It’s no secret I am in the midst of some serious deep-diving through the micronutrient evidence base & at a depth of about 30 metres I struck Boron! Don’t yawn! I saw that. Thinking, ‘boring’, when we hear, ‘Boron’, is almost as bankable as watching everyone reach for their water bottles when you mention anything hydration-related 🤣 But I am here to restore your positive regard for this mineral and remediate its bad (& boring) rep! In preparation for the Nutrient Prescriber’s Program we started each nutrient review with the seminal contemporary nutritional texts and then launched ourselves headlong into the latest & greatest research. By the end of all the Boron bits in all my trusty texts the yawn was not gorn! But the moment I started reading the research I was like, ‘Are we even talking about the same thing?!’Turns out we’re not 😵🤦♀️
You see Boron has been a longstanding victim of identity theft. What we’ve been lead to believe is Boron is weed-killer and ant-poison and look it does give us some of the benefits of Boron but not all. And it possess a pharmacokinetic & toxicity profile that naturally occurring Boron simply does not.
Who decided that the Boron that is ubiquitous in our environment but almost exclusively consumed by us only after biotransformation by plants – could just skip that last bit and still be safe and optimally beneficial?! Probably the same guy that came up with folic acid, may I suggest? Anyway, enough is enough. We all need to relearn Boron – naturally occurring Boron – in the form of Sugar Borate Esters (SBE)- the evidence of benefits for which will blow all of our little minds! Well it certainly blew mine! Looks like this natural form of Boron is going to hit the Australian market in the not-too-distant-future 🐦 can’t wait to see which supplier is sufficiently progressive and research-aware that they bring this to market, having been available as a high grade supplement, employed in numerous RCTS OS for some time. But this little Update in Under 30 is not waiting around for that release date – there is much to be gained from SBEs right now – so make some noise as the real Boron at last takes the stage!🎤
Boron has been the victim of longstanding identity theft and we unknowingly have been interacting with its imposter. Contrary to everything you’ve ever been told about this mineral, naturally occurring Boron is full to overflowing with benefits for our gut, our bones, our brain, our management of other minerals and is safe in large quantities. That ‘bad guy Boron’ you were introduced to and is still present in many of your supplements is a form we never consume in food…and therein lies a world of difference! Come meet the real Boron so you and your patients can get the real benefits!
You can purchase The Boron Deception: How We’ve Been Fooledhere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
Wow, menopause is really having a moment, isn’t it? Or is that just me (and my mates who are all somewhere on that perimenopausal path)?! But seriously, medical perception of this reproductive transition is undergoing a revolution right now—widening the lens to take in more diverse potential presentations and lengthening the period of impact recognised both ‘before, during, and after’ that last, last…no hang on…last period. But I fear we are at a crucial crossroads. Anything could be related to (peri)menopause, but not everything is or should be.
There are several other conditions whose onset tends to rise or peak at the same age and stage for women, and due to their shared features, they get missed & misdiagnosed, misattributed to that!(more…)
Any steps towards inclusivity in societal & cultural terms are cause for celebration but in medicine, that can come in the form of a ‘diagnosis of inclusion’, the opposite, of course, of a ‘diagnosis of exclusion’ and potentially as slippery and loose as it sounds. That’s the somewhat precarious position we find ourselves presently in with perimenopause and menopause. With greater recognition of just how long health effects can kick in before there are any cycle changes [2-12 years for those of you playing along at home] and the widening lens now taking in the diversity of such health effects, women’s health has had a win. But, I would argue, this is not without a double edge. After all, aren’t we, as a result, more at risk, as women, of having everything attributed to “just ‘the change’, love”, and, in turn, going to be offered sex hormones more often as the solution?
Let’s play a word association game of minerals & their major roles
I say, ‘Potassium’. Maybe you say, ‘Sodium Potassium Pump’ I say, ‘Magnesium’. You say, ‘Muscles?’ I say, ‘Calcium’. You say, “Bones’….
But I say, Second Messenger. And arguably the most pervasive & potent one, at that. Remind you about second messengers? Well, sure. They are the ones who get sh*t done. Not like a boss (i.e. hormone or neurotransmitter) who shout directives from above but never step foot inside the dirty guts of the engine room itself. It’s the second messengers who run these messages from the outside of the cell to the inside and the engine room, to ensure that the directive is actually actioned! Amazing huh! And free calcium in the blood is, as I said, really a superhero even among the second messengers – with its regular responsibilities including: Insulin, TSH, Adrenaline, Oxytocin, Serotonin receptor activation etc etc
Does, it have a dark side? Well, sure. Don’t most superheroes?
