And it will. It knocked again on a practitioner’s door last week. She in turn knocked on mine. It turned out to be a very familiar story:
Firstly:Patient presents distressed – recently a nurse applied the term ‘Chronic Kidney Disease’ to HER (note no one has ever mentioned this diagnosis) Secondly:She is in stage 3 of 5 Then: This practitioner is left to have ‘the conversation’ but wants to know where to start, ‘What do I say?’ Next up:And what else can I do for her – are we really able to make a difference?
Familiar to you too? So,1st & 2nd: Yes, this is not uncommon we would have to say and even with age-appropriate reference range adjustment, her GFR consistently in the 50s, flags premature decline. Then: What DO you say? Well this clearly is a delicate area, not only because of the level of patient distress and concern but because, at this stage the practitioner knows nothing more than what the patient tells her and her ELFTs over the last 2 years. This is not enough information, right? Chronic Kidney Disease is a heterogeneous condition, with many different causes, manifestations, comorbid conditions, and factors affecting prognosis (Levey et al., 2009) So while most individuals certainly progress from stage I to II and II to III the rate at which they do this differs dramatically.
Two years of data is not long enough for us to appreciate the trajectory of her CKD & means we are unable to provide the patient with any kind of perspective:
‘With no further decline in GFR or progression in stages over 5 years, you’re doing well, so keep doing what you’re doing!’ Vs ‘Ok, I can see what looks like a little period of accelerated decline – let’s review what’s been happening and how we can turn this around”
“Please sir can I have some more?’ Yes, back to her primary carers to request more information to fill in the gaps, and ideally more labs to calculate & observe the trajectory for yourself. Next Up: What do we have to offer the patient with CKD stage III? Soooooooooooooooooooooooooooooooooo much!! When is adequate hydration helpful? Always, except Stage V! (and these patients are not coming to see us) What are our treatment objectives & our evidence backed medicines to meet these? Hcy lowering (note often referred to as ‘folate refractory’ in renal dx), vitamin D adequacy, lowering the acid load, supporting the microbiome & in turn the Renal-GIT axis…hang on, got to go…someone’s knocking 😅 but hopefully we all can see, when they present to us, they are indeed knocking on the right door ✊
Nutritional or naturopathic support for the kidneys tends to have been over-looked in our training and yet research suggests there is much in our tool kit that can make an enormous difference to this system, in particular, slowing the progression of chronic kidney disease in patients. Rachel talks about what these key evidence based interventions are and also gives you the tools to identify the early pathology markers of renal impairment – the earlier the recognition, the earlier we can make a start on the remedy.
It seems almost farcical to question the merits of hydration for our renal health but is this actually the truism we have been lead to believe? Where does the recommendation of ‘8 glasses a day’ come from and what is the level of evidence to support it and in whom? Or should we in fact be setting our sights on output ie. 24 hr urinary volume, over input. Do all kidneys love water – or does this relationship change with the progressive impairment seen in CKD which affects up to 30% of our middle-aged population? When does hydration become harassment?
Most practitioners graduated with not much more than a few ‘kidney’ herbs and an under-appreciation of the contribution renal health makes to wellbeing. It’s not just about waste and water. In reality, the kidneys are pivotal in just about every major element: blood, bones, pH balance, methylation, control of oxidative stress, the GIT microbiome and more! And we are seeing the impact of this in our patients in all sorts of subtle and not so subtle presentations. This new instalment in diagnostics, brings the renal system into the spotlight so we can confidently identify and better manage its critical contribution. In addition to this, just like with other routine labs such as LFTs, we unpack how these so-called ‘renal markers’ can flag a plethora of other insights into your patients, from reflecting (un)healthy muscle mass, to calculating individual dietary protein adequacy, from key ‘danger and distress’ signals in response to disturbed metabolism, oxidative stress to certain types of GIT dysbiosis! We call this Explained, Expanded and Exploded because these routine labs can deliver XXX sized insights into your patients.
I’m intrigued by the silence. Hair loss in women is frighteningly common, following pregnancy, menopause & with extreme stress (wait is that a tautology? 🙄) In fact it can strike at any age and for a multitude of reasons. When it happened to me a few years back I also initially responded with silence, terrified that if I said it out loud it would make it real, but when my daughter suddenly asked, ‘Mum are you losing your hair?’ with her trademark attention to detail & exquisite empathy, she gave me the words & a good kick into gear, simultaneously. Now I am fascinated by women’s silence around this generally, how little we share our stories & forewarn others, & as practitioners, the lack of adequate training we’ve had identifying the different types (hint: it involves donning gloves or if restricted to online consulting, knowing how to organise correctly positioned pics) & from there finding the right solutions.
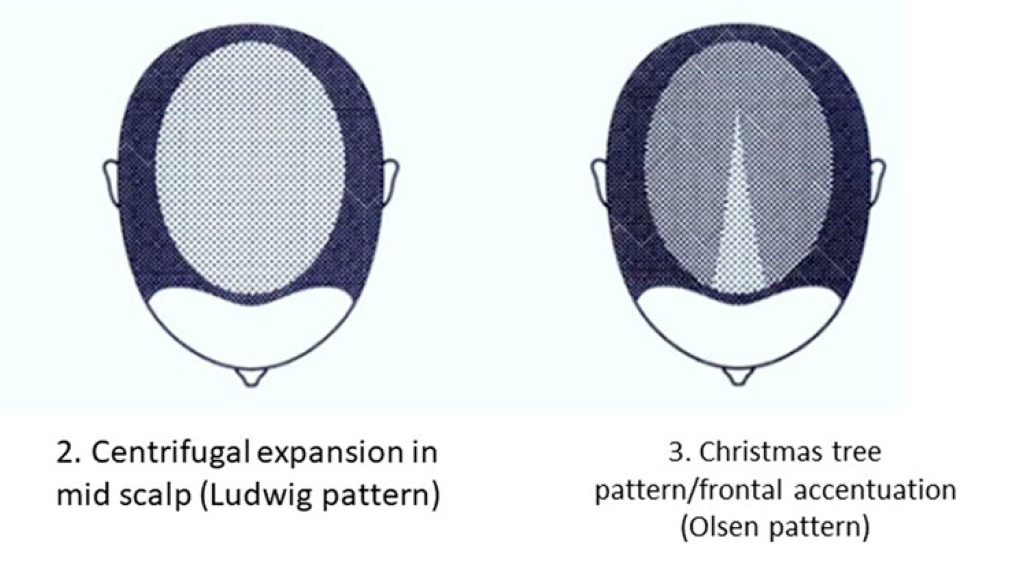
While Female Pattern Hair Loss (FPHL) is the dominant type in women – it only applies to the following pattern:
But alopecia due to stress, thyroid disorders, autoimmunity, contact dermatitis etc will affect different regions of the scalp and with a different onset & progression.
