What’s the most common thyroid disease you’re seeing in practice? Nope, try again. I’m serious. There would be very few of us who’d get this right without cheating. It’s nodules. Current figures suggest 1/2 of all us middle-agers have them and by the time we’re 80 that’s risen to 90%! There’s a school of thought that says these figures have jumped purely because of increased rates of thyroid imaging and we should stop sticking our nose in places it doesn’t belong. Just because they are there doesn’t mean we need to know about them or that they are causing trouble. All this is true and yet there is a percentage of patients for whom these nodules are a whole lot of trouble, in fact, that’s why they’re coming to see you…they (& possibly you!) just don’t know it yet.
Nodules, outside of radiation exposure, have always been primarily viewed as a nutritional deficiency disease: Iodine. While this was always a bit one-dimensional (poor selenium…when will you ever get your due?) it’s an explanation that no longer fits as well as it once did because even in populations who have addressed iodine deficiency, the incidence of nodules continues to rise.
So, what now?
New nutritional drivers have been identified but rather than being about our deficiencies they speak to our nutritional excesses. And while iodine is not totally out of a job here, some people of course are still experiencing long-term suboptimal iodine which can trigger nodule development, we now need to question if there is any therapeutic role for iodine once the nodules are established. Well the answer is both ‘yes, maybe’ and ‘absolutely not’. The determinant being whether we’re dealing with Hot or Cold. Unfortunately most patients and therefore their practitioners can’t tell the difference. But it is the presence or absence of a hot nodule that radically changes what complementary medicines you can and can’t use and what an effective treatment plan looks like.
I’ve seen a lot of thyroid nodule cases pop up in mentoring this year and it’s been a great learning opportunity for everyone to get comfortable with clues in both patients’ presentation & their pathology. While iodine deficiency no longer ‘fits’ like it did, nutritional medicine should arguably remain the primary approach to their management and the new research gives even more credence to this and identifies a far greater range of dietary and supplemental tools.
Thyroid nodules are going to explain a surprising number of our subclinical (hypo and hyper) thyroid patients and we already have a dispensary full of powerful interventions but we need to start by familiarising ourselves with their story: their why (they happen), their what (this means for patients) and their how (on earth are we going to address these effectively) Knowing your Hot from your Cold…is step one.
An increasing number of our patients have thyroid concerns but unbeknown to many of us the most likely explanation of all is thyroid nodules, whose incidence is on the rise globally.The development of nodules has always been primarily viewed as a nutritional disease. Traditionally attributed to chronic iodine deficiency but recently novel nutritional causes have emerged . Benign nodules come in 2 flavours: hot and cold and while patients can present with a mixture, it is the presence or absence of a hot nodule that radically changes what complementary medicines you can and can’t use and what an effective treatment plan looks like. The pointers, as is often the case, are there for us in the patient’s presentation and pathology, so knowing the difference is no longer a guessing game. This UU30 comes with a great visual clinical resource and includes key papers on the nutritional management of nodules.
You can purchase Are You Running Hot and Cold on Thyroid Nodules here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
*****Your RAN Online Account has a NEW LOOK!!*****
Next time your log in, you will experience a more user friendly way to search, view, listen and download your resources. Find out what’s new here.
How might your patients’ Nickel exposure wreak havoc with their health? What might that look like? It may be lurking behind labels like IBS, non-coeliac gluten sensitivity, contact dermatitis of unknown origin,(with or without alopecia) or even CFS. “Then how does Nickel, which can’t even claim fame as a heavy metal, manage such diverse detrimental effects’? I hear you ask. In 3 easy steps 1) exposure…we’re all exposed, Ni is ubiquitous in our soil, our food, our environment so don’t bother trying to run from it 2) it hits our gut where our microbiome and intestinal lining may constitute the first fallen soldiers 3) exposure to our immune system can lead to sensitisation, and the subsequent development of a hypersensitivity response to each following exposure …and at worst precipitation of an autoimmune process. You got all that?
So therein lies the big question: how can we help patients whose health problems stem from Noxious Nickel? We could run and hide…from our jewellery, our mobile phones, dental interventions, most food (!), but we’d be wasting our time…we’re surrounded!
As always, we go back to the science and we find others have done the work for us. Not google though. Google ‘low nickel diet’ and like ‘low oxalate diet’, you’re likely to get a whole heap of hogwash! How reassuring then that there is a validated dietary scoring tool to assist patients lower their dietary Nickel and that numerous other studies can show us the way in terms of use of mineral balancing strategies, probiotics etc. These resources plus more are all included in the latest Update in Under 30: Noxious Nickel part 2 as well as a discussion of what assessments we have available to confirm nickel as the culprit. But here’s something for free: hair nickel concentration (HTMA) is not by any means diagnostic in these cases, because it’s not necessarily about an issue of overall higher exposure it’s about an aberrant immune response to Nickel at any level. Just saying. You know me….not scared of controversy in the pursuit of improved patient outcomes. Ok a bit scared… 😁
In this instalment it’s time to get down and dirty and detailed about how to best identify those patients who may have Nickel related pathology and presentations. We cover testing options, typical systems affected from GIT to autoimmunity and the most extreme form: Systemic Nickel Allergy Syndrome. We outline Nickel management strategies in a world full of it (!) and we include several key papers for additional resources and support. How noxious is Nickel for some of your patients? Well by the end of this you’ll know and better still, know what to do once that’s established.
Hear all about it by listening to my latest Update in Under 30:
For all Update in Under 30 Subscribers, it’s now available in your online account and if you are not a subscriber you can purchase this individually here.
Ok here’s some tough Tuesday talk..not all tests are valid. Tougher still…not all of the mainstream nor the functional pathology ones. I am talking across the board here. Each and every pathology parameter requires good knowledge about its strengths. limitations and, one of my absolute favourite nemeses, confounders. “How on earth am I supposed to learn all that and everything else I have to know too?!!” I hear you scream at your screen. Btw keep yourself nice if you’re in public while you’re reading this 😉
But rather than imagining you need to have this level of knowledge for all tests, I would suggest you set yourself a hit list of the ones you rely on most, either in terms of frequency or in terms of the degree to which they direct your decisions about patient care…can I mention (ahem) Iron studies here perhaps for us all…but maybe you have a specialist area so you use a particular investigation routinely or at least frequently…
CDSAs? Breath tests for SIBO? Oxalates?