If the available Calcium in blood and the extracellular environment is too high then basically bad sh*t gets done. Including vasoconstriction, clotting, deposition of calcium in the wrong place like arteries and joints and etc etc. That’s why the amount of Calcium in our blood is the MOST tightly regulated of all electrolytes and, in turn, has the NARROWEST of reference ranges. But will a Serum Calcium level always tell you when there is a problem with Calcium regulation? No. You’d need to have measured the major regulator itself, Parathyroid Hormone (PTH). Wait, am I seriously trying to tell you, that Serum Calcium alone can look completely normal in spite of really damaging Calcium dysregulation underway – leading to accelerated BMD loss, increased cardiovascular and renal risks etc.? I most certainly am.
So do you know which of your patients’ really need PTH assessment and why 1 dominant group amongst those, is any woman leading up to and following menopause?
No? Well you better pull up a pew and have a listen and a watch then! Yes this latest Update in Under 30 episode even comes with a little video tutorial!🤓🤯
Parathyroid hormone is a career criminal. In addition to buoying dropping blood calcium levels via legitimate means, it illegitimately achieves this by stealing it from our bones. But you wouldn’t know it – because like all career criminals this occurs completely under the radar. Elevated PTH, however, constitutes the most modifiable risk factor for bone mineral density loss & fracture risk and offers the biggest BMD gains secondary to its normalisation. In addition to this, even within range but ‘high-normal’ PTH correlates with a range of other cardiovascular and urinary presentations & if combined with elevated serum calcium can become a multi-systemic presentation (GIT, Mental health etc) frequently mistaken for other aetiologies. So how can we be alert to this ‘bone thief’? Which of our patients will benefit the most from PTH measurement and monitoring? This recording, resource & video tutorial on how to use a Ca PTH Nomogram answers all!
You can purchase Unmasking Hyperparathyroidism – Menopause & Morehere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account. You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
I shared this recently on socials but for those of us that don’t hang around that ‘hood I am sharing again here because it is just too important. While we’re busy updating our knowledge regarding reproductive health for women (soooo many huge headlines of late!)…ahhhhh…this might be something we all want to read!🤓
This thought-provoking reviewchallenges the long held assumption that oestrogen is at the root of much breast cancer causation. Instead it creates the case for PROGESTERONE as the actual source of oncogenesisand relegates oestrogen to merely (but monstrously) fanning the flames.
Now before anyone panics (?too late ) you need to read the article in its entirety – esp this not being about demonstrable differences in measurable P4 levels – and keep in mind that this hypothesis, though well argued and supported by evidence also from trans-gender individuals, is not currently a consensus. BUT what I think it does really well is SHAKE THE TREE🌴🥥 and prompt us to challenge our own biases and blind-spots. For far too long in IM Oestrogen has been made out to be the baddy. I too am guilty of having done that. And Progesterone everyone’s saviour! Of course there are a lot of PMDD sufferers who have good grounds to punch us for even suggesting this.
But of late – many of my peers have helped remediate oestrogen’s reputation and put us back on a more balanced path – I am thinking of @Sandra Villella especially here.
Who straight away responded to my post regarding this on socials, “I just got back from the Australasian menopause Congress in Queenstown, and the different types of exogenous progestogens are certainly implicated in breast cancer.” And then generously shared some of the hot off the press slides and stats from the Australasian Menopause Society.
In a nutshell she says, “Breast cancer increases with age and with increased time of use and those increases are greater when Progesterone is included in the MHT prescription”
And whoah…maybe we all need to rethink all the pro-progesterone prescribing…dare I say?!
Btw – the article implies that having anovulatory cycles might actually be protective too!!
Not my normal space and speciality area but I keep finding these gems in women’s hormonal & repro health and I feel a duty of care to share!
Update and Under 30 Podcast episodes are streamed monthly audios and resources to keep you up to date with the latest ‘must-knows’ in integrative medicine, covering a wide variety of topics from diagnostics to diet, all through the lens of an integrative health model. Every month each new episode will provide you with a quick scientific review with ‘clinic-ready’ practice tips, in under 30 minutes. In addition, the subscription gives you access to the ENTIRE back catalogue of UU30 audios that have been released…that’s over 120 episodes! You can become an Update in Under 30 Subscriber to access the entire library of Update in Under 30 audios and resources here.
