Remember the days when we had the brain all back-to-front & upside down? Anatomy & physiology told us it was an island, completely protected by the blood-brain-barrier from pathology in the rest of the body, that it was incapable of regeneration after damage and that it didn’t have its own lymphatic system. All wrong. Which presents a problem, the CNS is absolutely in trouble if other parts of our body are (!), but also some solutions: plasticity and the brain’s own capacity for cleaning up after itself. New research has revealed more about this critical CNS cleansing and what is likely to get in the way of this
The latest Medscape update on this is quite poetic, speaking to the movement of body fluids like tides within the human body.
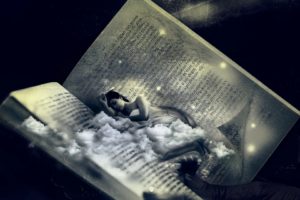
“They found that the blood flow to the brain diminishes, allowing for an influx of cerebrospinal fluid (CSF), washing away the day’s detritus of proteins and other waste substances that might harm the brain if they aren’t cleared out.”
But these particular tide times are restricted to sleep – having never been identified during awake states & even more specifically only during our Deep Sleep, the period of slowest brainwave activity. The speculation is, of course, given sleep issues predate or are a feature of neurological and mental health conditions, that perhaps this comes back to the impeded process of waste removal that accompanies this and how this may contribute to accelerated negative neurological change. For example, beta-amyloid proteins are well known to be removed most rapidly during our sleep and this week I’ve been faced with a small mob of patients who have substantial cognitive impairment risk from a genetic standpoint (e.g. Apo E 4 carriers in families riddled with dementia) but their unmanaged long-standing insomnia plus or minus OSA is likely just AS risky. So here we are again back at one of the key non-negotiables for health: Sleep.
I often say to my patients, ‘There is nothing I can give you in a bottle or a blend than can do one 100th of what healthy (quantity & quality) sleep can do for your wellbeing today or for preventing health issues for you in the future’
And then I say it out loud again when no one else is around just to ensure we’re all aware of that 😉
The brain is no longer considered an immunoprivileged organ separated from immune cells by the blood-brain barrier, with research revealing numerous interactions between the neurological and immune systems. A large body of evidence now shows that these interactions, in particular an imbalance in pro-oxidant & antioxidant systems, play a clinically relevant role in the mental health issues of our patients and may go some way to explain why patients with chronic inflammation frequently present with mood and cognitive issues. Identifying and addressing the source of the inflammation (musculoskeletal, gastrointestinal etc.) therefore potentially addresses the underpinning cause and creates a ‘win-win’ scenario for patients. This updated recording aptly named: The Inflamed Brain, covers all this and more!
Assessing Adrenals can be hit and miss, especially given that even more so than other labs, timing is everything. That’s why endocrinologists typically won’t look at anything less than a 24hr urine collection. If the total output is deemed to be high = Cushing’s and if it’s low = Addison’s. Sounds simple right? But to say only values outside of this reference range flag a problem might just be a case of throwing the baby out with the bathwater (or urine in this case!). Especially given it has been established that humans frequently fail at correct & complete 24hr urine collection! Alternatively we can use saliva or blood assays and capture the cortisol at any given time point, comparing that to expectations based on diurnal rhythm – but again, how are the reference ranges for these ascertained and is there such as thing as low normal. high normal results for cortisol, that actually warrant follow up investigation? I’m so glad you asked.
I see a number of patients who present with possible indications of flagging adrenals: from some distinguishing, but far from definitive features, in the clinical picture, to secondary lab markers. However, when they ‘limp’ over the line with their morning blood cortisol result I am often left talking to myself in an echo chamber about the need for more follow up.
But with the RCPA a.m. reference range of 200-650 nmol/L (Some seriously wide goalposts!) and some labs even going down to 150 with their minimum acceptable level for morning cortisol…are we right to still flag hypocortisolism (for any reason) as a differential in patients with low normal results?
Well Medscape yet again delivered Christmas 🤶 early last week with the largest study to date of blood cortisol, that has narrowed what’s ‘normal’ significantly…at least in terms of how low you can go before warranting further investigation. In this study they tested blood cortisol in the morning and afternoon, in over 1200 individuals presenting at an endocrinology clinic to determine in real world terms how low is too low (and associated with an increased likelihood of genuine adrenal insufficiency). They then gave this new ‘minimum cortisol’ a bit of test-run in 2 other large cohorts of patients to check it really did work as an effective cut off and wham bang…we now have a fully validated bare minimum… and guess what…it’s 275 nmol/L in the morning and 250 nmol/L in the afternoon!
Let’s be clear, their cut-off has what’s called a low ‘positive predictive value’ – which means most people (approx 2/3) with cortisol under this cut-off, upon further investigation (typically the ACTH stimulation test) will be found to be fine. BUT the point of this study was to ensure we don’t miss patients with adrenal problems just because they have ‘within range’ cortisol…and this new cut-off delivers on that.
This is big helpful news actually. Previously with patients who had am cortisol between 150- 275 we tended to find ourselves in ‘no man’s land’ – unable to provide enough of an argument about why adrenal insufficiency should still be on the differential list but unable to abandon that suspicion entirely. Thanks Medscape! Now if all the labs, RCPA and the referring physicians can just read this study and shift their goal posts…🙄
Our Group Mentoring 2020 Doors are just…about…to…close!
TODAY!
So if you love labs (or want to learn to love them more), desire to be a better diagnostic detective than you already are and want truly independent mentoring in a collegiate and structured environment for next year and you haven’t applied yet…best shove your foot to hold that door open right now! We offer a range of different levels & types of special interest groups: from New Graduates & the Mental Health Primer group (for those wanting to upskill and focus on this area), from rotating case presentations in our regular groups which are a mix of funky similarly skilled clinicians, to our pure GP group…take our pick! But get in quick by emailing us right this very second: [email protected]
This week’s wonder-full paper and light-bulb discovery was prompted by a 34 year old woman with a history of Depo Provera injections over several years to control unruly menstrual bleeding and pain. She was subsequently diagnosed at 28 with osteoporosis. That’s not a mispelling…not -penia, -porosis. Now I may be a bit slower than some on the ol’ synthetic hormone fallout front but when it was pointed out that this is a known possible side effect of this synthetic progestin (even features in the consumer brochure), which is used for a range of indications in both pre and post-menopausal women, I did a double-take. What kind of progesterone replacement impacts your bone health negatively and how? And therein the real trouble started.
So fixated are we (myself included) on the evils of oestrogen, I think we’ve failed to notice the wolf in sheep’s clothing that can be synthetic progestins for some patients. Not just in general terms of concern regarding all synthetic hormones but as a result specifically of their interaction with glucocorticoid receptors (GR). This excellent paper reviews this aspect of the 2 most commonly used ones: medroxyprogesterone acetate (MPA) and norethisterone enanthate.
The bottom-line? MPA (which is Depo provera) is a significant GR agonist. That means it’s behaving like cortisol producing a degree of immune suppression and constituting yet another mechanism, in addition to the low oestrogen state it induces, by which negative bone effects may be mediated. This is not a mild or minor action according to this and other research. This is likely to have significant implications for some women, including this 34 year old female. Some women see reversal of this demineralisation following cessation, but not all and the younger your first exposure, the higher the likelihood it won’t correct. This woman had other osteoporotic risk factors, sure, but never enough on their own to produce such severity so young. Mind. Blown.🎆 Or is that just me?
