For all those Mentoring Virgins 😇out there wanting a clearer understanding of what it’s really like to be part of my group mentoring, this video is a little snippet from a session with one of my groups. This year has flown by and I have thoroughly enjoyed working with each fabulous group of dedicated ‘life-long learners’.
OH YES!!…and the real announcement is…..(drum roll)… It’s that time of the year….Applications open next week for GROUP MENTORING in 2020!
As a result of the generous feedback and insights from our current Mentees, we are always fine tuning our program & level of service. Yep…it just keeps getting better and better every year!! We are keeping everything that so many practitioners have told us they love from the past 7 years (wow….have I been doing it for that long?!) and simplyimproving the already incredibly popular formula, with some great new features for 2020.
New 15min Follow up with one on one with me! via Zoom for those cases that have been presented in our group mentoring sessions. This is a brand new format to follow up on how your client is going after the session – what’s working, and what’s happening now, what should you do next? Rachel will spend 15 mins with you on Zoom 1-2 months after you presented your client case. The recording will then be uploaded to Basecamp so the whole group can catch up on the progress and extend our learning opportunities again.
We’ve expanded our mentees 30% discount to ALL Rachel Arthur Nutrition products on our website for 2020.When you join the Group Mentoring Program, you will receive a discount code that you can use for any and all purchases on Rachel’s website throughout 2020– the Update in Under 30 subscriptions, Audio and Video recordings, Packages on Pathology, Thyroid, Iron.
Certificate for CPE Hours– we’ve done this for the last 2 years and will continue to do so to make your CPE easier at your end
General and Specialist Groups – we’ve had a great response to our specialist groups this year, and we are offering these again in 2020, so you can choose from:
General Group Mentoring–our regular case presentation groups, with practitioners taking turns to present a case, or just listen in. Yes, this ‘fly on the wall option’ which we’ve come to learn is preferred by some praccies (due to a lack of time, good cases or confidence) is finally getting formalised for 2020!
GP dedicated Group – this depends on our final numbers of applicants for 2020. This year we had a combined group of GPs and naturopaths with advanced standing, which has worked well. Either way, we have a good track record in catering to the needs of doctors, medical specialists and dual qualified naturopaths (osteo, psychology etc).
New Graduate Groups – great opportunity for New Grads to build confidence as they leap from student to practitioner, or for practitioners wanting to refresh their core clinical skills such as MindMaps, Pathology, Improved Case Taking etc.
Mental Health Primer Group – topic based to build on your knowledge in the role of naturopathic medicine in Mental Health – from screening tools to key management issues, specialist diagnostics and beyond.
Mental Health General Group Mentoring – practitioners presenting their client cases with a focus on primarily Mental Health presentations.
“I believe the mentoring you are offering is allowing me to develop myself into the type of practitioner that I want to be.
I really aim to provide evidence based treatments, and wish to utilise pathology testing results as one of the major diagnostics in my practice. I can see that every mentoring session with you brings me closer to that, filling my knowledge gaps every time. You and your knowledge base is so inspiring, and I only hope that one day I will know close to some of what you know!” – Andrea Robertson
And don’t forget some of the offerings our Group Mentoring consistently delivers as part of your program – the opportunity to learn every month via high level applied knowledge not theoretical and to see it in action with tracking and updates on patient progress, our incredible online resource sharing platform for communication and support between sessions and the opportunity for sharing of pearls of knowledge from my 20+ years of experience and research together with the collective wisdom and know-how of each unique group.
“I am one of Rachel’s New Grad mentees. My first year out has been pretty overwhelming and I wanted to let Rachel know that I have been watching the zoom sessions and have learned so much to take my clinical confidence and practice to the next level. She has an amazing gift of nailing the important aspects of practice and giving useful usable information that brings together the fuzz of everything you have learned and ties it all up with a neat bow with her pearls of wisdom every month. I plan to be a mentee again next year (and for many years I suspect)” – Bek Di Mauro
REGISTRATIONS OPEN 14 October!
To read more about the program click here. Information on how to apply will be released on 14 October. Join the waiting list now so you won’t miss out by sending us an email on [email protected].
Forehead USB not required. Phew. All that is required, is a real thirst for new knowledge, rapid development of your diagnostic skills and a willingness to commit an hour every month to tap into your new Brain’s Trust: Rachel and a collection of colleagues with a shared desire (general practice or mental health-focused) and similar level of experience to you – new graduate, medical, naturopathic or dual qualification. And take one great leap forward closer to being the practitioner you want to be.
The Rachel Arthur Group Mentoring Program has the longest (7 years and counting!!) and most impressive track record of practitioner satisfaction for value for money and meeting clinician’s key learning outcomes.
And the long-awaited good news is…we will offer our New Graduate Program, which debuted this year to much critical acclaim, again in 2020!
Being part of the 12-month group program allows you to connect to a community of like-minded, similarly-skilled practitioners in a structured teaching environment either via case-based presentations (regular groups) or via an interactive curriculum (New Graduates, Mental Health Introduction). You’ll be plugged into 11 other practitioners and together with Rachel’s brain, you’ll receive the knowledge and confidence to assess, investigate and manage no matter who and what walks through the door. Our profession thrives when we thrive as individuals and central to this is building networks of ‘similar others’ in order to find your tribe and benefit from the ‘collective’.
