Wow, menopause is really having a moment, isn’t it? Or is that just me (and my mates who are all somewhere on that perimenopausal path)?! But seriously, medical perception of this reproductive transition is undergoing a revolution right now—widening the lens to take in more diverse potential presentations and lengthening the period of impact recognised both ‘before, during, and after’ that last, last…no hang on…last period. But I fear we are at a crucial crossroads. Anything could be related to (peri)menopause, but not everything is or should be.
There are several other conditions whose onset tends to rise or peak at the same age and stage for women, and due to their shared features, they get missed & misdiagnosed, misattributed to that!(more…)
The debasing of BMI as a stand-alone assessment of weight is long overdue given its significant limitations and lack of meaningfulness with respect to overall health. This coincides with a bigger societal and cultural shift towards inclusivity which involves redressing bias against people with diverse body sizes and compositions.
And how do we, as integrative health professionals, continue to uphold our principles of prevention and treating the cause when excess adiposity may be a very real contributor? While ensuring we ‘see’ and treat each individual in front of us, not our assumptions about adiposity, not our body size bias nor blind spots?
One part of the answer: read and be led by their lab results – because pathology is nothing if not personalised.(more…)
What level of Serum Ferritin represents ’empty’? As in complete depletion of iron stores?
Is it any value below the minimum of the reference range? e.g. < 30 mcg/L Or does the bottom of the reference range allow for a buffer and ’empty’ is substantially lower than this? Could patients actually be ’empty’ but still have Serum Ferritin values within the normal range? Could the same Serum Ferritin value occur in one patient on ’empty’ but with adequate stores in another?
Ever met a set of thyroid results you didn’t like? Because you couldn’t work them out? Because they defied your expectations, & therefore your understanding, of how they should look in this patient given their weight, nutrition, meds, diagnoses? Yeah – me too.
In simple terms this is because we are taught ‘perfect patterns’ in thyroid interpretation: * Iodine deficiency produces HN (high-normal) TSH and a shift towards T3 *Inflammation produces low TSH and T3 with a shift towards rT3 *Viral attack of the thyroid itself causes HN levels of both T4 & T3 due to spillage of preformed hormones, & secondary suppression of TSH
So can I ask: What about the patient who has a virus that is causing significant inflammation, attacking the gland directly but has a pre-existing Iodine deficiency? Seriously. What would you expect to see as the HPT responds to all of these concurrent disruptors?(more…)
Any pathology test is only of value if the result produced is ‘real’, or, representative of that individual, right? So the timing of the test is a major pivot point then: do I tell my patient to present for the test, or collect the sample themselves, on their ‘best’, their ‘worst’ or their ‘average’ day? 🤷♀️ Well, that all depends on the question you are trying to answer.
Whenever we reach or refer for a test, we have a question in mind we’re seeking an answer to. But the question always comes in two parts, at least.
Part 1: How much progesterone is she making? Part 2: …When she’s ovulated & her corpus luteum should be most productive?
A third might refine the question you’re answering further by adding another contextual clarification
Part 3,4,5: …When she’s eating her regular diet, not exercising excessively or under extreme stress
Without these other parts – the answer to the first one: How much progesterone is she making (full stop), is hard to correctly interpret, right? By refining and expanding on the full extent of our question, we can be clear about which elements of this patient’s life the result likely reflects. We might say that for her, this time-point, or set of collection conditions, is a ‘real reflection’ of her generally and therefore, representative. But what if she does occasionally undertake a 5 day fast, or train for & compete in marathons? If we were to specifically test during these times, we answer a different question, right? Likewise every time we instruct a patient to present for their blood tests (routine or fancy schmancy): Fasted, Rested, Hydrated and off their supplements – is this sound advice or a misdirection? Well it depends on the individual in front of you and the real question you want answered about them 🤓
Ahhhhh I love rules: both the making of them and the subsequent breaking of them 🦜🏴☠️
The collection conditions for any pathology test – can refine or ruin the question you were hoping to have answered about your patient but is it always appropriate to ask everyone to ensure their preparation for the test was ‘ideal’? What if their real life is far from ‘ideal’ and contrasts dramatically with these ‘conditions’ e.g. they forget to drink water but never alcohol! Or do they run 20km every weekday and 40 on weekends? And why would we tell some patients to stop their supplements prior to a blood-test and not others? If our goal is to ensure any pathology test answers the question we need answered we need to know how to respond to these and other scenarios. This new update is all about keeping results ‘real’ & representative.
