During mentoring sessions over the last week I’ve been prompted to ask a few practitioners if their patient had any signs, either clinically or in their pathology results, of high oestrogen.Each time it kind of caught the practitioner off guard because their patients weren’t presenting with conditions overtly related to an oestrogen excess and they hadn’t specifically ‘tested’ for this. However, in each instance the information was already there in the case, it was just a matter of knowing what markers to look for.
So some patients scream ‘high oestrogen’ right from the minute they enter the room? But often others present with health problems that don’t necessarily appear related at first glance. Regardless, their condition absolutely could be being compounded by this background imbalance – think thyroid & other autoimmune conditions for example.
There are plenty of patients who don’t have the exaggerated clinical presentation but still have this imbalance as a significant compounder or perpetuating issue in terms of their pathology.
Relax – I am not suggesting salivary hormones or any form of expensive testing all round (!) – in fact what I am saying is before you even consider yet another pay out of pocket test, costing your patient more time and money, we should look to the clues that are already there, in standard blood tests. Amazingly, you can infer a lot not just about the overall oestrogenic load but also pick up some clues as well about where the excess might be coming from.
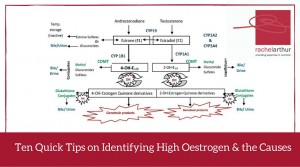
In this Update Rachel brings together her 10 quick tips on how to recognise either high oestrogen and/or the potential underpinning reason behind the excess, in a range of easily accessible markers. A great refresher and synthesis of ideas on this important aspect of diagnosis and clinical management. This Update in Under 30 is now available to purchase as a download, click here to find out more or if you’re interested in a 12mo subscription click here
We now suspect that many of the drivers behind PCOS are heritable components – a genetic vulnerability passed from parents, possibly one but often both. This growing understanding has identified a phenomenon referred to as ‘PCOS families’ i.e. a family in which at least one female has confirmed PCOS.
Being a primary biological relative of someone with PCOS, it would seem, suggests a shared risk, even if you are a son, or brother or father.
So beyond the very high rates of undiagnosed PCOS in sisters of someone already diagnosed, there is much talk now about a male PCOS phenotype equivalent.(more…)
As we head rapidly towards the change over of our calendars we would like to offer you a special on the very best educational recordings from 2014 – buy 2 CDs before Jan 31st and receive one complimentary Premium Audio Recording of your choice OR purchase 4 CDs and receive a 3 month Premium Audio subscription for free.
It’s been a busy year during which Rachel has delivered 7 very successful new seminars in the area of mental health and beyond, most notably fortifying her role as a leader in the field of diagnostics and pathology interpretation. This has included collaborations with ACNEM, Biomedica, Health Masters Live, MINDD and Nutrition Care, however, each recording is classic Rachel – full of fresh perspectives on diagnosis & treatment, colourful analogies & humour. In case you missed some of these this year or want a copy for keeps – here’s a quick summary of the 2014 recordings included in this end of year offer: (more…)
In spite of several advantages of salivary hormone assessment, one important piece of information you miss out on when you do this rather than blood assays, is the SHBG result. Sex hormone binding globulin is a protein produced in the liver that, as the name suggests, binds our sex hormones rendering them inactive and therefore buffering us against their full potency. They bind the sex hormones to different degrees – the androgens most potently and oestradiol to a lesser extent but curiously it’s higher oestrogen that represents the major hormonal driver of increased SHBG production (including synthetic oestrogens). (more…)