
What’s your knee-jerk response to 52Y Lipids Lucy & Liver, whose ALT & AST suddenly jumped above range when she was put on statins? They’re damaging her liver? You’d be wrong. One of the practitioners who undertook the MasterCourse in Comprehensive Diagnostics just graduated with flying colours when she was able to correctly identify the true cause of this patient’s LFT abnormalities, can you?
[Cheeky hint: there is more than one explanation/process at play]
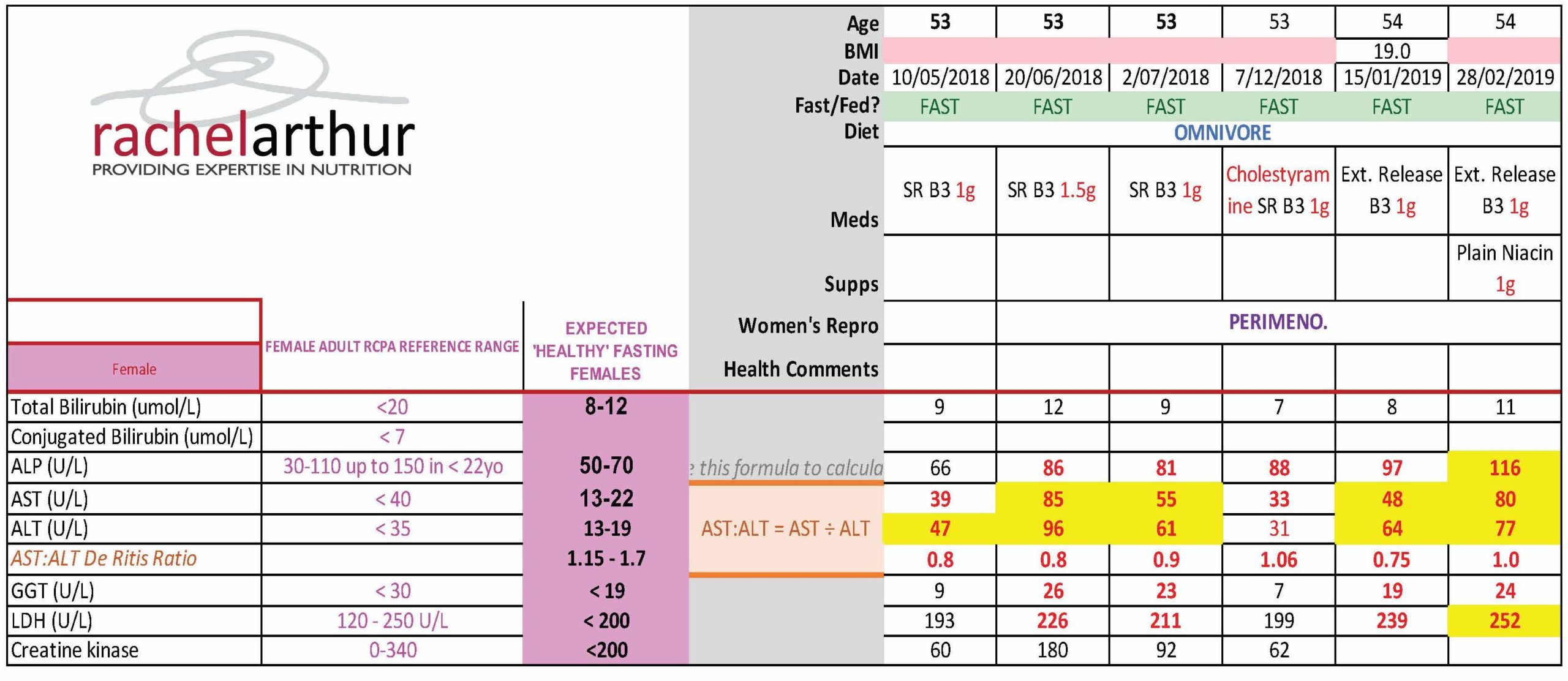
This naturopath now knows her pathology patterns. She knows the interpretation of any liver enzyme must also take into account the movement in other markers, to make meaning of the whole. Because so-called ‘liver enzymes’ are never exclusive to the liver. They are expressed in multiple other tissues and organs – sometimes at equal concentrations to their liver-level (e.g. ALP and bone). For some, even referring to them as a ‘liver enzyme’ is a mislabelling of sorts, with minimal expression in the liver itself compared with ubiquitous distribution all over the body (e.g. GGT & LDH). Of course this is both a blessing and a curse. A curse if you make the mistake of only interpreting their levels through a ‘liver lens’…a blessing if you know when they are flagging problems elsewhere through the specific pattern recognition. So back to Lucy – the statins had induced a rhabdomyolysis not hepatocellular damage. The clues? Significant AST dominance over ALT, above range CK and LDH.
So if the statins weren’t causing increased hepatocellular damage what is that increasingly high-normal ALP pattern all about?
Bones. And again, this practitioner picked it. And then got to win herself some pretty BIG credit and credibility points with all the other health professionals sharing care of this patient by suggesting that they clarify and confirm this by referring her for an ALP bone isoenzyme assay, which answers the question: is the elevated ALP originating from the liver, the intestines or from the bone? Bingo, bones it is! Or was, because this practitioner was able to alert not only the patient but all the other practitioners treating her to the increased bone remodelling taking place, independent of the statin reaction, but part of her perimenopause. Left unchecked this would escalate further of course at menopause and leave her bones in bad shape. This is just one illustration of how we can show ourselves the be the incredible one we are on the shared-care team.
Being lab literate and pathology proficient, sets you apart from the rest and enables you to practice truly preventative medicine.
How else would we have known she was experiencing increased BMD loss that may be the start of something truly tragic?
Realise the true value you can extract from the most commonly performed labs.
Join Rachel Arthur LIVE on the MasterCourse I: Comprehensive Diagnostics WATCH PARTY
This skill is the biggest ‘game-changer’ in Integrative Medicine!
Want to know more? Head over to my website here and check out more of the great benefits and bonuses of joining this program
This course is a fantastic learning opportunity to identify the many intricacies in cases that have previously been missed.