While none of us are likely to be advocating for replacement sex hormones without very careful consideration, this has really helped me to change channels off my oestrogen obsession and become alert to the potential for broader effects from synthetic progestins. MPA…you’re firmly on my radar now in a whole new way.
As always, our patients teach us the most and thanks to Amanda Mullemeister for bringing hers to our recent mentoring session. The learning is never one-directional and I am so privileged to share in these discoveries with all of my mentees, every week. I just wanted to share some light from this particular light-bulb 💡
If you’ve heard Rachel speak ever (!) you probably know she’s on a mission to stop the late diagnosis of osteoporosis in patients and as part of this reminds us that this is a condition that develops over a lifetime not overnight – so waiting until women are 65yrs and men are 70yrs (which is the standard recommended age for BMD screening) seems a little remiss in terms of identifying our opportunity for preventative medicine. Are there earlier warning signs that we are ignoring or specific tests more sensitive and accessible than DXA scans that we could be ordering to better monitor patients who are at higher risk of bone demineralisation? The answers are of course, yes and yes! This Update in Under 30 outlines the clinical tools we should be using to uncover unhealthy bones earlier in our patients, how to implement them, their limitations and their strengths.
Stop press. No, seriously. This new research warrants the attention of every practitioner working with children & teenagers. In the largest paediatric study of its kind to date, which included 2,480 children aged 10-18yrs diagnosed with hyperthyroidism (Grave’s or otherwise), Zader & colleagues found
Double the rate of ADHD diagnoses
5 times the rate of Bipolar diagnoses (almost 7 times in males)
5 times the rate of suicidality
That’s what I said: in 10-18 year olds
What is most alarming of course is that these mental health diagnoses were made in half of these children >3 months prior to the diagnosis of hyperthyroidism. What does this mean? It means we are missing this critical biological driver in this patient group. We all recognise the potential for some psychological presentations people affected with thyroid conditions, however, perhaps we are more alert to this in adults and letting it slip off our radar in kids? There’s been renewed talk about the over- and mis-diagnosing of ADHD lately and given that research has found up to 80% of hyperthyroid children meet ADHD diagnostic criteria this is one of the 1st place arguably to look! It also means, as these researchers discuss in detail, these kids are being medicated with psychiatric meds that in fact may, at the least mask their abnormal thyroid, lead to the incorrect diagnosis of hypothyroidism (lithium & even stimulants for example) or exacerbate their hyperthyroidism (quetiapine). But wait there’s more and it’s essential to understand.
Zadar & colleagues note that while we can not be 100% clear about the direction of the relationship…e.g. were these children already at risk psychologically and the hyperthyroidism just exacerbated that, they note that correction of the TFTs does not always equate to ‘cure’ of the mental health issues. This is not entirely surprising of course. What the problem emerges via a combination of biology and psychology & we resolve or remedy the biology…guess what you have left? PLUS the learned behaviours etc from suffering from anxiety, impaired cognition, suicidality they’ve been battling at the hands of excess T3 and a subsequent tsunami of reactive oxygen species.
This is one of those papers we should all have to read top to toe and therefore ideally be able to access for free but alas 🙁 What you can read is the Medscape review of this, which is a reasonable summary but the full paper is worth it if you can. You know the other key take home here…the diagnosis of hyperthyroidism was only made with overt out of range TFTs… which begs the question what about all those subclinical hyperthyroid cases we know exist? Yes, no wonder this paper has RACHEL’ S FAVOURITE written all over it…paediatric thyroid assessment and missed biological drivers of mental health and the opportunity to get better at both…can my research reading get any better this week?!🤓
Currently in Australia there is limited use of age specific reference ranges for thyroid parameters in children & teenagers yet they are essential for correct interpretation and diagnosis. Even doctors & specialists seem to be at a loss with diagnosing thyroid problems in kids unless they are extreme presentations. Subclinical thyroid presentations, however, are increasing in both children and adults. Many practitioners competent in adult thyroid identification & management are less familiar and confident with knowing when why and how to test in this population. Make sure you’re not missing thyroid imbalance in your paediatric patients…early detection makes treatment easy.
Remember when I said you say tomatoes… equal histamine but I say, well maybe oxalates, maybe Nickel? So in the UU30 released just last week How Noxious is Nickel we get down and dirtily detailed with just why Nickel, which is almost ubiquitous in soils and therefore the food and water we consume, may prove to be a catalyst for change in the digestive systems of our patients and beyond. While we humans don’t have any actual use for this metal, many bacteria do and this means in a Nickel rich diet or environment, some will thrive and others struggle, potentially creating unrest in our very own microbiotic megacity.
It’s bigger & broader than this though, with Ni triggered contact allergies not just possible on the skin like we commonly see for some individuals with cheap jewellery. The gastrointestinal lining may also manifest a similar reaction. Yes, you heard me right.
What would this look like? Well, a patient who ‘reacts to’ tomatoes, legumes, nuts maybe and given the chance (!) chocolate cake with icing especially, which happens to be highest containing Ni food documented 👀 Someone who has been given an IBS label, or has even been diagnosed with gastritis. Still a non-believer? Check out these papers to get you started. The labyrinth of potential food reactions makes us dizzy yet again! We seriously need a map and compass to find our way through this with patients!
While nickel sits rather benignly among its mineral mates in the transition metals of the periodic table, it is a metal that humans are constantly exposed to yet have no need for. What could possibly go wrong? Well, a lot it seems. Nickel is the most prevalent metal allergen worldwide and beyond this, there is strong evidence of its potential to trigger autoimmunity, major endocrine pathology and a raft of GIT problems that masquerade as other conditions like IBS & NCGS. This episode captures the dance we all do with the ‘Devil’s Copper’ and why some of our patients are likely to end up with a bigger dose and a much bigger disease picture as a result of noxious nickel.
For all Update in Under 30 Subscribers, it’s now available in your online account and if you are not a subscriber you can purchase this individually here.
Kupfernickel. It’s the original German name for Nickel and it literally translates to ‘Copper Nickel’ which inferred it to be the ‘Copper Nickel’ aka ‘Devil’s Copper’…because each metal can masquerade and be mistaken for the other! There’s an interesting story behind this of course and lo and behold the explanation (as is often the case with minerals and metals) is revealed by looking at where Nickel sits in the periodic table. Haven’t heard me rave on before about how all the key nutritional relationships are illustrated in that cornerstone of chemistry?? Where have you been?! Nickel is a transition metal and that tells us many things – including that its key relationships and interactions are likely to be with Iron, Cobalt, Zinc and Copper. And guess what? It’s all true. Still, I’ve had another Nickel-centric chemistry lesson of late because I actually had not the slightest appreciation of how noxious this can make it for us humans.
It started with one patient then, as is always the way, I’ve had about 3 in the past few months: predominantly women, some with ‘known’ nickel allergies, in the form of jewellery-related dermatitis and sometimes not, many with significant gut disturbance (IBS like, non-infectious gastritis) and most with early or advanced autoimmunity.