“Rachel is a wealth of information, she has such a knack for breaking down cases. All case presentations no matter how complex are nicely deconstructed into bite sized bits of information that’s easy to digest and take away and put into practice. This mentorship program is worth its weight in gold, it shows you how to deconstruct cases, develop knowledge, gain greater clinical insights and you’ve got a fabulous base of other knowledge practitioners you can ask questions. Can’t wait for the rest of the cases! And you can count me in as a second year mentee next year.” – Megan
In Group Mentoring you’ll be learning core clinical skills that you can apply in realtime to your practice and be able to ask questions along the way. The most valued aspect of the mentoring is the ability to discuss practice experiences with the mentor and to hear and learn from all the group members, sharing experiences, knowledge and learning as we go during the sessions.The bonus of these sessions is you’ll find your tribe, gain support and radically build your toolkit.
I love witnessing every practitioner’s growth, I want everyone to find mentors to support them in their career in integrative health. – Rachel
“Having the group session each month, as well as having Basecamp to bounce ideas around in, is a reassuring connection to know is there if I need it. Having just started practice this year and working in an environment without other Nat’s around, I have noticed the occasional feeling of isolation. So having the monthly catch up keeps me feeling connected to other clinicians and gives me exposure to other cases and perspectives that I wouldn’t have otherwise had.” – Georgie
Going by the landslide of registrations for 2019, Group Mentoring is fast becoming a popular choice and could be an integrative part of your practice & your career progression.
So if being part of the community excites you and if the thought of learning and benefiting from a collective knowledge base that is strong and pulls on expertise outside of our own, now’s the time to join the conversation through Group Mentoring.
Tonic. Homeostatic modulator. These terms and concepts, which have a long tradition in herbal medicine (and let’s be clear, were considered yet another example of the wishy-washiness of the modality) are being appropriated by some areas of mainstream medicine right now. Cheer up ‘leaky gut’, you’re no longer alone! And arguably misappropriated by the public’s very ‘lay’ interpretation of the science on medicinal cannabis and its subsequent elevation to panacea, of late.
“So many of my patients are telling me they’re taking Cannabis now, just as a tonic”, says yet another practitioner to me recently, “No, not for pain, they’re young and fit but they take it because it’s a homeostatic regulator!!”
Oh lordy…
The capacity to maintain homeostasis, and particularly in the face of adversity or imbalance, is a sign of the vitality of the individual, according to what I remember from naturopathic philosophy (and have truly taken on and observed firsthand)…so just back up there a tad and explain to me how this one herb proposes to do this for everyone on a one-size-fits-all-fashion? As confessed in an earlier communication, I am a cannabis convert. But only in the sense of appreciating the niche areas where it is likely to offer true therapeutic benefits. I still have the words of warning from the brilliant Professor Michael Lintzeris, the Director of the Drug & Alcohol Services, South East Sydney Local Health District; Conjoint Professor, Division of Addiction Medicine etc., ringing in my ears, pleading with health practitioners to not ‘fall’ for cannabis in the way we have previously ‘fallen’ (so far and landed so badly) for the panaceas of the past: opiates and benzodiazepines. Most notable major omission for me, in an otherwise rigorous scientific debate of late, is any discussion about its potential for impacting fertility.
There is in fact evidence to suggest ‘sperm under the influence’…’lose their way’ and are less effective at finding and fertilising the egg. Sorry but the image always makes me chuckle…stoned sperm. ‘Hey, dude where’s my egg?!’ style. But it’s not funny when impaired fertility is a problem affecting so many these days, and we still are guilty of over-focusing on ‘her’ and under-assessing ‘him’…and lo and behold it could be his chronic cannabis use to blame. We had a case recently, years of unprotected sex, daily cannabis, no baby, no dots connected. We may think this is a handy incidental contraceptive for young men sitting on couches with cones (one mum recently said as much to me) but for the rest…?
As practitioners we should know as much about investigating and treating male hormone imbalances as we do female ones, yet this is often not the case. While we are increasingly aware of everyone’s exposure to lifestyle & environmental endocrine disruptors and the fragility of the HPO axis, we sometimes fail to recognise that the reproductive health of our male patients is equally under threat. This is clearly demonstrated by generally diminishing levels of testosterone amongst men and increasingly early onset of andropause. These issues then become barriers to achieving success in other health areas with your clients, mood, metabolism, fertility and beyond. Learn more here
I’d love to continue this conversation with you… so join me and be part of my ongoing dialog on this and my other blogs by following my Facebook page.
Following an important weekend of discussing mental health from a more balanced perspective (that’s my new less provocative term for ‘integrative’ or dare I even mumble…holistic) in Perth for ACNEM, I remain alert but not alarmed of how much is still to be revealed in this area. Recently, for example, in our mental health dedicated mentoring group, we discussed a case of a somewhat atypical schizophrenia presentation in a middle-age female migrant. Fortunately, I co-chair these sessions with an incredible clinical psychologist who was quick to pick up that no CNS auto-antibodies had been tested, and given the peculiarities of the case they should have. This is a relatively new area, in terms of more mainstream acceptance of this as a differential in some psychiatric presentations and provision of these tests now through mainstream labs, but it would appear it is far from common knowledge. Then I read this brilliant article and…well I think we all need to read it. Here are some snippets…
“Scientists had previously noted that certain autoimmune diseases, such as lupus, were associated with psychosis. And they’d begun to suspect that some infections might, by activating the immune system, contribute to psychiatric conditions. But Dalmau provided meticulous proof that the immune system could attack the brain. The development of a test for the disorder, and the fact that very sick patients could recover with treatment, prompted a wave of interest in autoimmune conditions of the central nervous system. In total, scientists have identified about two dozen others—including dementia-like conditions, epilepsies, and a Parkinson’s-like “stiff person” syndrome—and many experts suspect that more exist…
Robert Yolken, a scientist at Johns Hopkins University, estimates that about one-third of schizophrenics show signs of immune activation (though he adds that this could be related to other factors, such as smoking and obesity). And autoimmune diseases are more common among schizophrenics and their immediate families than among the general population, which could hint at a shared genetic vulnerability.”