I can barely bring myself to write the word given how overused it has been of late 🤐🙄😯😕🙃 But I gotta say something! If we have found ourselves currently in a place where every second (or indeed single!) patient has a ‘histamine issue’ then I am afraid that it is we, that have an issue. (more…)
Have you been told somewhere by someone that the ‘perfect’ TSH is 1.5 mIU/L? This is a wonderful, terrible & wonderfully terrible example of ‘magical numbers medicine’. As a push-back against the published reference ranges we’re given, that are so wide you could drive a truck through them, there has been an over-correction by some, leading to the myth of ‘magic numbers’. We can narrow the reference range substantially for many parameters with good rationale, make no mistake about that but once we start setting ‘aspirational goals’ that are explicitly rigid…well we’ve done 2 things 1) forgotten about the patient to whom this result belongs and 2) disregarded viewing each result as part of a ‘pattern’, that we must piece together and make sense of.
Back to TSH then… if my obese patient had a value of 1.5 mIU/L this in fact would be woefully inadequate – so too a child at any weight.
And we expect a higher value as well in our elderly clients too and this level there may be, in fact, increased mortality.
But the same result would be excessively & worringly high in my patient who’s undergone thyroidectomy.
Realising the full value of any test result in terms of what it reveals about the person sitting in front of you, requires these more thinking and more thoughtfulness. Unfortunately, a list of ‘magic numbers’ will often lead you astray. And building your scientific knowledge about labs will not only help you avoid the pitfalls of pathology but will strengthen your pathophysiology prowess in surprising ways, saving your patients a packet in terms of additional extraneous testing and help you truly personalise your prescriptions…because the ‘invisible (biochemical individuality, oxidative stress, genetic probabilities, subclinical states, imbalanced or burdened processes etc) just became visible’. I started requesting lab results early in my career and years later was lucky enough to be taken under the wing of Dr. Tini Gruner. I found some of our shared notes, from 10 years ago, scribbled all over patient results recently and I was struck by just how lucky I was to have her encouragement to really pursue my interest and how she was a guiding force about learning to recognise pathology patterns over single parameters. A decade on I can concede, much of my clinical and educative success has come off the back of this foundational skill-set and I know, this is true for so many I’ve taught too.
“The guidance I’ve received over the years from Rachel in relation to pathology interpretation has been one of the most valuable (and fascinating) investments I’ve made as a clinician. Her teachings have filled gaps in my knowledge base I never knew needed filling and have significantly enhanced my understanding of the inner workings of the body! Rachel has an incredible ability to make the numbers that patient’s so often present us with, both understandable and clinically meaningful. The knowledge I’ve gained by investing in this skillset has paid off in dividends and I’m certain will continue to do so into the future.”
Stacey Curcio – Cultivating Wellness
I hope you’ll join me for the most exciting up-skilling opportunity in learning labs yet. Oh…and all this talk about thyroid testing..this next MasterCourse series is focused on revolutionising your understanding of thyroid, adrenal, HPT & HPA markers based on the very latest research & findings & marry these together with everything you learned in MasterCourse I (ELFTs, FBE, Lipids & Glucose) to understand the ‘whole story’.
…an absolute treasure trove of free integrative health information about your patient!
DEEP DIVE INTO REAL CASE STUDIES TO DEMONSTRATE EACH PATHOLOGY PATTERN IN ACTION. ]\
There are limited places. To sign up for Rachel’s LIVE Series – MasterCourse II: Thyroid & Adrenal Diagnostics and for more information click here.
I’ve spent the best part of about 4 months recording my *NEW* Advanced Thyroid Assessment training. I told my team this would be easy and quick, given it was to be based on a great little 2-part, 2hr updated presentation I delivered just last year for ACNEM!! Sixteen weeks (like seriously…most of it) numerous rewrites and retakes later, our final product is 4 parts that goes for over 12hrs in total & has a bonus Adrenal recording! And yeah my team are impressed but unimpressed too if you know what I mean?!🙄🤪
Every time another, ‘Oh wow!’, or ‘No way!’, escaped my lips, it was a source of personal celebration, as another deeper layer of learning revealed itself.
But to the wonderful, somewhat weary and definitely wary Sally, who does all my powerpoints, it was met with, ‘Oh boy!’, because it meant many multiple new slides to build full of visual metaphors, animation acrobatics, if not an entire new Part!*#@^
Her sage advice along the infinite research road I’ve been travelling was : ‘Stop. You’re going to have to stop.’