And the vast amount of scientific literature on the prevalence of Ni allergy (conservative figures suggest 15% population with a very high female:male) and its capacity to go beyond the ‘cosmetic’ and trigger gross immunological aberrations in Th1 cells, well, the case for Noxious Nickel is one of those things that once you see it, you can’t ‘unsee’, ever. Think if you or your patients have never had an issue with wearing cheap jewellery we can rule this one out? Think again. While the jewellery reaction might be the helpful clue in some patients, there are also 3 other ways that the old Kupfernickel may be undermining your health. And yes! The fact that contact dermatitis to nickel-containing silver jewellery is such a common issue tells us straight up, that its absorbed via our skin, think: watches, mobile phones, e-cigarettes, hair clips, and…yes I am having another crack at these again…tattoos! We also inhale and consume it via a wide variety of food and drink we consume. Oh and did I mention dental interventions, yet? 👀 Sheesh….
So while we all accept humans have zero requirement for Nickel, it’s in us all the time and the question is (always) how each individual inner chemistry lab (!) is interacting with it and to what extent this may explain some pretty potent health problems, from GIT disturbance to Hashimotos and from skin conditions and alopecia to CFS & Fibromyalgia-like conditions.
My latest Update in Under 30: How Noxious is Nickel – highlights the fundamentals of Nickel in terms of our sources of exposure and who is most susceptible and just how this can play out as a driver of disease. Next month we move onto our testing options, drilling down into the myriad signs & symptoms and how to effectively manage the patient dancing with the Devil’s Copper. This one has been a real ‘sleeper’ for me, but it’s time to wake the beast for us all 👀
While nickel sits benignly among its mineral mates in the transition metals of the periodic table, it is a metal that humans are constantly exposed to yet have no need for. What could possibly go wrong? Well, a lot it seems. Nickel is the most prevalent metal allergen worldwide and beyond this there is strong evidence of its potential to trigger autoimmunity, major endocrine pathology and a raft of GIT problems that masquerade as other conditions like IBS & NCGS. This episode captures the dance we all do with the ‘Devil’s Copper’ and why some of our patients are likely to end up with a bigger dose and a much bigger disease picture as a result of noxious nickel.
Hear all about it by listening to my latest Update in Under 30:
For all Update in Under 30 Subscribers, it’s now available in your online account and if you are not a subscriber you can purchase this individually here.
There I said it. It was always going to happen. I’m ok, thanks for asking. This week we had a case of a woman diagnosed with MS in her late 20s. That was 5 years ago and she’s been medicated ever since with an immunosuppressant and she is understandably very nervous about taking any complementary medicine that would pull against this medication, interfering with its actions. Her concerns extended to zinc supplementation in spite of her plasma zinc being 7 umol/L. That’s right, 7. Zinc STAT, right? But slow up there everyone, her apprehension is not necessarily unfounded.
The top nutritional research topics in MS are: Vitamin D (for der…we all knew that, right?), Vitamin A and Zinc. The fan-mail for the first two, as key immuno-modulators in both prevention and in established conditions, is almost at stalker level.
In contrast Zinc attracts both fan and hate mail.
Although the jury is far from in, there’s growing concern that while extracellular levels of Zinc may appear low in MS (that includes of course plasma/serum values) the same individual may actually have elevated levels inside their cells and more specifically inside their CNS.Gulp. But wait there’s more. There is a hypothesis that Zinc dysregulation may be a pathophysiological driver in MS. Double Gulp. My (nutritional) soul mate has shown a potential dark side finally and is sitting under a cloud of suspicion. So what do we need to do differently?
If you’re seeing MS patients you need to be up on the sizeable pile of research into CM in this condition. A brilliant place to start is this very readable review of ‘Vitamins in MS’.
And specifically in regard to Zinc status in your MS patients? Well my advice is don’t rely on a plasma/serum Zinc alone – but couple this with an rbc Zn to ensure there is no sign of intracellular accumulation at play before you make a decision about treatment. Not a perfect solution, but while we’re unlikely outside of research to ever be able to measure CNS zinc concentrations, a reasonable approach. An unchecked zinc deficiency is in no-one’s interests either, including your MS patients – so it’s about gathering the best quality information you can to walk that fine line of adequacy not excess. And if you’re still reeling at the very thought that Zinc has a dark side – remember I did warn you…in Mastering Micronutrients – which is essentially a series of truth-bombs one of which, is every nutrient has a sting in its tail, a U-shaped dose response and a dark side. We need to get to know them all.
Let’s make sense of the over-arching nutrition principles, that will profoundly change your understanding and application of this modality Truly understanding the ‘big’ concepts, so often overlooked, or incorrectly taught, ensures you get the critical ‘small’ detail in your nutritional prescriptions right. In this 4 hour recording, together with key clinical tools, we talk about the tough stuff: dose-response curves, active versus passive stores and excretory pathways and ooh lah lah…the myth of taking ‘activated vitamins’. Even those who feel satisfied with their original training – will find a lot in this critical review that is new, insightful and truly practise-changing!
Tonic. Homeostatic modulator. These terms and concepts, which have a long tradition in herbal medicine (and let’s be clear, were considered yet another example of the wishy-washiness of the modality) are being appropriated by some areas of mainstream medicine right now. Cheer up ‘leaky gut’, you’re no longer alone! And arguably misappropriated by the public’s very ‘lay’ interpretation of the science on medicinal cannabis and its subsequent elevation to panacea, of late.
“So many of my patients are telling me they’re taking Cannabis now, just as a tonic”, says yet another practitioner to me recently, “No, not for pain, they’re young and fit but they take it because it’s a homeostatic regulator!!”
Oh lordy…
The capacity to maintain homeostasis, and particularly in the face of adversity or imbalance, is a sign of the vitality of the individual, according to what I remember from naturopathic philosophy (and have truly taken on and observed firsthand)…so just back up there a tad and explain to me how this one herb proposes to do this for everyone on a one-size-fits-all-fashion? As confessed in an earlier communication, I am a cannabis convert. But only in the sense of appreciating the niche areas where it is likely to offer true therapeutic benefits. I still have the words of warning from the brilliant Professor Michael Lintzeris, the Director of the Drug & Alcohol Services, South East Sydney Local Health District; Conjoint Professor, Division of Addiction Medicine etc., ringing in my ears, pleading with health practitioners to not ‘fall’ for cannabis in the way we have previously ‘fallen’ (so far and landed so badly) for the panaceas of the past: opiates and benzodiazepines. Most notable major omission for me, in an otherwise rigorous scientific debate of late, is any discussion about its potential for impacting fertility.
There is in fact evidence to suggest ‘sperm under the influence’…’lose their way’ and are less effective at finding and fertilising the egg. Sorry but the image always makes me chuckle…stoned sperm. ‘Hey, dude where’s my egg?!’ style. But it’s not funny when impaired fertility is a problem affecting so many these days, and we still are guilty of over-focusing on ‘her’ and under-assessing ‘him’…and lo and behold it could be his chronic cannabis use to blame. We had a case recently, years of unprotected sex, daily cannabis, no baby, no dots connected. We may think this is a handy incidental contraceptive for young men sitting on couches with cones (one mum recently said as much to me) but for the rest…?