There are some potent practical take-homes in this article embedded especially within the story of an 11-year-old boy who was admitted to hospital with profound psychiatric features – initially misdiagnosed and managed as BPAD and later found to have autoimmune encephalitis. First and foremost: psychiatric conditions develop gradually. When there is an acute onset in the absence of an acute trauma – the possibility of a biological (esp autoimmune) driver should be elevated in your differentials. And the mother of this boy, now aged 21 and having undergone 5 relapses and recoveries in between, virtually echoes the thoughts and findings of Carl Pfeiffer half a century ago, when she says, “Too often, psychosis is seen as the disease itself but psychosis is like a fever, it’s a symptom of a lot of different illnesses.” Important for thought.
Could dairy intake in susceptible individuals be a risk promoter for mental health problems? In addition to evidence of the exorphin derivatives from certain caseins interacting with our endogenous opiate system discussed in part 1, we now look at the evidence in support of other milk madness mechanisms. Specifically, the IgG and IgA antibodies about what this tells us about the patient sitting in front of us about their gut generally and about their mental health risks, specifically. The literature in this area dates back to the 1970s but the findings of more recent and more rigorous research are compelling. Find out more here.
I was at the Medicinal Cannabis (MC) in Mental Health Conference run by GHI on the weekend and I have to confess, I inhaled. Seriously, deeply, inhaled. Just as I had hoped, this was a very high level of information on this important topic, delivered by outstanding presenters: from authorised Australian MC prescribers, to the head American researcher of the largest MC trial to be run in psychiatry – from brilliant pharmacognosists whose every day is spent immersed in complex cannabis chemistry to our very own national (naturopathic) treasure, Justin Sinclair. I left there with thousands of words typed into my laptop, and about a thousand more in my brain, spilling out onto anyone who stood still long enough. Ahem…thank you my dear tolerant family & friends 😉
Let’s be clear. I am not in a position to prescribe medicinal cannabis. Nor do I want to, right now. But like me, patient purchases off the green market in response to DIY diagnosis and prescribing are on the up and up. I have felt concern and apprehension about this but not known enough to engage in any conversation. Now, watch out… I’m finding my words!
I left the conference with a much clearer sense of the patients and presentations for whom it may prove medicinal – most obviously for those conditions outlined in the WHO review including nausea and vomiting in cancer and pain refractory to other analgesics. In addition to this, we were privileged to hear from a mum and son who have had to employ cannabis for the last half a dozen years following his diagnosis of an inoperable brain tumour, that originally robbed him of his literacy, his joy of reading and his overall quality of life, with high frequency seizures and intractable vomiting etc. MC has remarkably given much of this back to him. And I remain optimistic about future potential uses in psychiatry – especially within certain PTSD cohorts thanks to this small but promising study by Greer et al in 2014. Inspired by this paper and her extensive experience treating war veterans with PTSD, Dr. Sue Sisley, who spoke at the conference, executed a similar study of 6000 veterans for a MC inhalation trial. I’ve got a spoiler for you…the study failed – publication pending.
But before you add 1 + 1 and get 3.879…let me tell you, there is nothing as powerful and revealing as hearing researchers talk firsthand about their trials. When Sue put up actual photos of the medicinal cannabis they were supplied with for this study…the room collectively let out a giant Gasp!
It was brown, full of stem and…wait for it…mould. Yup. But that is what they, and as Sue poignantly pointed out, & what every other group of American researchers who run studies on MC as opposed to synthetics or extracts, have to use. So…are any negative outcome a surprise? No. But it will no doubt be interpreted as a sign that we shouldn’t pursue research in the area of MC and PTSD. We should. Have I completely ditched my concerns about negative mental health impact from cannabis? Absolutely not. And Professor Michael Lintzeris, the Director of the Drug & Alcohol Services South East Sydney Local Health District; Conjoint Professor, Division of Addiction Medicine etc., spoke eloquently & comprehensively to this inherent duality of this herb in this regard. Even the most isolated and lauded (non-intoxicating) constituent of cannabis can be both help and hindrance to anxiety and depression sufferers and most clearly, Michael warned us not to make MC the opiates and benzodiazepine panacea promises of the past, buying the rhetoric of ‘no tolerance, no dependence, no risk’. How each individual’s mood and mental state responds to MC, whole plant, extracts or isolated constituents, from anxiogenic to anxiolytic and from depressant to antidepressant, has been clearly demonstrated to differ according to genes, ‘endocannabinoid tone’, route of administration and dose. Seems like all roads lead to an individualised health care approach & prescription…yet again 😉
Need a road map to think your way through the integrative work-up of your Mental Health patients?
In Mastering Mental health: New Assessments & Management Resources in your Clinic, Rachel introduces you to new clinical tools that she has been developing to help us all better master the maze of mental health. With so many possible biological drivers: from methylation to inflammation and from gonads to gut, these tools can help you quickly identify those most relevant to each patient and also outline the strategies necessary for redressing these. This presentation comes with an extensive library of resources including pdf of Assessments Tools and Case Study Notes.
