Hear ye, hear ye…Adrenal Fatigue is Dead!

That’s the word on integrative medicine street. I had a sense this was coming, not just a tightening of our terminology but also a challenge of the very concept of ‘adrenal burnout’. Hear me out. (more…)
That’s the word on integrative medicine street. I had a sense this was coming, not just a tightening of our terminology but also a challenge of the very concept of ‘adrenal burnout’. Hear me out. (more…)

I just want to scream with joy…and then keep on screaming with utter frustration! Last week I presented the culmination of months of work looking into the extraordinary manifold relationships between thyroid health, fertility, pregnancy & post-partum health for mum and bub.
The findings are breathtaking: whether it’s about being able to put thyroid Abs firmly on the ‘Must Screen’ list for preconception care, given their ability to double-quadruple the rate of early miscarriage or their propensity for triggering post-partum thyroiditis in 50% of women who possess them or being able to state emphatically that maternal low iodine (prior to conception as well as during pregnancy) remains the number one risk for the thyroid’s healthy transition to pregnancy. The evidence is overwhelming that we need to pay very close attention to the thyroid. (more…)

Have you still got some thyroid patients that don’t fit any sort of traditional thyroid disease model and are difficult to get results with? Oh yes me too… and watch out…I’ve been spending the last few weeks with my nose firmly embedded in hundreds of articles digging around for more answers. As I am presenting on thyroid conditions for ACNEM in Adelaide March 18-19th, I couldn’t resist going back to the literature to see if by delving a little deeper again I could come up with some more answers to these weird, wacky and hard to treat thyroid presentations that we’re increasingly seeing and guess what…I think I’ve found a few gems. (more…)

Back a few weeks ago I had the pleasure of presenting at the Integria Symposium and the even greater pleasure of listening to some of the fabulous speakers …you see I’ve heard my stuff before! 😉 The ‘Mosaic of Autoimmunity’ was delivered by the very funny and knowledgeable Professor Yehuda Shoenfeld, who reiterated the sequence of events now well recognised to precede and precipitate autoimmunity: genetic susceptibility + endocrine context + environmental trigger –>autoimmunity.
Clinicians know that overwhelmingly women dominate when it comes to autoimmune disease epidemiology and most understand that this is a consequence of oestrogen’s immunostimulatory effects. Professor Shoenfeld, described the female, or E2 dominant, immune system as being ‘super charged’ and that increased rates of autoimmune diseases were a reflection of this. Sometimes practitioners do initially great work with a/immune clients – clearing up the diet & gut, ensuring vitamin D adequacy etc and then get ‘stuck’ or plateau with antibody levels that ‘won’t budge’. Going back and checking the hormonal contribution in the case is often indicated. If the patient has an unhealthy E2 dominance and /or impaired detoxification and clearance of this hormone then working on this aspect often kickstarts the next stage of improvement.
A new thing to me (I know I’m a bit slow sometimes 🙁 ) was his mention of the potential link also with high prolactin (PRL). The literature on this is extensive and hyperprolactinemia (HPRL), even just mild elevations, have been correlated with a very long list of both systemic and organ specific diseases including: (more…)
During mentoring sessions over the last week I’ve been prompted to ask a few practitioners if their patient had any signs, either clinically or in their pathology results, of high oestrogen. Each time it kind of caught the practitioner off guard because their patients weren’t presenting with conditions overtly related to an oestrogen excess and they hadn’t specifically ‘tested’ for this. However, in each instance the information was already there in the case, it was just a matter of knowing what markers to look for.
So some patients scream ‘high oestrogen’ right from the minute they enter the room? But often others present with health problems that don’t necessarily appear related at first glance. Regardless, their condition absolutely could be being compounded by this background imbalance – think thyroid & other autoimmune conditions for example.
There are plenty of patients who don’t have the exaggerated clinical presentation but still have this imbalance as a significant compounder or perpetuating issue in terms of their pathology.
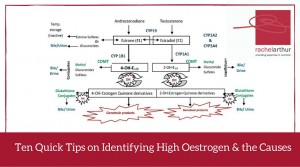
Relax – I am not suggesting salivary hormones or any form of expensive testing all round (!) – in fact what I am saying is before you even consider yet another pay out of pocket test, costing your patient more time and money, we should look to the clues that are already there, in standard blood tests. Amazingly, you can infer a lot not just about the overall oestrogenic load but also pick up some clues as well about where the excess might be coming from.
In this Update Rachel brings together her 10 quick tips on how to recognise either high oestrogen and/or the potential underpinning reason behind the excess, in a range of easily accessible markers. A great refresher and synthesis of ideas on this important aspect of diagnosis and clinical management. This Update in Under 30 is now available to purchase as a download, click here to find out more or if you’re interested in a 12mo subscription click here

