Still. And yes – like you – I don’t see any slowing down any time soon in this extraordinary paradigm shift occurring in medicine and health. Which for us humans involves one humbling discovery after another.
Here we were thinking we made our dietary choices from a place of free will & individual preferences 🤣🦠
Thinking those microscopic mates, were making those B vitamins, and SCFAs and and and…for us & our benefit 🤣🤣🦠🦠
And while there’s a lotta love going on between our microbes and our micronutrients – in both directions – Pat Benatar said it best, “Love is a battlefield”
(sorry but I feel compelled to insert a link here for the youngsters – you’re welcome 😉)
The tussle over who gets to access those nutrients that are actually essential to both of us (the hostage and the microbiota) is an absolute turf war, peeps, and this battleground has seen some bloodshed! The new new question being raised is how the prescribing of nutrients, especially at the higher doses we tend to use, trickles down to influence and impact those microorganisms who reside in the bowel. Directly – as a selection pressure we have, likely unintentionally unknowingly, introduced. Which species do well when exposed to levels of a vitamin or a macro or trace mineral that are simply unobtainable in the diet? Yes – research answering these questions has begun in earnest revealing some positive ‘prebiotic-like actions’ of some but not of course for all nor in all scenarios. Want to learn more about this latest aspect we need to consider when formulating our nutrition prescriptions? You can either jump in and join us in the Nutrient Prescribers Program which kicks off next week to get across absolutely everything new in nutritional medicine or just dip your toe in here with our latest Update In Under 30: The Micronutrient Microbiota Universe
The world of health science went microbiota-mad a few turns back and there’s no sign of an end. Research continues to reveal the breadth of the GIT microbiota’s positive & negative reach, in particular, & with discovery upon discovery we’ve come to understand how often the microbiota are ‘managing us’. Both in terms of being integral to the success of our digestive, immunological, metabolic etc processes but also in a self-serving way, for example, directing our dietary preferences to satisfy their own needs. This has understandably prompted the question about the impact micronutrient supplementation is unintentionally having as a selection pressure on our gut microbes. Which bugs like which B vitamins when taken in excess of the amounts achievable in the diet? And which microbes flourish and which falter when we radically change their mineral exposure?
You can purchase The Micronutrient Microbiota Universehere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
I’m intrigued by the silence. Hair loss in women is frighteningly common, following pregnancy, menopause & with extreme stress (wait is that a tautology? 🙄) In fact it can strike at any age and for a multitude of reasons. When it happened to me a few years back I also initially responded with silence, terrified that if I said it out loud it would make it real, but when my daughter suddenly asked, ‘Mum are you losing your hair?’ with her trademark attention to detail & exquisite empathy, she gave me the words & a good kick into gear, simultaneously. Now I am fascinated by women’s silence around this generally, how little we share our stories & forewarn others, & as practitioners, the lack of adequate training we’ve had identifying the different types (hint: it involves donning gloves or if restricted to online consulting, knowing how to organise correctly positioned pics) & from there finding the right solutions.
