you or do you not automatically correct for creatinine when you report urinary iodine results?’ I was worried I had given you guys some bad advice 🙁 …here’s what I found out:(more…)
No matter how long I am in practise there is always a group of patients for whom ‘vaginal thrush’ is a major problem. Most of us have some fabulous tricks up our sleeves to help resolve these issues & reduce their susceptibility – intravaginal lactulose is one of mine thanks to Jason Hawrelak. And then you come across those clients who vigilantly do every thing you ask them to and yet you fail to completely resolve the issue. Doh!
One of the most important things to do with all clients presenting with ‘thrush’ sooner rather than later is send them STAT (!) for a vaginal swab.
Not only does this clarify if it is in fact actually thrush (2/3 of self-diagnosed women get it wrong according to research!) but better again it names the actual culprit. It may come as a surprise but not all vulvovaginitis is due to Candida albicans – increasingly they are the result of other Candida species and this is something you absolutely need to know.
During a recent mentoring session, a practitioner wanted to better understand why she had a group of patients whose thrush seemed so resistant to her usually successful treatment. Here’s my initial response in a nutshell… (more…)
So…a 40 something female walks into your clinic with depression & anxiety…sounds common enough right? But here’s the twist: she’s already seen another practitioner who ran a range of investigations revealing she has pyrroles, high copper levels & is homozygous for the C677T MTHFR mutation. Her medical history includes significant use of Ecstasy and a partial thyroidectomy due to nodules & she has persistently high TSH. But wait there’s more!…The first practitioner upon discovering all of this put the patient on 12 different products which included zinc, B6, evening primrose oil, vitamin D, thyroid support etc etc. And guess what…the patient feels worse!
Frequently our patients are just as complex as this case & sometimes our attempts to narrow the treatment focus through thorough investigation instead leaves us feeling we now have even more things we need to deal with than before! Feeling overwhelmed?? Often! At risk of completely overwhelming the client as well? Definitely! And a reflex to throw your whole dispensary at a client never ends well.(more…)
I’m only human & there are some questions that do make me silently groan & invisibly (I hope!) roll my eyes. One is the old chestnut: “but the Japanese consume on average 7mg of iodine a day!” which is typically offered up as a rationale for the need for mega dosing of iodine in everyone. This is of course only a partial truth & the missing bits make all the difference! The Japanese have some of the highest rates of thyroid disease in the world & this is in part, attributed to their high iodine exposure. Secondly, it’s simplistic & flawed to isolate one characteristic of a whole diet & not appreciate that its effect or impact is mitigated by the context of the entire diet & lifestyle of that population. In the case of the Japanese, for example, this includes relatively intake of isoflavones, key goitrogens which will reduce the bioavailability of the iodine both within the gut & at the thyroid. Harrumph! I love iodine & am frequently suspicious of a deficiency in my clients, however, like many nutrients feel that our ultimate objective is for optimal nutrition…not excessive.
Am I just a conservative scaredy cat perpetuating fear around this topic in the industry? Well…..no. There is accumulating international evidence of big spikes in autoimmune thyroid disease diagnoses following the introduction of iodine fortification programs in previously iodine deficient countries such as Greece, Turkey & Brazil. There is of course evidence as well that iodine supplementation in Grave’s & Hashimoto’s disease can lead to delayed recovery or worsening of the condition.(more…)
Like all thyroid disease, post-partum thyroid conditions seem to be on the rise – and often they rewrite the rule book when it comes to thyroid pathology & its management. Therefore for many of us it can add an extra element of uncertainty about how to help these clients.
One of our graduate practitioners has a great example of this, a 33yo female who developed late gestational diabetes and is now struggling with a new baby and an autoimmune thyroid disease! What would you do? Does post-partum thyroiditis have unique triggers/drivers that require specific treatment? What can you/should you be doing differently because she is still breastfeeding? What’s the likely progression/prognosis?
This is your invitation to come along and find out the answers to these questions and more. During our live graduate mentoring session on Monday 15th June at 3.30pm AEST we’ll work through all aspects of the case, from history to presentation and from looking for clues in her pathology results to where to start with treatment.(more…)
Ever noticed that thing called RDW (red cell distribution width) reported in your patients’ haematology results? Given that this parameter is currently regarded as one of the most important & earliest markers of a wide range of serious diseases, you might start paying some more attention to it from now on!
Dr. Michael Hayter, cleverly refers to RDW as being a reflection of the ‘Quality Control’ of an individual’s red blood cell synthesis.
As it’s a measure of how similar or dissimilar our rbcs are in terms of size, smaller values (suggesting homogeneous rbcs) are regarded as healthy, while higher RDWs suggest that some part of rbc synthesis and/or clearance process is faulty.
This makes perfect sense in the context of nutritional anaemias like iron and B12/folate which all produce elevated RDW results but new research proposes that this rbc size disparity is also a common linking feature in just about every major disease, often predating diagnosis or in cases of established pathology signalling progression and warning of imminent poor outcomes for the individual.
There have been 100s of papers published just in the past 4 years on this topic and the findings are nothing if not dramatic. One of the biggest things I’ve realised is that, while Australian pathology companies suggest that all RDW results < 16% are acceptable, in the light of these new associations, a more accurate cut-off is probably around 13.5%! The big question now to answer is, is the increased RDW a passive marker of pathology or actively involved in the pathogenesis of these major diseases. For now, we should be scrutinising our patients’ RDW results more closely and being alert to what these markers are telling us about our clients threats & risks. I’ve recorded a 30min audio summarising all the information I’ve come across on this topic and how to apply it in your patients which you can access here.
Alternatively, if you’re happy to chomp into some juicy journal articles yourself then check out these ones to start with
 Got any patients on Natural Thyroid Extracts (NTE)? Me too…and I am finding it’s on the increase. What’s the deal? What do we need to understand about this form of thyroid replacement therapy to best monitor and manage those patients already on it or contemplating taking it? Does it really offer advantages to all hypothyroid patients or just to a subset of those and how would we recognise these people who might benefit the most?
Got any patients on Natural Thyroid Extracts (NTE)? Me too…and I am finding it’s on the increase. What’s the deal? What do we need to understand about this form of thyroid replacement therapy to best monitor and manage those patients already on it or contemplating taking it? Does it really offer advantages to all hypothyroid patients or just to a subset of those and how would we recognise these people who might benefit the most?

 Often we assume our patients know at least the basics about health – especially about things soooo seemingly basic…that we fear mentioning them would offend and make us look like someone trying to teach grandma anything! But there are some instances where I’ve found I have simply assumed too much.
Often we assume our patients know at least the basics about health – especially about things soooo seemingly basic…that we fear mentioning them would offend and make us look like someone trying to teach grandma anything! But there are some instances where I’ve found I have simply assumed too much.


 Recently, while I was touring around the country talking all things Acid Base (!), I spent a bit of time talking to practitioners about the limitations of our current protocols and assessment tools for detecting ‘Bad Bones’. I was surrounded by a sea of nodding heads and when I offered a solution in the form of additional bone health markers, I could see light bulbs going on all over the room 🙂
Recently, while I was touring around the country talking all things Acid Base (!), I spent a bit of time talking to practitioners about the limitations of our current protocols and assessment tools for detecting ‘Bad Bones’. I was surrounded by a sea of nodding heads and when I offered a solution in the form of additional bone health markers, I could see light bulbs going on all over the room 🙂