So I didbut now I am this meme. Everything I see currently through the lens of thyroid health, I talk in tongues TFTs and my brain is one giant neural network of integrative endocrinological circuits! I have fallen in love with this topic, this neuroendocrine axis and its ‘first responder’ role all over again! Hence our little thyroid character below – all ‘antennaed’ up – is one of the many tools we’ve developed for this training, to teach us that ‘bad thyroids’ per se are extremely rare – but bad scenarios are common (too much or too little of any macronutrient, key micronutrients, a change in the internal or external environment etc etc) and this little fellow and his board of directors (no – not the hypothalamus or pituitary!) – well it’s their job to ‘read the room’, right?!
In the absence of this key understanding we risk: A lot of lazy labelling in thyroid health – ‘You have a bad thyroid – that’s why you…[can’t lose weight, feel tired, have SIBO etc]’ Misdirected treatment & especially a tendency to overload the butterfly with ‘thyroid’ nutrients – which can do more harm than good
I’ve said many times, ‘perfect number pathology is a myth’ but it runs rife in practitioners’ beliefs about TFT results with complete disregard of the person those labs belong too! Did you know, for example, that your TFTs should all be higher if your BMI is? That your T4:T3 ratio should never be 3:1 if you are on replacement, have hot nodules, are pregnant or are acutely unwell etc etc etc? How about how low your Selenium or Iron levels need to be before this factor will influence the actual levels of thyroid hormones measurable – & what the impact of these deficiencies are well before then that is far more sinister and serious? Yep…you see here I am, pouring just some of the tiny take-homes of Advanced Thyroid Assessment ALL over you!
Watch this space my new Thyroid training is just around the corner!
An increasing number of our patients have thyroid concerns but unbeknown to many of us the most likely explanation of all is thyroid nodules, whose incidence is on the rise globally. The development of nodules has always been primarily viewed as a nutritional disease. Traditionally attributed to chronic iodine deficiency but recently novel nutritional causes have emerged. Benign nodules come in 2 flavours: hot and cold and while patients can present with a mixture, it is the presence or absence of a hot nodule that radically changes what complementary medicines you can and can’t use and what an effective treatment plan looks like. The pointers, as is often the case, are there for us in the patient’s presentation and pathology, so knowing the difference is no longer a guessing game. This UU30 comes with a great visual clinical resource and includes key papers on the nutritional management of nodules.
Copper deficiency happens in kids, so does copper toxicity and both are serious concerns, but do we know when to accurately call either? First, we have to know ‘normal’. If we know what normal Serum Copper values look like in children, then we can easily spot those falling below or above this, right? That’s the first hurdle we tend to knock over and break a toe on! Being a mineral whose levels vary widely in soil from country to country, globally, the differences in reference ranges are breathtaking & absurd. Add to that, that copper is a key mineral in kids, driving huge demand for it during key periods of development, so the range for pre-schoolers isn’t the same as the primary or high schoolers – not that your lab is flagging that. Unhelpful? Yes. Dangerous, even? Potentially.
To diagnose ‘Copper Excess’ in a child is a big call to make.
One, because most practitioners are unaware just how much Copper a child really needs at each age & two, high copper is often a messenger for something else going on and then three, the primary objective based on this diagnosis becomes to lower their Copper but we could be either shooting the messenger or missing the mark all together…right?
Copper excess does happen but not nearly as often as practitioners believe it does. And in kids, the fall-out from such misdiagnosis is bigger. And missing a Copper deficiency? (because we’re not as well-trained to recognise it and because Copper has been sadly demonised) Likely to have myriad negative impacts at this vulnerable age…almost none of which generate symptoms or a distinct clinical picture e.g. secondary iron deficiency, low neutrophils without necessarily compromised immunity. But what about the holy grail get-out of jail adjective: ‘relative’. You know, ‘this is at least a Copper excess relative to their Zinc?’
Well, to form this opinion you’re likely calculating the Zn:Cu ratio and applying an ideal adult value of 1:1 but show me the primary evidence that supports this for kids…anywhere? The Zn & Cu relationship shifts as we move through life-stages and in fact Copper is supposed to dominate through a lot of our childhood so…ummmmm…no.
HTMA Copper side-steps all of this?..double no.