And remember, by the time YOU, the practitioner, can spot a patient is losing hair when they simply walk into the room, they have ALREADY LOST 50%😢 This is why I think we need to push back against the silence. The research is unflinching about the serious psychological impact this has on women – especially in cultures which place so much emphasis on looks generally, and hair, specifically as a commodity of very high value in women. The diagram above comes from a 2019 update on the phenomenon of FHPL and it’s a good articulation of the knowns and unknowns (pssst spoiler alert…it ain’t about androgens!) but let’s never forget the other causes and cures. So let’s make sure as the trusted practitioners women present to so often, we are sensitive enough to have this tricky conversation & skilled enough to help 💪
Stop Pulling Your Hair Out – The FPHL Answers You Need
Female Pattern Hair Loss (FPHL) is everywhere, perhaps you just haven’t been looking. As the leading cause of alopecia in women globally and with 1 in 5 women affected at any age, we’ve all got clients who have FPHL to different degrees. We need to be better able to recognise the early features of this condition which profoundly impairs quality of life and induces depression in its sufferers and that begins with validating patients’ concerns when they report “thinning” or “increased losses”. But what do we do from there? This recording talks you through the assessment, diagnosis and management of FPHL based on a combination of the most recent research and Rachel’s clinical experiences. Once you’ve ‘seen’ FPHL.., you won’t ever ‘unsee’ it and your patients will thank you.
I confess I was a chemistry nerd ‘way back when’, but my skill for stoichiometric calculations had sadly slipped by the time my kids needed help with high-school science & now my son, who’s about to graduate from chemical engineering, is my ‘chem-friend’ 🙄🧐 I suspect he feels FB messenger wasn’t intended for such use – or at least there should be some veneer of, ‘Hi darling how are you?’ before…’Need to talk through these pharmacokinetic datasets’ However, the one equation that was like turning a light on in my brain & therefore never forgotten was the Fenton reaction – basically metals’ MO for messing with our biology, especially iron. Turns out – it’s the most essential and helpful in understanding health & disease:
Endometriosis IBD Neurogenerative disorders: MS, PD, Alzheimer’s Higher than healthy GGT Impaired COMT or catechol excess for other reasons Cardiovascular disease & Diabetes Vitiligo Both the Big Cs Heavy metal burden Iron dysregulation (Obesity, HFE mutations, Thalassaemia) & Excess (IV or oral over-treatment etc)
(almost) All roads lead to radicals & reactive species…if you follow the Fenton pathway & iron leads us down this path more often than any other metal. Certainly sometimes for good: like protecting us against pathogens and destroying dodgy cells, but when it gets out of hand, a key pathophysiological process in a long list of disease. So understanding how to recognise patients prone to dysregulation of this mineral, avoiding iron over-treatment at all costs (I am seeing incorrect and excessive use of IV iron in many patients make it stop!) and identifying means to contain and control its movement, are important. Oh and in case the Fenton has faded in memory, it goes a little something like this:
While rates of iron deficiency and related anaemia continue to grow, the increase in prescriptions of IV Fe have expanded exponentially in western countries. What is behind this change in practice regarding how we treat iron deficiency and does it match with responsible prescribing? Do the benefits always outweigh the risks? And while we’re on the topic, who is most likely to benefit and what are all the risks? In light of a current class action in the US, relating to a lesser talked about adverse event associated with IV Fe and recent complaints here in Australia against GPs, allegedly due to inadequate information to enable informed patient consent…it’s time to answer these questions and more. When is IV Fe a means of rescue and when is it a risky repletion strategy with no evidence of advantage? Click here for this episode.
Maybe it’s tax-time, just my wintery whinge or a tirade triggered by missing my twins’ 21st birthday due to border restrictions 😶 butI’m sorry for all the shouting of late…about interpreting iron studies, about the copper misinformed etc etc. and my gorgeous new grad mentees copped a full monologue, with links to articles, recordings & the Coeliac Society, when they asked me to expand on why we must exclude coeliac disease before removing gluten from anyone’s diet. I was so glad they asked though! I’m now using my inside voice.
But I don’t want my message to be misdirected and I fear it might be. It’s not you and it’s not me
‘We’ are doing our best. We are working in a field that demands us to be across soooooo many domains of knowledge and information, from the basic & not-so-basic medical sciences, to pathology interpretation, nutrition, herbal medicine and beyond. It’s a lot. None of us are across it all. I’m certainly not. And I’m aware, that the frustration I feel at others’ misunderstandings sometimes is unfair, because I’ve benefited from excellent early teachers all the way through to having a job now, that keeps my head in the research daily. And even still, without a doubt, the gaps & shortfalls I observe and criticise in others, I could have made of myself, earlier in my career. We don’t know what we don’t know, until we know better, right.
It’s them
Who is this ‘them’ of which I speak? Well, 25 years ago when I completed my under-graduate (and walked 10 miles to school in the rain, without shoes or breakfast 👵) I believe I received the training required to be the naturopath that I needed to be. Safe, effective, knowing my scope – which was basically coughs. colds, atopy and risk mitigation for future chronic disease. I never saw a lab test during my under-grad. I would have read a set of iron studies badly and something like ELFTs, like it was Latin. I wasn’t made aware by my lecturers of the critical part I could play in my patients’ lives, either by advocating and advancing correct diagnosis or by obscuring, confounding and delaying it (sorry, still thinking about the gluten debate!). But back then, I think this was appropriate for the time, the state of play of our collective medical knowledge and for the role naturopaths were playing in the health landscape. Not any more.
If you haven’t had a chance to read the extensive research about ‘us’ (Australian nats, nuts & herbalists) published of late, who we are, what we do, how we are viewed and what our patients expect, then you could be in for a surprise.
We’re perceived by many, if not most, of our patients to be a primary health care provider – either flying solo or co-piloting with the patient’s GP (& no auto-pilot function!!!) and as clinicians for chronic comorbid cases not the acute cold. My how times have changed and the question is – has the knowledge and level of competency of those in educational roles & the quality of what they deliver a good fit? Sorry, but if the majority of a large new graduate cohort have left their training with a mantra of ‘we must not diagnose’ and INTSEAD are likely to advocate a gluten free diet RATHER THAN Coeliac testing with the patients doctor first – then we’re falling at the first: Primum non nocere. Sorry,I forgot, inside voice 🙄🤐
This Update in Under 30 recording speaks to the seriousness and primacy of identifying Coeliac Disease in any patient reporting a suspected reaction to gluten and takes you through the latest evidence on the best screening protocol. With an increased understanding about the strengths and limitations of gene testing, serology and biopsy, we have a clear map to follow now. Along the way Rachel outlines 3 additional potential mechanisms for ‘gluten’ reactions amongst our patients, what to look for and how to tell the difference.
Name a B vitamin. Hey, Bingo! It’s on the list! What list? The complete one from all the review papers & references to possible links between individual nutrient deficiencies & Angular Cheilitis – inflammation & cracking at the corners of the mouth. So does that mean more Bs are the answer for people presenting with this painful, recurring issue?…Ahhhhhh No. Yes, you heard me correctly, these deficiencies rarely cause the breakdown of the integrity of this very specific area of skin in the patients we see. So now we have a double ouch, right?
We might send patients away with a B complex and some lip balm and over a week the cheilitis resolves – which one was the most therapeutic? …I hate to tell you 👀
What is the underpinning cause(s) & the important message we are missing with this presentation? Well, it could be one or more of a long LONG list of differentials, ranging from anatomical, habitual, immune related to iatrogenic. And while many nutrient deficiency pictures can include this feature and therefore make the ‘possible’ list, only one makes the ‘probable’ list. And that’s iron but only in severe deficiency, aka anaemia and only affecting 1 in 5.
Me???