You can purchase Fasted, Rested, Hydrated & Unsupplemented? Exceptions to the Rulehere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
Burning, tingling, crawling, buzzing, humming, zapping, pins & needles, numbness: our patients often tell us about strange sensations they have in various parts of their body. It’s typically not their major concern, but they mention it as an aside, a curiosity, ‘another weird thing I get’. While they may have trivialised this, relative to their ‘real issues’ [insert gut, hormonal, mental health] we should do the opposite and bring this concern to top of the list to correctly identify the cause.
If bilateral sensory nerves are mis-messaging it typically means 1 of 2 things: 1. Nerve damage is occurring – and if allowed to progress this can become irreversible or extend to motor and central deficits 2. Nerves are irritated or impaired – and this tells you something ‘systemic’ is out of whack and these sensations are often the only alarm bell
The top cause of paraesthesia, falls into the first category and is of course diabetes – and yes even now diabetics will walk into your clinic not knowing they have this (a good old HbA1c should be routine to rule this out). Second on the list is alcohol dependence. The third most likely explanation for the patient with paraesthesia is nutritional. And in contrast to what many of us might incorrectly think, there is a long list of nutritional imbalances that can be responsible for either, nerve damage or irritation, and B12 deficiency is not in fact the most likely.
That’s right all you nutritional ninjas🐱👤 – that makes the correct identification of the cause & the solution our bag, right? I mean who else is going to do this, accurately?
Asking the right questions about these sensations helps you to quickly confirm when a nutritional cause is likely. From there we need to know how each single micronutrient excess or deficiency or in the case of some, ‘sort of single’ nutrients (we all know people who sit in this category, right?! So why not nutrients 😂) are likely to present, via ‘easy-to-spot’ key characteristics that cover: pattern of distribution, speed of onset and progression, risk factors, accompanying features etc. In our final New Graduate mentoring session for 2021, a practitioner presented her patient who rated her concerns as 1) Fatigue 2) PMS 3) GIT issues & 4) Tingling & crawling sensations across limbs, face, lips and tongue…and I was like, whoa stop right there, you might just have given us the answer to all of the above~!~! Seriously. Here’s a clue: it wasn’t oral allergy syndrome and it wasn’t B12. Can you pick it?🤓
The Patient with Paraesthesia – Part 1 Patients often mention experiencing peculiar sensations: crawling, tingling, burning, as an aside, as a ‘oh and by the way’. But while it may not be their top priority – it should be ours. That’s because nutritional imbalances are the 3rd most common cause of these and timely treatment is essential to prevent progression to more serious issues. The list of potential nutrient deficiencies and excesses behind these, is long, but this recording, the first part of 2, will help you narrow the differentials, nail the diagnosis & the solution.
The Patient with Paraesthesia – Part 2 In this continuation of this topic, we discuss several less talked about nutrients whose deficiencies drive potent pathology for the nervous system & move onto a cluster group of minerals, whose imbalances create functional irritation rather than organic change. This episode includes a range of excellent resources from videos demonstrating in-house tests you can perform to aid diagnosis, as well as our own Ready Reference which assists correctly categorising the different paraesthesia patterns and the nutrient issues behind them
You can purchase The Patient with Paraesthesia Part 1here and Part 2here.