I used to make the same mistake re Zn:Cu, I may have even taught you this?!🤦♀️ But as so often happens, a week spent in all the original scientific data and I’ve emerged a changed practitioner! Having been part of perpetuating this problematic premise in the past, I am determined to get the correct message out there to as many practitioners as possible. So help me spread the word on Copper in Kids – by telling others that this mineral is so critical to kids compared with adults, they will often have higher levels than ‘us’ and that until you’ve applied the right age-appropriate reference range and ruled out confounders you can’t possibly make a call on Copper. I mean, we kind of knew this all along, with healthy pregnancy Copper values being exponentially higher being a giant clue. Turns out kids’ ‘Copper Age’ extends way beyond the womb.
Copper, as a kingpin in angiogenesis, brain & bone building & iron regulation is a critical mineral during paediatric development. So much so, the kind of blood levels we see in a primary schooler might cause alarm if we saw them in an adult. So too their Zn:Cu. But higher blood Copper and more Copper than Zinc are not just healthy but perhaps necessary during certain paediatric periods. This recording redefines normal, low and high with a great clinical desktop tool to help you better interpret these labs, as well as reviewing the top causes and consequences of both types of Copper imbalance in kids.
The latest Update in Under 30 has landed. You can purchase January’s episode, Copper in Kids here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
-Your RAN Online Account has a NEW LOOK!!-
Next time your log in, you will experience a more user friendly way to search, view, listen and download your resources. Find out what’s new here.
Earlier this year at a Mental Health Training for IM doctors, 3 practitioners (myself, a doctor & a psychiatrist) walked into a bar…not really, but we did each present a case study of challenging patient & in whom we had some great outcomes. All 3 patients presented happened to have Gilbert’s Syndrome. Just in case you’re wondering if there was a secret Gilbert Syndrome Conference you didn’t get an invite to, no. Or that perhaps there was premeditation and intention on the organisers behalf for a bit of sub-theme and focus, no. While this was purely coincidental it does speak rather loudly to a couple of things though.
Patients with Gilbert’s syndrome are likely to be over-represented in our client base especially among those presenting with psychiatric and/or gut issues (and both presentations frustratingly for them, very hard to diagnose, define, pigeon hole etc) and secondly, even though their genes underpin their biological susceptibility to such health problems, great outcomes are really possible.
One of the challenges comes from the medical dismissiveness of this genetic issue as simply ‘benign hyperbilirubinemia’. This has lead to a lack of diagnosis in patients affected and when it is incidentally picked up on routine bloods, a lack of follow up education about what having approx. 30% less phase 2 glucuronidation activity, in their gut and their liver, is really likely to mean, not to mention radically altered bile composition and digestion (!) and how they can make better choices in light of this. Similarly this year in our Mental Health Specialist Mentoring Group, the issue of reduced efficacy and tolerance of psychiatric medications, in those with Gilbert’s, raised its head over and over again. Given that so many drugs within the psychiatric class add at the very least to the ‘substrate load’ of the UGT system, if not frankly inhibit some members of this enzyme family, as this paper (check out Table 2…superb!) shared by my colleague, Kate Worsfold, points out, it actually shouldn’t come as a surprise.
But there is a change a’coming with an influx of research leading to improved understanding of this seemingly mercurial malady, resolving many riddles, identifying new key ways to help these patients and at last….some exceptionally good news for those with Gilbert’s.
For example, when I started this conversation back in 2013 with the Update in Under 30 Gilbert’s Girls, that was in response to seeing so many women at the time presenting with significant imbalances in both their sex hormones and their neurobiology as a result of their UGT impairment. But of course it was never meant to imply GS is just a girl thing! In fact there is a 3:1 dominance of men with this condition and some very good reasons as to why: more red blood cells and more testosterone…the former being the primary source of bilirubin and the later a terrifically powerful UGT inhibitor. The news from the research frontier is nothing short of thrilling, rewriting our thoughts on what medications and supplements (!!) are the most problematic, improved dietary management, how to track their progress more accurately and why completely normalising their bilirubin is not the goal…hey did someone say…longer telomeres?! 😉
The latest Update in Under 30 has landed: Gilbert’s – New Goals and Good News and my team has gone all out in producing a brilliant desktop reference to go with this recording that aids better understanding and clear treatment aims for your GS patients.
You can purchase Gilbert’s: New Goals & Good News here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
**But if you’re just joining us & this important conversation now,
ideally get the basics and backstory first and purchase all 3 key episodes in ‘A Guide to Gilbert’s Package’
-Your RAN Online Account has a NEW LOOK!!-
Next time your log in, you will experience a more user friendly way to search, view, listen and download your resources. Find out what’s new here.