…Telling anyone to push the nutritional issues further down the list of differentials for any condition? Well, that’s unexpected
…possibly unprecedented
And no, antifungals aren’t the answer either. Yep, that might be worth a listen….👂
Just an annoying, embarrassing, cosmetic condition or could it be the clue that helps you ‘crack the case’? There is a surprisingly long list of differentials for this condition but most of us only know a few, reflexively reaching for either B vitamins or anti-fungal creams. Does either make sense? Does either address the cause(s) which we now recognise to be a unique series of risk factors in each individual? Or are we at risk of shooting the messenger and missing the message of Cracking Corners altogether?
You can purchase Cracking in the Corners – Angular Cheilitishere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
[Ahem] Ok let me explain…Several catch-cries from Australian ads have earnt themselves a lifelong place in my head and heart, taking up space where something more important should be, no doubt, but does anyone remember this SPC canned fruit (REALLY showing my age now!!) one, where the little boy chases the grape around the bowl and declares it a, ‘Slippery Little Sucker!’? Ok so this little boy is every one of us when we’re trying to ‘capture someone’s cortisol’ and just like the boy we will eventually achieve a ‘result’ – get a ‘number’ but what in fact does this mean in relation to your patient’s HPA axis, stress perception, responsivity, recovery etc etc?
Recently I was presented with 2 cortisol results for a patient taken within the same 24hrs – her blood am result was above range, while her 24hr urine flagged under-functioning of her HPA axis generally. Both were accurate.
Had I have only have seen one, I would have formed the wrong opinion and only gleaned part of her overall HPA story. Every different type of cortisol capture – from different mediums: blood, saliva & urine – to different collection conditions: time of day, fasting V fed, specific stressor exposure etc answers a different question about our patient’s HPA axis. So to use any form of cortisol assessment well we need to start with 2 understandings: 1) it is a slippery little sucker indeed and no one test can answer all our questions – or as Miller & colleagues more eloquently put it, “Remember, all models are wrong; the practical question is, how wrong do they have to be to not to be useful” and 2) be clear about the most important question you have about your patient you are trying to answer and that will make your choice of test (& timing & & &) patent. But do you know enough about cortisol regulation to be clear about the ‘sweet spot’ of each test?
The Cortisol Awakening Response has understandably attracted the bulk of the research focus over the last decade and accordingly has risen in popularity in practice & while it remains a very valuable way to answer certain questions about patients, our understanding of its limitations continue to grow. For example there is a disconnect between CAR & diurnal cortisol secretion – so in essence your CAR can look woke but your ‘Slope’ may be broke! If you’re a fan of this method, make sure you catch up on the CAR-Expert Consensus Guidelines by Stalder et aland if you’d like to get clear about which test and when, when it comes to all the key options for Cortisol Capture..
then let’s dive in together with my latest Update in Under 30 instalment
I have! And just recently a stark contrast between the results from 2 different methods of cortisol capture in the same patient illustrated just how likely this is. How do we ‘capture’ something so ‘dynamic’ and interpret anything of substance from a ‘static’ assessment technique? But rather than throw up our hands and throw out the whole attempt to measure cortisol, we can improve the rigor, reliability and real-world meaningfulness of our patients’ results by refining our timing of tests, choosing the medium wisely & manipulating test conditions to answer specific questions about their HPA function. Great desktop reference included!
You can purchase Cortisol – Have You Been Caught Out?here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
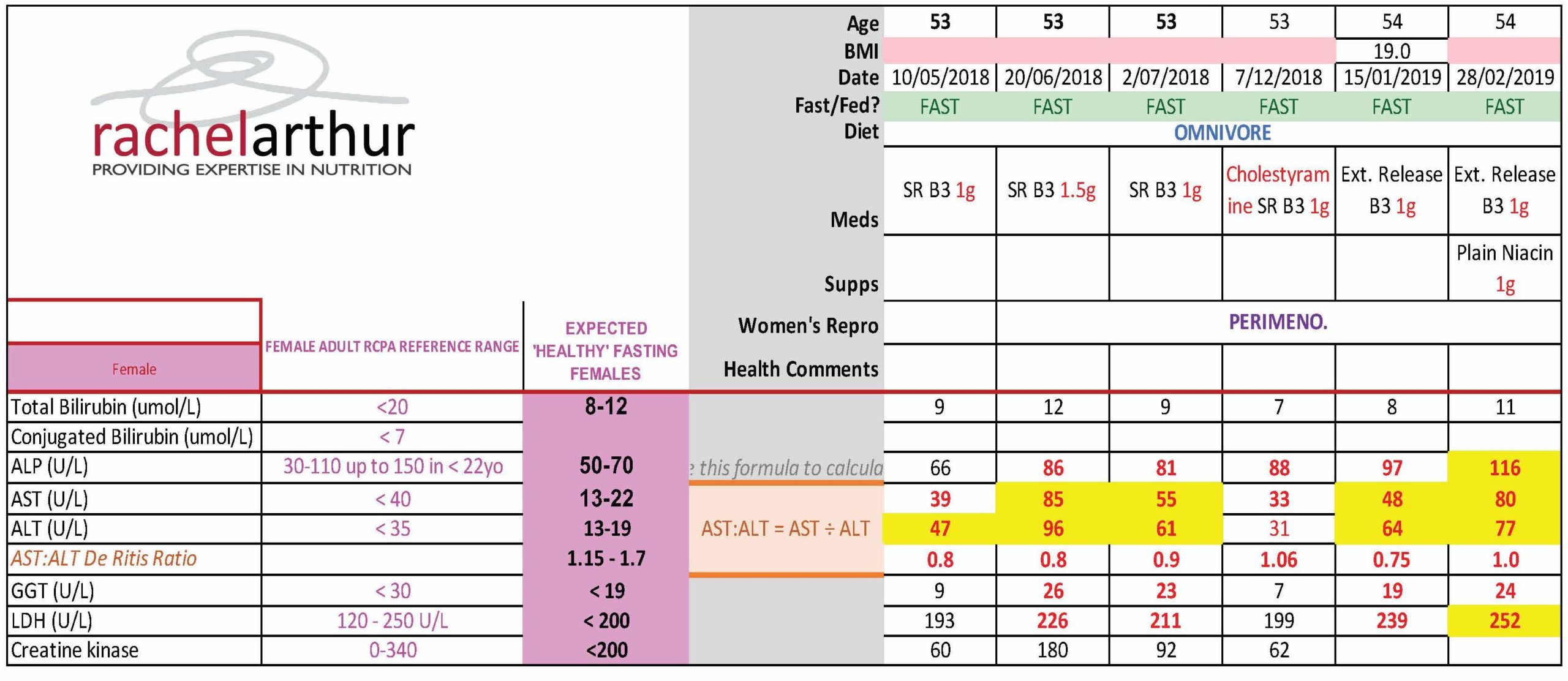
What’s your knee-jerk response to 52Y Lipids Lucy & Liver, whose ALT & AST suddenly jumped above range when she was put on statins? They’re damaging her liver? You’d be wrong. One of the practitioners who undertook the MasterCourse in Comprehensive Diagnostics just graduated with flying colours when she was able to correctly identify the true cause of this patient’s LFT abnormalities, can you?
[Cheeky hint: there is more than one explanation/process at play]
This naturopath now knows her pathology patterns. She knows the interpretation of any liver enzyme must also take into account the movement in other markers, to make meaning of the whole. Because so-called ‘liver enzymes’ are never exclusive to the liver. They are expressed in multiple other tissues and organs – sometimes at equal concentrations to their liver-level (e.g. ALP and bone). For some, even referring to them as a ‘liver enzyme’ is a mislabelling of sorts, with minimal expression in the liver itself compared with ubiquitous distribution all over the body (e.g. GGT & LDH). Of course this is both a blessing and a curse. A curse if you make the mistake of only interpreting their levels through a ‘liver lens’…a blessing if you know when they are flagging problems elsewhere through the specific pattern recognition. So back to Lucy – the statins had induced a rhabdomyolysis not hepatocellular damage. The clues? Significant AST dominance over ALT, above range CK and LDH.