BUY PART 1 & PART 2 TOGETHER AND RECEIVE 10% DISCOUNT BY USING CODE BUNDLE12
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
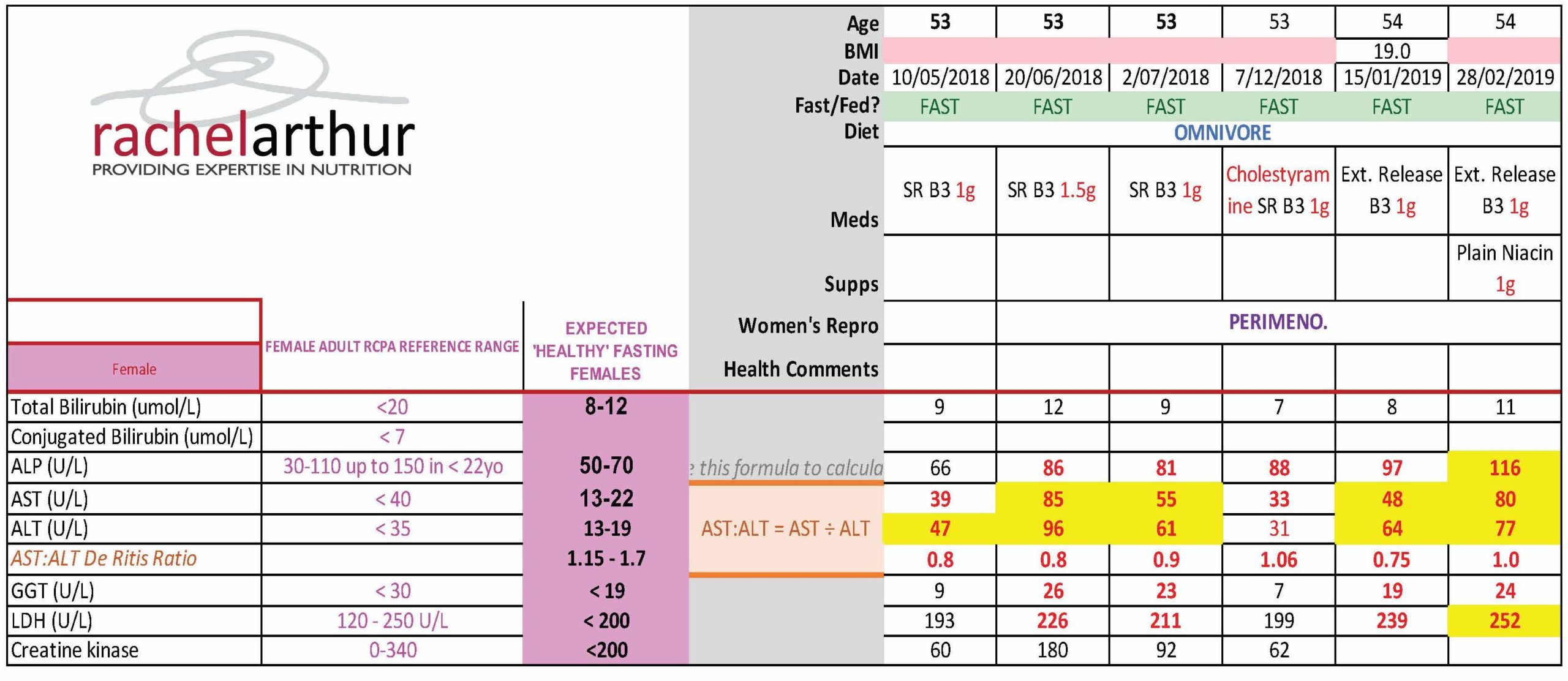
You know when you learn about a ‘new’ dis-ease driver and then you actually have to stop yourself from diagnosing every patient with it? I’ve done this dance with Gilbert’s Syndrome for over a decade, so too maybe have some of you? And while there have been many, many occasions when I’ve been certain it’s Gilbert’s (clear robust & reproducible patterns of high bilirubin without other explanation) there are other times when I’ve been left wondering, and with questions. Like – what about a fluctuating pattern – sometimes ‘within range’ sometimes above or at least high-normal – with no other explanation? What about the patient whose symptom-story is a perfect fit – prone to nausea, early satiety, gut issues, food reactions and anxiety all worse for increased oestrogen…but the total serum bilirubin is 14 micromoles/L? I mean, 14, right? that’s well below the top of that range, but remarkably higher than the majority of women of the same age, eating the same diet. And you ask yourself…could it…be??
It could.