We kicked off mentoring this year with some great cases last week. One was a pregnant hyperthyroid client. During the session the wonderful practitioner mentions that the client is using Withania somnifera as required for anxiety.
Insert sound of brakes screeching to a dangerous squealing crash! Here’s a situation where I would give Withania a miss. (more…)

Howdy hard working praccies 🙂 well I received a very interesting email this week from someone asking me if I thought her urinary iodine result was accurate or if, as I have written about previously (https://rachelarthur.com.au/concentrating-concentration-getting-urinary-iodine-right/), it needed to be corrected for the creatinine content of her urine. Her raw iodine result was 24ug/L which suggests severe iodine deficiency. Her referring doctor however had also asked for creatinine and applied the creatinine correction formula I have previously described:
Iodine (mcg) ÷ Creatinine (mmol) X 8.85 = Corrected Iodine – which changed her result to 265 mcg/gCR which suggests she is NOT iodine deficient at all
She then asked another doctor to review the result who had told her 24ug/L was correct in the first place as ‘pathology companies automatically correct for the concentration of the urine’. Naturally the individual found the difference in opinions and results absolutely striking and ultimately disconcerting so she thought she’d ask me.
It was good to get this email because it made me go and check my facts, get in touch with all the major mainstream pathology companies we deal with and ask their labs ‘Do you or do you not automatically correct for creatinine when you report urinary iodine results?’ I was worried I had given you guys some bad advice 🙁 …here’s what I found out: (more…)
No matter how long I am in practise there is always a group of patients for whom ‘vaginal thrush’ is a major problem. Most of us have some fabulous tricks up our sleeves to help resolve these issues & reduce their susceptibility – intravaginal lactulose is one of mine thanks to Jason Hawrelak. And then you come across those clients who vigilantly do every thing you ask them to and yet you fail to completely resolve the issue. Doh!
One of the most important things to do with all clients presenting with ‘thrush’ sooner rather than later is send them STAT (!) for a vaginal swab.
Not only does this clarify if it is in fact actually thrush (2/3 of self-diagnosed women get it wrong according to research!) but better again it names the actual culprit. It may come as a surprise but not all vulvovaginitis is due to Candida albicans – increasingly they are the result of other Candida species and this is something you absolutely need to know.
During a recent mentoring session, a practitioner wanted to better understand why she had a group of patients whose thrush seemed so resistant to her usually successful treatment. Here’s my initial response in a nutshell… (more…)