As practitioners we should know as much about investigating and treating male hormone imbalances as we do female ones, yet this is often not the case. While we are increasingly aware of everyone’s exposure to lifestyle & environmental endocrine disruptors and the fragility of the HPO axis, we sometimes fail to recognise that the reproductive health of our male patients is equally under threat. This is clearly demonstrated by generally diminishing levels of testosterone amongst men and increasingly early onset of andropause. These issues then become barriers to achieving success in other health areas with your clients, mood, metabolism, fertility and beyond. Learn more here
I’d love to continue this conversation with you… so join me and be part of my ongoing dialog on this and my other blogs by following my Facebook page.
Following an important weekend of discussing mental health from a more balanced perspective (that’s my new less provocative term for ‘integrative’ or dare I even mumble…holistic) in Perth for ACNEM, I remain alert but not alarmed of how much is still to be revealed in this area. Recently, for example, in our mental health dedicated mentoring group, we discussed a case of a somewhat atypical schizophrenia presentation in a middle-age female migrant. Fortunately, I co-chair these sessions with an incredible clinical psychologist who was quick to pick up that no CNS auto-antibodies had been tested, and given the peculiarities of the case they should have. This is a relatively new area, in terms of more mainstream acceptance of this as a differential in some psychiatric presentations and provision of these tests now through mainstream labs, but it would appear it is far from common knowledge. Then I read this brilliant article and…well I think we all need to read it. Here are some snippets…
“Scientists had previously noted that certain autoimmune diseases, such as lupus, were associated with psychosis. And they’d begun to suspect that some infections might, by activating the immune system, contribute to psychiatric conditions. But Dalmau provided meticulous proof that the immune system could attack the brain. The development of a test for the disorder, and the fact that very sick patients could recover with treatment, prompted a wave of interest in autoimmune conditions of the central nervous system. In total, scientists have identified about two dozen others—including dementia-like conditions, epilepsies, and a Parkinson’s-like “stiff person” syndrome—and many experts suspect that more exist…
Robert Yolken, a scientist at Johns Hopkins University, estimates that about one-third of schizophrenics show signs of immune activation (though he adds that this could be related to other factors, such as smoking and obesity). And autoimmune diseases are more common among schizophrenics and their immediate families than among the general population, which could hint at a shared genetic vulnerability.”
There are some potent practical take-homes in this article embedded especially within the story of an 11-year-old boy who was admitted to hospital with profound psychiatric features – initially misdiagnosed and managed as BPAD and later found to have autoimmune encephalitis. First and foremost: psychiatric conditions develop gradually. When there is an acute onset in the absence of an acute trauma – the possibility of a biological (esp autoimmune) driver should be elevated in your differentials. And the mother of this boy, now aged 21 and having undergone 5 relapses and recoveries in between, virtually echoes the thoughts and findings of Carl Pfeiffer half a century ago, when she says, “Too often, psychosis is seen as the disease itself but psychosis is like a fever, it’s a symptom of a lot of different illnesses.” Important for thought.
Could dairy intake in susceptible individuals be a risk promoter for mental health problems? In addition to evidence of the exorphin derivatives from certain caseins interacting with our endogenous opiate system discussed in part 1, we now look at the evidence in support of other milk madness mechanisms. Specifically, the IgG and IgA antibodies about what this tells us about the patient sitting in front of us about their gut generally and about their mental health risks, specifically. The literature in this area dates back to the 1970s but the findings of more recent and more rigorous research are compelling. Find out more here.
I was at the Medicinal Cannabis (MC) in Mental Health Conference run by GHI on the weekend and I have to confess, I inhaled. Seriously, deeply, inhaled. Just as I had hoped, this was a very high level of information on this important topic, delivered by outstanding presenters: from authorised Australian MC prescribers, to the head American researcher of the largest MC trial to be run in psychiatry – from brilliant pharmacognosists whose every day is spent immersed in complex cannabis chemistry to our very own national (naturopathic) treasure, Justin Sinclair. I left there with thousands of words typed into my laptop, and about a thousand more in my brain, spilling out onto anyone who stood still long enough. Ahem…thank you my dear tolerant family & friends 😉
Let’s be clear. I am not in a position to prescribe medicinal cannabis. Nor do I want to, right now. But like me, patient purchases off the green market in response to DIY diagnosis and prescribing are on the up and up. I have felt concern and apprehension about this but not known enough to engage in any conversation. Now, watch out… I’m finding my words!
I left the conference with a much clearer sense of the patients and presentations for whom it may prove medicinal – most obviously for those conditions outlined in the WHO review including nausea and vomiting in cancer and pain refractory to other analgesics. In addition to this, we were privileged to hear from a mum and son who have had to employ cannabis for the last half a dozen years following his diagnosis of an inoperable brain tumour, that originally robbed him of his literacy, his joy of reading and his overall quality of life, with high frequency seizures and intractable vomiting etc. MC has remarkably given much of this back to him. And I remain optimistic about future potential uses in psychiatry – especially within certain PTSD cohorts thanks to this small but promising study by Greer et al in 2014. Inspired by this paper and her extensive experience treating war veterans with PTSD, Dr. Sue Sisley, who spoke at the conference, executed a similar study of 6000 veterans for a MC inhalation trial. I’ve got a spoiler for you…the study failed – publication pending.
But before you add 1 + 1 and get 3.879…let me tell you, there is nothing as powerful and revealing as hearing researchers talk firsthand about their trials. When Sue put up actual photos of the medicinal cannabis they were supplied with for this study…the room collectively let out a giant Gasp!
It was brown, full of stem and…wait for it…mould. Yup. But that is what they, and as Sue poignantly pointed out, & what every other group of American researchers who run studies on MC as opposed to synthetics or extracts, have to use. So…are any negative outcome a surprise? No. But it will no doubt be interpreted as a sign that we shouldn’t pursue research in the area of MC and PTSD. We should. Have I completely ditched my concerns about negative mental health impact from cannabis? Absolutely not. And Professor Michael Lintzeris, the Director of the Drug & Alcohol Services South East Sydney Local Health District; Conjoint Professor, Division of Addiction Medicine etc., spoke eloquently & comprehensively to this inherent duality of this herb in this regard. Even the most isolated and lauded (non-intoxicating) constituent of cannabis can be both help and hindrance to anxiety and depression sufferers and most clearly, Michael warned us not to make MC the opiates and benzodiazepine panacea promises of the past, buying the rhetoric of ‘no tolerance, no dependence, no risk’. How each individual’s mood and mental state responds to MC, whole plant, extracts or isolated constituents, from anxiogenic to anxiolytic and from depressant to antidepressant, has been clearly demonstrated to differ according to genes, ‘endocannabinoid tone’, route of administration and dose. Seems like all roads lead to an individualised health care approach & prescription…yet again 😉
Need a road map to think your way through the integrative work-up of your Mental Health patients?
In Mastering Mental health: New Assessments & Management Resources in your Clinic, Rachel introduces you to new clinical tools that she has been developing to help us all better master the maze of mental health. With so many possible biological drivers: from methylation to inflammation and from gonads to gut, these tools can help you quickly identify those most relevant to each patient and also outline the strategies necessary for redressing these. This presentation comes with an extensive library of resources including pdf of Assessments Tools and Case Study Notes.