The latest UU30 offering on Gilbert’s Syndrome constitutes a complete overhaul of everything we’ve previously been told about how to recognise and diagnose this polymorphism & it’s going to answer a lot of those ‘could it be’ questions we’ve all had! Known also as familial non-haemolytic jaundice and episodic hyperbilirubinaemia under stress – is everyone with Gilbert’s prone to jaundice? Uh, no. Total bilirubin levels typically have to get to 45 micromoles/L to evoke this effect – many of our GS patients won’t ever get there, some will with increased illness or other stress and may yellow a tad (like a fading bruise), while other patients of mine routinely have a bilirubin at this level but won’t experience jaundice unless they impair their UGT further via doing what they know they shouldn’t: extreme exercise or excess alcohol. The latest deep dive into GS diagnostics
But as much as we don’t want to miss this diagnosis we don’t want to mis-diagnose patients with it either!
Can you spot the difference? Don’t forget total serum bilirubin levels are the net result of haem catabolism – so you need to account for rate of blood production, destruction and of course rule out any biliary dx before you can take a guess at Gilbert’s. Oh and watch out for expected high bilirubin values in the fasting fan(atic)s!
For those people living with Gilbert Syndrome at last the research world & the real one are uniting – with greater detailed documentation of how this very common polymorphism presents and the mark it may make in their health story. However, given only 1/5 with Gilbert’s syndrome actually know they have this condition, who are we missing? This latest instalment rewrites our diagnostic criteria and corrects our past misunderstandings based on the very latest science, while shedding further light on what it’s like to live in Gilbert St.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
[Ahem] Ok let me explain…Several catch-cries from Australian ads have earnt themselves a lifelong place in my head and heart, taking up space where something more important should be, no doubt, but does anyone remember this SPC canned fruit (REALLY showing my age now!!) one, where the little boy chases the grape around the bowl and declares it a, ‘Slippery Little Sucker!’? Ok so this little boy is every one of us when we’re trying to ‘capture someone’s cortisol’ and just like the boy we will eventually achieve a ‘result’ – get a ‘number’ but what in fact does this mean in relation to your patient’s HPA axis, stress perception, responsivity, recovery etc etc?
Recently I was presented with 2 cortisol results for a patient taken within the same 24hrs – her blood am result was above range, while her 24hr urine flagged under-functioning of her HPA axis generally. Both were accurate.
Had I have only have seen one, I would have formed the wrong opinion and only gleaned part of her overall HPA story. Every different type of cortisol capture – from different mediums: blood, saliva & urine – to different collection conditions: time of day, fasting V fed, specific stressor exposure etc answers a different question about our patient’s HPA axis. So to use any form of cortisol assessment well we need to start with 2 understandings: 1) it is a slippery little sucker indeed and no one test can answer all our questions – or as Miller & colleagues more eloquently put it, “Remember, all models are wrong; the practical question is, how wrong do they have to be to not to be useful” and 2) be clear about the most important question you have about your patient you are trying to answer and that will make your choice of test (& timing & & &) patent. But do you know enough about cortisol regulation to be clear about the ‘sweet spot’ of each test?
The Cortisol Awakening Response has understandably attracted the bulk of the research focus over the last decade and accordingly has risen in popularity in practice & while it remains a very valuable way to answer certain questions about patients, our understanding of its limitations continue to grow. For example there is a disconnect between CAR & diurnal cortisol secretion – so in essence your CAR can look woke but your ‘Slope’ may be broke! If you’re a fan of this method, make sure you catch up on the CAR-Expert Consensus Guidelines by Stalder et aland if you’d like to get clear about which test and when, when it comes to all the key options for Cortisol Capture..
then let’s dive in together with my latest Update in Under 30 instalment
I have! And just recently a stark contrast between the results from 2 different methods of cortisol capture in the same patient illustrated just how likely this is. How do we ‘capture’ something so ‘dynamic’ and interpret anything of substance from a ‘static’ assessment technique? But rather than throw up our hands and throw out the whole attempt to measure cortisol, we can improve the rigor, reliability and real-world meaningfulness of our patients’ results by refining our timing of tests, choosing the medium wisely & manipulating test conditions to answer specific questions about their HPA function. Great desktop reference included!
You can purchase Cortisol – Have You Been Caught Out?here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
What’s your knee-jerk response to 52Y Lipids Lucy & Liver, whose ALT & AST suddenly jumped above range when she was put on statins? They’re damaging her liver? You’d be wrong. One of the practitioners who undertook the MasterCourse in Comprehensive Diagnostics just graduated with flying colours when she was able to correctly identify the true cause of this patient’s LFT abnormalities, can you?