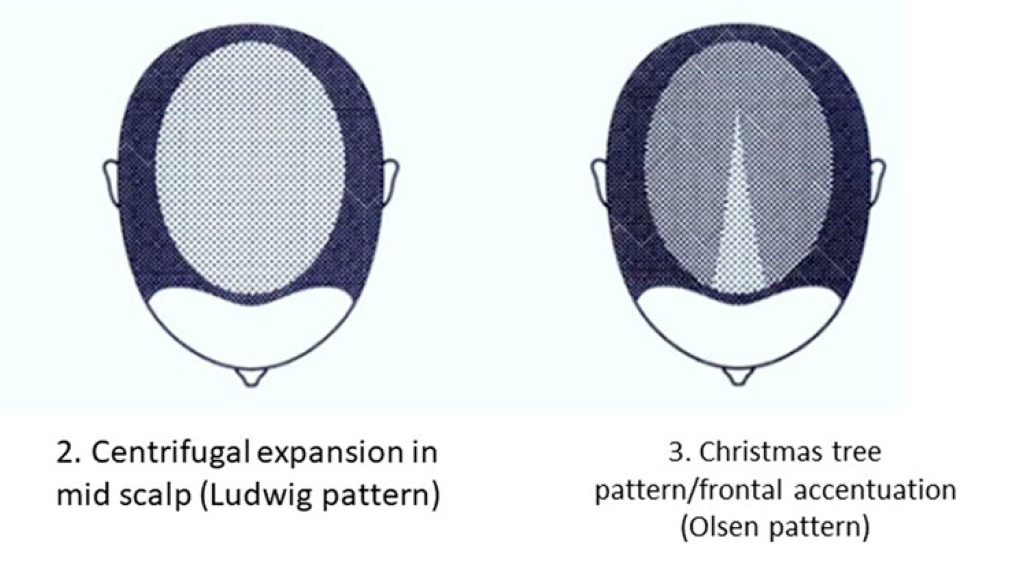
While Female Pattern Hair Loss (FPHL) is the dominant type in women – it only applies to the following pattern:
But alopecia due to stress, thyroid disorders, autoimmunity, contact dermatitis etc will affect different regions of the scalp and with a different onset & progression.
And remember, by the time YOU, the practitioner, can spot a patient is losing hair when they simply walk into the room, they have ALREADY LOST 50%😢 This is why I think we need to push back against the silence. The research is unflinching about the serious psychological impact this has on women – especially in cultures which place so much emphasis on looks generally, and hair, specifically as a commodity of very high value in women. The diagram above comes from a 2019 update on the phenomenon of FHPL and it’s a good articulation of the knowns and unknowns (pssst spoiler alert…it ain’t about androgens!) but let’s never forget the other causes and cures. So let’s make sure as the trusted practitioners women present to so often, we are sensitive enough to have this tricky conversation & skilled enough to help 💪
Stop Pulling Your Hair Out – The FPHL Answers You Need
Female Pattern Hair Loss (FPHL) is everywhere, perhaps you just haven’t been looking. As the leading cause of alopecia in women globally and with 1 in 5 women affected at any age, we’ve all got clients who have FPHL to different degrees. We need to be better able to recognise the early features of this condition which profoundly impairs quality of life and induces depression in its sufferers and that begins with validating patients’ concerns when they report “thinning” or “increased losses”. But what do we do from there? This recording talks you through the assessment, diagnosis and management of FPHL based on a combination of the most recent research and Rachel’s clinical experiences. Once you’ve ‘seen’ FPHL.., you won’t ever ‘unsee’ it and your patients will thank you.
No, this is not a trick question & it’s certainly not a silly one. IBS, as many of us know, has a very loose diagnostic criteria: visceral hypersensitivity coupled with altered motility in the absence of organic disease. Hence it tends to ‘loosely’ fit a vast number of patients struggling with GIT issues. The differential diagnostic algorithm all health professionals are encouraged to use for patients presenting with GIT issues leads us to this IBS label, just as soon as we’ve excluded the red flags. But this ‘early opt out’ according to many experts, including Schiller et al in the American Journal of Gastroenterology, tends to propagate the illusion we’ve reached our diagnostic destination: practitioners stop thinking about the ‘why’ & stop looking for the real drivers & causes, which is the key to shifting the refractory patient into remission.
For those presenting with chronic diarrhoea, Bile Acid Diarrhoea (BAD) is in the diagnostic algorithm & there is strong evidence it’s at play in almost half of these patients! It’s just that BAD, is the next station along the line after IBS-D, which means most clinicians have sadly disembarked already 🙁
Bile acids, as key biological agents, in both the behaviour & health of the gut & metabolic dx, are getting a lot of attention right now. While Bile acid malabsorption (BAM) in disorders of the small intestine such as Crohn’s & undiagnosed or refractory Coeliac dx, as well as other miscellaneous GIT disorders that clearly disrupt the bile acid balancing act of the gut-liver axis, have been known for a long time, there’s a new kid on the gut block, previously only known as the idiot, I mean, idiopathic BAD. But us idiots have finally worked it out! This is not about malabsorption but about excess production of bile acids and this pathophysiology is drastically over-represented in IBS-D patients.