May I please then politely suggest that you get to know these inside and out? Not based purely on the information and assistance that the test provider provides you..but you scrutinise them independently. Top to bottom. Because that’s your business, right? And your diagnoses and treatment decisions are pivoting on these results. Jason Hawrelak gave us all some great examples, including his informal experiment of sending the same stool sample to multiple labs. Don’t know about this and his findings?? If you’re in the business of ordering stool tests, you need to. I am doing this all the time with numerous pathology markers because diagnostics is my passion (alright, obsession)…and recently I put Oxalate Assessment to the test and oh boy!
Here’s something for free:
If you are measuring urinary oxalates to diagnose oxalate overload in your patients and you, 1) are using a lab that does not preserve the urine as you collect it, using acidified containers or providing additional preservatives for take home testing kits….you are wasting your patients money and you are likely getting a lot of false positives, i.e. the result infers the patient has a problem when they don’t!!
And 2) if you are simply following the labs reference ranges for what ‘healthy’ urinary oxalates look like – you’re wasting your patients money again and likely getting false negatives – a failure to show a problem that is actually there! If you’re hunting oxalates…please ensure you have a current effective hunter’s licence…by getting up to speed fast regarding accurate investigation of this. Oh yes…it’s tough-talkin’-Tuesday and I’ve come out firing…watch out this may become a regular feature 🤷♀️
Update in Under 30: Oxalate Overload – Assessment and Management
Oxalates are present in many healthy foods and in all healthy people, but when ‘normal’ levels are exceeded they can spell trouble in a whole raft of different ways due to their extensive distribution across the body. Some tissues, however, have more problems than others, especially the urinary system and soft tissue and joints but now there are also questions about oxalates’ relationship with thyroid and breast issues. We review the latest evidence about the health consequences, blow the lid on accurate assessment for oxalate excess and talk management in this jam-packed update.
Show me a nutrient that doesn’t demonstrate a U shaped curve with our health (too little produces negative effects – too much produces negative effects) and I’ll go ‘HE!’ Go on…try it now… But the way many have been taught nutrition has lead to some erroneous thinking, it would seem, about the inherent ‘safety’ of all micronutrient prescriptions. To know these vitamins and minerals well is to respect their potency in every sense – from their incredibly positive application at both physiological doses, correcting deficiencies, and in a small number of scenarios almost pharmacological benefits, when used at doses that are intended to exceed the natural physiological state (think IV vitamin C, or high dose B3 for lipid-lowering as two famous examples), to their potential for fallout when healthy levels are unwittingly exceeded, especially long-term.
Our risks of over-supplying individual micronutrients have arguably been amplified by the industry’s increasing promotion of nutritional formulas or complexes over the use of single nutrients. How often do you go through and studiously add up all your cumulative totals for individual nutrients for each prescription?
Especially those that tend to find their way into such a large number of formulas and have clear upper limits, such as Vitamin B6, Folate, Selenium and Manganese…to name a few of my (not so) favourites.
Many of you will know I am a fan of staying single 😉 I mean using single nutrients rather than all the ‘bells-&-whistles-formulas’ we’ve come to rely on so heavily. This is one key reason. But the other is that many of these formulas are someone else’s, perhaps a whole tech team’s, idea of what a ‘generic’ low thyroid patient, or an ‘average’ immune challenged patient needs. Not sure about you, but I don’t subscribe to ‘average’ and ‘generic’ when it comes to nutrition…that’s one of naturopathic nutrition’s key criticisms of conventional dietetics, right? So where does this reliance on generic nutritional complexes comes from? Is it purely convenience -yours and the patients?
Or are we insecure in our confidence in creating our own crafted formulas? Is it a need to know our tools of trade better..because if we did, might we better realise the power and potency (positive or negative) of our own prescriptions? Especially in the realm of accurate assessment and individualised requirements.
The latter is my call to action on this, predictably! 😉
I am often asked about where my ‘nutritional nous’ comes from. Which magic journals do I subscribe to that fill my head so full? What non-existent-far-superior-course did I undertake? The answer I give is the same every time. I had one solid nutrition teacher in my under-graduate across my 4 years of naturopathic nutrition at SSNT. What made her so good and why has so much she taught stayed with me? She simply taught me every single nutrient literally from the ground (soil) all the way up (human nutritional physiology) and everything in between. Once you know each nutrient that well and the big concepts that are a truism in nutritional science…you can never go back and you will practice nutritional medicine at its best. My wishful thinking? I wish that for us all 😉
Let’s make sense of the over-arching nutrition principles, that will profoundly change your understanding and application of this modality Truly understanding the ‘big’ concepts, so often overlooked, or incorrectly taught, ensures you get the critical ‘small’ detail in your nutritional prescriptions right. In this 4 hour recording, together with key clinical tools, we talk about the tough stuff: dose-response curves, active versus passive stores and excretory pathways and ooh lah lah…the myth of taking ‘activated vitamins’. Even those who feel satisfied with their original training – will find a lot in this critical review that is new, insightful and truly practise-changing!
Black Tea & Green Tea & All My Dark Chocolate Sins
These are a few of my favourite things!!
Sounds like a kitchen roll-call at my house…how about yours? And your patients?!! You see I’ve been working away researching Oxaluria – a condition whereby individuals end up with too many oxalates in their body and ultimately their urine – which can be a problem in a proportion of people suffering with kidney stones, vulvodynia, joint pain etc and anyone with CKD and on my travels I came across this article on how the regular intake of green smoothies could in fact turn someone with normal oxlate levels and handling, into someone who has an acute induced Oxaluria. Yup.
Nobody panic. Remember this is not going to be problematic in all patients but just might be in some. But it left me wondering if we ‘clean-diet-prescribing-practitioners’ know all we really need to about, who not to prescribe green drinks to (or beetroot juice for that matter) and cap ‘ye olde’ dark chocolate quota for!
Or…keep them eating all these fabulous generally healthy foods but mitigate any elevated oxalate risk through correct food preparation & combinations?
There’s so much more to this topic than meets the eye. Because on top of what you eat, there’s the huge variability in terms of what you absorb…think it’s as simple as, whether someone has Oxalobacter in their bowel or not? Nope. Oh…and then there’s the 3rd element: how much you make yourselves…that’s where we need to have a serious chat about collagen, high dose turmeric & vitamin C supplements in susceptible individuals, people. Want to read more yourself? Here’s somewhere to start on the giant pile of papers here.
Oxalates are found in high concentrations in many of the ‘healthy food choices’ we promote and are even higher again, when these are organically farmed! Given the importance of individualising therapeutic diets are we able to quickly recognise those who need to lower their low of these naturally occurring plant products? Who shouldn’t be drinking green juices? And which of our patients might benefit from being educated about different food combinations and preparation to lower the oxalate load from these otherwise fabulous foods?