[Cheeky hint: there is more than one explanation/process at play]
This naturopath now knows her pathology patterns. She knows the interpretation of any liver enzyme must also take into account the movement in other markers, to make meaning of the whole. Because so-called ‘liver enzymes’ are never exclusive to the liver. They are expressed in multiple other tissues and organs – sometimes at equal concentrations to their liver-level (e.g. ALP and bone). For some, even referring to them as a ‘liver enzyme’ is a mislabelling of sorts, with minimal expression in the liver itself compared with ubiquitous distribution all over the body (e.g. GGT & LDH). Of course this is both a blessing and a curse. A curse if you make the mistake of only interpreting their levels through a ‘liver lens’…a blessing if you know when they are flagging problems elsewhere through the specific pattern recognition. So back to Lucy – the statins had induced a rhabdomyolysis not hepatocellular damage. The clues? Significant AST dominance over ALT, above range CK and LDH.
So if the statins weren’t causing increased hepatocellular damage what is that increasingly high-normal ALP pattern all about?
Bones. And again, this practitioner picked it. And then got to win herself some pretty BIG credit and credibility points with all the other health professionals sharing care of this patient by suggesting that they clarify and confirm this by referring her for an ALP bone isoenzyme assay, which answers the question: is the elevated ALP originating from the liver, the intestines or from the bone? Bingo, bones it is! Or was, because this practitioner was able to alert not only the patient but all the other practitioners treating her to the increased bone remodelling taking place, independent of the statin reaction, but part of her perimenopause. Left unchecked this would escalate further of course at menopause and leave her bones in bad shape. This is just one illustration of how we can show ourselves the be the incredible one we are on the shared-care team.
Being lab literate and pathology proficient, sets you apart from the rest and enables you to practice truly preventative medicine. How else would we have known she was experiencing increased BMD loss that may be the start of something truly tragic?
Realise the true value you can extract from the most commonly performed labs. Join Rachel Arthur LIVE on the MasterCourse I: Comprehensive Diagnostics WATCH PARTY This skill is the biggest ‘game-changer’ in Integrative Medicine! Want to know more? Head over to my website here and check out more of the great benefits and bonuses of joining this program This course is a fantastic learning opportunity to identify the many intricacies in cases that have previously been missed.
We have been madly working towards our anticipated December 2020 release. We’ve been in our own little cone of silence, busy editing over 20 hours of videos, putting together resources and extra bonus audios.
We’re really excited because we’re in the process of building, for the first time, quite an amazing comprehensive training package in diagnostics, that we know will not just serve, but surpass, integrative practitioners of all persuasions’, educational needs in this area. We wanted to let you know flooding, storms and resultant internet failure will not deter us from getting it done, but these forces of nature have slowed us down a little 🙄
So we now have a new release date of January 2021.
We’ve set the bar high and want this to be as fabulous as possible and ensure that the content translates cohesively from what were very dynamic live interactive sessions to an excellent ‘off the shelf” DIY learning experience so…. take the rest of the year off people!” Step away from the computer and enjoy time with your family during the festive season. You deserve it.
We wanted to thank you for your patience and know it will be worth the wait…
“Absolutely loved this course, I’ve listened to each of the recordings at least 3 times now taking furious notes and am still picking up new gems. Love that it’s helping me build up my knowledge and confidence in such a fundamental area of practice. The case studies are super valuable as they bring the labs to life, I’d be keen for more of these! Really appreciate all the extra PDFs / audios that have been added also. Eagerly awaiting MasterCourse II” – Naturopath | Australia
“Why wasn’t this content covered in medical school? As a psychiatrist, I have greatly benefited from attending this course which comprehensively covers the ins and outs of interpretation of pathology labs and how this applies to clinical cases – many of which have both physical and mental health considerations. I believe all doctors from general practitioners to specialists will gain from attending! ” – Psychiatrist | Australia
“Thank you so much for this course, it has been brilliant. It has ‘fuelled my practice’ and many people have benefited already – from such insights. It’s quite thrilling!!! I’ll definitely be signing up for the second course later next year” – Naturopath, Medical Herbalist | New Zealand
What does lockdown look like for you? More time spent…
A) Learning or B) Losing sleep over things outside of our control or C) Losing days just watching Tik Tok
I’m choosing ‘A’ and I know I’m keeping good company because last week many of my ‘nearest and dearest’ gathered on 2 occasions for some serious extra brain gym. The first was the ACNEM Fellowship Community of Practice that I had the privilege to co-chair with Dr. William Ferguson. A fantastic new initiative by @ACNEM to offer more hands-on mentoring and support to their doctors.