I take my job to heart. When someone asked me recently to choose the single value that spoke most to me personally I couldn’t seem to go past, ‘Purpose’. I feel very honoured to have contributed to the learning of so many health professionals in their undergraduate and so many more in their professional careers following graduation and I know that with this comes huge responsibility. Second on my values list (again, possibly unsurprising) is Empowerment & coming in with a photo finish at 3rd:Integrity. Discernment and critical thinking (about information, about research, about reflective practice) are perhaps the eggs in this souffle, helping us all to rise up.
As part of our critical thinking we need to accept a few truisms:
Research changes Experience changes Knowledge changes
Information is not static. So we need to ask ourselves, how long ago did I learn this? How long since I’ve checked it is still correct? And just because perhaps this information came out of the mouth of our mentors or teachers, makes it no less up for regular review. I’m trying to undertake these internal audits on a regular basis. Typically they’re prompted by bloody good questions my mentees have asked me. A question I can’t answer or, more to the point, I can’t answer with full confidence I’ve double-checked my old beliefs and understandings against new evidence recently…these almost always provoke a lost night of sleep for me. Not from sleeplessness per se but due to immersing myself in the latest research and performing a mini informal lit review, bringing out all my old beliefs/evidence etc. Marie Kondo style and asking do they still spark joy✨ (in light of the latest evidence)?! And yes sometimes there’s a little bit of heartache when you have to let your old tightly held beliefs and understandings go 😢
The 1st update is about N-acetyl cysteine. Some of you may have heard me previously question the efficacy of the vegan form. Now that all but 1 Australian product is vegan, produced from bacterial fermentation or purely synthetic, I was wayyyyyyyy overdue to check the validity of my old ideas. Let the record show, I was wrong. Unlike some other nutraceuticals like chondroitin sulphate, wherein the source radically changes the overall structure of the molecule and therefore its uptake and actions – the same is simply not true for NAC.
So those ducks, & their NAC rich feathers, can all sleep a little easier at last…phew! Now the 2nd internal audit well that did cause some tears for me…
We often identify patients who could do with a little glucuronidation first aid: marked dysbiosis, Gilbert’s syndrome, oestrogen excess, cancer risk (especially bowel, breast & prostate) and one of our nutritional go-to’s has typically been Calcium D Glucurate. While there is ample evidence that one of CDG’s metabolites: 1,4 GL – inhibits beta-glucuronidase, is an antioxidant, platelet activation inhibitor and generally all-round good guy to have onboard, new research strongly challenges that oral CDG will convert to this at levels sufficient to support this detoxification pathway. Sounds like we’re overdue for an update on this supplement and when and where it might be useful in addition to how to find the real deal in real food!
When a teenage girl presents seeking her first oral contraceptive pill (OCP) script, what information is she privy to that enables her to make an informed decision? Read the insert inside the box? Please. Which 50 year old, let alone 15 year old does that? Forget it! What might her doctor tell her? Perhaps about clotting risk, as part of their determination of the suitability of this form of contraception for her but is there any discussion about the potential for adverse mood effects? A recent study of over 1,000 teenage girls followed over more than a decade adds to other evidence that suggests this should be flagged as a consideration prior to the prescription being written.
Most integrative health practitioners not only know about the potential negative impact on mood from OCP use in women but we’ve observed firsthand the havoc it has wreaked in some teenage girls’ and women’s lives.
A very experienced practitioner I know says, ‘if I am hearing mood instability and then I see a significantly elevated serum copper and or cortisol in these girls that’s when I just say to have to say to them, you know I don’t think this is the best contraception for you!’
This latest study did not find higher rates of depression across all OCP users in this group of 16-25 year olds but when they looked at this at different ages they found its use increased depression scores and was associated specifically with more crying, eating problems and hypersomnia. The discussion around the enhanced vulnerability at this younger age compared with older girls centres on the relative immaturity of their CNS. But wait, I hear you critical thinking clinicians ask, perhaps those teenage girls had more depressive features prior to starting the OCP. Good thinking 99! And the answer is…maybe…but the relationship goes both ways: from the related Medscape Continuing Medical Educational Activity
“For 16-year-old girls, the association was weakened after adjusting for depressive symptoms before use of OCPs, but the findings remained significant. This suggests that the relationship between OCP use and depressive symptoms could be bidirectional…For instance, 16-year-old OCP users were more sexually active and had more stressful events, as well as more menstruation-related pain and acne, than their counterparts in the nonuser group. Analyses showed that all these factors weakened the association, although none diminished it.”