Hear all about it by listening to my latest Update in Under 30:
For all Update in Under 30 Subscribers, it’s now available in your online account and if you are not a subscriber you can purchase this individually here.
Integrative Psychiatry is an inspiring area to work in & its evidence base, acceptance and recognition of potency is rapidly growing & offering more patients, more. Going beyond the ‘neurotransmitter imbalance model’ for each presenting diagnosis helps us to see the unique mix of biological & psychological drivers in each individual who presents seeking our help. However sometimes I believe, we find ourselves falling into looking through the lens of just another short-list of alternate models:What kind of methylation imbalance does this person have? What sort of Zn, Cu issues?
While I am so grateful for having learned these tools and watched them be very successful in a portion of my mental health clients, they are simply not the answer for everyone. We need to keep our thinking and practices dynamic and up to date, to reflect the incredible increase in research in new areas of integrative psychiatry, such that more of our patients can benefit and that we can continue to think beyond the box…even if that box itself was originally so progressive!
What do you know, for example, about abnormal purine metabolism in mania and using serum urate as a BPAD prognostic marker in depressed patients? Think you can simply be guided by the reference range provided, think again. What could good old LFTs reveal about our patient’s mental health vulnerabilities and what have we potentially misunderstood about copper in this area, particularly in children?
I appreciate Zinc’s role in mental health as much as the next integrative practitioner. Okay, given my 20K word thesis manifesto, more. But increasingly I am seeing mental health patients who need treatment with different tools. This upcoming ACNEM Mental Health Module in Perth is on point: thinking outside of, outside the box!
While the above only speaks to what I’m presenting, I know Dr. Sanjeev Sharma will also be sharing his wealth of individualised management insights and he’s a big fan of addressing Chronic MIld Metabolic Acidosis as an early treatment objective. Maybe we all need to hear why? And I am so looking forward to getting a PTSD update from Christabelle and hear all about the research into therapeutic keto-diets in psychiatry from Cliff Harvey…haven’t read all those papers to know which conditions and when this approach shows merit? No, most of us haven’t. That’s the point of outsourcing our up-skilling to colleagues who we know are across these more than us and to boot have the clinical experience to ‘make real the research’. As I’ve said before, given the content of this upcoming ACNEM Mental Health program, I wish I wasn’t presenting really, so I could just kick back and take it all in, uninterrupted. But alas, I have some important new information on reading basic bloods through a mental health lens to share! I really hope to see you all there. Let’s get out of the rut of 3-4 nutritional approaches to mental health and make the most of the explosion of research and shared clinical experience.
ACNEM Face-to-Face Training Fremantle, 27-28 July 2019 at the Esplanade Hotel Fremantle by Rydges https://www.acnem.org/events/training
Oh and while you’re here…did you know the research into both beta-casomorphins and IgG casein reactions in relation to certain mental health diagnoses has taken some giant steps forward in the last couple of years? You should. Milk Madness is back and it’s via two distinct mechanisms – identifying which might be at play in your patients & correct management is now clearer than before. Want to get up to date in this area of mental health – check out our UU30 recordings: Milk Madness part 1 & part 2
No you’re right, it’s not long enough to be a Hemsworth’s mobile number but actually it’s more sought after 😉 If you’re up to date with reading & recognising all the different patterns of Iron Studies & the stories they tell, which is a daily business for most of us, then you will know by heart the striking pattern we call, ‘Pseudo Iron Deficiency’. You know the one where your patient’s serum iron & transferrin saturation are mischievously trying to trick you into thinking you need to give this patient iron…when in fact this is absolutely not what they need!
This is of course the result of the redistribution of iron during inflammation – iron is actively removed from the blood and sequestered in the liver instead. It’s designed to protect us from bacterial bogeymen, which is how our stone-age bodies interpret all inflammation of course.
Doesn’t sound familiar? Ok you need to start here or even embrace a full overhaul of all things iron here.
But for those of you nodding so hard you’re at risk of doing yourself an injury, this number is for you. We’ve often talked about the redistributional increase in patients’ ferritin levels in non-specific terms: it goes up..but by how much? Of course we would like to know because no one is fooling us with this transiently inflated value…but can we make an estimation as to what this person’s ferritin will drop to once this inflammation is resolved? Yes.
X 0.67
Write it down. Consider a tattoo, perhaps?
This glorious magic number comes from Thurnham et al paper in 2010 who did the number crunching on over 30 studies involving almost 9,000 individuals to determine the mathematical relationship between inflammatory states & markers and the reciprocal increases in ferritin. Their work is exceptional in that it also differentiates between incubation (pre-symptoms), early and late coalescence periods (if you want to differentiate your patients in this way and get even more specific then you need to read the paper), however, overall when we see a patient who has a CRP ≥5 mg /dL , we can multiply their ferritin by 0.67 and get a lot closer to the truth of their iron stores. Oh and another important detail they revealed, this magnitude of ferritin increase is more likely seen in women or those with baseline (non-inflamed) values < 100 ug/L..so generally more applicable to women than men. Thanks Thurnham and colleagues and the lovely Cheryl, my previous intern who brought this paper to my attention…you just took the guessing out of this extremely common clinical scenario 🙂
We’re not deaf…we heard that stampede of Iron-Inundated Practitioners!The Iron Packageis for you!
Our recordings and clinical resources for improving your skill-set in all things iron including, your accuracy of diagnosing deficiencies, pseudo-deficiencies & excesses, plus radically rethinking the best treatment approaches for each scenario…have been some of our most popular. Because nailing iron (pardon the pun) is harder than we were all lead to believe and at least 1 ‘iron maiden’ or ‘iron man’ walks into our practice every day, right? So we’ve brought together 5 extremely popular UU30’s on Iron into one bundle for the price of 4! So if you’re more than ready to graduate from ‘iron school’, now’s your best chance!
Those ‘still-believers’ look away now. One of the great myths, misconceptions and misunderstandings in nutritional medicine is that supplementation with specific nutrients will produce change specifically in one system, or pathway, which just happens to be the one that the practitioner has determined would benefit most/is targeting. Let me explain myself a bit better. When we give patients any nutrient, in the cases where it’s not simply to correct a global deficiency & therefore improve levels all round, it’s typically on the basis of a specific desirable therapeutic benefit, e.g. some magnesium to help their GABA production…, additional B3 would improve their mitochondria. Beautiful on paper…but like sending a letter to Santa in reality (I did warn you!)