The second, our own Give-back-Gratitude Live Q & A for our Update in Under 30 Subscribers where I used the time to check-in and see if we could further the learning offered by our monthly audios and clinical tools.
Having all of those who attended, in my ‘home’ was a fabulous contrast to our social distancing ‘new norm’, and seeing all those lovely faces and buzzing brains behind them, warmed the cockles of my cortex!
For those of you that couldn’t make our UU30 date, I wanted to share a few things we learned in lockdown this week:
Copper can be absorbed through the skin and penetrate to deeper layers potentially increasing serum levels butthe degree of uptake is highly variable and more likely with prolonged contact e.g. jewellery and pastes not showers etc
Just like the Zn:Cu, when reviewing patients’ albumin:globulin, we must first look at each value individually and consider causes and consequences of low or high values, otherwise we can ‘miss the message’
When understanding labs of anybody who is not a couch potato we need to ditch reference ranges based on the general population because they essentially are…couch potatoes and ask ourselves 3 questions: 1) Whois this person outside of being ‘sporty’2) Whatis the nature of their sportiness because exercise ain’t exercise in terms of physiological effects and 3) When are the tests being done in relation to any exercise
On that last note, I am so thrilled to be able to share my brand spanking new presentation The Impact of Exercise on Pathology Tests – Beyond Artefact to Understanding which I put together B.C. (Before COVID19) for a NZ speaking engagement. This actually has been one of the most satisfying areas of research to expand my own knowledge in…explained a LOT about what labs go whacky (and why and how to navigate around and through this) not just in what you might call ‘real athletes’ but in weekend warriors, crossfit crazies, MIL (men in Lycra) and the increasing number of middle-aged or older women who just love pounding the pavement. Know the types? Our clinics are full of them…it is time to learn their labs properly.
Overwhelmingly when we look at our patients’ labs we compare their results with a reference range derived from ‘the general population’ aka couch potatoes! Therein lies our first problem. Exercise is recommended for health but we don’t know what this ‘looks like’ in terms of labs. The reference ranges reflect and assume ‘average’ muscle mass & haemodynamics & ‘average’ nutritional requirements in people consuming the SAD (standard Australian diet) none of which apply to the exercise enthusiast, weekend warrior, least of all the professional athlete! Given an increasing number of our patients are embracing exercise, this is an important instruction in what healthy looks like, how to make meaning of otherwise meaningless comparisons and ultimately enable you to distinguish between what is healthy exercise-induced adaptation, an artefact and an actual aberration that flags possible negative impact of emerging pathology for other reasons.
Click here to add The Impact of Exercise on Pathology Tests to your online RAN Library.
For all UU30 Subscribers the full Live Q&A Recording is now available in your ‘active content’ of your online account.
When you start doing this with your patients’ pathology results, you know your client records are turning into a big hot mess and more importantly your ability to see the wood for the trees is seriously under threat! Private labs don’t play nicely with one another and if your patient has been to more than 1 pathology provider you lose an enormous amount of their potential value, blindsiding you to their patterns, & the most accurate interpretations. I have a saying when it comes to getting the most out of pathology in your practice: Cumulative Data is King & Context is Queen.
Increasingly we’re in in the fortunate position of patients taking responsibility for their health and coming armed with lab results – this cumulative data helps us to clearly see their ‘norms’ (as opposed to textbook ones) and therefore also any noteworthy variations.
But even in this luxurious position of multiple results across a variety of time points & stages of their life – our ability to derive the greatest understanding from these is greatly stunted if we don’t have the context.