And knowing if your IBS-D patient has a ‘BAD-thing’ going on, every researcher wants you to know, is game-changing. Explaining the strong heritability of this particular IBS subtype and the reason so many patients are refractory to standard IBS approaches.
We need to use distinctly different dietary strategies when IBS is BAD. Once again patients are our greatest teachers & I’ve relished the excuse one practitioner and her patient gave me to deep dive into the enormous body of BAD research, that is ‘so hot right now’! The way I look at, ask questions about and assess patients with chronic diarrhoea, especially IBS-D, is forever changed 💪🙏
When is I.B.S. B.A.D?
This is not a trick question. Up to 50% of all patients diagnosed with IBS-D actually have bile acid diarrhoea (BAD) underpinning their digestive complaints as well as some patients with unresolving diarrhoea post-cholecystectomy and gastro. Knowing which ones do and how to manage this, which requires distinctly different approaches from our general management of IBS, is the key. As always, good lessons come from those we learn in the clinic and this story starts with a patient and how we came to recognise the BAD in her belly.
Well, this is different, now I’m watching you! 😆 In early 2021 we released our very popular MasterCourse I: Comprehensive Diagnostics, as a ‘self-paced’ online offering for the many who missed out on attending live in 2020. Many have grabbed this opportunity with both hands (& a headset and some hardcore Do Not Disturb! signs) but we know that for some, doing the entire course on your own, >24hrs of video presentations, can be a tad onerous & overwhelming. We want to remove these barriers and empower & upskill as many practitioners in pathology interpretation as are keen, and as a means to achieve this, we’re offering the MasterCourse I Watch Party. So bring your bhujia and a beverage and let’s do this!!
Practitioners who sign up for this will be able to watch each session’s video replay live with other practitioners and have the opportunity to ask Rachel questions & participate in case discussions at the end. Another key detail is that we will run the sessions weekly, so that the full course is covered in just 6wks, from July 8th to August 12th.
MasterCourse I: Comprehensive Diagnostics LIVE WATCH PARTY 24 hours of live Zoom sessions + Bonus sessions! 8, 15, 22, 29 July & 5, 12 August on Thursday at 3.30pm to 7.30pm AEST.
Each Thursday, the video presentation for that week will be played so we can watch it together. Then Rachel will open up her webcam and mic, inviting you to do the same, to participate in a Q&A as well as set case discussions. When you register, you get immediate access to watch our preliminary/preparatory sessions, prior to 8 July: Accurate Pathology Interpretation Starts Here and the RAN Patient Pathology Manager Tutorial.
Below is an overview of the Watch Party schedule.
Week 1 – 8 July | SESSION 1: Acid Base Balance & Electrolytes
Week 2 – 15 July | SESSION 2: Renal Markers Week 3 – 22 July | SESSION 3: Liver Enzymes
Week 4 – 29 July | SESSION 4: Lipids & Glucose
Week 5 – 5 August | SESSION 5: Immune Markers
Week 6 – 12 August | SESSION 6: Haematology
“I thought my pathology skills were pretty up there until I did Rachel’s Diagnostic Masterclass course! Nothing like being knocked off my perch by a literal avalanche of new information, especially when it comes from the most commonly tests that we all use so often. The course has been a fantastic learning opportunity for me, and has since helped me pick out many intricacies in cases that have previously been missed.
The course structure was great, the level of detail was right up my alley, and the case studies were entertaining (in true RA fashion). Once again Rachel has increased my knowledge base, and help me provide way better service to my patients.” – Rohan Smith, Naturopath
Join Rachel on MasterCourse I: Comprehensive Diagnostics Watch Party and register here.
MasterCourse I is a pre-requisite to join MasterCourse II which will be delivered live in 2022.