Integrative Psychiatry is an inspiring area to work in & its evidence base, acceptance and recognition of potency is rapidly growing & offering more patients, more. Going beyond the ‘neurotransmitter imbalance model’ for each presenting diagnosis helps us to see the unique mix of biological & psychological drivers in each individual who presents seeking our help. However sometimes I believe, we find ourselves falling into looking through the lens of just another short-list of alternate models:What kind of methylation imbalance does this person have? What sort of Zn, Cu issues?
While I am so grateful for having learned these tools and watched them be very successful in a portion of my mental health clients, they are simply not the answer for everyone. We need to keep our thinking and practices dynamic and up to date, to reflect the incredible increase in research in new areas of integrative psychiatry, such that more of our patients can benefit and that we can continue to think beyond the box…even if that box itself was originally so progressive!
What do you know, for example, about abnormal purine metabolism in mania and using serum urate as a BPAD prognostic marker in depressed patients? Think you can simply be guided by the reference range provided, think again. What could good old LFTs reveal about our patient’s mental health vulnerabilities and what have we potentially misunderstood about copper in this area, particularly in children?
I appreciate Zinc’s role in mental health as much as the next integrative practitioner. Okay, given my 20K word thesis manifesto, more. But increasingly I am seeing mental health patients who need treatment with different tools. This upcoming ACNEM Mental Health Module in Perth is on point: thinking outside of, outside the box!
While the above only speaks to what I’m presenting, I know Dr. Sanjeev Sharma will also be sharing his wealth of individualised management insights and he’s a big fan of addressing Chronic MIld Metabolic Acidosis as an early treatment objective. Maybe we all need to hear why? And I am so looking forward to getting a PTSD update from Christabelle and hear all about the research into therapeutic keto-diets in psychiatry from Cliff Harvey…haven’t read all those papers to know which conditions and when this approach shows merit? No, most of us haven’t. That’s the point of outsourcing our up-skilling to colleagues who we know are across these more than us and to boot have the clinical experience to ‘make real the research’. As I’ve said before, given the content of this upcoming ACNEM Mental Health program, I wish I wasn’t presenting really, so I could just kick back and take it all in, uninterrupted. But alas, I have some important new information on reading basic bloods through a mental health lens to share! I really hope to see you all there. Let’s get out of the rut of 3-4 nutritional approaches to mental health and make the most of the explosion of research and shared clinical experience.
ACNEM Face-to-Face Training Fremantle, 27-28 July 2019 at the Esplanade Hotel Fremantle by Rydges https://www.acnem.org/events/training
Oh and while you’re here…did you know the research into both beta-casomorphins and IgG casein reactions in relation to certain mental health diagnoses has taken some giant steps forward in the last couple of years? You should. Milk Madness is back and it’s via two distinct mechanisms – identifying which might be at play in your patients & correct management is now clearer than before. Want to get up to date in this area of mental health – check out our UU30 recordings: Milk Madness part 1 & part 2
b. Every herbalist’s jaw at my table at the NHAA conference gala dinner, when I got almost all my Latin binomials right during the trivia quiz?…and after some champagne, that’s a particular achievement
c. My jaw, when I saw firsthand how much those herbalists could drink of ye-not-so-olde herbal extracts!!
d. The latest Update and Under 30 – Milk Madness Part 2
e. All of the above
If you answered, ‘e’…. you must have been one of those herbalists at my table, otherwise you have way too much insider information! But yes you are correct on all accounts. So this latest UU30 is an extension of our discussion last month about the potential contribution from to mental health from dairy intake in a subset of patients. This whole topic, the research for which dates all the way back to the 70s, was too big to fit into one – given the current evidence base that now depicts at least 2 different mechanisms that might be at play, and the different types of mental health problems, each has been linked with. Last month was all about retracing the ‘dietary exorphin’ path, this month it’s about the propensity for some individuals to make antibodies to casein and the significant growing data that suggest this happens to a larger extent in patients with certain psychiatric diagnoses. More importantly, we talk about the ‘why’.
What compelled me to make time to look through all the literature on this was that there is some. No seriously. When I initially learned of the GFCF dietary approach to ASD patients I was told that in spite of a lack of supportive research, the empirical clinical evidence was irrefutable, which I later saw with my own eyes. In the couple of decades since, I only really heard about negative findings, short trials of the elimination diet specifically in ASD kids, that failed to produce significant change. Funny how the bad stories rise to the top, right? But when I spent the time doing a thorough literature review, I found these negative findings were far from the whole story. In fact, I was really surprised by the high level of evidence employed by researchers of late, who have repeatedly found associations between either exorphin or antibody levels and patients with particular diagnoses, in addition to really progressing our understanding of why these measurable differences (urinary exorphins, plasma IgG and to a lesser extent IgA casein antibodies) are meaningful. Do we know everything? What do you think? The answer, of course, is always no. But we know enough to consider this aspect in our comprehensive workup of mental health patients and all their biological drivers and we know dramatically more than anyone in mainstream medicine, or the dairy industry for that matter, is ever going to let on!
If you want to hear a synthesis of the casein antibody link with mental health then download the latest UU30 – Milk Madness – part 2. If you can’t go that far, then “do yourself a favour” and read a couple of seriously important articles on this topic – and why not start at the deep end with this study by Severance in 2015.