So if the statins weren’t causing increased hepatocellular damage what is that increasingly high-normal ALP pattern all about?
Bones. And again, this practitioner picked it. And then got to win herself some pretty BIG credit and credibility points with all the other health professionals sharing care of this patient by suggesting that they clarify and confirm this by referring her for an ALP bone isoenzyme assay, which answers the question: is the elevated ALP originating from the liver, the intestines or from the bone? Bingo, bones it is! Or was, because this practitioner was able to alert not only the patient but all the other practitioners treating her to the increased bone remodelling taking place, independent of the statin reaction, but part of her perimenopause. Left unchecked this would escalate further of course at menopause and leave her bones in bad shape. This is just one illustration of how we can show ourselves the be the incredible one we are on the shared-care team.
Being lab literate and pathology proficient, sets you apart from the rest and enables you to practice truly preventative medicine. How else would we have known she was experiencing increased BMD loss that may be the start of something truly tragic?
Realise the true value you can extract from the most commonly performed labs. Join Rachel Arthur LIVE on the MasterCourse I: Comprehensive Diagnostics WATCH PARTY This skill is the biggest ‘game-changer’ in Integrative Medicine! Want to know more? Head over to my website here and check out more of the great benefits and bonuses of joining this program This course is a fantastic learning opportunity to identify the many intricacies in cases that have previously been missed.
Is it just me or do you view everything with a trained eye? My son always laughed when I wrote him a shopping list: I would list items under each shop and I always wrote down our local supermarket the Independent Grocers Association, like this: IgA…you all see what I was doing, right?!! It’s actually known to everyone else as IGA…well truth be told, I didn’t until he pointed it out 😂 Then there’s this relic I regularly pass, as I walk through bushy parkland near my home, ‘Hmmmmmm, B12 hey?’, I’d muse. I’d be embarrassed to tell you exactly how long it was before I realised OMG it’s not a shrine to the vitamin but an old road sign telling you…Byron 12kms!!!
I preferred my take on it to be honest, because invariably once past this, the remainder of my walk was full of scintillating B12 banter. Just internally, people, no one panic, I don’t walk the streets of this town spouting out crazy random nutritional tidbits…although, let’s face it, I would be in good company in, the Byron Bay region!
I have a deep respect for B12 – weird but true. As a result of my clinical experiences helping patients who had a previously ‘unseen need’ for this nutrient and the significant improvements that come with its replenishment. Plus the deep dive I did into the science of the different forms and their actions last year. In particular, I now have 2 families where the TCNII SNP is evident in mum and all her children. No gene testing necessary, the pattern is self-evident once you know what to look for and the clear ‘call to action’ – more B12 please! And just this month, a fresh aspect has come to my attention in regard some brand spanking new research on B12 and IBD and the microbial (im)balance of this vitamin as a pivot point for the pathophysiology. Wowza! Early days, but I think we’re headed next level on this nutrient again! And I can’t say, I’m surprised. For while I don’t think the CHOICE of the supplemental form for B12 is complex at all (hence why we need to separate the B12 from the B*S#!) I recognise it is a complex character far beyond what regular dietetics has reduced it to.
B12 is a routinely under-rated and recognised micronutrient, which is in fact in high demand by many of our patients. As nutritional research pushes back against defining adequacy as simply the prevention of the deficiency-associated disease (macrocyctic anaemia, irreversible neurological damage) we enter a new landscape of more individualised approaches where we’re better able to recognise and treat those at risk of falling below ‘optimal’. But how do we accurately identify this and then choose the ‘best’ B12 (methyl- cyano- adenosyl- hyroxo-) supplement? Does it need to be this complex? Time to sort the B12 from the B*S#!! This recording comes with a bunch of great resources including a clever clinical tool.
The average woman & her dog (& likely every other member of her household, be they furred or otherwise), can tell you that sudden changes in sex hormones can undermine, derange, psychopathise, impact her mind and mood. Hey, for me most days reverse parking is my mild super power, the envy of all, but on day 26 of my menstrual cycle, I can struggle with a ‘nose-to-kerb’! But if we are quick to attribute this to the fluctuating sex hormones produced by our ovaries, alone, we’d be making a mistake. A portion of these peripheral steroids do cross the BBB and act in our brain, so changes to these levels during any kind of transition: follicular to luteal, pregnant to post-partum, menstruating to menopausal, early adulthood to andropause, will be ‘felt’ but the sex (hormones) we have on our brains at any given time, are far more abundant, potent and complex than this, thanks to the brain’s ability to make its own.
So in fact, the amount of sex hormones active in the brain represent an intersection between peripheral and central steroidogenesis. These Neurosteroids, made ‘on site’, are as much produced in response to our mood, our neurobiology, our psychological and environmental stress, to help us navigate these, as they are the creators of mood itself.
Yes, these particular sex hormones, due to their actions in our brain, belong to that growing list of CNS celebrities: the Non-Classical Neuromodulators. Which, for the otherwise neurotransmitter-centric & obsessed among us (that’s everyone), makes mental health and illness much more complex than ‘serotonin deficiency’ or ‘glutamate excess’ and a whole lot more real. We now need to consider other entities like: ‘suboptimal LDLs’, 5 alpha reductase over or under-expression & ‘xs inhibitory tone via progesterone’.
The ‘sex on the brain’ of any patient therefore is impacted by both their Endocrine (ovaries, testes, adrenals) and Synaptocrine (neural) contributions – and these demonstrate some shared dependence (for cholesterol & healthy mitochondria etc) and independence.
We all know the depressing stats in support of the ‘ovarian withdrawal hypothesis’ and the risk to women’s mental health with each reproductive transition, and also in andropause in men, but the time has come to now deepen our understanding and to recognise we can have an imbalance of ‘sex’ on the brain – regardless of the ‘balance’ we might see in the periphery and put our thinking caps on about the options we have to address steroidogenesis either side of the blood brain barrier.
When it comes to a modern take on how sex hormones impact both the structure & function of our CNS, we need to blend the ‘old’ with the ‘new’. The ‘old’ tells us, production of sex hormones is in the gonads and action at a distant target anywhere else in the body, including our brain. And the ‘new’ is in the form of the ‘Synaptocrine’ – where production of these sex steroids is actually within neural tissue itself and their immediate actions occur close-by, in the synpase and at the post-synaptic neuronal membrane. These two contributive pathways show some shared dependence but also independence from one another and the balance of both has now been recognised to be integral to the overall health of the nervous system.
Something’s just come up today again and I think we need to talk about it. A positive result on a stool PCR microbiome test for H. pylori, understandably, might be heard as a clear call to action to go in guns blazing with an eradication approach. But is it? Trust me, I’ve had more than my fair share of battles with this bug & can understand being keen to have it be gone BUT first things first, let’s be clear about what the result speaks to.
Does it say, “Here! Look over here! Here’s the source of your patient’s GIT distress,” or even, “Here’s a pathogen that has taken up residence in their GIT and is a risk for future dx!”
No, not necessarily. It speaks to its presence.
And that may be only fleetingly, as it passes through. I’ve seen it before and so have many other experienced practitioners: a positive stool PCR that is at odds with the results of gold standard H.pylori testing, the UBT, faecal antigens or blood serology, all freely available through the GP. And the reality is, if you have a negative UBT, there’s no urease production, the trademark trouble-making of this bug. If you have negative blood serology, your immune system has never ‘met’ this bug or, in the minority of cases, you’ve tested in that brief early exposure window prior to antibody production (2wks) so you should retest within the month, to confirm or refute. And if you don’t have any faecal antigen…it ain’t in da’ house…so to speak 😅 If there’s something new here, then have a quick read of Medscape’s great work-up summary. So, clearly we need to confirm before we open fire.
We (me included) have been so single-minded about increasing the ‘sensitivity’ with our testing methods, we may have left ‘specificity’, in broader sense, behind & that creates a new problem.
This leads us and the patient down the garden path of false attribution and time and money wasted ‘treating’ a ghost gut issue. And no one wants to be put on a pylori protocol when they really didn’t need to. Trust me 🙄 But if someone does come back confirmed, well then…
For a bacteria identified just a few decades ago as being a cause of chronic gastritis, atrophic gastritis and gastric carcinoma, the escalation of number of antibiotics used to eradicate it (4 at last count + PPI) has been nothing short of breath-taking. A management approach more consistent with both integrative medicine and with an improved understanding of the delicate microbiome focuses on changing the gastric environment to ‘remove the welcome mat’. What do we know about how to do this successfully? It turns out…quite a lot.
Well, this is different, now I’m watching you! 😆 In early 2021 we released our very popular MasterCourse I: Comprehensive Diagnostics, as a ‘self-paced’ online offering for the many who missed out on attending live in 2020. Many have grabbed this opportunity with both hands (& a headset and some hardcore Do Not Disturb! signs) but we know that for some, doing the entire course on your own, >24hrs of video presentations, can be a tad onerous & overwhelming. We want to remove these barriers and empower & upskill as many practitioners in pathology interpretation as are keen, and as a means to achieve this, we’re offering the MasterCourse I Watch Party. So bring your bhujia and a beverage and let’s do this!!
Practitioners who sign up for this will be able to watch each session’s video replay live with other practitioners and have the opportunity to ask Rachel questions & participate in case discussions at the end. Another key detail is that we will run the sessions weekly, so that the full course is covered in just 6wks, from July 8th to August 12th.
MasterCourse I: Comprehensive Diagnostics LIVE WATCH PARTY 24 hours of live Zoom sessions + Bonus sessions! 8, 15, 22, 29 July & 5, 12 August on Thursday at 3.30pm to 7.30pm AEST.
Each Thursday, the video presentation for that week will be played so we can watch it together. Then Rachel will open up her webcam and mic, inviting you to do the same, to participate in a Q&A as well as set case discussions. When you register, you get immediate access to watch our preliminary/preparatory sessions, prior to 8 July: Accurate Pathology Interpretation Starts Here and the RAN Patient Pathology Manager Tutorial.
Below is an overview of the Watch Party schedule.
Week 1 – 8 July | SESSION 1: Acid Base Balance & Electrolytes
Week 2 – 15 July | SESSION 2: Renal Markers Week 3 – 22 July | SESSION 3: Liver Enzymes
Week 4 – 29 July | SESSION 4: Lipids & Glucose
Week 5 – 5 August | SESSION 5: Immune Markers
Week 6 – 12 August | SESSION 6: Haematology
“I thought my pathology skills were pretty up there until I did Rachel’s Diagnostic Masterclass course! Nothing like being knocked off my perch by a literal avalanche of new information, especially when it comes from the most commonly tests that we all use so often. The course has been a fantastic learning opportunity for me, and has since helped me pick out many intricacies in cases that have previously been missed.
The course structure was great, the level of detail was right up my alley, and the case studies were entertaining (in true RA fashion). Once again Rachel has increased my knowledge base, and help me provide way better service to my patients.” – Rohan Smith, Naturopath
Join Rachel on MasterCourse I: Comprehensive Diagnostics Watch Party and register here.
MasterCourse I is a pre-requisite to join MasterCourse II which will be delivered live in 2022.
If I could be granted 1 wish regarding all health professionals, it would be that we were all competent in reading Iron Studies. Think that’s overstating the issue? Or not a bodacious enough way to ‘spend’ my wish? I don’t. Especially when you consider the impact of GPs in this space.
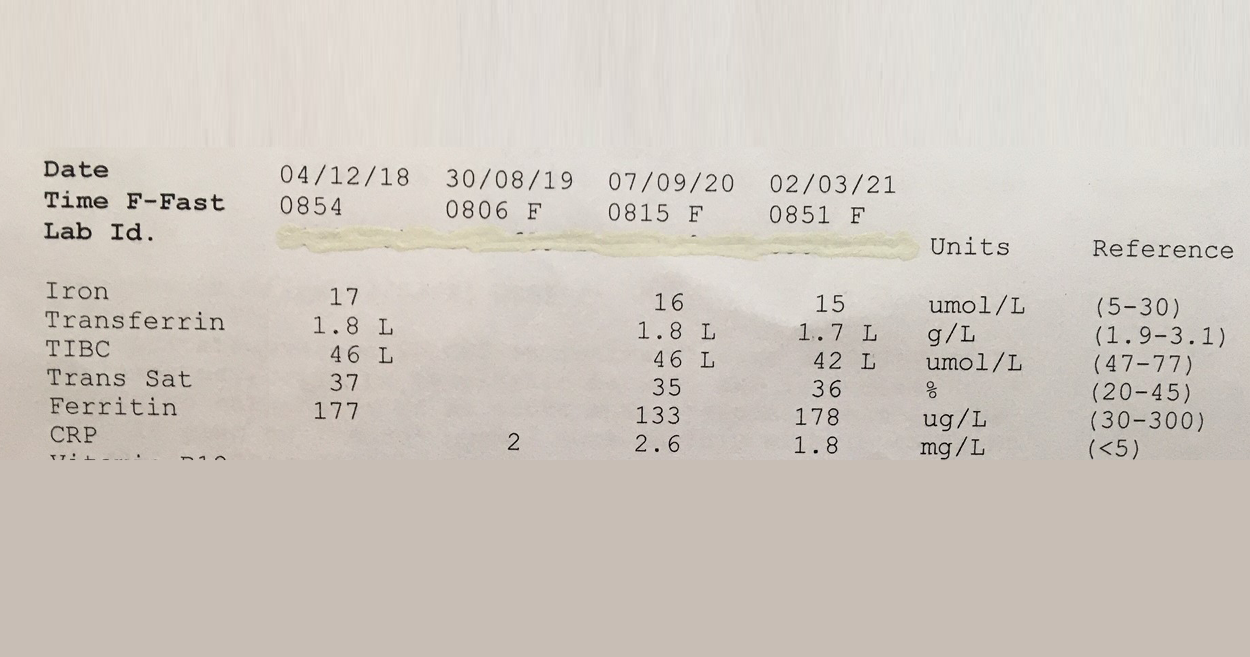
This 57Y male was asked to make a follow up appointment with his doctor, to discuss his ‘abnormal’ results which he was informed constitute Iron deficiency. Consequently he was was advised to start an iron supplement! #@!*
Your thoughts? Revoke this doctors medical licence? Insist on some very du jour ‘re-training’ at the very least? I mean, if you think this Iron pattern flags a deficiency or shortfall, then you’re as good as reading a map upside down and back to front…and written in a foreign language!! The ‘Ls’ in his latest labs flag he has suppressed transferrin, indicative of negative feedback inhibition of GIT uptake of this mineral, secondary to healthy stores or inflammation. And it’s not just that more iron is not indicated but that more iron in fact presents a patient like this with increased and unnecessary risk: to their microbiome, intestinal wall health, even according to the larger longer studies a potential correlation with colorectal cancer risk, if taken long term. Let alone the whole cardiovascular conundrum. Better still this same patient was told a few years back that he might have iron overload! Again the ‘map’ could only have been being read, upside down, back to front to reach such a conclusion!
So the one patient in just a few years by 2 different doctors has been diagnosed incorrectly with 2 different iron issues. Yep.
And sadly I have sooooo many more cases of missed and mis-diagnoses with regard to this mineral. The latest RCPA Position Statement on the Use of Iron Studies, underscores that assessment of iron status and GPs competence in knowing when to do this and how to interpret, is an important part of core general practice. Given it “is the commonest nutritional deficiency state in Australia and is significantly under-diagnosed” This succinct document offers a quick crash course in Iron nutrition for doctors and it hits all the right marks with advice about not ordering ferritin as a stand-alone because “the interactive nature of the three components allows for more accurate interpretation”and this simple but sage advice:
“Transferrin, iron transport protein, tends to increase in ID… A better strategy (than being tricked by Serum Fe) is to report transferrin saturation. A low transferrin saturation in the setting of an equivocal ferritin level is suggestive of iron deficiency. An elevated transferrin saturation is the first manifestation of iron overload.“
I mean seriously, do doctors read these RAGCP resources & recommendations, or is it just me? 🤓😂
Need a rip-roaring review on how to really read iron studies? Or know another health professional who does?!! Consider this Easter Educational Gift Instead of Eggs!! So You Think You Know How To Read Iron Studies?
Overt Iron Deficiency Anaemia or Haemochromatosis aside…do you understand the critical insights markers like transferrin and its saturation reveal about your patients iron status? Most practitioners don’t and as a result give iron when they shouldn’t and fail to sometimes when they should. This audio complete with an amazing cheat sheet for interpreting your patients Iron Study results will sharpen your skills around iron assessment, enabling you to recognise the real story of your patients’ relationship with iron.
‘Hey Alexa, What’s that formula for correcting urinary iodine for hydration status?’ Oh yes, if only she could answer these kind of questions!
There’s no one here by that name but we get these kind of emails all the time [Oh and also for Freya who hasn’t worked here in like 5 years!!😂] But we love them because it means our blogs provide useful, sought after and (we like to think!) really really hard to get anywhere else answers . But hey try it, Ask Siri! We’re always forthcoming with references – not just citations but the full low down and dirty full texts (as long as we’ve managed to get our hands on it!!) and we know which topics particularly hit a spot across our professional group by not just the number of enquiries but how far the actual blog they’re referring to, dates back. So we’ve just received more comms regarding one that’s often on high rotation…a post I wrote on urinary Iodine Assessment & how and why we should adjust for hydration! That was 2014…what a vintage 🤩 Show’s though how topical and tricky this little test is.
The iodine landscape has undergone radical change recently. We’ve moved from recognising the resurfacing of a widespread deficiency, to large-scale food fortification that has failed to correct deficiency in most and produced excesses in a few. Parallel to this, we have the ever growing incidence of thyroid disorders and some radically contrasting ideas regarding iodine’s role in both aetiology and treatment. Micrograms V milligrams? Random urinary iodine or iodine loading test? Important new evidence and clinical experience helps us understand more about how to accurately assess patients’ need for iodine and know when & how to use it therapeutically & when not to!
The first time I saw a set of lab results was when a patient brought them in to her appointment. True. In spite of the comprehensive training I’d received in nutrition and biochemistry and pathophysiology my undergraduate did not include one single lesson on lab interpretation & now here I was faced with some badly formatted inkjet printed document full of numbers I was supposed to make sense of. Was the patient right to expect me to be lab literate?
We profess to be proficient in identifying and correcting nutritional deficiencies, as much as, cardiovascular risk, chronic inflammation, methylation imbalance etc etc so surely these ‘numbers’ are essential to informing our baseline understanding of & decision making regarding the management of our patients, as well as tools for monitoring their progress & safety.
Let alone the knowledge we need to work collaboratively with other health care professionals and show ourselves to be the asset that we are.
And herein lies the golden opportunity, I believe. Most of us do possess excellent foundational knowledge in nutritional biochemistry etc, much more so than other health professionals, who are ordering and seeing these results routinely, they will often tell you this themselves. And while more recent naturopathic, nutritional & herbal medicine graduates have had some basic orientation and education in pathology, are we really making the most of this powerful marriage of knowledge areas? What would we see, if we made it our business to view the same labs?So much more.
We can see warning signs well before the diagnosis, we can see the process behind the emerging or established pathology rather than simply a disease label, and accordingly, the individualisation of our patients’ presentations and their prescriptions.
But first we need to learn our labs.
That very first patient who turned up with results in her hot little hand started me on this path to lab literacy. Later, I was lucky enough to find a kindred spirit & mentor during my time at SCU, with Dr. Tini Gruner and then Dr. Michael Hayter, whom I co-presented my first diagnostics course with many years ago, and every day my patients and my mentees’ deepen my understanding. This path to lab literacy goes on forever I suspect, but with every new corner I turn, I am reminded of and rewarded by all that it has gifted me and my patients.
I’d like to share that gift with you through stories filled with new favourite characters, like ‘Mr More More More Monocyte’ above, engaging animations, loads of real cases, heaps of humour and plenty of practice in pattern-recognition, that make remembering, what can be very detailed content, doable.
In other words: The MasterCourse in Comprehensive Diagnostics I is finally here as a self-paced learning program you can undertake yourself. We know you’ll get as much out of it as those who attended live:
“I thought my pathology skills were pretty up there until I did Rachel’s Diagnostic MasterCourse! Nothing like being knocked off my perch by a literal avalanche of new information, especially when it comes from the most commonly tests that we all use so often. The course has beena fantastic learning opportunity for me, and has since helped me pick out many intricacies in cases that have previously been missed.”
– Rohan Smith | Clinical Nutritionist
MasterCourse 1: Comprehensive Diagnostics is a self-paced online program Gives you access to 24+ hours of streamed video presentations, 2 x Bonus Update in Under 30 episodes (The Calcium Conspiracy & Using Urea to Creatinine Values for Protein Adequacy) PLUS resources, a template and pdfs of all presentations. This package includes $200 worth of bonus material and remains forever in your online account. You will also receive access to any future updates of resources and our template. More information can be found here.
This is a pre-requisite for MasterCourse II that will be delivered live in 2021.
I love a little temporal lobe tap. Especially the kind patients provide. This week mine came from a mentee’s patient who, while presenting with concerns about possible perimenopause, was found to have radical shifts in her thyroid hormones, largely thanks to a dramatic increase in TPO Abs (>1000). The patient’s other presenting complaint was ongoing gastritis (confirmed via scope) and reflux…and that’s when I started to deep-dive into the archaeological archives of my brain…with the…’didn’t I have somewhere in here, in some dark dusty deep recess…a connection between the two?!’
Aha! With the help of a torch [read Google Scholar] the temporal tap bore fruit. 1 in 4 patients with AITD (Hashimoto’s or Graves, you choose!) test positive to Parietal Cell Antibodies
I’ve created (clearly, not-so)SmartArt graphics on powerpoint slides on this exact topic, waxed lyrical about it in my thyroid training packages…but in fact needed a temporal tap to be reminded! And in turn thought, well gosh if this has slipped from my mind, it might just have slipped from yours too! ‘Thyrogastric autoimmunity’ as it’s called, refers to a patient group that exhibit antibodies to both and remember, the antibodies precede the condition in both disorders, so you can have a patient with established AITD, who has zero gastric symptoms but tests positive for the antibody…an important heads-up, as it speaks to significant risk of the subsequent development of gastritis in the following years. This excellent prospective study of AITD patients by Tozzoli and colleagues mapped exactly that! Jump forward just another day or so and…
I’m preparing for our final FiNAl FINAL Q & A on Haematology for our MasterCourse in Comprehensive Diagnostics and I’m wrestling with all the conflicting ‘facts’ about the anaemia that may present alongside hypothyroidism – it has been documented and described as being macrocytic, normocytic and even microcytic… how can it possibly be so diverse I wonder and then 💡 I’m guessing the presence or absence of these parietal cell Abs likely has something to do with it!!
Anyway, it’s getting towards the end of a VeRy loooooooooooooooooooooooooooooong year…thought we could all do with a temporal tap 😉
A few things really took up a disproportionate amount of our time & attention in 2020: Zoom, Mask Fashion & Gin based hand sanitiser.On a personal note I need to confess another: Iron. So while my one true (mineral) love remains zinc, iron answer hunting has infiltrated a lot of my days and some nights! There’s no hiding it…3 out of my 12 UU30 episodes this year have iron in the title 🙄 a sure sign its been on my and my mentees’ minds and sitting across the desk from a lot of health professionals in human form. And this affair I’ve been having, like most, started innocently… it started with a just a ‘quickie’, you know a quick question from a well meaning practitioner: “So, what’s expected in terms of ferritin levels across pregnancy?”
There are 2 answers to this. The first reflects the practice guidelines for GPs and obstetricians in most western countries: > 30 mcg/L regardless of trimester And then there’s another that is [ahem] evidence based, accounts for the essentiality of physiological anaemia in pregnancy &, naturally, trimester specific
There’s a big Fe-ar factor at play when it comes to answering the question, ‘Does this woman have enough iron for her and bub?’ Public health and practice guidelines appear to assume we are ‘guilty’ until proven innocent, patients are worried and health professionals are plagued with their own doubts about whether they’re ‘reading this right?!’ I’m sure we’ve all been in the situation where we feel our pregnant patient is doing well iron wise early in pregnancy, only for them to have that routine antenatal 28wk GP/Ob visit and discover a total panic has descended upon the patient and the rest of the health care team, with calls for ‘IV Iron STAT!’ But 28wks is the height of haemodilution right? You know, that time when ferritin, Hb and Hct should look at their lowest, right? There certainly is a limit to how low we want any pregnant woman to go – for her and her baby’s health but that limit is not the one routinely used and the truly evidenced based one is going to shock you. So what? What’s the issues if we are a little Fe-ar based about Fe, resulting in hypervigilance (calling a deficiency when there isn’t actually one) and giving them a ‘boost’ of more iron, surely this is good news ultimately for baby’s iron levels and for lactation and for…sorry what? No?
There’s a U shaped Curve for Iron supplementation & serum Ferritin levels in pregnant women?!!
It starts with a simple enough question: What should women’s ferritin levels be in pregnancy? But the answer will surprise many. There are in fact two. The first reflects the practice guidelines for GPs and obstetricians in most western countries regardless of trimester and then there’s another that is arguably more evidence based, accounts for the essentiality of physiological anaemia in pregnancy & is also, sensibly, trimester specific. To challenge the ‘noise’ and have the confidence that ‘normal’ is ‘enough’, we need to better understand the mother’s protective physiological adaptation of iron regulation and the intricate systems the foetus has to ensure its needs are met. This of course is not without limit, so we need to also be clear about the maternal serum ferritin threshold for negative impact on the foetus and newborn. Getting the balance or iron right in pregnancy for both mother and baby, is perhaps easier than we have been led to believe.
Well, obviously(!)…this has been a year heavy on pathology interpretation for me and the huge number of practitioners who’ve just spent the last 6 months taking that learning journey with me. I celebrate and congratulate them all for their commitment to their own professional development and also their investment, in what is arguably, the most potent yet overlooked set of skills of any health professional… the ability to read bloods. Basic bloods. Mainstream labs. No…but to really read them. Backed by all the scientific understanding about what these parameters actually are, how they perform and what they (dis)prove e.g. subclinical inflammation and ramped up oxidative stress – not an informed guess but mappable…right there but where no one else can apparently see it! But I digress!
Actually what I wanted to discuss was the whole erroneous notion of ‘normal’.
No, I am not speaking from the heart about my personal quirks, sense of humour or dress sense but rather the incorrect assumption that a reference range defines ‘normal’ and that our answer for each patient and each result is, a Yes or a No!
In this brilliant article by Whyte & Kelly published in the BMJ they spell out this falsehood succinctly. They note that the term ‘normal range’ has slipped into medical language from the misunderstanding that all lab results follow a Gaussian (aka bell shaped curve & later referred to as ‘normal distribution’) pattern but many simply don’t. So for some parameters a result near the ‘middle of the reference interval’ constitutes aspirational whereas for others it spells danger. Add to this, that these reference intervals are mathematically determined to reflect the expected values of 95% of your patient population (mean +/- 2 SD either side) so…that means the chance of a YES…”Your patient’s results are ABNORMAL!”… is just 5%. And hey…who said all the values within the reference range are all equally “normal” or better yet, healthy?! Not these authors, nor I, nor the praccies who’ve just done our course. So while, in many regards, these goalposts are too wide, they are also too narrow – typically only representing a subset of adults age-wise and Caucasians, yes they are both ageist and racist (yep, I said it!). And if our practitioners have learnt anything it’s about keeping an ol’ eagle eye on the sneaky intra-individual shift! Only spotted, of course, if you know your patient’s normal (not theirs compared to anyone else…just theirs) and then spot a shift. [I can hear they’re shushing 🤫me…they’ve got it already, alright!!]
So this is music 🎻to my ears, from Whyte & Kelly: “The intraindividual variation in laboratory values is usually much smaller than the interindividual variability (ie, the variation in the population). Variation in the concentration of an analyte, if significantly outside of a patient’s usual values (but still within the reference interval), could be a sign of early or latent disease”
So if you want to tap into the power of pathology…start with Whyte & Kelly, maybe even dip your pinky in the pool by checking out Accurate Pathology Results Interpretation Starts Here – an easy little 1.5hr kickstarter…or jump right in the deep end with the rest of us pathology reading polo players and sign up for the MasterCourse 1: Comprehensive Diagnostics for some DIY summer fun 🌊
ps I know your type and know that is EXACTLY the kind of weird nerdy thing you have planned for your break…you should see my summer fun list!!! 😅
MasterCourse 1: Comprehensive Diagnostics is a self-paced online program due for release in December. The course has pver 18 hours of video presentations plus 2 free bonus sessions 1) Accurate Pathology Interpretation Starts Here and 2) Patient Pathology Manager and access to resources and tools within, for your own use. This is a pre-requisite for MasterCourse II that will be delivered live in 2021.