What does lockdown look like for you? More time spent…
A) Learning or B) Losing sleep over things outside of our control or C) Losing days just watching Tik Tok
I’m choosing ‘A’ and I know I’m keeping good company because last week many of my ‘nearest and dearest’ gathered on 2 occasions for some serious extra brain gym. The first was the ACNEM Fellowship Community of Practice that I had the privilege to co-chair with Dr. William Ferguson. A fantastic new initiative by @ACNEM to offer more hands-on mentoring and support to their doctors.
The second, our own Give-back-Gratitude Live Q & A for our Update in Under 30 Subscribers where I used the time to check-in and see if we could further the learning offered by our monthly audios and clinical tools.
Having all of those who attended, in my ‘home’ was a fabulous contrast to our social distancing ‘new norm’, and seeing all those lovely faces and buzzing brains behind them, warmed the cockles of my cortex!
For those of you that couldn’t make our UU30 date, I wanted to share a few things we learned in lockdown this week:
Copper can be absorbed through the skin and penetrate to deeper layers potentially increasing serum levels butthe degree of uptake is highly variable and more likely with prolonged contact e.g. jewellery and pastes not showers etc
Just like the Zn:Cu, when reviewing patients’ albumin:globulin, we must first look at each value individually and consider causes and consequences of low or high values, otherwise we can ‘miss the message’
When understanding labs of anybody who is not a couch potato we need to ditch reference ranges based on the general population because they essentially are…couch potatoes and ask ourselves 3 questions: 1) Whois this person outside of being ‘sporty’2) Whatis the nature of their sportiness because exercise ain’t exercise in terms of physiological effects and 3) When are the tests being done in relation to any exercise
On that last note, I am so thrilled to be able to share my brand spanking new presentation The Impact of Exercise on Pathology Tests – Beyond Artefact to Understanding which I put together B.C. (Before COVID19) for a NZ speaking engagement. This actually has been one of the most satisfying areas of research to expand my own knowledge in…explained a LOT about what labs go whacky (and why and how to navigate around and through this) not just in what you might call ‘real athletes’ but in weekend warriors, crossfit crazies, MIL (men in Lycra) and the increasing number of middle-aged or older women who just love pounding the pavement. Know the types? Our clinics are full of them…it is time to learn their labs properly.
Overwhelmingly when we look at our patients’ labs we compare their results with a reference range derived from ‘the general population’ aka couch potatoes! Therein lies our first problem. Exercise is recommended for health but we don’t know what this ‘looks like’ in terms of labs. The reference ranges reflect and assume ‘average’ muscle mass & haemodynamics & ‘average’ nutritional requirements in people consuming the SAD (standard Australian diet) none of which apply to the exercise enthusiast, weekend warrior, least of all the professional athlete! Given an increasing number of our patients are embracing exercise, this is an important instruction in what healthy looks like, how to make meaning of otherwise meaningless comparisons and ultimately enable you to distinguish between what is healthy exercise-induced adaptation, an artefact and an actual aberration that flags possible negative impact of emerging pathology for other reasons.
Click here to add The Impact of Exercise on Pathology Tests to your online RAN Library.
For all UU30 Subscribers the full Live Q&A Recording is now available in your ‘active content’ of your online account.
I had the privilege of presenting at the Integria GIT Symposium last weekend. For those of you who attended, you’ve gone back to your clinic with a bunch of new ideas and inspiration I hope…oh and a new respect, terror and watchfulness for threadworm thanks to me! In my presentation I outlined the many presentations of this infestation, what to watch for and the risk of chronic recurrence due,in particular, to a reduced ability for some individuals to produce chondroitin sulfate which renders the GIT environment hostile to worms.
Chronic threadworm is a huge & grossly under-recognised issue in paediatrics, often presenting as behavioural & cognitive disorders (and these can be severe), bruxism, enuresis etc. of course, but another presentation typically missed is vulvovaginitis, vulval pain or UTI like sx in young girls.(more…)