Could dairy intake in susceptible individuals be a risk promoter for mental health problems? In addition to evidence of the exorphin derivatives from certain caseins interacting with our endogenous opiate system discussed in part 1, we now look at the evidence in support of other milk madness mechanisms. Specifically, the IgG and, to a much lesser extent, IgA antibodies about what this tells us about the patient sitting in front of us about their gut generally and about their mental health risks, specifically. The literature in this area dates back to the 1970s but the findings of more recent and more rigorous research are compelling.
So this is not news to most people who know me but I don’t like taking things out of people’s diet. As a result, in a room full of naturopaths & integrative medicos, I might be voted the least likely to use the phrase, “No Gluten or Dairy for you!” [said with the Soup Nazi’s accent from Seinfeld]. I must have slept through that class when we were taught to do this for absolutely every patient. But seriously, I try not to remove or exclude foods without a very strong rationale and evidence-base that relates directly to the person sitting in front of me, for several reasons: 1) those seeds are powerful ones to plant in your patient’s mind…how do they carry that with them as they move through life, navigating food and social settings etc etc…all well and good if this is a proven life-long pathological provocation for them but otherwise… 2) dietary exclusion is stressful for families & in kids especially, can create disordered eating and a range of other psychological impacts and 3) GFDF diets are not necessarily healthier in the basic nutrition stakes…if you haven’t read Sue Shephard’s work on the deterioration of diet quality in GF patients…you should. It can be much healthier of course…but often the real-world application of the principle doesn’t always match the lovely ‘serving suggestion image’ on all the GFDF highly processed, packaged foods!!
So listen up people, because now I’m talking about when I would seriously consider joining in on the GFDF chant.
The one patient group I’ve never quibbled over the benefits of GFDF, has been the autistic one. I was taught the merits of this approach early on by a few fabulous courageous integrative doctors and paediatricians who came back from the front-line of their clinics, reporting good effects. I then had the important firsthand experience of unprecedented verabilisation in a non-verbal ASD child’ after excluding these foods. But what I’ve been thinking a lot (and reading a lot!) about lately is the possibility that these ‘dietary exorphins’ may have negative mood effects in other subsets of mental health patients. My thought process is like slow TV! That aside, there’s a lot to be said for taking the time to really getting across an issue – even if that involves reading papers from as far back as the 1960s when the idea of a negative role for dietary exorphins in schizophrenics was first floated by Dohan & colleagues.
Let me say, when you go back to the beginning it’s undeniably a shaky start for the exorphin evidence base, but as you read the studies that emerge from decade to decade until the noughties…it reveals a nagging research topic that won’t go away and a fascinating process of discovery.
So is the devil really in the (regular commercial cow’s) milk? Well I think for some patients it may well be a contributor – most notably those with features consistent with the pattern of excess opiate effects including a higher dopamine picture, regardless of the mental health label they’ve been given, although, more commonly seen in ASD, psychotic presentations etc. But how do we work out which ones, because none of the evidence points to it affecting 100% of these groups…well that’s where we need to go back and truly understand the structure of these dietary exorphins and just how they potentially wreak havoc in some.
The latest UU30 takes your through the story of BCM-7 with a summary of research compile over half a century in Under 30 minutes!
There is a well-rehearsed chant in the integrative management for ASD individuals, “Gluten free- casein free diets” is based on the dietary exorphin theory which suggests these foods generate bioactive peptides that act unfavourably in the brain. Where did this theory emerge from and how strong or weak is the evidence upon which this therapeutic intervention stands? Even more interesting, is there support of this theory in a wider range of mental health presentations such as schizophrenia, post-partum psychosis and depression. Is there such a thing as milk madness for a subset of our patients?
Hear all about it by listening to my latest Update in Under 30: Milk Madness – Is it a thing? For all Update in Under 30 Subscribers, it’s now available in your online account and if you are not a subscriber you can purchase this individually here.
Hear Hear…on all levels, right. But this is actually the first recommendation of an easy to read patient resource for families dealing with adolescent depression, that you and your patients can access here. As lovely as the picture above makes parenting look, the one to one (or even 2 to 1) ratio isn’t realistic or necessarily optimal for anyone. I think we can all make a great addition to any parent’s team, especially given the emphasis these recommendations place on nutrition, sleep and exercise as being central to improving mental health…full-stop..and in this age group.
But while some things are the same between depressed adolescent and adults, there are important differences we need to be aware of: like the best assessment tools and the barriers for teenagers (and parents) in admitting there is an issue. Think, parent guilt and over-attribution, standing defiantly on the top rung of that ladder!
They also mention different types of therapy for this age-group and I have to say the old CBT…oh yes it gets wheeled out yet again…really does offer something, given the kind of kids I’ve seen this work a treat on. This is a developmental staged characterised by curiosity and a desire to understand more about the real stuff of life…rather than the soft focus lens we got them to look through in primary school. I’ve seen teenagers benefit enormously from sitting with a good psychologist or GP who can explain the ‘brain mechanics’ of depression, or anxiety (amygdala activation that sends the frontal lobe executive control offline etc). They love the demystification and, in the best cases, feel re-empowered by this knowledge. Not perfect for every teenage but it does work for many. And then there’s the parental advice to discuss suicidal ideation.
Yes parents, even more than practitioners, fear the ‘planting of seeds’ when contemplating this topic with their teens but the opposite is true. This paper is hot on the heels of an editorial, revealing that 50% of parents were unaware of their teenager’s suicidal thoughts.
There is much to be gained from the ‘knowing’ and so much to lose from avoiding this one. It’s the beginning of another school year (at any level) and with this can bring significant stressors and provocation for mental health challenges. Let’s encourage every parent, to get themselves a team and take our own place in that invaluable roadside assist crew.