The commentary surrounding this latest study is essentially 1) this is not the first study to find an association and others have been more able to demonstrate that COCP use predated the mood disorder in those affected and 2) those exhibiting higher depressive scores did not actually score strongly for anhedonia or sadness which are the most typical features in adult depression – so perhaps we are missing some of these negatively impacted young women. Awareness regarding reproductive psychology is rapidly growing and in Australia we are fortunate to have emerging hubs to seek help and specialist advice in this area, such as the important work of Professor Jayashri Kulkarni and colleagues out of the Women’s Mental Health Clinic. I’ve referred patients, both when a patient’s mental health appears to be caused or aggravated by use of hormonal agents but which they can’t not use for various reasons and for those small number of women in whom I feel hormonal management may in fact offer a psychiatric solution. So again I am asking, while we know & mainstream medicine increasingly knows about this association…who’s telling these young women?
How many of your clients are on a combination OCP? Do you know the full extent of the physiological impact as a result and are you able to identify to key pathology indicators of the size of that impact?
We’re all aware that in theory OCP use correlates with a range of elevated risks but in reality many females will make the decision that the pros, in terms of contraception or control of acne etc., outweigh the cons. What if we could provide more individualised advice by looking to their pathology results and identifying and quantifying specific danger signs for each individual? This approach enables us to better support patients who chose this form of contraception and to accurately identify those that should be be encouraged to find other safer options more biochemically suited to them. Learn more here.
This year I heard a great quote that hit the spot for me: anyone who offers you a simple solution to a complex problem is lying or misguided, the solution to a complex problem will inherently be complex. Dang! I’m frequently reminded of this in relation to many different aspects of working in integrative health. Or even just answering work-related questions socially. Random-friend-I-haven’t-met- yet, upon finding out I work in nutrition, asks: Is [insert any given food, beverage, macronutrient, micronutrient] good for you? In spite of over 20 years of this happening, I confess, the poker face still requires concentration.
The poker face is necessary of course to
a) conceal my amusement at how predictable humans are and
b) to cushion the blow for them as I tear down the delusion that real nutritional science is simple and can be served up in a soundbyte or
c) lie and infer that it is, just to get out of there faster!
But recently, I’ve had another reminder of that ‘in here’ rather than ‘out there’, about how even as practitioners we long for things to be simpler than they are. This month in mentoring I’ve been talking about the dark side of both zinc and Akkermansia muciniphila (I know wash my mouth out right?!) in neurological issues. What, but we had them on the good guys list?! Remember the answer to a complex problem (and human health surely owns this territory) will inherently be complex, right? Similarly, I’ve been digging deep in research about beta-glucuronidase, that enzyme that undoes our phase 2 detoxification of oestrogen, bilirubin and a long list of nasty xenobiotics, earning it the informal title of ‘bad ass biomarker’…scoundrel! And well, I’ve found some really nice things to say about it…like actually it extends the half life of most of our flavonoids such as quercetin, isoflavones etc etc and that’s a great thing for increasing their positive punch given that their rapid detoxification limits how much we can benefit from them. Turns out, like everything else, even dear old beta-glucuronidase exhibits light and shade.
How I ended up losing a weekend to such papers was because I was trying to resolve some burning questions about Ca-D-glucurate (CDG) that I’ve had for as long as I’ve been recommending it to people who arguably could benefit from a little less beta-glucuronidase activity.
My two most pressing ones were: How much is required to be effective & Where’s the evidence?
And that’s when the fight broke out [just in my head] You see every review I’ve read, every piece of product information too, repeats the mantra CDG 500mg TID but turns out this is based on…not much. More uncomfortable still, is that even our assumption that we can convert CDG into its active form has been strongly challenged. The new research, which is not the work from the 1990s that everyone cites, is a must read…or if you actually have a life, and other ways to spend a weekend then maybe just spend 30 mins with me in my Update in Under 30 this month 😂 I wanted to keep it simple and neat and tidy. I tried I promise. But in the end…wouldn’t you know it…it’s complex.
So to bring everyone up to speed, including myself!, I recorded an UU30 on…
The ABC of CDG We often identify patients who could do with a little glucuronidation first aid: marked dysbiosis, Gilbert’s syndrome, oestrogen excess, cancer risk (especially bowel, breast & prostate) and one of our nutritional go-to’s has typically been Calcium D Glucurate. While there is ample evidence that one of CDG’s metabolites : 1,4 GL – inhibits beta-glucuronidase, is an antioxidant, platelet activation inhibitor and generally all round good guy to have on board, new research strongly challenges that oral CDG will convert to this at levels sufficient to support our detoxification pathways. Sounds like we’re overdue for an update on this supplement and when and where it might be useful in addition to how to find the real deal in real food!