Truth Bomb No.1: There are nutrient distribution pecking orders that have nothing to do with who you ‘addressed’ it to
This dictates that when something is given orally, for most nutrients, the gut itself has first dibs. So the cells of your digestive tract meet their needs before any other part of your body gets a look in. Sometimes the digestive system’s needs can be quite substantial and leave little for any other part of the body…not mentioning any names (ahem) Glutamine!
Truth Bomb No.2: En route to the ‘target’, these nutrients get delivered and distributed to many other tissues – with possibly not so desirable or intended effects!
You may determine that a patient needs iron because their ferritin hasn’t got a pulse…so you keep giving them daily high dose oral iron to ‘fix’ this…not realising you’re making their GIT dysbiosis and gut inflammation worse in the process. Or you feel their mysterious ‘methylation cycle’, happening predominantly in the liver and kidneys, could do with a folate delivery…perhaps ignoring the very worrying fact that their colon may have already had a ‘gut full’. Literally. Hence the concerns and caution against supplementing with folate in patients with established colorectal cancer. So is bypassing the gut via IM or IV nutrients the answer…well yes and no…but mostly no. Read on…
Truth Bomb No.3: Those pathways that use the nutrient you’re supplementing, that are most active in the patient’s body currently – which is determined by many factors (genes, physiology, feedback circuits, pathophysiology) and rarely simply by the availability of nutrients – will take take the next lion’s share of that nutrient
Wanting to nutritionally support someone’s thyroid, you know tyrosine is the backbone of the thyroid hormones, so you include this in the hypothyroid prescription. Will it help? Who knows? Being a non-essential amino acid the body exhibits very complex regulation of its distribution and use – with thyroid precursor availability being only one job on a very long list! And if this was in a patient who is regularly smoking cannabis, due to upregulation of the tyrosine hydroxylase enzyme – there is likely to be more of the supplement headed for even more dopamine production and very little or none reaching in fact your intended target. And don’t get me (re)started on Glutamine – supplements of which in an anxious and glutamate dominated patient will make…G.L.U.T.A.M.A.T.E…right…not GABA! 🙁
Sorry, I know, it hurts right? But these are essential teachings, that tend to have been over-looked or under-played I find, in nutrition education, regardless of training: nutritionists, naturopaths, IM doctors, dual qualification practitioners remedial therapists. Nutritional medicine is a wonderful and potent modality when it’s done well…but we need to revisit some core truths and principles that many of us have missed out on, to ensure we’re not writing letters to Santa.
Let’s start with Micronutrients. Let’s talk make sense of the over-arching nutrition principles, that will profoundly change your understanding and application of this modality Truly understanding the ‘big’ concepts, so often overlooked, or incorrectly taught, ensures you get the critical ‘small’ detail in your nutritional prescriptions right. In this 4 hour recording, together with key clinical tools, we talk about the tough stuff: dose-response curves, active versus passive stores and excretory pathways and ooh lah lah…the myth of taking ‘activated vitamins’. Even those who felt well trained – will find a lot in this critical review that is new, insightful and truly practise-changing!
What makes integrative health professionals stand out is that we take the time and have the attention to detail to capture the ‘whole health story’ of each patient. As a result, however, we tend to end up with vast amounts of information for every client: detailed medical histories, broad systems-reviews, condition specific validated screening surveys, in-house physical assessment data, not to mention a pile of past pathology results…and that’s before we start our own investigative path!
So as you sit at your desk with a plethora of information in front of you, you’re probably thinking, ‘Great, so much valuable information – Oh dear…so much valuable information!’ and struggling to separate the critical narrative from the noise.
Plagued by circular questions: ‘Where do I start?’, ‘What needs to come first?’, ‘Which treatment objectives will pack the most punch for this patient right now?’, ‘What really requires further investigation and what can wait?’ … your thoughts jump around, from one shiny thing to the next…you can ‘see’ so many of the connections… but can you see them all, the whole interconnectedness, and therefore the prescription, laid out in front of you like a road map to follow?
Introducing the two essential tools (aka secret weapons)…
MindMapping & Timelines
… the actual practice of gathering vast amount of a patients case onto one piece of paper.
Yes, that’s what I said ONE PIECE of paper!
Sounds too good to be true?? Well, they don’t quite give you super powers but they will help you write the patient prescription for you and not just one prescription but typically, for the next 12 months. These tools can turn good clinicians into great ones and, once you master them, save enormous amount of your time on your patient work-ups. Relevant to all health professionals who use an integrated approach, the utilisation of these tools, will also reveal to you much about what you know, but didn’t immediately realise (e.g. the means by which gut dysbiosis contributes to impaired oestrogen detoxification), and just as importantly, highlight your knowledge gaps & therefore opportunities for further growth along the way (e.g. how do inflamed joints disrupt GIT tight junctions?).
As ‘whole picture people’ we bite off a lot! It’s these systems, timelines and MindMapping, that Rachel has found help her, and so many other clinicians, truly ‘digest’ the case, optimising our understanding and management.
“I loved this session and think it’s very relevant. I have used these tools before, but never mastered them or used them regularly. I have mostly used mind maps for study, so I love this application and with practice, think I will get used to using them for every case.”
“AMAZING!!! Fantastic health links that I did not know and really consolidated my knowledge on how to produce a Mindmap and how to be better at it! Fabulous session. Thank you”
“Most difficult is challenging existing patterns of thinking around mindmaps and training my brain to approach it more effectively (plus getting faster). This will come with practice. Most satisfying is seeing how useful they can be when done well at the start in terms of time saving in the overall case (across years) and getting to the core (s) of the case. Great session!”
In the Part 1 Video, Rachel teaches you how to effectively perform a case work-up that does justice to the holistic framework and model. At the end of this presentation there is a practice run for you to create a MindMap and Timeline. PDF sample case notes, MindMap and timelines are included.
In the Part 2 Video, Rachel demonstrates in detail how to put a MindMap together from case notes. You’ll be able to see ‘in action’ how to apply all the information from Video 1 and have all your questions answered. PDF’s of both slideshows are included.
Remember biochemical individuality folks? That great core underpinning principle of naturopathic & integrative nutrition. We should always keep this in front of mind, when something utterly fabulous for absolutely everyone pops its head up. Like every month or so, in the area of health, correct?
Fasting, in all its forms, is having a lot of time centre-stage right now. What a novel & truly prehistoric notion in this era of food 24/7! I get it and I agree, most of us would do much better by regularly moving out of the top paddock.
BUT…and there has to be a but…or we are no longer treating the individual…
Some of whom, due to specific conditions or biochemical tendencies, do utterly horribly with any sort of prolonged periods between feeds. I already have a hit-list of conditions where fasting and food restriction is a no-no…then I saw a set of labs the other day from a patient who self-initiates regular, 4-6 day fasts during one of said fasts,whose alarming results jumped out in bold, italicized CAPITALS, illuminated itself in neon pink and reminded me to remind you! This patient’s (extended) fasting labs went a little like this… total bilirubin 48 (normally 15 umol/L), bicarbonate 18 (normally 26 mmol/L), corresponding anion gap 20 (normally 12), uric acid 0.62 (normally 0.4 mmol/L). Are you thinking what I am thinking B1?
So here’s my hit-list of ‘fasting = foe’ for – still subject to case by case assessment (of course!! because we treat the individual, right?!)…but
Any individual with a history of, or currently risk factors for, disordered eating, e.g. orthorexia, bulimia, binge eating disorder, anorexia
Gilbert’s Syndrome
Low T3 – thyroid ‘hibernation’
Hypocortisolemia
Anxiety and PTSD
Drug addiction
Children, pregnant women, the elderly…of course!
In short: any patient whose condition or biochemistry may be too negatively impacted even in the short term by any of the following: higher cortisol release, significant slowing of phase II detoxification, or radically elevated acidosis, should step away from the fast and towards the fridge! 🙂 🙂
Thyroid hibernation produces a low T3 value coupled with a ‘lowish’ TSH and typically a clinical picture of hypothyroidism. As the practitioner we are faced with the conundrum of how to effectively ‘wake up’ the pituitary which appears to be sleeping on the job. This audio connects up the dots between this type of thyroid dysfunction, dietary patterns, restrictive eating (including a history of eating disorders), carbohydrate intake and disturbed iodine nutrition of the thyroid gland. This pattern is increasingly seen in practice and this audio is a must for anyone working in the area.
Do you know that saying, ‘mind your Ps and Qs?’ It basically means mind your manners and I heard that a lot as a kid 😉 But what we really need to hear now, as practitioners and promoters of healthy eating and wellness is really, Mind your P’s and P’s because a lot of biggest health consequences of any diet are determined by the balance or imbalance of two major players; protein and potassium. We’re always looking for simpler ways to enable patients and ourselves to be able to both recognise the strengths and weaknesses of their diets and, better still, apply a simple method to making better choices moving forward. Eyeballing the protein and potassium rich sources in any diet speaks volumes about other essential dietary characteristics and the likely impact of diet on health – and getting the relationship between these two right should be a goal for us all.
“World Health Organization (WHO) Dietary Targets for Sodium and Potassium are Unrealistic”, reads the recent headline from yet another study finding that humans would rather challenge the solid science of human potassium requirements than acknowledge the urgent need to turn this ship of fools around!
This large study, conducted over 18 countries, involving over 100 thousand individuals, reported that 0.002% met these targets. That’s 1 person in 50,000. Now, the researchers’ response to this is that we should lower our dietary potassium expectations….such that the targets are more achievable and so that (frankly) we are less perpetually disappointed in ourselves and our terrible food choices. Wha????Back up there. The WHO guidelines, just like any other nutrition authority, derived these minimum amounts from a thorough review of the science that speaks to our physiological requirements and the level of nutrients that have been shown to be associated with health. Australia’s own fairly conservative NHMRC suggests even higher amounts for good health! Perhaps rather than revise the established dietary targets we should revise what we’re putting in our mouth!
So where does protein come into this? Well one of the most important and central nutrient dynamics is the balance or imbalance of our intake of both. And in this regard, yet again, we have a surprising lot in common with plants! Whether you’re trying to understand optimal nutrition conditions for growth (nitrogen alone won’t get a plant there, nor protein alone in a human) or the intricacies and nuances of finely tuning our physiological processes such as cardiovascular function, renal health, blood glucose management etc. the answer lies in a happy marriage between these two.
In this area of nutrition, we should be listening most closely in fact to renal specialists/researchers. These ‘undercover’ protein and potassium experts have been talking about this for a long time and in particular, in my humble opinion, Lynda Frassetto has lead that charge for decades. If you haven’t read much on this issue and want somewhere to start at least, jump into her pivotal paper from 2001 which eloquently explains why the human design can not shoulder a potassium shortfall…well not without causing real health problems…like the ones we’re seeing in record numbers currently and why the protein potassium balance of any diet is a major health determinant. That’s why giving ourselves and our patients the knowledge and the tools (yes lovely shiny meaningful infographics included!!), to quickly determine their protein potassium balance, are so necessary and important.
Thanks to Frassetto and many other researchers’ work, looking at food through this protein potassium lens has sharpened my focus and I think it’s about time we all took a good look 🙂
Check out the latest UU30 to hear the latest information…
The health consequences of any diet are largely determined by the balance or imbalance of two major players & proxy markers; protein and potassium. When it comes to this area of nutrition, we should be listening more closely to renal specialists whose research shows why the human design cannot support a potassium shortfall and the health consequences of this. Whether you’re trying to understand optimal nutrition conditions for growth (nitrogen alone won’t get a plant there, nor protein alone in a human) or the intricacies and nuances of finely tuning our physiological processes such as cardiovascular function, renal health, blood glucose management etc. the answer lies in a truly happy marriage between our intake of these two. These recording comes with a clinical resource tool to help you quickly identify the dietary protein:potassium balance for your clients.
Hear all about it by listening to my latest Update in Under 30: Mind Your P’s and P’s For all Update in Under 30 Subscribers, it’s now available in your online account and if you are not a subscriber you can purchase this individually here.
When I was studying my under-graduate I imagined my clinic was going to be full of them: well patients wanting to maintain or even improve upon their wellness. Turns out…not so much…all the really really sick people have taken their spots and the former has been listed as an endangered species. But I do catch glimpses of them, as I am sure we all do, in their natural habitat, with over-flowing baskets at the organic grocery store or farmer’s market, routinely up the front of the pilates class and also sometimes in our clinics. So now that naturopathy, by consumer demand, not practitioner intent, has transitioned so much into the ‘unwellness space’, do we know anymore what to do with the well ones??
I heard some great talks at the NHAA conference recently. One, in particular, was by my stellar colleague, Liza Oates, who observed that contemporary naturopaths tend to respond to these clients in 1 of 2 ways:
a) Unaccustomed to a patient who eats, exercises, sleeps and balances their work & non-work worlds better than themselves…PANIC…
b) Dig deep back through the dusty archives of their personal & family medical history until they FIND A PROBLEM THEY CAN TREAT!!! such as, ‘Once I was constipated for a couple of days’ or, ‘Once I took a course of antibiotics’.