For example: if he was ‘cross-fit-keto-crazy’ at the time, if she’d stopped being pregnant & started breastfeeding, if in light of a major shift in thyroid hormone results, they were on biotin, or iodine, or changed their dose of thyroxine or were drinking straight from the udder of a soybean (!) these all seem like fairly critical contextual details to be across, right? All of these factors: diet, acute health context, medications, reproductive state, even season… impact the lab results we expect to see and therefore should be captured and considered to form the most accurate interpretation. But how do we pull it all together in a systematic way that SAVES us time and SAVES your sanity and can keep growing alongside your ever-growing patient notes? Cue the: RAN Patient Pathology Manager!
Systems for sorting through huge amounts of patient information help us make sense of what we’re seeing…and help us spot the source & solutions.
Systematised patient timelines for a better overview of the chronology of any case, the RAN Patient Pathology Manager not only holds all the data for you, helping you keep more accurate records & make the most correct interpretation from these, but also maps and monitors changes related to various interventions. Lastly there’s my old BFF, Mindmaps and Timelines not ancient torture tools of clinical supervisors (!) but rather what distinguishes us as integrative, enabling us a to work up a case in a truly holistic fashion instead of: symptom–> solution, symptom –> solution. These are the 3 key clinic systems I really wished I’d had from the get-go…so, me and my team created them! We’ve re-crafted them with each year and this year our RANPatient Pathology Manager has undergone a significant evolutionary leap and it comes with a comprehensive video explaining how to easily get the most out of this resource for all your patients. We always share these tools with all our mentees but we’re frequently asked how others can access them so this year we thought those of you out there just wanting a foot up with some better systems might like to get your hands on them too! Maybe this is one very practical part of the ‘new year new you’?
It’s that time of year when we tend to set our intentions both personally and professionally. For me, between the many meals, pressies and dunks in the river, I slip into some ‘silent work’. In particular, I find myself flagging a couple of key areas that I want to sharpen my knowledge in this year. I’ve already picked mine…have you identified yours?
For many practitioners if there is one topic in nutritional medicine that seems to be more generous than any other it would have to be iron: Iron gives us patients…loads of them! Patients who present with deficiency, with overload, with something in between but still noteworthy, or on iron and that’s causing them all sorts of problems.
But Iron’s generosity doesn’t end there.
It also tends to give a lot of practitioners a bit of a headache!
That’s because a) we were mistakenly taught about iron as if it were just another one of the mineral mob and accordingly allocated grossly inadequate time to do more than scratch the surface of what we need to know and b) what we need to know, thanks to it being the most researched mineral, has undergone a couple of major revelations and revolutions since then anyway! So we can benefit from Iron’s generosity most and leave its other unwanted pressies (the headaches, confusion, frustration & suboptimal management of patients) under the tree – we just need to give iron the real attention it deserves, filling in the gaps in ours and many people’s knowledge about this critical nutrient. And boy, do we (and I mean everyone!! including doctors, midwives, pharmacists…anyone who has ever called iron deficiency on a client!!) need to learn how to correctly read iron studies!!!
Because iron also gives us much needed insight into other micronutrients and just how exquisitely sophisticated their roles & regulation can be. Thanks to it being one of the ‘older minerals’ we know more about it than any other and in turn we have the most advanced assessment methods: Iron studies, a collection of 4 parameters, like 4 chapters in a book or 4 key characters in a play, that need to be viewed separately and then together to understand the whole story.
Yes it’s true the learning doesn’t ever end and as I’ve continued to learn about new iron research I’ve added to our one-stop-iron-resource-shop..the Iron Package. Our very latest edition? A new clinical cheat sheet with some other important numbers on there you want to have at your fingertips whenever you read iron studies. So if you’ve already purchased and have access to the Iron Package…SURPRISE! 🤩 Go back and look again and if not, there’s never been a time like now. Oh iron, you’re sooooo generous!! 😉
Listen to these audios and download the resources straight away in your online account.
If you’ve already purchased ‘Update in Under 30: How to Read Iron Studies’ or ‘Iron Package’ you will find this new clinical cheat sheet available with these audios when you log in to your account.