This is a succinct recap of the many investigative paths we need to follow when presented with kids or teenagers with behavioural disorders. From grass roots dietary assessment through to the key pathology testing that is most helpful in clarifying the role & treatment approach of integrative nutrition for each individual child.
Finally a systematic review puts paid to the nonsense that ‘withdrawal from antidepressants’ is problematic only for a few, is ‘mild’ & ‘lasts only 1-2 weeks’ with no treatment necessary other than reassurance, which is still being perpetuated by current prescribing guidelines both here and overseas. In fact their review found that 56% of patients experienced problems with stopping antidepressants and the majority of these rated these as ‘severe’. Back in the good/bad old days when I worked for a pharmaceutical company who made psych meds the phenomenon of an ‘initiation phase’ during which time suicidal risk was heightened, was acknowledged and freely discussed…in-house at least. However, the concept of a ‘withdrawal syndrome’ was less clear. Anyone who has witnessed patients coming off ‘even the cleanest’ SSRIs will speak to a potential myriad of worrisome experiences including…
“Typical AD withdrawal reactions includeincreased anxiety, flu-like symptoms, insomnia, nausea, imbalance, sensory disturbances, and hyperarousal. Dizziness, electric shock-like sensations, brain zaps, diarrhoea, headaches, muscle spasms and tremors, agitation, hallucinations, confusion, malaise, sweatingand irritability are also reported (Warner, Bobo, Warner, Reid, & Rachal, 2006, Healy, 2012). Although the aforementioned symptoms are the most common physical symptoms, there is also evidence that AD withdrawal can induce mania and hypomania, (Goldstein et al., 1999; Naryan & Haddad, 2011) emotional blunting and an inability to cry, (Holguin-Lew & Bell, 2013) long-term or even permanent sexual dysfunction (Csoka & Shipko, 2006).”
Previously termed ‘discontinuation syndrome’ by expert panels – to distinguish these inconvenient effects from the more seriously viewed (read nasty) benzo-associated discontinuation problems – was an act of smoke and mirrors, according to this scathing and insightful review by Davies and Read, who argue strongly this is a clear cut withdrawal picture and it deserves as much consideration and concern. In particular they point out that of course, patients can experience these symptoms even without ‘discontinuation’ – but simply as a result of a delayed or skipped dose, an intentional dose reduction etc. And they provide the alarming context that one third of people in the U.K. (and likely similar developed countries) who take antidepressants for more than two years have no evidence-based clinical indications for continuing to take them. But wait..I’m just getting to the worst bit, this is the part that gets me personally…having been a peddler in the past of these meds and in certain patients still spruiking their benefits, I am in no disagreement about them being necessary, helpful & even life-savers in some patients…yes I have seen this too many times to ignore it…BUT…and now this is where I start raising my voice a tad….
Patients need to make informed choices, and having a clear understanding of what you are likely to experience on any given medication has been shown to improve outcomes but according to the 2 largest surveys conducted to date,< 2% of antidepressant users are being told any of this. Do you know why? Well, let’s start with the misleading guidelines… if the RACGP says it isn’t so…then can we expect their GP to know or say any differently?
Grrrrrrrr…. yes that’s me…not a wild animal in the room with you.
Because you know what happens in the absence of this?! And let me say I have also seen this too many times to ignore as well, people feel compelled to stay on them & this is truly heartbreaking to witness. The experience of a reduced dose or a period without is so terrifyingly disconcerting to that poor unsuspecting individual, and without explanation, is misinterpreted by them (and according to this review often by their doctor as well!!) as being either a sign of their inherent mental instability and need for ongoing medication, or misdiagnosed as a separate condition. Ok…apologies, this is over a decade of pent up frustration…resurfacing as a result of reading this incredibly important and disturbing review. I think I need a little lie down now 🙁
Helping patients off anti-depressants is a challenging and important function that must be initiated by the patient with the full support of the prescribing practitioner, however there’s a role for complementary medicine here too. Rachel walks you through a range of strategies and when you might consider each. Listen to thefree samplehere from the Update in Under 30 from 2013 – Leaving Anti-depressants Behind. Or perhaps you’re interested in all things Mental Health and should find out more about our specialist mentoring group running in 2019.
Forever fascinated by the neurobiology of various mental health presentations, addiction included, two medical news items caught my attention this week. If you’ve ever heard me speak on addiction, in somewhat simplistic terms, it is very much about the reward centre of the brain and how strongly all recreational drugs hit on this. Think rats tapping levers with their feet to continually self-administer cocaine…to the exclusion of all else….kind of magnitude of reward hits. You may have also heard me quote or misquote (!) someone famous who once said something to the effect of….and I am totally paraphrasing poorly here: if we can’t seek pleasure legitimately, we will seek it illegitimately.
So thisstory from ABC newsabout a Newcastle addiction group support program showing some early signs of greater retention and engagement and therefore potential success with addicts…because they incorporate prizes…well that makes so much sense!
The article is important to read in its entirety as it creates the context – especially for many people suffering from addiction who tell tragic stories of lives where the only rewards/prizes and even gifts they’ve ever known, being drug-related – even from a young age. So to normalise reward to some extent, and give individuals an experience of constructive legitimate versions of this, is actually desperately needed and ground-breaking.
How can we incorporate some element of this in our interactions with these patients?