I know…we’re hilarious…we have to laugh at ourselves 😉 Liza offered up some great ideas about how to approach our consults with these patients. Many of her tips, however, could be applied to the rest of our patients as well to gather some really valuable insights. And it’s always great to hear from someone who has been seeing patients over decades…there’s so much to be gained from those who’ve gone before us (or alongside us…in my case!) and can speak to these firsthand lessons. Here are just a few of her pearls
The ‘not stressed’ patient
We encounter a lot of people who can misreport their stress levels, not because they are trying to lead us astray but that’s that slippery slope of self-reporting & the possibility that someone has normalised their ‘load’. Liza says she likes to step away from that potential trigger word, ‘stress’ and instead ask, ” What are your tell-tale signs when the demands exceed your capacity?”
This is not so that we can fulfil option b) mentioned at the beginning…digging desperately to find some unwellness to treat – but rather as an aid for both practitioner and patient alike to understand better that individual’s response to their psychosocial environment.
Ask them to design their own health retreat
If they reply, “I would start every day with a little meditation and yoga, a chai and then a healthy hot meal”, then these can be translated into little goals we can set to bring some of their ‘best self ‘ into their every day. It also helps to better understand their values, individualised self-soothing and self-care & great prescriptions to begin with, given they’re telling you they are already at contemplation in terms of their readiness for behavioural change. They’re not going to require too much convincing – they’re already converts they just need permission and support to implement.
And if you’re sitting there reading this and thinking, ‘Hey! These are exactly the patients I want my clinic full of”…then to hear more of Liza & Greg Connolly’s commentary and insights about how the wellness space has been hijacked by others and how naturopathy needs to move centre-stage in this increasingly popular trend, take a listen to this interview they recorded at the conference.
This UU30 recording from our back catalogue on the behavioural change model and how it impacts patients’ response to our advice is a key element in developing a professional approach that actually works. Unless practitioners are aware of the way that patients approach changing their dietary behaviour or exercise regimes, they the mystery of non-compliance will never be solved!
b. Every herbalist’s jaw at my table at the NHAA conference gala dinner, when I got almost all my Latin binomials right during the trivia quiz?…and after some champagne, that’s a particular achievement
c. My jaw, when I saw firsthand how much those herbalists could drink of ye-not-so-olde herbal extracts!!
d. The latest Update and Under 30 – Milk Madness Part 2
e. All of the above
If you answered, ‘e’…. you must have been one of those herbalists at my table, otherwise you have way too much insider information! But yes you are correct on all accounts. So this latest UU30 is an extension of our discussion last month about the potential contribution from to mental health from dairy intake in a subset of patients. This whole topic, the research for which dates all the way back to the 70s, was too big to fit into one – given the current evidence base that now depicts at least 2 different mechanisms that might be at play, and the different types of mental health problems, each has been linked with. Last month was all about retracing the ‘dietary exorphin’ path, this month it’s about the propensity for some individuals to make antibodies to casein and the significant growing data that suggest this happens to a larger extent in patients with certain psychiatric diagnoses. More importantly, we talk about the ‘why’.
What compelled me to make time to look through all the literature on this was that there is some. No seriously. When I initially learned of the GFCF dietary approach to ASD patients I was told that in spite of a lack of supportive research, the empirical clinical evidence was irrefutable, which I later saw with my own eyes. In the couple of decades since, I only really heard about negative findings, short trials of the elimination diet specifically in ASD kids, that failed to produce significant change. Funny how the bad stories rise to the top, right? But when I spent the time doing a thorough literature review, I found these negative findings were far from the whole story. In fact, I was really surprised by the high level of evidence employed by researchers of late, who have repeatedly found associations between either exorphin or antibody levels and patients with particular diagnoses, in addition to really progressing our understanding of why these measurable differences (urinary exorphins, plasma IgG and to a lesser extent IgA casein antibodies) are meaningful. Do we know everything? What do you think? The answer, of course, is always no. But we know enough to consider this aspect in our comprehensive workup of mental health patients and all their biological drivers and we know dramatically more than anyone in mainstream medicine, or the dairy industry for that matter, is ever going to let on!
If you want to hear a synthesis of the casein antibody link with mental health then download the latest UU30 – Milk Madness – part 2. If you can’t go that far, then “do yourself a favour” and read a couple of seriously important articles on this topic – and why not start at the deep end with this study by Severance in 2015.
Could dairy intake in susceptible individuals be a risk promoter for mental health problems? In addition to evidence of the exorphin derivatives from certain caseins interacting with our endogenous opiate system discussed in part 1, we now look at the evidence in support of other milk madness mechanisms. Specifically, the IgG and, to a much lesser extent, IgA antibodies about what this tells us about the patient sitting in front of us about their gut generally and about their mental health risks, specifically. The literature in this area dates back to the 1970s but the findings of more recent and more rigorous research are compelling.
So you’ve gone to all the effort. Be that writing referral letters suggesting some pathology investigations might be warranted or you’ve coached your patients endlessly to get copies of ones done elsewhere so that you may be privy to their findings. Worse still, you’ve directly requested the pathology, with your patient paying out of pocket for the tests. Then the results come in and they look…well wrong. You, as the conscientious clinician, typically do 3 things:
Step 1 Spend hours pouring over & over the labs and back over the case notes
Step 2 Worry about the new differential diagnoses that are now suddenly seemingly a possibility in your patient. It doesn’t look good.
Step 3 Doubt your own pathology reading ability, ‘Hey maybe I just don’t understand these bloods like I thought I did’
But (often)…it’s not you, it’s them.
And that’s what I often explain to practitioners who contact me (step 4). You see sometimes what they’re losing sleep over are what I call, Bad Bloods. Occasionally, the fault of the pathology company…but way way way more often the fault of the patient and the referring practitioner, who has not educated the patient correctly about what to do and not do prior to blood collection for certain tests. I am excited to see how many practitioners are competent with pathology reading these days and building their skills and confidence all the time, that’s why it is so so disheartening for the practitioners (and for me as a mother hen mentor) when they lose time (& sleep) getting to Step 3 when they should be able to spot ‘Bad Bloods’ fast. There are 7 classic give-away patterns.
Will are unlikely to know every quirk of every blood test our patients will ever have done, but knowing what constitutes the ideal time and conditions for the most commonly performed ones, can go a long way to minimising any future Bad Bloods between you and patient as well. This includes things like exercise, alcohol intake, duration fasting and even sexual intimacy…yup!