Show me a nutrient that doesn’t demonstrate a U shaped curve with our health (too little produces negative effects – too much produces negative effects) and I’ll go ‘HE!’ Go on…try it now… But the way many have been taught nutrition has lead to some erroneous thinking, it would seem, about the inherent ‘safety’ of all micronutrient prescriptions. To know these vitamins and minerals well is to respect their potency in every sense – from their incredibly positive application at both physiological doses, correcting deficiencies, and in a small number of scenarios almost pharmacological benefits, when used at doses that are intended to exceed the natural physiological state (think IV vitamin C, or high dose B3 for lipid-lowering as two famous examples), to their potential for fallout when healthy levels are unwittingly exceeded, especially long-term.
Our risks of over-supplying individual micronutrients have arguably been amplified by the industry’s increasing promotion of nutritional formulas or complexes over the use of single nutrients. How often do you go through and studiously add up all your cumulative totals for individual nutrients for each prescription?
Especially those that tend to find their way into such a large number of formulas and have clear upper limits, such as Vitamin B6, Folate, Selenium and Manganese…to name a few of my (not so) favourites.
Many of you will know I am a fan of staying single 😉 I mean using single nutrients rather than all the ‘bells-&-whistles-formulas’ we’ve come to rely on so heavily. This is one key reason. But the other is that many of these formulas are someone else’s, perhaps a whole tech team’s, idea of what a ‘generic’ low thyroid patient, or an ‘average’ immune challenged patient needs. Not sure about you, but I don’t subscribe to ‘average’ and ‘generic’ when it comes to nutrition…that’s one of naturopathic nutrition’s key criticisms of conventional dietetics, right? So where does this reliance on generic nutritional complexes comes from? Is it purely convenience -yours and the patients?
Or are we insecure in our confidence in creating our own crafted formulas? Is it a need to know our tools of trade better..because if we did, might we better realise the power and potency (positive or negative) of our own prescriptions? Especially in the realm of accurate assessment and individualised requirements.
The latter is my call to action on this, predictably! 😉
I am often asked about where my ‘nutritional nous’ comes from. Which magic journals do I subscribe to that fill my head so full? What non-existent-far-superior-course did I undertake? The answer I give is the same every time. I had one solid nutrition teacher in my under-graduate across my 4 years of naturopathic nutrition at SSNT. What made her so good and why has so much she taught stayed with me? She simply taught me every single nutrient literally from the ground (soil) all the way up (human nutritional physiology) and everything in between. Once you know each nutrient that well and the big concepts that are a truism in nutritional science…you can never go back and you will practice nutritional medicine at its best. My wishful thinking? I wish that for us all 😉
Let’s make sense of the over-arching nutrition principles, that will profoundly change your understanding and application of this modality Truly understanding the ‘big’ concepts, so often overlooked, or incorrectly taught, ensures you get the critical ‘small’ detail in your nutritional prescriptions right. In this 4 hour recording, together with key clinical tools, we talk about the tough stuff: dose-response curves, active versus passive stores and excretory pathways and ooh lah lah…the myth of taking ‘activated vitamins’. Even those who feel satisfied with their original training – will find a lot in this critical review that is new, insightful and truly practise-changing!
Do you know that saying, ‘mind your Ps and Qs?’ It basically means mind your manners and I heard that a lot as a kid 😉 But what we really need to hear now, as practitioners and promoters of healthy eating and wellness is really, Mind your P’s and P’s because a lot of biggest health consequences of any diet are determined by the balance or imbalance of two major players; protein and potassium. We’re always looking for simpler ways to enable patients and ourselves to be able to both recognise the strengths and weaknesses of their diets and, better still, apply a simple method to making better choices moving forward. Eyeballing the protein and potassium rich sources in any diet speaks volumes about other essential dietary characteristics and the likely impact of diet on health – and getting the relationship between these two right should be a goal for us all.
“World Health Organization (WHO) Dietary Targets for Sodium and Potassium are Unrealistic”, reads the recent headline from yet another study finding that humans would rather challenge the solid science of human potassium requirements than acknowledge the urgent need to turn this ship of fools around!
This large study, conducted over 18 countries, involving over 100 thousand individuals, reported that 0.002% met these targets. That’s 1 person in 50,000. Now, the researchers’ response to this is that we should lower our dietary potassium expectations….such that the targets are more achievable and so that (frankly) we are less perpetually disappointed in ourselves and our terrible food choices. Wha????Back up there. The WHO guidelines, just like any other nutrition authority, derived these minimum amounts from a thorough review of the science that speaks to our physiological requirements and the level of nutrients that have been shown to be associated with health. Australia’s own fairly conservative NHMRC suggests even higher amounts for good health! Perhaps rather than revise the established dietary targets we should revise what we’re putting in our mouth!
So where does protein come into this? Well one of the most important and central nutrient dynamics is the balance or imbalance of our intake of both. And in this regard, yet again, we have a surprising lot in common with plants! Whether you’re trying to understand optimal nutrition conditions for growth (nitrogen alone won’t get a plant there, nor protein alone in a human) or the intricacies and nuances of finely tuning our physiological processes such as cardiovascular function, renal health, blood glucose management etc. the answer lies in a happy marriage between these two.
In this area of nutrition, we should be listening most closely in fact to renal specialists/researchers. These ‘undercover’ protein and potassium experts have been talking about this for a long time and in particular, in my humble opinion, Lynda Frassetto has lead that charge for decades. If you haven’t read much on this issue and want somewhere to start at least, jump into her pivotal paper from 2001 which eloquently explains why the human design can not shoulder a potassium shortfall…well not without causing real health problems…like the ones we’re seeing in record numbers currently and why the protein potassium balance of any diet is a major health determinant. That’s why giving ourselves and our patients the knowledge and the tools (yes lovely shiny meaningful infographics included!!), to quickly determine their protein potassium balance, are so necessary and important.
Thanks to Frassetto and many other researchers’ work, looking at food through this protein potassium lens has sharpened my focus and I think it’s about time we all took a good look 🙂
Check out the latest UU30 to hear the latest information…
The health consequences of any diet are largely determined by the balance or imbalance of two major players & proxy markers; protein and potassium. When it comes to this area of nutrition, we should be listening more closely to renal specialists whose research shows why the human design cannot support a potassium shortfall and the health consequences of this. Whether you’re trying to understand optimal nutrition conditions for growth (nitrogen alone won’t get a plant there, nor protein alone in a human) or the intricacies and nuances of finely tuning our physiological processes such as cardiovascular function, renal health, blood glucose management etc. the answer lies in a truly happy marriage between our intake of these two. These recording comes with a clinical resource tool to help you quickly identify the dietary protein:potassium balance for your clients.
Hear all about it by listening to my latest Update in Under 30: Mind Your P’s and P’s For all Update in Under 30 Subscribers, it’s now available in your online account and if you are not a subscriber you can purchase this individually here.