Sometimes we wonder who put the invisible sign up out the front of our practice, right? The one that says…absolutely everyone with Condition ‘Z’ come and see me, now! I’m sure you know what I’m describing. Well this week I have hit the trifecta, performed a neat little hat-trick and diagnosed 3 patients with Gilbert’s Syndrome who all present in their own individual way but actually each one also with quite a textbook Gilbert’s picture, it almost beggars belief. Have a little look
70yo Female says: Since childhood she has felt like she has had a rock in her stomach after she eats. This ‘rock’ is there for hours. Her stools are never the same in spite of a regular diet and she has always been uptight and anxious. All her bilirubin results are in the 20s & she reports she’s ‘always’ had high values
55yo Male with severe ‘constitutional anxiety’ and surprisingly high oestrogen and a worrisome profile of oestrogen metabolites. His bilirubin is in the 20s
30yo something Female presents with unexplained severe unwellness for 20yrs that mostly involves nausea, bloating, a functional gut disorder without a real diagnosis, anxiety, depression and poor stress tolerance. Her bilirubin fluctuates between 30 to high 40s.(more…)
Duck duck GOOSE!Do you know this game? That’s how I’m feeling with oestrogen – high-high-high-LOW!-of late. Likely similar to your experience, the majority of my female clients battle with oestrogen dominance, therefore I get so used to looking for it, expecting it: the high Cu, the profoundly elevated SHBG, maybe a raised ESR. So much so that sometimes the low ones can catch you out, especially of course when it happens in women way way before menopause.
We’re so resolved to hear bad press about oestrogen and to be armed ready to saturate our patients with broccoli extracts of the highest order – do we remember the clinical features and markers of an oestrogen deficit and know what to do with those women who simply don’t have enough?(more…)
During mentoring sessions over the last week I’ve been prompted to ask a few practitioners if their patient had any signs, either clinically or in their pathology results, of high oestrogen.Each time it kind of caught the practitioner off guard because their patients weren’t presenting with conditions overtly related to an oestrogen excess and they hadn’t specifically ‘tested’ for this. However, in each instance the information was already there in the case, it was just a matter of knowing what markers to look for.
So some patients scream ‘high oestrogen’ right from the minute they enter the room? But often others present with health problems that don’t necessarily appear related at first glance. Regardless, their condition absolutely could be being compounded by this background imbalance – think thyroid & other autoimmune conditions for example.
There are plenty of patients who don’t have the exaggerated clinical presentation but still have this imbalance as a significant compounder or perpetuating issue in terms of their pathology.
Relax – I am not suggesting salivary hormones or any form of expensive testing all round (!) – in fact what I am saying is before you even consider yet another pay out of pocket test, costing your patient more time and money, we should look to the clues that are already there, in standard blood tests. Amazingly, you can infer a lot not just about the overall oestrogenic load but also pick up some clues as well about where the excess might be coming from.
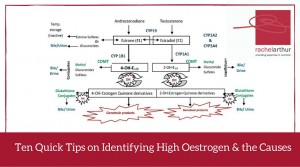
In this Update Rachel brings together her 10 quick tips on how to recognise either high oestrogen and/or the potential underpinning reason behind the excess, in a range of easily accessible markers. A great refresher and synthesis of ideas on this important aspect of diagnosis and clinical management. This Update in Under 30 is now available to purchase as a download, click here to find out more or if you’re interested in a 12mo subscription click here
 Wow, menopause is really having a moment, isn’t it? Or is that just me (and my mates who are all somewhere on that perimenopausal path)?! But seriously, medical perception of this reproductive transition is undergoing a revolution right now—widening the lens to take in more diverse potential presentations and lengthening the period of impact recognised both ‘before, during, and after’ that last, last…no hang on…last period. But I fear we are at a crucial crossroads. Anything could be related to (peri)menopause, but not everything is or should be.
Wow, menopause is really having a moment, isn’t it? Or is that just me (and my mates who are all somewhere on that perimenopausal path)?! But seriously, medical perception of this reproductive transition is undergoing a revolution right now—widening the lens to take in more diverse potential presentations and lengthening the period of impact recognised both ‘before, during, and after’ that last, last…no hang on…last period. But I fear we are at a crucial crossroads. Anything could be related to (peri)menopause, but not everything is or should be.

 You can purchase
You can purchase