This month’s Update in Under 30 installment Beware of Bad Bloodsteaches you the 7 patterns to watch for and provides you with a great resource stipulating the best collection conditions for the most common blood tests. Don’t let Bad Blood come between you and your patient, the right diagnosis & management or just some well-deserved sleep!
Good practitioners are being led to bad conclusions by some patients’ pathology results. Not because they can’t interpret them or the testing has no merit but because they just don’t know when to discard a set because they are ‘bad’. Occasionally, the fault of the pathology company but much more often the fault of the patient and the referring practitioner, who has not educated the patient correctly about what to do and not do prior to blood collection for certain tests. This recording clearly describes the 7 classic give-away patterns of ‘Bad Bloods’ which will enable you to spot them fast in the future. In addition to this. while we are unlikely to know the idiosyncrasies of very lab our patients will ever have done, knowing the ideal collection times and conditions for the most common ones assists you and your patients to avoid any in the future – handy clinic resource included.
Hear all about it by listening to my latest Update in Under 30: Beware of Bad Bloods. For all Update in Under 30 Subscribers, it’s now available in your online account and if you are not a subscriber you can purchase this individually here.
How long? How long must we sing this song? I’m feeling a bit 80s anthemic and righteous. It turns out that patients’ bowel movements could be improved by using a foot stool?!! Who said that??
Only every naturopath, ever. Right?
But now medical researchers are singing the praises of the Stool Stool too…sorry, I mean the ‘defaecation postural modification device’…because lo and behold a new study of over 1000 bowel movements revealed using a stool to elevate your feet while on the toilet improved the speed and ease, improved full emptying, reduced the strain etc of laxation, >70% of the time, even in ‘healthy, non-constipated patients’. There’s a quick video you can watch to get across this groundbreaking research, or you can read the full article here. I’ve been educating patients about this for about 20 years and it never fails to revolutionise their world!
It would seem that elevating your feet results in straightening “the unnatural bend in the rectum that occurs when sitting on the toilet by placing the body in the squatting position nature intended”…hang on a second…who’s calling what unnatural???…I think the highfalutin anti-anatomical bathroom contraption, we westerners call a toilet, wins the ‘unnatural’ crown!
Next thing you know there’ll be a study that tells us squatting to have babies makes more sense that lying on your back…right?! 🙂
Love talking all-things Stool?
Fabulous Farty Fibre is a previous UU30 recording. Rachel at her warmest and funniest reminds us that fibre is a critical component to good nutrition and is often overlooked, partly due to the popularity of paleolithic and no grain diets. This UU30 details the important functions of different types of fibre and therefore the importance and therapeutic applications for fibre diversity.
Oh no, it’s her again 🙁 I mean the chick in the photostock image not the other ‘her’, me. I know. It’s the end of another mammoth year, you’re tired, worn out, used-up all your brain-power quota (a little projection?) and I can hear you begging for mercy when I start a sentence with…”So you think you know….” followed by, “blah blah blahIron,” but hear me out.
Correctly identifying & managing iron issues is a bread & butter part of our business, right?
With Iron deficiency affecting an estimated 1 in 5 women and Iron excess almost another 1 in 5 – patients with one form of iron imbalance or another tend to be over-represented in waiting rooms.
Anyone can spot overt iron deficiency anaemia or full-blown haemochromatosis but many health professionals find the ‘in-betweens’ confusing and fail to recognise some key patterns we see over and over again, that spell out clearly your patient’s current relationship-status with this essential mineral. This often results in giving iron when it wasn’t needed and missing it when it was. If you’re imagining someone else, i.e. the person who ordered the Iron Studies for your patient, will step in and accurately interpret the more curly results can I just say D-O-N’-T...they’re often as perplexed or even more so than you. After starting this conversation a year ago with So you think you know how to Treat Iron Deficiency, & its baby sister, So you think know the best Iron Supplements, our (imaginary) switchboard went crazy. While practitioners got the message loud and clear about how to improve the likelihood of treatment success in iron deficient patients, hot on the heels of this came email, after fax, after carrier pigeon, with examples of patients’ Iron Studies, the ‘somewhere in between ones’, accompanied by the equivalent of a dog head tilt…aka ‘I don’t get it’.
And this is to be expected.
What were you taught about reading Iron Studies? Was it made out to be all about ferritin? And TSH is a solid stand-alone marker of thyroid health, right? 😉
Were you introduced to the other essential parameters included in Iron Studies, explained how they contribute to your diagnosis and reveal important details about the patient’s ability to regulate this mineral or not? About when to dose and when to hold your fire?
Nah…I didn’t think so. But it’s up to us, people, to hone our skills in Iron Study interpretation…because individualised nutrition is our ‘thang’ and more than any other nutritional assessment, this collection of markers, actually allows us to go beyond the ‘one size fits all’ model…everyone must have X of this and Z of that in their blood tests…and see each patient’s actual individualised need and relationship with this mineral. In the latest Update in Under 30, I introduce you to 3 key players in iron assessment and the insights each offers become so clear, you’ll be able to read any combination or permutation of iron results that walk through your door. To boot, I’ve included a wizz-bang cheat-sheet of those iron patterns that are frequently seen and rarely recognised, including one totally novel one that I’ve never talked about before…to make your job even easier and put you well and truly ahead of the pack in understanding iron nutrition. It’s Christmas…and as the mantra goes…we can always fit just a little more in at Christmas time, right? 😉
Overt Iron Deficiency Anaemia or Haemochromatosis aside…do you understand the critical insights markers like transferrin and its saturation reveal about your patients iron status? Most practitioners don’t and as a result give iron when they shouldn’t and fail to sometimes when they should. This audio complete with an amazing cheat sheet for interpreting your patients Iron Study results will sharpen your skills around iron assessment, enabling you to recognise the real story of your patients’ relationship with iron.
A few months back I seriously ‘blew over’. Not on an RBT but on a UBT (Urea Breath Test). In spite of it being not the kind of test you want to score top marks for, my result was in the high 2000s, when all I needed was around 800 to confirm, and anything over 50 to be suspicious, that Helicobacter pylori had taken up residence in my stomach lining. I tell you, I knew it when I blew it! 😉 After ingesting the radioactive urea and waiting to blow up my sampling balloon, I felt like I could still fill a room full of balloons with all the gas being produced in my stomach and those balloons, I imagined, would all rise to the ceiling as if full of helium! Yep…I burped all the way home, which was representative of what I’d been experiencing daily for a month beforehand and what lead me to get the test done.