How often were we told this in our training? And how often have we found this to be true in practice? And now suddenly, it seems, the medical researchers (at last!) are rapidly coming around to this core concept?? Our microbiome is suddenly the hottest property on the body block, and it seems every interested party is shouting, ‘Buy!Buy!Buy!’ As integrative health practitioners, of course, we had a major head-start, not just by appreciating the gut’s central positioning in the whole health story (iridology beliefs, maps & teasers aside!!) but also a heads-up about the damage the western diet, our medication exposures and lifestyle tend to wreak upon it. A favourite quote of Jason Hawrelak’s by Justin Sonnenburg, “The western diet starves your microbial self”, underscores the significance of just one element of this impact. And…are we all clear that the increasing number of patients reporting adverse food reactions, once again, overwhelmingly are a response to aberrant processes in the GIT?
Sounds silly it’s so obvious right, but it’s easy to get distracted & misattribute blame…for example, it’s the food that’s the problem. Well yes in a minority of situations interactions between someone’s genes, immune system and a particular food turns something otherwise healthy into something pathological, but for the majority, the food itself & in others is healthy, & could be beneficial to this individual, if only we could resolve their GIT issues…like FODMAPs for example.
Not the problem, just the messenger.
So if the ‘problem food’ is just the messenger, what’s the actual message we need to understand? Is it that this patient has medication, disease or otherwise induced hypochlorhydria, impairing ‘chopping up’ of potential antigens implicated in immune mediated food reactions? Or is that this person’s got fat maldigestion &/or malabsorption so that in addition to not tolerating fats, they may experience dietary oxalate intolerance to boot? Or are the food reactions the result of altered microflora changing what we can and can’t digest (via their critical contribution) & absorb?
So what message does the presence of IgG antibodies to consumed foods send us about the state of someone’s gut? It’s telling us 2 things: this individual exhibits abnormal intestinal permeability & currently in the context of this leaky gut, these foods may constitute a barrier to resolving this & other symptoms as well.
We’ve recently released the mp4 (that’s audio plus the movie version of the slideshow so grab your popcorn…that’s if you don’t have a corn issue!) of A Guide to Investigating Adverse Food Reactions – What’s IgG got to do with it? which details the science behind IgG, including debunking, the incorrect debunking of IgG food antibody testing!! But more than this, it overviews the whole maze of adverse food reactions, articulates a logical investigative path for practitioners through this maze, and helps us to really understand that finding the food(s) responsible for a patient’s symptoms is not the final destination..and can be in fact a distraction, if we don’t cut to the chase and find out the why…and funnily enough…my dear old iridology teachers and colleagues...it almost always comes back to the gut 😉
Confronted with the possibility of adverse food reactions in an increasing number of our patients can be an overwhelming prospect, in terms of accurately identifying and understanding the faulty mechanism underpinning these aberrant responses to healthy foods. Elimination of culprits in most situations is only a short term reliever, not an appropriate long term solution, so to optimise results we need to know the real mechanism of action. The majority of these, of course, stem from the gut, but being able to elucidate exactly which of the many things that can go wrong there, is going wrong and therefore what foods are problematic until we address this, is the key. This 2hr mp4 is all about the bigger picture and helping you find method in the madness that can be the AFR landscape. Along the way, we detail the science of where IgG reactions fit into this and it’s a fascinating story that just might be the missing puzzle in your leaky gut patients.
b. Every herbalist’s jaw at my table at the NHAA conference gala dinner, when I got almost all my Latin binomials right during the trivia quiz?…and after some champagne, that’s a particular achievement
c. My jaw, when I saw firsthand how much those herbalists could drink of ye-not-so-olde herbal extracts!!
d. The latest Update and Under 30 – Milk Madness Part 2
e. All of the above
If you answered, ‘e’…. you must have been one of those herbalists at my table, otherwise you have way too much insider information! But yes you are correct on all accounts. So this latest UU30 is an extension of our discussion last month about the potential contribution from to mental health from dairy intake in a subset of patients. This whole topic, the research for which dates all the way back to the 70s, was too big to fit into one – given the current evidence base that now depicts at least 2 different mechanisms that might be at play, and the different types of mental health problems, each has been linked with. Last month was all about retracing the ‘dietary exorphin’ path, this month it’s about the propensity for some individuals to make antibodies to casein and the significant growing data that suggest this happens to a larger extent in patients with certain psychiatric diagnoses. More importantly, we talk about the ‘why’.
What compelled me to make time to look through all the literature on this was that there is some. No seriously. When I initially learned of the GFCF dietary approach to ASD patients I was told that in spite of a lack of supportive research, the empirical clinical evidence was irrefutable, which I later saw with my own eyes. In the couple of decades since, I only really heard about negative findings, short trials of the elimination diet specifically in ASD kids, that failed to produce significant change. Funny how the bad stories rise to the top, right? But when I spent the time doing a thorough literature review, I found these negative findings were far from the whole story. In fact, I was really surprised by the high level of evidence employed by researchers of late, who have repeatedly found associations between either exorphin or antibody levels and patients with particular diagnoses, in addition to really progressing our understanding of why these measurable differences (urinary exorphins, plasma IgG and to a lesser extent IgA casein antibodies) are meaningful. Do we know everything? What do you think? The answer, of course, is always no. But we know enough to consider this aspect in our comprehensive workup of mental health patients and all their biological drivers and we know dramatically more than anyone in mainstream medicine, or the dairy industry for that matter, is ever going to let on!
If you want to hear a synthesis of the casein antibody link with mental health then download the latest UU30 – Milk Madness – part 2. If you can’t go that far, then “do yourself a favour” and read a couple of seriously important articles on this topic – and why not start at the deep end with this study by Severance in 2015.
Could dairy intake in susceptible individuals be a risk promoter for mental health problems? In addition to evidence of the exorphin derivatives from certain caseins interacting with our endogenous opiate system discussed in part 1, we now look at the evidence in support of other milk madness mechanisms. Specifically, the IgG and, to a much lesser extent, IgA antibodies about what this tells us about the patient sitting in front of us about their gut generally and about their mental health risks, specifically. The literature in this area dates back to the 1970s but the findings of more recent and more rigorous research are compelling.
We’re not deaf…we heard that stampede of Iron-Inundated Practitioners!
Our recordings and clinical resources for improving your skill-set in all things iron including, your accuracy of diagnosing deficiencies, pseudo-deficiencies & excesses, plus radically rethinking the best treatment approaches for each scenario…have been some of our most popular. Because nailing iron (pardon the pun) is harder than we were all lead to believe and at least 1 ‘iron maiden’ or ‘iron man’ walks into our practice every day, right? So we’ve brought together 5 extremely popular UU30’s on Iron into one bundle for the price of 4! So if you’re more than ready to graduate from ‘iron school’, now’s your best chance!
1. So You Think You Know How to Read Iron Studies? (≤30 min audio + Cheat Sheet)
Overt Iron Deficiency Anaemia or Haemochromatosis aside…do you understand the critical insights markers like transferrin and its saturation reveal about your patients iron status? Most practitioners don’t and as a result give iron when they shouldn’t and fail to sometimes when they should. This audio complete with an amazing cheat sheet for interpreting your patients Iron Study results will sharpen your skills around iron assessment, enabling you to recognise the real story of your patients’ relationship with iron.
2. Pseudo Iron Deficiency (≤30 minute audio)
The most common mistake made in the interpretation of Iron Studies is this one: confusing inflammation driven iron ‘hiding’ with a genuine iron deficiency. Worse still, following through and giving such a patient oral iron – when in fact it is at its most ‘toxic’ to them.