This skillset has been found by many to be biggest ‘game-changer’ in Integrative Health You can view the full course outline here.
As a health practitioner, you are always actively building: your reputation, your practice and your knowledge.There’s theoretical …and then there’s applied. Some of the biggest leaps we take forward as practitioners come with being shown how (rather than told) & then being forced to ‘do the work’ ourselves, rather than being exposed to simply more information, be that about pathology, patient prescriptions or practice structure! The slogan ‘Just Do It!’, might have already been nabbed and TMed by a huge corporate beast, but this doesn’t undo the universal truth of it! Prefer your mantras to come from mystical philosophers rather than monster multinationals? How about this then?
I hear and I forget. I see and I remember. I do and I understand. Confucius
This mentoring community that I am a part of, we are about applied learning. We learn by doing. We learn, not just through each individual’s patient encounters but through the collective clinical experience. We make what can otherwise be an isolating experience of constantly, seemingly, reinventing the wheel, if not many wheels (!), into one of collegiality and ‘using the force’. If you haven’t experienced Group Mentoring with me previously and are thinking about next year being your year (see below to find out more about our 2021 offerings), we put together this fun little video here to get across that mentoring isn’t about a conversation between just two people.
With Group Mentoring you’ll be learning, through the application of core clinical skills, improved patient questioning, methodical information gathering, evidence based answer finding & getting access to resources that you can apply in real-time in your own practice.
“Having the group session each month, as well as having Basecamp to bounce ideas around in, is a reassuring connection to know is there if I need it. Having just started practice this year and working in an environment without other Nats around, I have noticed the occasional feeling of isolation. So having the monthly catch up keeps me feeling connected to other clinicians and gives me exposure to other cases and perspectives that I wouldn’t have otherwise had.” – Georgie
We have a range of groups on offer to suit all levels and most types of integrative health modalities. Go to our Group Mentoring page to discover the groups and bonus extras on offer for 2021.
Going by the landslide registrations for 2020, our ongoing excellent retention rate of practitioners from year to year & our already overflowing waitlist for 2021, the reputation of RAN Group Mentoring is highly regarded and a popular choice.
So, if being part of our community excites you and if the thought of learning and applying collective knowledge from expertise outside of our own, now’s the time to put your hat 🎩 in the ring, put your hand up ✋🏼 & join the conversation 📣 through Group Mentoring.
We’ve been talking all about the dangers of excess fuel in our blood recently. You know, just like nature…too much fuel underfoot creates a fire hazard. So too in the bloods of our patients. The key fuels I am referring to, of course, are lipids (triglycerides & cholesterol) and glucose. Our tissues need ready access to both but Balanced Blood Supply & Mastery of Management is key.
In terms of excesses, lipids play the long-game…wreaking havoc over a long period primarily via their vulnerability to form peroxides, which in turn create a chain of oxidative stress and depletes our antioxidant artillery.
In contrast, even outside of insulin dependent diabetes, for the rest of our patients, glucose plays a fast and furious game, being a highly reactive substance capable of causing both glycation and oxidation. We describe even high-normal levels of glucose as something akin to the ‘Bull in the China Shop’, disrupting the function of the endothelial linings and damaging a variety of plasma proteins (not just haemoglobin) that float within them. But do we have a way to routinely measure the level of damage occurring in our non-diabetic but somewhat glucose intolerant patients? Sure! Just check the C-CCTV footage!
The extra C stands for ‘Carb’ and yes we can potentially check the Carb-Closed-Circuit-TV ‘tape’ in every patient.
It’s called HbA1c and measuring this provides us with an opportunity to review their personal ‘tape’ of the last 2-3 months for evidence of excesses.
Helpful, hey. But we actually have so many great tools through regular routine labs at our disposal to understand the glucose disposal or dys-disposal(!) at play in our patients! You’ve just got to know where to look (urate, triglycerides, insulin, HOMA-IR etc) and what each piece of information is telling you. We’ve had SO MUCH FUN with this particular topic in the MasterCourse this month…or is that just me 🙄 No, I know it was, because our live session chatbox was full of ‘blown brain emojis’!! 🤯🤯🤯 I can’t wait to share this course content far and wide at the end of year with those of you that missed out on attending live.
In the meantime if you want to learn more about glycation which is the new inflammation, out there in research-land, you know…the source of all evil including ageing itself(!!) then check this out…
Glycation is a normal physiological process that, just like inflammation and oxidative stress, can get out of hand, contributing to disease processes. Currently there is an explosion of correlational research suggesting relationships between higher levels of Advanced Glycation End-products (AGE) in individuals who have fertility problems, psychiatric conditions, osteoporosis, premature skin ageing, cancer…you name it! New research implicates diet heavily in the determination of individual’s levels of AGE but there is devil in the detail – there are ‘4 Ps’ of dietary AGE contribution that we need to be mindful of when we are giving dietary advice and trying to move patients towards wellness. This Update in Under 30 recording: Are You Feeling Your ‘AGE’ will open the lid on the ‘new black’ in chronic health & ageing.
My how the time just flies when you’re chasing answers from private pathology companies! As Brisbane based naturopath, Sandi Cooper, can attest to having recently been down the seemingly eternal email trail with a pathology company trying to ascertain if their urinary iodine result accounts for the concentration of the urine sample (via the iodine:creatinine) or doesn’t….because of course it can make the world 🌎 of difference. Like clarifying that someone who appears to have very little iodine in their urine, actually has a lot or vice versa! I wrote about this back when I was a mere ‘babe blogger’, more than 5 years ago. After recently reading this historical document, Sandi has been practising due diligence and checking with her providers whether they have already corrected for creatinine..or whether she needs to herself and she shared that multi-departmental epic email endurance event thread with me. The short answer? They used to and now they don’t. Why? Oh…formatting issues or something 🙄
But just in case you do want the ‘short answer’ regarding your particular pathology provider…without emailing enigmas…the answer is, in fact, in front of you & it’s Super Short!
mcg/g Vsmcg/L
If your patient’s urinary iodine result (random or 24hr) is reported using the units on the left, sometimes actually written mcg/grCR, then BiNGo! The pathology provider has done the creatinine correction for you. If they only report the urinary iodine results using the units on the right…it’s time for some maths to avoid misinterpretation. No one panic, the formula is easy: Iodine (mcg) ÷ Creatinine (mmol) X 8.85 = Corrected Iodine. So don’t lose time sending endless emails like poor Sandy or placing countless calls, like poor Nina on my team…who has to pursue pathology providers on an almost daily basis for answers to our zillions of sensible questions!! Just check the units! You’re welcome everyone 😉 oh thank you Sandi for chasing this again and sorry about needing to chase this again! 😳
And if all of this is nEWs to yOU, you might want to review what you thought you knew, about Comprehensive Thyroid Assessment too!
We can never rest when it comes to learning more about the individual nuances of our patients thyroid pictures! In this 90min recording, Rachel covers the key thyroid parameters both functional & autoimmune (TSH, T4, T3, rT3, TPO, TgAbs, TRAB). As well as the most accurate methods of assessing relevant thyroid nutrients: iodine & selenium & a genuinely game-changing insight on interpretation of these . Finally she pulls all the individual parameters together to illustrate common patterns of thyroid imbalance – making it almost as easy 1-2-3! Well, hey..it’s the thyroid…a fickle fellow.