We had a great case in one of our graduate mentoring sessions the other day (thanks Kate 😉 ) , about a 40 something mum of 3 who reported to have cyclical mood and depression. Further investigation of the case, however, revealed that some of the key characteristics of the mood disorder were actually anger, aggression, irritability, hyperactivity, vivid nightmares etc. This particularly came to light with her responses to a mood survey that the practitioner had asked her to complete. I think validated tools like this (esp. DASS), when used appropriately, can give us enormous insight – often revealing things we might not have thought to ask about or that the client might not have voluntarily offered up, particularly if they are not socially accepted or attractive qualities.
If you practice anything like me, then Vitex is an absolute reflex response (think the very funny reflex paper ad – that’s me in my clinic!) & godsend for most cyclical mood issues. However, apart from the fact that this woman’s key period of mood aggravation, although clearly related to her menstrual cycle, was day 5-14 rather than during the late luteal phase, there was another stand out reason for me why I definitely wouldn’t use Vitex. (more…)
So…a 40 something female walks into your clinic with depression & anxiety…sounds common enough right? But here’s the twist: she’s already seen another practitioner who ran a range of investigations revealing she has pyrroles, high copper levels & is homozygous for the C677T MTHFR mutation. Her medical history includes significant use of Ecstasy and a partial thyroidectomy due to nodules & she has persistently high TSH. But wait there’s more!…The first practitioner upon discovering all of this put the patient on 12 different products which included zinc, B6, evening primrose oil, vitamin D, thyroid support etc etc. And guess what…the patient feels worse!
Frequently our patients are just as complex as this case & sometimes our attempts to narrow the treatment focus through thorough investigation instead leaves us feeling we now have even more things we need to deal with than before! Feeling overwhelmed?? Often! At risk of completely overwhelming the client as well? Definitely! And a reflex to throw your whole dispensary at a client never ends well. (more…)
I’m only human & there are some questions that do make me silently groan & invisibly (I hope!) roll my eyes. One is the old chestnut: “but the Japanese consume on average 7mg of iodine a day!” which is typically offered up as a rationale for the need for mega dosing of iodine in everyone. This is of course only a partial truth & the missing bits make all the difference! The Japanese have some of the highest rates of thyroid disease in the world & this is in part, attributed to their high iodine exposure. Secondly, it’s simplistic & flawed to isolate one characteristic of a whole diet & not appreciate that its effect or impact is mitigated by the context of the entire diet & lifestyle of that population. In the case of the Japanese, for example, this includes relatively intake of isoflavones, key goitrogens which will reduce the bioavailability of the iodine both within the gut & at the thyroid. Harrumph! I love iodine & am frequently suspicious of a deficiency in my clients, however, like many nutrients feel that our ultimate objective is for optimal nutrition…not excessive.
Am I just a conservative scaredy cat perpetuating fear around this topic in the industry? Well…..no. There is accumulating international evidence of big spikes in autoimmune thyroid disease diagnoses following the introduction of iodine fortification programs in previously iodine deficient countries such as Greece, Turkey & Brazil. There is of course evidence as well that iodine supplementation in Grave’s & Hashimoto’s disease can lead to delayed recovery or worsening of the condition. (more…)
Like all thyroid disease, post-partum thyroid conditions seem to be on the rise – and often they rewrite the rule book when it comes to thyroid pathology & its management. Therefore for many of us it can add an extra element of uncertainty about how to help these clients.
One of our graduate practitioners has a great example of this, a 33yo female who developed late gestational diabetes and is now struggling with a new baby and an autoimmune thyroid disease! What would you do? Does post-partum thyroiditis have unique triggers/drivers that require specific treatment? What can you/should you be doing differently because she is still breastfeeding? What’s the likely progression/prognosis?
This is your invitation to come along and find out the answers to these questions and more. During our live graduate mentoring session on Monday 15th June at 3.30pm AEST we’ll work through all aspects of the case, from history to presentation and from looking for clues in her pathology results to where to start with treatment. (more…)
One of the most common questions I’m asked is whether I have a ‘set list’ of tests that I request for every patient. Of course there is no ‘one size fits all’ in health & each patient presents with their own novel combination of issues & investigative challenges, however, years of clinical experience have taught me which pathology parameters are the most clinically meaningful.
Asking yourself, ‘Will the results of this test determine my thoughts about treatment & therefore ultimately the clinical outcome for my patient?’, before referring for any investigation is a good habit to get into.
Many of us are increasingly aware of the changing environment around pathology testing, which includes reduced access to some tests in mainstream pathology. Rbc folate has had its subsidy withdrawn which means if we request this we’re now likely to receive a serum value or nothing. But does this matter? (more…)
We should all be as skilled in investigating & treating male hormone imbalances as we are female ones, yet this is often not the case. A lack of confidence in this area, which seems to be an issue for many, in particular will compromise our ability to question male clients comprehensively and effectively about their reproductive health and ultimately reduce our capacity for making good clinical decisions and achieving the best outcomes for them. If you’re female, how would you feel seeing a male practitioner who doesn’t ask you about your menstrual cycle in detail?
Many of us are at risk of committing similar crimes but we need not be. (more…)