This audio together with some key patient pathology examples will prevent you ever falling for this one! Learn how to recognise a ‘Pseudo Iron Deficiency’ in a heartbeat!
3. Iron Overload… But not as you know it (≤30 minute audio)
We’re increasingly seeing high ferritin levels in our patients and getting more comfortable referring those patients for gene testing of the haemochromatosis mutations; but, do you know how to distinguish between high ferritin levels that are likely to be genetic and those that are not? This can save you and your patient time and money and there are some strong road signs you need to know. In addition to this, what could cause ferritin results in the hundreds if it’s not genetic nor inflammation? This Update in Under 30 summary will help you streamline your investigations and add a whole new dimension to understanding iron overload…but not as you know it!
4. So You Think You Know How To Treat Iron Deficiency? (≤30 min audio)
And then you don’t. The reality is we all struggle at times with correcting low ferritin or iron deficiency anaemia – so what have we got wrong? In spite of being the most common nutritional deficiency worldwide, the traditional treatment approaches to supplementation have been rudimentary, falling under the hit hard and heavy model e.g. 70mg TIDS, and are relatively unconvincing in terms of success. New research into iron homeostasis has revealed why these prescriptions are all wrong and what even us low-dosers need to do to get it more right, more often!
5. So You Think You Know the Best Iron Supplement, Right?! (≤30 min audio + Iron Supplement Guide)
Iron supplementation, regardless of brand, presents us with some major challenges: low efficacy, poor tolerability & high toxicity – in terms of oxidative stress, inflammation (local and systemic) and detrimental effects on patients’ microbiome. What should we look for to minimise these issues & enhance our patients’ chance of success. Which nutritional adjuvants are likely to turn a non-responder into a success story and how do we tailor the approach for each patient? It’s not what you’ve been taught nor is it what you think! This comes with a bonus clinical tool, a fabulous easy reference guide – to help you individualise your approach to iron deficiency and increase your likelihood of success.
You’ll never look at iron studies or your iron-challenged patients the same way.
Listen to these audios straight away in your online account.
So this is not news to most people who know me but I don’t like taking things out of people’s diet. As a result, in a room full of naturopaths & integrative medicos, I might be voted the least likely to use the phrase, “No Gluten or Dairy for you!” [said with the Soup Nazi’s accent from Seinfeld]. I must have slept through that class when we were taught to do this for absolutely every patient. But seriously, I try not to remove or exclude foods without a very strong rationale and evidence-base that relates directly to the person sitting in front of me, for several reasons: 1) those seeds are powerful ones to plant in your patient’s mind…how do they carry that with them as they move through life, navigating food and social settings etc etc…all well and good if this is a proven life-long pathological provocation for them but otherwise… 2) dietary exclusion is stressful for families & in kids especially, can create disordered eating and a range of other psychological impacts and 3) GFDF diets are not necessarily healthier in the basic nutrition stakes…if you haven’t read Sue Shephard’s work on the deterioration of diet quality in GF patients…you should. It can be much healthier of course…but often the real-world application of the principle doesn’t always match the lovely ‘serving suggestion image’ on all the GFDF highly processed, packaged foods!!
So listen up people, because now I’m talking about when I would seriously consider joining in on the GFDF chant.
The one patient group I’ve never quibbled over the benefits of GFDF, has been the autistic one. I was taught the merits of this approach early on by a few fabulous courageous integrative doctors and paediatricians who came back from the front-line of their clinics, reporting good effects. I then had the important firsthand experience of unprecedented verabilisation in a non-verbal ASD child’ after excluding these foods. But what I’ve been thinking a lot (and reading a lot!) about lately is the possibility that these ‘dietary exorphins’ may have negative mood effects in other subsets of mental health patients. My thought process is like slow TV! That aside, there’s a lot to be said for taking the time to really getting across an issue – even if that involves reading papers from as far back as the 1960s when the idea of a negative role for dietary exorphins in schizophrenics was first floated by Dohan & colleagues.
Let me say, when you go back to the beginning it’s undeniably a shaky start for the exorphin evidence base, but as you read the studies that emerge from decade to decade until the noughties…it reveals a nagging research topic that won’t go away and a fascinating process of discovery.
So is the devil really in the (regular commercial cow’s) milk? Well I think for some patients it may well be a contributor – most notably those with features consistent with the pattern of excess opiate effects including a higher dopamine picture, regardless of the mental health label they’ve been given, although, more commonly seen in ASD, psychotic presentations etc. But how do we work out which ones, because none of the evidence points to it affecting 100% of these groups…well that’s where we need to go back and truly understand the structure of these dietary exorphins and just how they potentially wreak havoc in some.
The latest UU30 takes your through the story of BCM-7 with a summary of research compile over half a century in Under 30 minutes!
There is a well-rehearsed chant in the integrative management for ASD individuals, “Gluten free- casein free diets” is based on the dietary exorphin theory which suggests these foods generate bioactive peptides that act unfavourably in the brain. Where did this theory emerge from and how strong or weak is the evidence upon which this therapeutic intervention stands? Even more interesting, is there support of this theory in a wider range of mental health presentations such as schizophrenia, post-partum psychosis and depression. Is there such a thing as milk madness for a subset of our patients?
Hear all about it by listening to my latest Update in Under 30: Milk Madness – Is it a thing? For all Update in Under 30 Subscribers, it’s now available in your online account and if you are not a subscriber you can purchase this individually here.
Let’s talk turkey about our pharmaceutical Pet Hates, mine are Proton Pump Inhibitors (PPIs). They irk me more than any other drug class. It’s not entirely rational. Let’s face it, they have some stiff competition but for some reason, in my mind, they almost always win: helping so little & at such a high cost to patients. What fuels my fire of course is their over-prescription, followed closely by the complete disregard for the prescribing guidelines which state:
“When clinically indicated, PPIs should be used for the shortest duration necessary and chronic use is not recommended except for treatment of pathological hypersecretory conditions including Zollinger-Ellison syndrome and maintenance healing of erosive oesophagitis.”
Sorry…did I hear you correctly?Chronic use is not recommended – yet this is one of the drugs most commonly on ‘set and forget mode’ in general practice. To boot, their chronic use has been associated with a number of serious concerns, which I’ve touched on before, from osteoporosis to increased rates of GIT infections. not to mention just the little ol’ detail of malabsorption of multiple nutrients! But this week, yet another health concern has popped up and into my inbox…and well..I found myself shouting at the medical newsfeed on my screen…[again] 🙁
“In their analysis, more than 42,500 adverse events reported to the US Food and Drug Administration by patients on PPI monotherapy were compared with more than 8300 reports from patients on histamine-2 receptor antagonists (H2RAs)….Patients on PPIs alone were 28 times more likely to report chronic kidney disease than those taking H2RAs, while the frequency of acute kidney injury reports was around four times higher…Reports of end-stage renal disease were 35-fold higher among PPI users, while reports of renal nephrolithiasis were three times higher”
To be clear, while these increased rates are TERRIBLE and unacceptable in the context of the ‘set and forget’ prescribing that seems it be rife in most countries, they still only effect a small % of patients e.g. approx 5% of patients had adverse renal effects on PPIs Vs 1% on the older generation H2 blockers for reflux but it’s yet another reason (like we needed more?!) to think twice before our patients are initiated on these meds, which are presented to patients as being benign. Typically with drug development, the older drugs in a class are superseded by newer ones that are ‘cleaner’, and therefore more effective with less adverse effects but this is one situation where if one of my patients really did need a med, I would say out with the new and in with the old!