But initially, it wasn’t so clear.
The very first symptom I experienced was a sudden onset of severe tightness around my throat that lasted for minutes but started to happen multiple times in a day. Yep..no one panic. Together with a strange sensation of ‘extreme emptiness’ in my stomach on waking or delayed meals, and then mild nausea both with an empty and full stomach…only some days or weeks later the fabulously-unprecedented-&-socially-adorable-burping started, proper.
So a month or so later, I’ve solved my own mystery. Happy? Not in the least…where the heck have I picked up H.pylori from? Yes…that’s what I said because it had to come from somewhere people…right? I think there is much we have misunderstood about this bacteria with an incredibly long and interesting human history. Animals don’t and can’t carry this bacteria. The evidence suggests that it can’t survive for very long in the environment either (approx 4 days) but that is long enough to get into our food and water and maybe even onto shared chopsticks…just saying (listen in to hear the lowdown on all these and more!) Essentially hoomans are the traffickers, people! In fact one of the things that surprises people the most is the very high prevalence in young children and the clusters of positive tests & identical strains within families…but once you learn a little more about this bacteria…it won’t surprise you at all.(more…)
If you’ve not seen Kitty Flanagan’s skit on current coffee culture...it’s essential viewing. In true Kitty-fashion, she wants to simplify coffee ordering down to 2 basic lines – White or Black – says all our pretentious coffee orders; macchiato, skinny, decaf, half strength, latte etc can essentially be reduced down to a much faster 2 queue system. But she’s forgotten the line for taking your coffee rectally. Sorry – did I make you just spill your coffee? Knowing How across health trends Kitty is, she’ll add this 3rd queue soon, if the number of patients asking me about this or telling me they’re already doing it. Now, while enemas had a place in naturopathic history, my training never covered them and, consequently, I’ve never included them in my practice. But the more hype I heard around coffee enemas specifically, the more I thought we better find out as much as we can, so at least we can better inform ourselves and our patients. And of course the monkey on your back, called FOMO, jumps up and down, incessantly asking, “Are you (and your patients) missing out on an amazing therapy?”
The first patient who told me they were using coffee enemas daily was a celeb. A very anxious one. Who also told me she couldn’t possibly drink chai let alone coffee because of the caffeine. This had me a bit stumped…I knew she wasn’t inserting decaff up there and I thought…well given the colon is SUCH an absorptive surface surely this is why she reported feeling, ‘so energised, more clear headed’ etc. with every enema?
When I look back over how I’ve raised my kids there are a few serious ‘what tha…’ moments – like the time I thought shopping with a child in rollerskates was doable…I mean she loved those rollerskates and she was amazingly agile and good…just not quite good enough to hold onto that 1L Biodynamic Yoghurt sufficiently…who knew?! Dietary wise, I can look back and be critical in hindsight about different details, the contents of our fridge and pantry have morphed over the years with my changing knowledge (money & time!) but there are a few things I can confidently say – ‘Nailed it’, accompanied by a fist pump! We’re all meat eaters, not carnivores by any stretch of the imagination but we do partake, however the kids and I were just reflecting the other day on the absolute constancy of legumes in our life. (I know you want CCTV footage of our dinner time chats now don’t you 😉 ) There would rarely be a day in our house without them…several times!
Now I sound like I’m showing off but trust me it’s not that impressive or exotic – it goes a little something like this: soup,(split red lentils or cannellini), bolognaise & lasagne (1:4 brown lentils with the meat), nachos for school lunches (kidney beans 4:1 with mince), falafel & hummus (chick peas) & tofu (my kids love this stuff for snacks often & for mains at least once a week).
Ok now everyone relax, I don’t make our own almond milk, grow our own vegetables or ferment stuff…see…it’s swings & roundabouts 😉(more…)
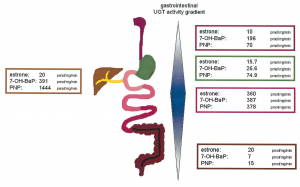
I’ve had my nose in all the research on Gilbert’s Syndrome again..watch this space…in the interim just thought I’d share this image and a couple of important details I may not have been able to convey when you last heard me talk (very fast!) about this important and common polymorphism:
While the incidence is approximately 10% of Caucasian population, rates are heavily influenced by ethnic background and the highest rates (up to 1/4) are seen in Middle Eastern populations
Gone are the days of thinking this condition only effects bilirubin levels and the enzyme responsible for its clearance – more recent research has shown over 3/4 of patients with Gilbert’s Syndrome have multiple SNPs that compromise clusters of enzymes within the glucuronidation pathway – with varying patterns – this goes a good chunk of the way to explaining the variability we see in bilirubin levels and symptom pictures across patients all deemed to have Gilbert’s Syndrome. This also explains why figures of reduced glucuronidation activity vary anywhere between 10% less to 90% less! It depends on your cluster..but the average reduction is around 50%
UGT enzymes, the ones affected in Gilbert’s, are also expressed all the way down the GIT and constitute important food and drug handling. These UGTs are most active in the small intestines,as you can see above, but may explain why Gilbert’s patients are ‘more sensitive’ to medications than just paracetamol!
And are you still thinking you need to run an $$$ gene test to confirm your Gilbert’s hunch in a client whose bilirubin sits consistently high normal or high? Think again… here’s a great little diagnostic short-cut that even theRoyal College of Pathologists Australasiacites as sufficient evidence to confirm the polymorphism:
In the face of elevated total bilirubin levels and in the absence of liver pathology or increased haemolysis to explain this..”If the diagnosis is uncertain the serum bilirubin fasting level can be measured and should exceed the non-fasting level by >50%.”
Nice. So that means you only need to demonstrate that the patient’s fasting total bilirubin levels go up by at least 50% compared with their fed levels and BINGO you have your diagnosis. Much easier. Oh and this image comes from an interesting paper from Tukey & Strassburg 2001 – but is probably not for the faint-hearted 😉
Stay tuned for more 🙂
Just new to this condition and need a soft place to land with understanding Gilbert’s Syndrome? This previous UU30 is just the thing! Affectionately called Gilbert’s Girls because in particular it details a set of twins with this condition, this short audio explains the basics about this common polymorphism and why we tend to see a lot of patients who have this…even if no one has pointed it out to them yet! You could be the first to provide them with this important understanding about how genetics is impacting their detox pathways, changing their sex hormone handling and perhaps setting them up for both mental health issues and some serious upset guts! Better still, what to do once we have that diagnosis.