The second ABC news item touts ‘a new generation drug that restores balance to the brain’ but is actually just a teaser about…wait for it…cue stage right…a not so old favourite…N-acetyl cysteine! Although this is effectively a recruitment drive for methamphetamine addicted individuals into a new 12 week trial of NAC, run by the National Drug Research Institute, taking place in Melbourne, Geelong and Wollongong, it gives NAC a great wrap and rationale for being a good adjunct in addiction, of course. Just a reminder folks that naturopaths belong on that multi-modality health care team for people struggling with addiction, and we do have some potent therapies to contribute.
A couple of years back I was asked to deliver an educational session to a group of hospital based mental health specialists on the merits of NAC. My favourite question/comment at the end of my detailed presentation from a very experienced psychiatrist was, “Well if N-acetyl cysteine is so good for mental health…why haven’t I heard about it before now?!”
I hope they follow the ABC news 🙂
Want to Get Up Close to N-acetyl Cysteine in Mental Health? Previous ideas regarding the pathophysiology of mental illness have been profoundly challenged in recent times, particularly in light of the limited success of the pharmaceuticals that ‘should have worked better’ had our hypotheses been correct. Novel drivers such as oxidative stress, inflammation and mitochondrial dysfunction are on everyone’s lips and N-acetyl cysteine is in prime position in this new landscape, to be a novel and effective therapy for mental illness. This presentation brings you up to date with the current NAC research in a large number of mental health conditions & translates this into the clinical context.
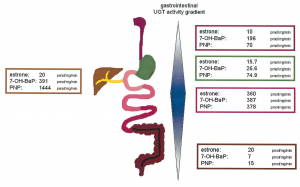
I’ve had my nose in all the research on Gilbert’s Syndrome again..watch this space…in the interim just thought I’d share this image and a couple of important details I may not have been able to convey when you last heard me talk (very fast!) about this important and common polymorphism:
While the incidence is approximately 10% of Caucasian population, rates are heavily influenced by ethnic background and the highest rates (up to 1/4) are seen in Middle Eastern populations
Gone are the days of thinking this condition only effects bilirubin levels and the enzyme responsible for its clearance – more recent research has shown over 3/4 of patients with Gilbert’s Syndrome have multiple SNPs that compromise clusters of enzymes within the glucuronidation pathway – with varying patterns – this goes a good chunk of the way to explaining the variability we see in bilirubin levels and symptom pictures across patients all deemed to have Gilbert’s Syndrome. This also explains why figures of reduced glucuronidation activity vary anywhere between 10% less to 90% less! It depends on your cluster..but the average reduction is around 50%
UGT enzymes, the ones affected in Gilbert’s, are also expressed all the way down the GIT and constitute important food and drug handling. These UGTs are most active in the small intestines,as you can see above, but may explain why Gilbert’s patients are ‘more sensitive’ to medications than just paracetamol!
And are you still thinking you need to run an $$$ gene test to confirm your Gilbert’s hunch in a client whose bilirubin sits consistently high normal or high? Think again… here’s a great little diagnostic short-cut that even theRoyal College of Pathologists Australasiacites as sufficient evidence to confirm the polymorphism:
In the face of elevated total bilirubin levels and in the absence of liver pathology or increased haemolysis to explain this..”If the diagnosis is uncertain the serum bilirubin fasting level can be measured and should exceed the non-fasting level by >50%.”
Nice. So that means you only need to demonstrate that the patient’s fasting total bilirubin levels go up by at least 50% compared with their fed levels and BINGO you have your diagnosis. Much easier. Oh and this image comes from an interesting paper from Tukey & Strassburg 2001 – but is probably not for the faint-hearted 😉
Stay tuned for more 🙂
Just new to this condition and need a soft place to land with understanding Gilbert’s Syndrome? This previous UU30 is just the thing! Affectionately called Gilbert’s Girls because in particular it details a set of twins with this condition, this short audio explains the basics about this common polymorphism and why we tend to see a lot of patients who have this…even if no one has pointed it out to them yet! You could be the first to provide them with this important understanding about how genetics is impacting their detox pathways, changing their sex hormone handling and perhaps setting them up for both mental health issues and some serious upset guts! Better still, what to do once we have that diagnosis.
Sometimes we wonder who put the invisible sign up out the front of our practice, right? The one that says…absolutely everyone with Condition ‘Z’ come and see me, now! I’m sure you know what I’m describing. Well this week I have hit the trifecta, performed a neat little hat-trick and diagnosed 3 patients with Gilbert’s Syndrome who all present in their own individual way but actually each one also with quite a textbook Gilbert’s picture, it almost beggars belief. Have a little look
70yo Female says: Since childhood she has felt like she has had a rock in her stomach after she eats. This ‘rock’ is there for hours. Her stools are never the same in spite of a regular diet and she has always been uptight and anxious. All her bilirubin results are in the 20s & she reports she’s ‘always’ had high values
55yo Male with severe ‘constitutional anxiety’ and surprisingly high oestrogen and a worrisome profile of oestrogen metabolites. His bilirubin is in the 20s
30yo something Female presents with unexplained severe unwellness for 20yrs that mostly involves nausea, bloating, a functional gut disorder without a real diagnosis, anxiety, depression and poor stress tolerance. Her bilirubin fluctuates between 30 to high 40s.(more…)
Recognise your own name or someone else’s on this list?
Dear 2017 Group Minties aka Mentees. I have always struggled with the term, ‘mentees’…seems too American or something and this morning when I was out walking, I had a light-bulb moment – I am proposing a re-branding to something much closer to home (!)… I propose we rename you Minties!! Because you are always fresh and you give me & your fellow Minties always something; cases, questions, clinical conundrums, ethical dilemmas, every month to seriously get our teeth stuck into! Cheesy but true 😉
Congratulations on completing your full year of group mentoring – and if this is your 2nd, your 3rd even your 4th year then I bow to you even more deeply.