Thyroid function is critical to successful conception, healthy pregnancies, babies and mum’s post-partum wellbeing, so we need to take the time to ensure we’re monitoring it properly.
First of all you need the right tool for the right job & that means we need trimester specific reference ranges – which unfortunately many pathology companies don’t use in Australia. Due to the thyrotropic action of HCG (acting a bit like TSH), TSH should actually decrease in the 1st trimester and while TSH is less affected in 2nd and 3rd trimesters it should still actually sit lower than in non-pregnant females. (more…)
We now suspect that many of the drivers behind PCOS are heritable components – a genetic vulnerability passed from parents, possibly one but often both. This growing understanding has identified a phenomenon referred to as ‘PCOS families’ i.e. a family in which at least one female has confirmed PCOS.
Being a primary biological relative of someone with PCOS, it would seem, suggests a shared risk, even if you are a son, or brother or father.
So beyond the very high rates of undiagnosed PCOS in sisters of someone already diagnosed, there is much talk now about a male PCOS phenotype equivalent. (more…)
As we head rapidly towards the change over of our calendars we would like to offer you a special on the very best educational recordings from 2014 – buy 2 CDs before Jan 31st and receive one complimentary Premium Audio Recording of your choice OR purchase 4 CDs and receive a 3 month Premium Audio subscription for free.
It’s been a busy year during which Rachel has delivered 7 very successful new seminars in the area of mental health and beyond, most notably fortifying her role as a leader in the field of diagnostics and pathology interpretation. This has included collaborations with ACNEM, Biomedica, Health Masters Live, MINDD and Nutrition Care, however, each recording is classic Rachel – full of fresh perspectives on diagnosis & treatment, colourful analogies & humour. In case you missed some of these this year or want a copy for keeps – here’s a quick summary of the 2014 recordings included in this end of year offer: (more…)
We’ve just had another mentoring case in which a 40 something female with deficiencies of almost all other minerals but ‘pretty normal ferritin levels’ presented with a range of endocrine problems and arthralgia. Sounds as if iron’s not the problem right? Except that in this case her iron studies also tell us that her transferrin saturation % on last check was 48%. The diagnostic criteria for hereditary haemachromatosis (HH) necessitates elevated ferritin – to indicate that the iron stores are reaching saturation, however, while this becomes evident at relatively young ages in men (20s-40s), who have no specific excretory pathway for iron, is this still appropriate in menstruating female, whose monthly periods may mask the HH tendency with regard to ferritin? I’m guessing you know what my answer is already! 😉
Some would argue that HH, in spite of being an inherited disorder, is only clinically meaningful once the ferritin is elevated ( earlier and more potent elevations are seen in people possessing the C282Y genotype) but again this is very much up for debate in the current scientific literature, with a lot of research concluding that the transferrin saturation (also referred to as the transferrin ratio) being an important prognostic indicator for various chronic diseases including CVD.
When we go back to basics and remember the higher the transferrin percentage the more iron is being delivered to tissues around the body (whether they like/want it or not! so we refer to this as being ‘iron dumping’) and the higher the serum iron, the more unbound iron is in the system – a key source of oxidative stress..it becomes patently clear that these two parameters are important early warning signs of a tendency to iron overload, increased risk of heavy metal toxicity and already active mineral imbalance. So in future keep your eyes open for women with fasting transferrin saturation values that consistently sit above 35% and men, > 40% and if you do see a series of suspicious values – consider the genotype test through mainstream labs.
Apologies for having a one-track mind currently but yes I’m still banging on about the thyroid this week. You see, this year in my own clinic I connected up some dots I hadn’t connected before via a series of young female patients. Each of these women presented with some hypothyroid features, most notably, low basal body temperatures, fatigue and weight gain and while their thyroid hormones (TSH, T4 and T3) were all technically ‘within range’, their T3 levels were very low (low 3s) and the TSH seemed to sit low as well (<1.5). Normally of course, when T3 levels drop we expect TSH secretion from the pituitary to rise in response, as a means to correcting this dip, however, this part of regulation appeared ‘blunted’ or even ‘broken’ in these women.
So why would their pituitary be sleeping on the job, allowing them effectively to experience long term suboptimal thyroid function? (more…)
Just been speaking on the thyroid at ACNEM last week and am finding that practitioners across the board are getting more and more curly thyroid cases. One scenario that we increasingly see is something that might be described as ‘T3 resistance’, when your patient’s T3 value looks healthy but they continue to manifest the signs and symptoms of hypothyroidism. There are several differentials to consider of course (more…)