One scenario where PPIs in combo with multiple antibiotics get routinely rolled out is of course H.pylori infections. But does this make sense??
For a bacteria identified just a few decades ago as being a cause of chronic gastritis, atrophic gastritis and gastric carcinoma, the escalation of number of antibiotics used to eradicate it (4 at last count + PPI) has been nothing short of breathtaking. A management approach more consistent with both integrative medicine and with an improved understanding of the delicate microbiome focuses on changing the gastric environment to ‘remove the welcome mat’. What do we know about how to do this successfully? It turns out…quite a lot. You can find out here with our previous UU30: H.pylori- Eradicate or Rehabilitate?
How long? How long must we sing this song? I’m feeling a bit 80s anthemic and righteous. It turns out that patients’ bowel movements could be improved by using a foot stool?!! Who said that??
Only every naturopath, ever. Right?
But now medical researchers are singing the praises of the Stool Stool too…sorry, I mean the ‘defaecation postural modification device’…because lo and behold a new study of over 1000 bowel movements revealed using a stool to elevate your feet while on the toilet improved the speed and ease, improved full emptying, reduced the strain etc of laxation, >70% of the time, even in ‘healthy, non-constipated patients’. There’s a quick video you can watch to get across this groundbreaking research, or you can read the full article here. I’ve been educating patients about this for about 20 years and it never fails to revolutionise their world!
It would seem that elevating your feet results in straightening “the unnatural bend in the rectum that occurs when sitting on the toilet by placing the body in the squatting position nature intended”…hang on a second…who’s calling what unnatural???…I think the highfalutin anti-anatomical bathroom contraption, we westerners call a toilet, wins the ‘unnatural’ crown!
Next thing you know there’ll be a study that tells us squatting to have babies makes more sense that lying on your back…right?! 🙂
Love talking all-things Stool?
Fabulous Farty Fibre is a previous UU30 recording. Rachel at her warmest and funniest reminds us that fibre is a critical component to good nutrition and is often overlooked, partly due to the popularity of paleolithic and no grain diets. This UU30 details the important functions of different types of fibre and therefore the importance and therapeutic applications for fibre diversity.
Virginal skin, as my sister calls it, is on the endangered list. She also predicts that as a result, it will be a highly sort after commodity in the future and I agree but our reasons are a little different. Hers are aesthetic and mine are well, health-based.
I dislike spreading fear in the wellness world, especially around the area of autoimmunity, which is already plagued with podcasting puritans, espousing the notion that people with autoimmune conditions need to give up every single source of joy in their lives and then, and only then, they will be healed
[Silent Scream !!!!!!]
The essential formula for autoimmunity is generally thought to be: genetic susceptibility + environmental trigger = Bingo! i.e. Hashimoto’s or Grave’s or AS or or or…There are already so many candidates, both confirmed and speculated, on the environmental triggers list, from individual nutrient deficiencies, to food groups, from infectious organisms to of course, the big monster under the bed and everywhere else (!), environmental toxins. But wait there’s one more.
Recently I was prompted to ask one of my mentors whether tattoo inks contained heavy metals. His reply, “I seriously doubt that heavy metal-free tattoo inks even exist.” Then someone on my team forwarded me this well referenced article that contains the above quote titled, Toxic Chemicals Found in Tattoos: Links to Autoimmune & Inflammatory Diseases. I haven’t had a chance to read their citations and understand the real implications of this very plausible biological threat and I can’t do anything about the skull & crossbones on my back but I can warn my kids, my patients and anyone else with virginal skin to rethink the ink.
It’s summer time for all of us in the southern hemisphere & that means….Slip Slop Slap?!
Vitamin D deficiency has been associated with a long list of major health conditions: from autoimmunity to mental health & almost everything in between. This has lead to many of us recommending high dose vitamin D supplementation for a large proportion of our patients but do we understand everything we need to to be certain of the merits and safety of this? In this provocative podcast, Should We Rethink High Dose Vitamin D, Rachel outlines the key unresolved vitamin D dilemmas that should encourage us to exercise caution with supplementation and outlines how adequate sun exposure is associated with improved health outcomes independent of the production and action of vitamin D.
Did you and all your patients survive Spring? Have you had a chance to restock the shelves with all the big-gun-Quercetin-products for the next allergy onslaught…or maybe for patients presenting with other conditions that respond well to this, like leaky gut, asthma, MCAS, Grave’s disease? Either way…can I ask you a Quiet Quercetin Question…how high do you go?
I ask this because I know myself to be pretty heavy-handed at times, especially in those severely affected by traditional allergies..and the results are so impressive for patients and practitioners alike, it’s easy to perhaps get very enthusiastic with this approach, with doses sneaking higher and higher… if a little is so good then a lot must be great!
“Severe eczema and allergic asthma – [Insert preferred big-gun-Quercetin-product] 2 three times a day – STAT!”
And we use it across all patients, right? I love it in kids, teens and adults, men and women. So I kind of stopped dead in my tracks when a colleague recently said…”I do the same…buckets of Quercetin especially over hayfever season but Rach, what about it’s phyto-oestrogenic effects? Should we be worried?” Ah…yup…that’s right…being a flavanoid…it has them. Now let’s be clear about one thing, unlike some practitioners I am NOT, I repeat, NOT against phytoestrogens nor even (ahem) soy 😉 but the question was great because it got me thinking…at high-end supplement doses we are producing levels in the body 100s if not 1000s of times higher than a fruit and vegetable rich diet ever can….is it time we knew a little bit more about what Quercetin does at this level, or is suspected of doing and not just the benefits. Therefore we can be more informed about who we should not be so generous or so long-term with our big Quercetin prescriptions?
So I started busying myself in the literature and it turns out THERE IS A LOT OF LITERATURE!
[Note to said colleague who asked me question, you owe me some sleep] But at least I got an answer!
If you want a bit of DIY drilling then this Andes et al paper is an excellent overview of quercetin supplementation safety concerns…but it doesn’t cover everything. We need to talk. We need to talk about that dang estrogen aspect but it’s bigger than that – you see Quercetin doesn’t just engage with oestrogen receptors like a ‘normal’ phytoestrogen…it messes with levels of this hormone via several other paths…and where does that lead us…? Listen in to the latest UU30 Querctin – Are We Pushing the Limits? and you’ll know exactly our destination. This is important for the Quercetin Queens (both male and female) among us…and that’s like…everyone…right? 🙂
Quercetin has become an absolute go-to treatment for many practitioners faced with patients affected with allergies and high histamine. It is in this context, that often we find ourselves using large amounts over long periods. Supplemental quercetin exhibits a 5-20 fold higher bioavailability than its dietary counterpart, therefore increasing body levels beyond what a diet could ever achieve. This introduces more potent novel actions: anti-thyroid, pro-oestrogenic, detoxification disrupting…are we pushing the limits of desirable effects and introducing some undesirable ones and who should we be most conservative in?