Thank you for including me on your support team and entrusting me with helping you grow & develop as exceptional practitioners.
You should be celebrated for your commitment to your own learning & your endeavour to always improve your knowledge and skills.(more…)
Are you hearing me? Yup, it’s been a BIG year..and to think I don’t even have the ANS technically to blame this year!! How about you?
But listening to myself say this to people, in my wrap-up of the year-that-just-was, I am thinking….Has anyone EVER got to the end of year and exclaimed, “Wow! That was a small one?!”
Not me, not ever, well not in my living memory! But somehow I forget. I get to December and I think, ‘Geez, I’ve never felt this spent before! I need to go on holidays and never come back, retire from work and retreat from the world’, until someone who loves me, and who has a longer memory than a goldfish says, ‘Love, you always feel just like this.’ The upside to this annual amnesia is, it pushes me to make very conscious choices for my holidays.(more…)
Standing at the podium, I looked down at my notes & slowly read out the title of my presentation to the hundreds of people attending, ‘Paediatric Digestive Issues & Neurocognitive Abnormalities’ and briefly froze thinking, Holy Heck (!) this is someone else’s presentation! Seriously. No, this is not one of my work stress dreams. This happened. I thought…oh my how am I going to deliver this, it sounds very complex and lofty and scary!!
Then I saw my scribbled hand notes on the page, the unofficial name I had affectionately given this presentation as I researched, compiled my case studies and brought it into being, months prior and I instantly relaxed…oh…Kids’ Guts Are Mental…now that I have some serious experience with and something to say about!(more…)
May was the month of teenage girls presenting with severe digestive problems, especially ‘food intolerances’, leading to avoidance of specific foods and at times significantly reduced food intake overall. As integrative health practitioners, validating and creating insight for clients on the nature and source of their food reactions is our bread and butter, right? Is it wheat? Dairy? Gluten? FODMAPs? Salicylates? Oxalates? We are not surprised by how many ‘sick’ patients we see in spite of a theoretically ‘healthy diet’ – healthy for others perhaps but not for the individual in front of you, right? But what if I told you that each of these teenage girls had a BMI < 18 kg/m2, does that change your opinion about your role? Would you assess, monitor and manage these teenage girls differently? You should.
Take the example of one of my clients: 14yo female with a BMI 16.3, who had her first confirmed food reaction under 2yo with failure to thrive, which was attributed by a paediatrician & dietitian at the time to severe salicylate sensitivity. She underwent jejunal biopsy at 3yo for suspected coeliac disease, due to ongoing concerns and a primary relative with CD but it was NAD. In the 11 years since, there have been a couple of other digestive diagnoses based on solid evidence, such as mainstream stool PCR testing. So surely, the fact that she is underweight & that she skips lunch at school due to digestive discomfort is proportionate and explained by her organic digestive issues. Or is it?(more…)
This year has been a steep learning curve but this is exactly as I had hoped and planned for. I strapped myself in for my roller-coaster ride, a series of intensive upskilling initiatives undertaken with mentors and experts in specialist areas, and I haven’t hurled yet or screamed loud enough to make the operator stop the ride (seriously this happened to me in about 1997 on a Pirate Ship in Rosebud!)…but I have come close 😉
One of the really big lessons has come from getting more into the science behind pyrroluria and urinary pyrrole testing again. What motivated me to tackle this spikey beast? Well, like many people who have been introduced to the concept of pyrrole testing and pyrrole driven mental health presentations – I had a lot of questions that hadn’t been adequately answered. Those gaps left me with some uncertainty about the validity of this investigation and about the interpretation of the results. I also have introduced this pyrrole theory to many naturopaths and hence feel a responsibility to polish up my knowledge on this and set the record straight.
Last but not least, in our local area we reputedly have a ‘pyrroluria plague’ at play – every man woman and their dog is getting this diagnosis and it had added not only to my misgivings about testing but also my concern about misdirected & unsafe treatment.(more…)
Duck duck GOOSE!Do you know this game? That’s how I’m feeling with oestrogen – high-high-high-LOW!-of late. Likely similar to your experience, the majority of my female clients battle with oestrogen dominance, therefore I get so used to looking for it, expecting it: the high Cu, the profoundly elevated SHBG, maybe a raised ESR. So much so that sometimes the low ones can catch you out, especially of course when it happens in women way way before menopause.
We’re so resolved to hear bad press about oestrogen and to be armed ready to saturate our patients with broccoli extracts of the highest order – do we remember the clinical features and markers of an oestrogen deficit and know what to do with those women who simply don’t have enough?(more…)
Want to start 2017 with some good news? Sometimes working with patients challenged by mental health I get scared. A well-known colleague of mine introduced me to the notion of the ‘clinician in crisis’. The practitioner who, in the face of their patient’s extraordinary pain & distress feels overcome by the need to Do Something…Anything. Over time I have learned to spot, what we call a ‘desperation prescription’, the patient who is on 3+ psych medications all from different drug classes and still remains tragically symptomatic. It is potentially frightening stuff. I’ve had the same experience with patients using herbs and nutrients. The patient’s biological drivers may seem straight forward on paper, but they fail to respond as predicted. Nobody has a 100% success rate…not me, not Ben Lynch, not Kelly Brogan…as much as their marketing machines might make you think otherwise.(more…)