Behind their deceptively-dated inkjet printing and boring black and white font (punctuated occasionally by a comparatively thrilling red H or L)mainstream pathology results actually offer a goldmine of information and insight about your patients….if you know where to look. And even the most seemingly status quo reference ranges for routine labs reveal so much, if you understand how to identify when results are ‘expected’ or even ‘optimal’, as opposed to ‘unexpected’ or ‘the new (ab)normal’, reflective of an increasingly unhealthy population. Because unlike measurements of beauty, wealth or intelligence…more B12, TSH, GGT etc. etc. is not necessarily better and in fact being ‘average’ may sometimes be the aspirational goal 😉
Many holistic practitioners feel unnecessarily ‘locked out of labs’ due to inadequate training or, even worse, the false belief they are not relevant to their naturopathic work-up but they are abundant in holistic insights about our patients.
You can change that today and start developing your mild naturopathic super-power in diagnostics.
“Rachel – I have to say thank you, thank you, thank you!! That session on pathology was epic. It has really made me look at each set of path results I have seen in a different context. In terms of relevance – a definite 10/10. Everything from the reference range info to looking for any clinical and collection notes – definitely gives more scope in mining for those answers. Can’t wait for the next session 🙂 “
Chris Hibbert (Group Mentoring Program 2019)
To boot, upskilling just a little in accurate pathology interpretation will help you write better referral letters, practice true individualised medicine and sort the real from the rubbish in terms of all the **whizzbang-bright-sparkly-functional tests** you and your patients are being offered in spades.
“I’m totally enjoying the pathology sessions. I use pathology in my clinic all the time but have learnt so much from these last couple of sessions and I know I can squeeze out a lot more. I’m a convert (within reason) to the idea of many of the OS functional medicine practitioners who prescribe to the ‘test don’t guess’ motto and that pathology highlights the body’s ‘debris’ which can lead us to a certain pathway, system and help us go back up stream to the point of origin. I feel that’s the unique value we add to our clients’ health. Thanks Rachel.”
Elke Jesdinsky (New Graduate Mentee 2019)
We need to start with a good grasp of ‘lab language’ and have the veils of mystery around reference ranges removed so we can make the most out of all these results our patients already have, if not in their hot little hand then in their equally hot not so little (!) medical records.
Mainstream pathology results actually offer a goldmine of information and insight about your patients. However to realise their full value and make the most accurate interpretations we need to first learn more about ‘lab language’, upskill in finding our way around reports which are packed with a surprising amount of hidden extras, demystify reference ranges and then develop a logical critical process we can apply to every result of any patient to get the real take-home. Packaged with numerous specifically developed resources to aid in your application of these skills this is a foundational offering that changes practices.
 Wow, menopause is really having a moment, isn’t it? Or is that just me (and my mates who are all somewhere on that perimenopausal path)?! But seriously, medical perception of this reproductive transition is undergoing a revolution right now—widening the lens to take in more diverse potential presentations and lengthening the period of impact recognised both ‘before, during, and after’ that last, last…no hang on…last period. But I fear we are at a crucial crossroads. Anything could be related to (peri)menopause, but not everything is or should be.
Wow, menopause is really having a moment, isn’t it? Or is that just me (and my mates who are all somewhere on that perimenopausal path)?! But seriously, medical perception of this reproductive transition is undergoing a revolution right now—widening the lens to take in more diverse potential presentations and lengthening the period of impact recognised both ‘before, during, and after’ that last, last…no hang on…last period. But I fear we are at a crucial crossroads. Anything could be related to (peri)menopause, but not everything is or should be. The debasing of BMI as a stand-alone assessment of weight is long overdue given its significant limitations and lack of meaningfulness with respect to overall health. This coincides with a bigger societal and cultural shift towards inclusivity which involves redressing bias against people with diverse body sizes and compositions.
The debasing of BMI as a stand-alone assessment of weight is long overdue given its significant limitations and lack of meaningfulness with respect to overall health. This coincides with a bigger societal and cultural shift towards inclusivity which involves redressing bias against people with diverse body sizes and compositions. 


 Burning, tingling, crawling, buzzing, humming, zapping, pins & needles, numbness:
Burning, tingling, crawling, buzzing, humming, zapping, pins & needles, numbness: