And for weeks now I’ve really been banging 🥁🥁 The 1st drum was me making us all salivate & suffer through my month-long Mediterranean feast The 2nd, my ongoing incurable fixation on the ‘Power of the Ps’ – Protein & Potassium, not just individually, in terms of meeting optimal requirements for each, but relationally, as in, the (im)balance between them & the clear goals that have come from research for best health outcomes.
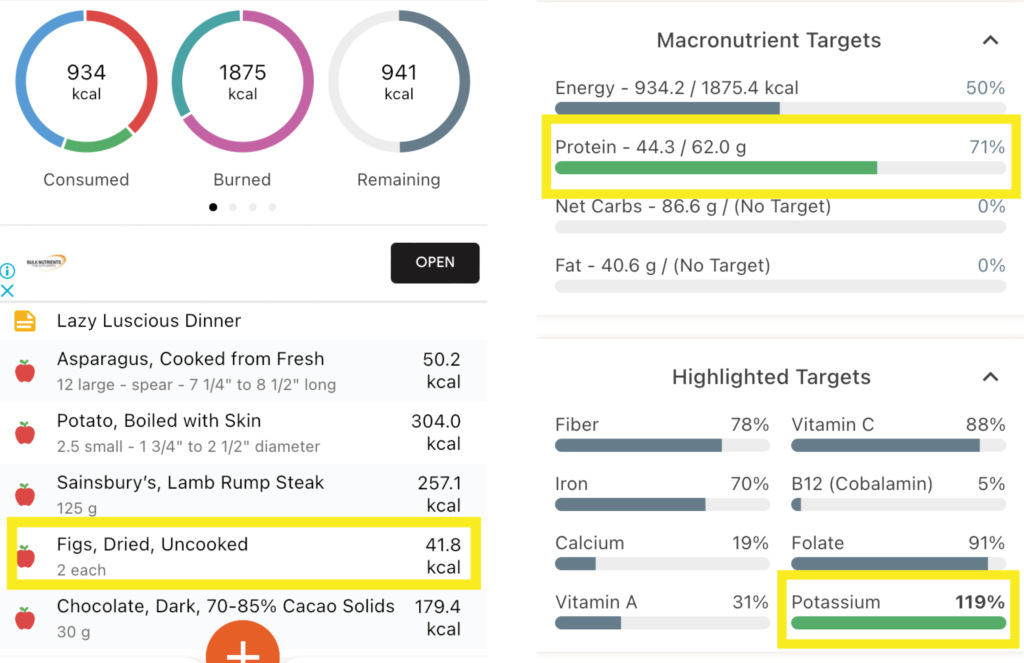
Maybe now you can hear the individual drumbeats merging to form some sort of chorus rather than a cacophony?! I can🎶 And largely that’s because I decided to put the Ps & Ps principles (Total Protein:Potassium < 1; Animal Protein:Potassium <0.6 etc) into practice, entering my own meals into software to see how often I kicked each goal and how often I missed (& [ouch] kicked myself). Personally, I think thirty years in the game can lead to some laziness around looking in depth at our own dietary habits. As in, I know the ‘rules’ right, back to front, so I’ve told the ref to have the rest of the season off! My meals are both mantra and memory foam. There’s a lot of eat and repeat. Like my heavy lunchtime reliance on my ‘protein power pack’: 2 XL soft boiled eggs on 1 piece of avocado paleo toast and a bunch of asparagus. My (in)famous buckwheat breakfasts loaded with nuts, yoghurt & fruit. My bulk-cooked plant protein heavy, animal protein light, stews, sauces and soups. Even, what I considered my laziest but luscious organic farmers market meal, pan fried lamb rump steak, steamed fresh new season potatoes & a bunch of asparagus. So which of these would you have put your money on for the most Ps& Ps goals kicked? 🤓🤯
The Lazy Luscious Steak & Veg Meal Wins with… Total Protein : Potassium of 0.56! Animal Protein : Potassium of 0.41 Btw that’s because of the Potassium-punch of Potatoes [>2200mg!] and the finale of Figs & dark chocolate [329mg]! Animal Protein : Vegetable Protein of 2 : 1 (ok so you can’t win everything!)
Now obviously I am just looking at each meal individually, but the Protein & Potassium goals are really daily ones, however, I, like most people, don’t lay out the totality of my ideal food intake for the day and then think, now how do I make this all edible?! I think in meals not metadata! So this little exercise was already incredibly rich in insights, checking my assumptions and snapping me out of some misguided mental calculations into the real world, placing a ref back on the pitch! I’m not ditching any of these favourites – just more mindful of what meal goes with others across the day, for better balance. Now all this analysis is time-consuming of course and while various software will do the macro and micro crunch, as far as I know, you still need to do all the Protein and Potassium calculations by hand, Ah yup. So, 1) I’m stopping now & 2) I’m thinking about creating a little spreadsheet that auto-calculates a lot of these targets once you’ve obtained that basic elemental data to input, for easier use in the future – would you use it?? [insert answer here 🙋♂️]
And then you can show me your kick arse protein/potassium combo! Because clearly even us ‘experts’ apparently need data to double-check our assumptions!
Now where’s the other 🥁 in all this, that Mediterranean one, I hear you ask? It’s in the figs! My lamb dinner actually just missed reaching the targets for protein and potassium balance…until my fig finale! And remember, what the Greeks say, ‘A few figs a day keep the chronic-mild-metabolic-acidosis at bay!’ 😂 Just jokes…
To prevent or minimise our slow but steady march towards sarcopenia, the need for dietary protein adequacy to fuel muscle maintenance is a no-brainer – but how does ageing affect this? We get less bang for our buck. We have to eat more, to get the same ‘amount’ but do you know why this is? Add to this, that also as we age, we experience a greater acid burden from a lower acid dietary load. And given that a higher acid load (PRAL), has been shown to have a negative effect on muscle and bone markers in the past, clearly to ensure optimal health of our bones and muscles as we age, we have a riddle, or two, we need to solve. How do we use Protein and Potassium intakes to benchmark our patient’s diet quality and musculoskeletal risks and can we modify their consumption of either, to drive therapeutic gains in terms of both BMD and muscle?
You can purchase The Protein & Potassium Riddle of Ageing – Muscles and Boneshere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
And it will. It knocked again on a practitioner’s door last week. She in turn knocked on mine. It turned out to be a very familiar story:
Firstly:Patient presents distressed – recently a nurse applied the term ‘Chronic Kidney Disease’ to HER (note no one has ever mentioned this diagnosis) Secondly:She is in stage 3 of 5 Then: This practitioner is left to have ‘the conversation’ but wants to know where to start, ‘What do I say?’ Next up:And what else can I do for her – are we really able to make a difference?
Familiar to you too? So,1st & 2nd: Yes, this is not uncommon we would have to say and even with age-appropriate reference range adjustment, her GFR consistently in the 50s, flags premature decline. Then: What DO you say? Well this clearly is a delicate area, not only because of the level of patient distress and concern but because, at this stage the practitioner knows nothing more than what the patient tells her and her ELFTs over the last 2 years. This is not enough information, right? Chronic Kidney Disease is a heterogeneous condition, with many different causes, manifestations, comorbid conditions, and factors affecting prognosis (Levey et al., 2009) So while most individuals certainly progress from stage I to II and II to III the rate at which they do this differs dramatically.
Two years of data is not long enough for us to appreciate the trajectory of her CKD & means we are unable to provide the patient with any kind of perspective:
‘With no further decline in GFR or progression in stages over 5 years, you’re doing well, so keep doing what you’re doing!’ Vs ‘Ok, I can see what looks like a little period of accelerated decline – let’s review what’s been happening and how we can turn this around”
“Please sir can I have some more?’ Yes, back to her primary carers to request more information to fill in the gaps, and ideally more labs to calculate & observe the trajectory for yourself. Next Up: What do we have to offer the patient with CKD stage III? Soooooooooooooooooooooooooooooooooo much!! When is adequate hydration helpful? Always, except Stage V! (and these patients are not coming to see us) What are our treatment objectives & our evidence backed medicines to meet these? Hcy lowering (note often referred to as ‘folate refractory’ in renal dx), vitamin D adequacy, lowering the acid load, supporting the microbiome & in turn the Renal-GIT axis…hang on, got to go…someone’s knocking 😅 but hopefully we all can see, when they present to us, they are indeed knocking on the right door ✊
Nutritional or naturopathic support for the kidneys tends to have been over-looked in our training and yet research suggests there is much in our tool kit that can make an enormous difference to this system, in particular, slowing the progression of chronic kidney disease in patients. Rachel talks about what these key evidence based interventions are and also gives you the tools to identify the early pathology markers of renal impairment – the earlier the recognition, the earlier we can make a start on the remedy.
It seems almost farcical to question the merits of hydration for our renal health but is this actually the truism we have been lead to believe? Where does the recommendation of ‘8 glasses a day’ come from and what is the level of evidence to support it and in whom? Or should we in fact be setting our sights on output ie. 24 hr urinary volume, over input. Do all kidneys love water – or does this relationship change with the progressive impairment seen in CKD which affects up to 30% of our middle-aged population? When does hydration become harassment?
Most practitioners graduated with not much more than a few ‘kidney’ herbs and an under-appreciation of the contribution renal health makes to wellbeing. It’s not just about waste and water. In reality, the kidneys are pivotal in just about every major element: blood, bones, pH balance, methylation, control of oxidative stress, the GIT microbiome and more! And we are seeing the impact of this in our patients in all sorts of subtle and not so subtle presentations. This new instalment in diagnostics, brings the renal system into the spotlight so we can confidently identify and better manage its critical contribution. In addition to this, just like with other routine labs such as LFTs, we unpack how these so-called ‘renal markers’ can flag a plethora of other insights into your patients, from reflecting (un)healthy muscle mass, to calculating individual dietary protein adequacy, from key ‘danger and distress’ signals in response to disturbed metabolism, oxidative stress to certain types of GIT dysbiosis! We call this Explained, Expanded and Exploded because these routine labs can deliver XXX sized insights into your patients.
That’s not a word you hear often spoken by people practising nutritional medicine. Which is odd. I mean outside of the whole, ‘I’m not good with sulphites so I just have to add these magic drops into my glass of red so I can knock back my share,” often overheard at our conferences… it’s like this essential macromineral, pivotal to human health for things like barrier function, antioxidant defence and our basic ability to create the white cells for immune defence (for that matter), detoxification, musculoskeletal tissue integrity etc has just not received its due attention from us. Not entirely surprising given 1) there’s no RDI and 2) there’s no lab test to assess an individual’s status and how about 3) because we were never taught about it!
But the biggest ‘call to action’ here is that, in spite of items 1, 2 & 3, we’re ‘prescribing’ Sulphur Strategies all the time!
Take one of my favourite examples;GAGs. Glycosaminoglycans like Glucosamine sulphate (not the crappy, found to be not as effective, other forms that we now see more commonly) hit the headlines back in the noughties as an effective arthritis remedy. This is one of the 100s of our body’s ‘end products’ of its endogenous Sulphur Stream. We naturally make this in adequate amounts to ensure the integrity of our joints (and many other tissues of course!) when we have enough Sulphur in the ‘top pool’ (organic Sulphur) to trickle down to the 2nd pool (Inorganic Sulphur), therefore creating a constant essential supply of something known as ‘the universal Sulphur donor’ – ‘PAPs’, to its friends 😉 Like a waterfall, it helps to have a good flow from the top to increase the likelihood we’ll have anything to ‘show’ at the bottom.
So when we give a patient Glucosamine Sulphate it may well help. Or not. But did we ‘treat the cause’ of their Sulphur problem? Should we have treated higher up, increasing the size of either the organic or inorganic pool to have improved and widened the benefits for their health? Or, as is equally common, actually identified why someone might need more Sulphur than most – due to increased demand and losses?
Herein lies my reason for liking this particular Sulphur story somuch. The common medication that places the highest ‘demand’ on Sulphur (due to its need for detoxification) is paracetamol. There’s no debate regarding this – just absolute scientific consensus. NSAIDs and steroids also negatively affect the Sulphur status of individuals, as does Vitamin D deficiency and chronic mild metabolic acidosis. Now how commonly are these phenomena co-occurring in our patients afflicted with arthritis? And traditionally of course, what was the remedy for arthritis? Sulphur springs.
Unseen Sulphur – Time To Take A Look If you don’t have a clear picture of the gross daily requirements, determinants of altered individual needs, sources, regulation & associated deficiency picture of Sulphur, you’re not alone. Turns out this essential macromineral remains ‘unseen’ by most, even though you’re probably writing prescriptions every day that have Sulphur as their key component. From the simple: Taurine, N-acetyl cysteine, Protein powders, to the sublime: Brassica extracts & concentrates, N-acetyl Glucosamine, Alpha Lipoic acid etc. In order to use these Sulphur strategies successfully and safely, however, we need to fill in the missing detail on its metabolism, the difference between the ‘organic’ and ‘inorganic pools’, how regulation regularly goes wrong even in those seemingly consuming enough and how to balance the risks of this reactive medicine with its substantial therapeutic value. This recording comes with a great clinical tool to help you, at last, see the Sulphur strategy most indicated for your patient.
You can purchase Unseen Sulphur – Time to Take a Lookhere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
I say: Biotin, Broccoli Sprouts & Bone Broth You say….?
If you said: ‘Sulphur’, go directly to the top of the class, passing ‘Go’ & collecting $200 on your way!🤓 If you nervously said…”I don’t know, they all start with ‘B’ ?”, you are not alone. In fact, most integrative health professionals aren’t aware of the Sulphur Strategies they’re using, probably, everyday. But it’s time we all were.
How about this list? Glycosaminoglycans (GAGs for joint, gut etc tissue integrity), Cerebroside Sulphate (Myelin), Metallothionein, Glutathione, Hydrogen Sulphide (H2S), Co-Enzyme A, Lipoic acid, SAMe, are just some things Sulphur is essential for.
I could go on…and on and on. You see Sulphur, in spite of being an essential macromineral (adult dietary requirements > 1g per day) and critical to health, remains largely unseen. Often we don’t know when we’re writing patient prescriptions that actually we’re using a particular vehicle for Sulphur and therefore we’re also not able to discern which, of the very long list of options (dietary and supplements), makes the most sense in this patient at this time. We’re not to blame, not many ‘possess the power’ to see it, it seems. Por old essential, irreplaceable Sulphur doesn’t even have an RDI. But the time has come to take a good look. We need to know how patients are able to meet their needs, who needs more and how, very commonly, someone who is seemingly ‘consuming enough’ may still exhibit a functional Sulphur deficiency with poor musculoskeletal tissue integrity, low white cell replication capacity or higher oxidative stress load etc and in those who do have a shortfall, how to treat successfully & safely. Who needs a top down approach (more protein, methionine, cysteine, bone broth) and in whom would that be a risky path and using ‘downstream’ Sulphur products instead would be a better balance of pros and cons?
Because all Sulphur needs to be handled with care.
That’s right. Like other highly chemically reactive minerals, with reactivity comes risk – a great potency that requires careful consideration of both form and dose, so that we can harness this power for good not…well evil’s a bit strong…but how about, for not-good. I’m a bit of fan of Sulphur and using Sulphur strategies in my patients. I think it has interesting echoes with our past: the ‘healing’ waters of a Sulphur Spring and of course even further back the old ‘brimstone and treacle’ medicine of eons ago. This paper by Nimni in 2007: Are we getting enough sulfur in our diet? got me thinking about Sulphur again in a contemporary context, over a decade ago, I’ve done a lot more thinking, researching and prescribing since then but it seems that Sulphur still remains ‘unseen’ by most. But with the rise and rise and rise of popular Sulphur-based supplements (alpha lipoic acid, GSH, N-acetyl glucosamine, Brassica & Allium extracts and concentrates, N-acetyl-cysteine etc) I think it’s time to talk.
If you don’t have a clear picture of the gross daily requirements, determinants of altered individual needs, sources, regulation & associated deficiency picture of Sulphur, you’re not alone. Turns out this essential macromineral remains ‘unseen’ by most, even though you’re probably writing prescriptions everyday that have Sulphur as their key component. From the simple: Taurine, N-acetyl cysteine, Protein powders, to the sublime: Brassica extracts & concentrates, N-acetyl Glucosamine, Alpha Lipoic acid etc. In order to use these Sulphur strategies successfully and safely, however, we need to fill in the missing detail on its metabolism, the difference between the ‘organic’ and ‘inorganic pools’, how regulation regularly goes wrong, even in those seemingly consuming enough, and how to balance the risks of this reactive medicine with its substantial therapeutic value. This recording comes with a great clinical tool to help you at last see the Sulphur strategy most indicated for your patient.
The latest Update in Under 30 has landed!!!
You can purchase Unseen Sulphur – Time to Take a Lookhere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
I don’t know about you but I don’t count myself among the conspiracy theorists. While I may have been partial to the occasional one over my lifetime, you have my word, I never inhaled. Or at least not since I learned the practise of scientific enquiry and the application of critical thinking to all evidence. The two together tend to put a dampener on the whole: earth is flat & the moon-landing was a hoax…kind of notions. But there is one conspiracy I think all of us in nutritional medicine have been the victim of: The Calcium Conspiracy.
Not in the vein of speculations regarding excessive lobbying & undue influence of the Dairy Corporation on dietary guidelines. Nor even arguments that this has gone so far as to inflate the RDIs for this nutrient. Nope, I am actually good with the RDIs for this mineral. High level evidence confirms that our intake of Calcium was enormous even before the Agricultural Revolution, and therefore BD (Before Dairy) 😂
Man, those roots and tubers and other bushfoods sure were nutrient dense, not like the stuff we consume these days!
No, the Calcium Conspiracy we’ve all been lead to believe is that it is the boss. The boss of bones. The boss of the parathyroid. The boss of the other minerals. And especially the boss of Magnesium. While you might have heard me describe Calcium as a ‘bully’ in the GIT (let’s call this the slide 😅) and I stand by that, it is far from being the boss of the rest of the playground! In fact its regulation is largely at the hands of other nutrients..not naming any names…[Magnesium😳] So while, all of us trained in nutrition have had the significance of the Calcium-Magnesium relationship & the mantra “2:1, 2:1, 2:1” drilled into us, which we repeat at night to get ourselves to sleep (or did they mean to take not just ‘talk’ these minerals, to help with sleep?!) Our teaching created this conspiracy – a misperception that Calcium is the boss and Magnesium its long-forgotten lackey. Well guess who’s really calling the shots and on whom?!
Have you ever heard the saying, ‘It can take Magnesium to fix a Calcium problem”? I’ve not just heard it but seen it many, many times in my patients.
But how do you tell which patients need both and which ones, just one? It comes down to understanding the exquisitely sophisticated way Magnesium lords it over Calcium – via the parathyroid and Vitamin D metabolism and how we can see this patently in the pathology (regular screening labs) of your clients. I think there is a bias in integrative nutrition – we favour Magnesium – it goes into our supplement recommendations for so many of our patients and while the rationale for this is valid – all dietary surveys show magnesium under-consumption to be rampant in the SAD – I don’t actually think all of us know 1) how much we should be giving (yes there is a limit) 2) how to discern who needs what, in spite of a lack of a good Magnesium assay and 3) the true potency in the prescription when we get these things right or wrong! This study by Sahota et al is so far my favourite for 2020..it’s 14 years old and the sample size is small but its methodology and examination of when Magnesium can fix a Calcium issue and when it can’t, is superb. Together with about 50 other papers I’ve just imbibed…they’ve refined my thinking, tremendously. There’s a Calcium Conspiracy, alright, but just throwing Magnesium at everyone in arbitrary doses is not the solution…. “2:1, 2:1, 2:1…..”😴
There’s a conspiracy going on regarding Calcium but it’s probably not the one you imagine. We have been lead to believe that Calcium is the boss: the boss of the bones, of the other minerals and certainly of its often over-looked lackey, Magnesium. But the truth is, we have it all the wrong way round. There is a sophisticated synergism between these two minerals but the brains and the brawn in this relationship are held by the latter and we need to understand how to recognise when Magnesium is ‘pulling the strings’, to produce low calcium, in our patients and how to find the sweet spot of their synergy. This recording comes with a great resource to use in your clinic, with explicit redefinition of ‘what healthy looks like’.
Have you been told somewhere by someone that the ‘perfect’ TSH is 1.5 mIU/L? This is a wonderful, terrible & wonderfully terrible example of ‘magical numbers medicine’. As a push-back against the published reference ranges we’re given, that are so wide you could drive a truck through them, there has been an over-correction by some, leading to the myth of ‘magic numbers’. We can narrow the reference range substantially for many parameters with good rationale, make no mistake about that but once we start setting ‘aspirational goals’ that are explicitly rigid…well we’ve done 2 things 1) forgotten about the patient to whom this result belongs and 2) disregarded viewing each result as part of a ‘pattern’, that we must piece together and make sense of.
Back to TSH then… if my obese patient had a value of 1.5 mIU/L this in fact would be woefully inadequate.
Also too low for any patient, no matter their size, if their T4 is low and we’d like a higher value as well for risk minimisation in our elderly clients too.
But the same result would be excessively & worringly high in my patient who’s undergone thyroidectomy.
Being given a list of ‘magic numbers’ will never replace learning labs correctly. When we do this, we come to truly know that meaning can only be made of the markers when you can answer the following questions:
What is this (metabolite, analyte, binding agent, plasma protein etc)?
What do I know about its physiological and biochemical context – what is its role and regulation in the blood, what moves it and to what magnitude?
How have the reference ranges been determined for this lab – who am I comparing my patient to?
Therefore, what is the significance of a result that is: ‘normal’, ‘low normal’, ‘high normal’, below or above the range?
Does this value ‘fit’ with my patient?
What else could explain an unexpected result?
How strong is my level of evidence?
What do I need to do from here to confirm or refute this?
And a few more 😉
Realising the full value of any test result in terms of what it reveals about the person sitting in front of you, requires these skills. Unfortunately, in contrast a list of magic numbers will often lead you astray. And building your scientific knowledge about labs will not only help you avoid the pitfalls of pathology but will strengthen your pathophysiology prowess in surprising ways, saving your patients a packet in terms of additional extraneous testing and help you truly personalise your prescriptions…because the ‘invisible (biochemical individuality, oxidative stress, genetic probabilities, subclinical states, imbalanced or burdened processes etc) just became visible’. I started requesting lab results early in my career and years later was lucky enough to be taken under the wing of Dr. Tini Gruner. I found some of our shared notes, from 10 years ago, scribbled all over patient results recently and I was struck by just how lucky I was to have her encouragement to really pursue my interest and how she was a guiding force about learning to recognise pathology patterns over single parameters. A decade on I can confess, much of clinical and educative success has come off the back of this foundational skill-set and I know, this is true for so many I’ve taught too.
“The guidance I’ve received over the years from Rachel in relation to pathology interpretation has been one of the most valuable (and fascinating) investments I’ve made as a clinician. Her teachings have filled gaps in my knowledge base I never knew needed filling and have significantly enhanced my understanding of the inner workings of the body! Rachel has an incredible ability to make the numbers that patient’s so often present us with, both understandable and clinically meaningful. The knowledge I’ve gained by investing in this skillset has paid off in dividends and I’m certain will continue to do so into the future.”
Stacey Curcio – Cultivating Wellness
I hope you’ll join me for the most exciting up-skilling opportunity in learning labs yet. Oh…and all this talk about thyroid testing..that’s just a serving suggestion 😉 this year my MasterCourse is focused on the most routine labs of all: ELFTs, FBE, WCC, Lipid and Glucose Panels…an absolute treasure trove of free integrative health information about your patient!
This skillset has been found by many to be biggest ‘game-changer’ in Integrative Medicine!
There are limited places. To sign up for the MasterCourse: Comprehensive Diagnostics click here. For more information about the program click here.
Did someone explain the kidneys are like a really important, not to be forgotten, under-estimated, ignored or under-valued kind of organ in your training as a naturopath?No, me neither. I mean I know Buchu and Uva and Zea (on a first name basis only, clearly!) and …no actually, I’m done. But seriously, it didn’t take too long in practice to stumble across a whole lot of bad when kidneys aren’t getting the attention they warrant and equally to develop a slight obsession with renal markers in all of my patients not just because of their incredible impact on whole health but also because of what ‘lay beneath’.
As you might suspect, I get sent labs all the time from practitioners. Stop no! That is not an invitation!
Often it’s client’s renal markers which I do appreciate because it tells me there is an increasing number of praccies that absolutely have done some post-grad DIY knowledge building about these bean-shaped babies and their critical contribution to health. The results might come with a question like, “What’s going on with their kidneys?!” [insert worried face emoji of choosing]
To which my reply is often… “not much but boy do we need to talk about your patient’s GIT microbiome! [or] mental health! [or] sarcopenia!”
Say what? Yes abnormalities within the renal markers: urea, creatinine and uric acid may be a reflection of renal issues. But if you know where each of these molecules enters the blood,exits the body and all the interesting good & bad they can get up to in between…then the patterns speak less (if at all in some instances) to what’s going down in the kidneys but instead give you an incredible insight into key issues all over the body: from the gut to the brain. But wait there’s more! Want to know what’s the latest and greatest in management of advanced renal disease? Treat the gut to lower the urea. What about managing mania? Add in a gout treatment to lower uric acid. Dang! This is holistic health at its best with those poor kidneys no longer being left out in the cold!
“Who knew urea, creatinine, GFR and uric acid could be such a Goldmine….Mind…officially…blown!” New Graduate Mentee 2019
Most practitioners graduated with not much more than a few ‘kidney’ herbs and an under-appreciation of the contribution renal health makes to wellbeing. It’s not just about waste and water. In reality, the kidneys are pivotal in just about every major element: blood, bones, pH balance, methylation, control of oxidative stress, the GIT microbiome and more! And we are seeing the impact of this in our patients in all sorts of subtle and not so subtle presentations. This new instalment in diagnostics, brings the renal system into the spotlight so we can confidently identify and better manage its critical contribution. In addition to this, just like with other routine labs such as LFTs, we unpack how these so-called ‘renal markers’ can flag a plethora of other insights into your patients, from reflecting (un)healthy muscle mass to calculating individual dietary protein adequacy, from key ‘danger and distress’ signals in response to disturbed metabolism, oxidative stress to certain types of GIT dysbiosis! We call this Renal Markers: Explained, Expanded and Exploded because these routine labs can deliver XXX sized insights into your patients.
Do you know that saying, ‘mind your Ps and Qs?’ It basically means mind your manners and I heard that a lot as a kid 😉 But what we really need to hear now, as practitioners and promoters of healthy eating and wellness is really, Mind your P’s and P’s because a lot of biggest health consequences of any diet are determined by the balance or imbalance of two major players; protein and potassium. We’re always looking for simpler ways to enable patients and ourselves to be able to both recognise the strengths and weaknesses of their diets and, better still, apply a simple method to making better choices moving forward. Eyeballing the protein and potassium rich sources in any diet speaks volumes about other essential dietary characteristics and the likely impact of diet on health – and getting the relationship between these two right should be a goal for us all.
“World Health Organization (WHO) Dietary Targets for Sodium and Potassium are Unrealistic”, reads the recent headline from yet another study finding that humans would rather challenge the solid science of human potassium requirements than acknowledge the urgent need to turn this ship of fools around!
This large study, conducted over 18 countries, involving over 100 thousand individuals, reported that 0.002% met these targets. That’s 1 person in 50,000. Now, the researchers’ response to this is that we should lower our dietary potassium expectations….such that the targets are more achievable and so that (frankly) we are less perpetually disappointed in ourselves and our terrible food choices. Wha????Back up there. The WHO guidelines, just like any other nutrition authority, derived these minimum amounts from a thorough review of the science that speaks to our physiological requirements and the level of nutrients that have been shown to be associated with health. Australia’s own fairly conservative NHMRC suggests even higher amounts for good health! Perhaps rather than revise the established dietary targets we should revise what we’re putting in our mouth!
So where does protein come into this? Well one of the most important and central nutrient dynamics is the balance or imbalance of our intake of both. And in this regard, yet again, we have a surprising lot in common with plants! Whether you’re trying to understand optimal nutrition conditions for growth (nitrogen alone won’t get a plant there, nor protein alone in a human) or the intricacies and nuances of finely tuning our physiological processes such as cardiovascular function, renal health, blood glucose management etc. the answer lies in a happy marriage between these two.
In this area of nutrition, we should be listening most closely in fact to renal specialists/researchers. These ‘undercover’ protein and potassium experts have been talking about this for a long time and in particular, in my humble opinion, Lynda Frassetto has lead that charge for decades. If you haven’t read much on this issue and want somewhere to start at least, jump into her pivotal paper from 2001 which eloquently explains why the human design can not shoulder a potassium shortfall…well not without causing real health problems…like the ones we’re seeing in record numbers currently and why the protein potassium balance of any diet is a major health determinant. That’s why giving ourselves and our patients the knowledge and the tools (yes lovely shiny meaningful infographics included!!), to quickly determine their protein potassium balance, are so necessary and important.
Thanks to Frassetto and many other researchers’ work, looking at food through this protein potassium lens has sharpened my focus and I think it’s about time we all took a good look 🙂
Check out the latest UU30 to hear the latest information…
The health consequences of any diet are largely determined by the balance or imbalance of two major players & proxy markers; protein and potassium. When it comes to this area of nutrition, we should be listening more closely to renal specialists whose research shows why the human design cannot support a potassium shortfall and the health consequences of this. Whether you’re trying to understand optimal nutrition conditions for growth (nitrogen alone won’t get a plant there, nor protein alone in a human) or the intricacies and nuances of finely tuning our physiological processes such as cardiovascular function, renal health, blood glucose management etc. the answer lies in a truly happy marriage between our intake of these two. These recording comes with a clinical resource tool to help you quickly identify the dietary protein:potassium balance for your clients.
Hear all about it by listening to my latest Update in Under 30: Mind Your P’s and P’s For all Update in Under 30 Subscribers, it’s now available in your online account and if you are not a subscriber you can purchase this individually here.
As an avid reader of medical news I face a barrage of headlines both domestic & international everyday. I feel this is important for many reasons – not just so that I know what’s being said about their medicine but what they’re saying about ours as well! Anyone see the jaw-dropping headline last week: Could Probiotics be bad for your gut? Yep.
Now how many of you didn’t make it past the headline? It’s hard isn’t it.
There’s almost a reflexive shutdown for many of us to dismiss such a proposition as simply ‘ridiculous’, surely on par with our response to an article from a climate skeptic…as we shake our heads with ‘you gotta be joking right?’… but unless we read on, we’ll never know. (more…)
When I look back over how I’ve raised my kids there are a few serious ‘what tha…’ moments – like the time I thought shopping with a child in rollerskates was doable…I mean she loved those rollerskates and she was amazingly agile and good…just not quite good enough to hold onto that 1L Biodynamic Yoghurt sufficiently…who knew?! Dietary wise, I can look back and be critical in hindsight about different details, the contents of our fridge and pantry have morphed over the years with my changing knowledge (money & time!) but there are a few things I can confidently say – ‘Nailed it’, accompanied by a fist pump! We’re all meat eaters, not carnivores by any stretch of the imagination but we do partake, however the kids and I were just reflecting the other day on the absolute constancy of legumes in our life. (I know you want CCTV footage of our dinner time chats now don’t you 😉 ) There would rarely be a day in our house without them…several times!
Now I sound like I’m showing off but trust me it’s not that impressive or exotic – it goes a little something like this: soup,(split red lentils or cannellini), bolognaise & lasagne (1:4 brown lentils with the meat), nachos for school lunches (kidney beans 4:1 with mince), falafel & hummus (chick peas) & tofu (my kids love this stuff for snacks often & for mains at least once a week).
Ok now everyone relax, I don’t make our own almond milk, grow our own vegetables or ferment stuff…see…it’s swings & roundabouts 😉(more…)
Help!!! I’m about to share the stage at the 3rd International Acid-Base Symposium on the 25th-27th Jun, with the best acid-base researchers in the world, all of whom I actively stalk (well read and recite everything they’ve ever published but close enough!) I’m terrified and excited in equal doses…but urgently need to change my presentation approach because until now I’ve had the privileged position of simply fulfilling the town-crier role, announcing far and wide the findings of theirincredible research into acid base physiology and their findings about impact of chronic mild metabolic acidosis. But I can’t quote Arnett to Arnett! I can’t tell Dawson-Hughes about the incredible insights of Dawson-Hughes’ large body of work in this area! Oh my Goodness (cue, shaking knees), I’m going to meet Thomas Remer…of Potential Renal Acid Load Formula Fame!!
Yes, my partner is a musician and through him I have brushed shoulders with all kinds of famous…but nothing that has made my heart beat quite this fast!
No, I haven’t gone crazy for the ‘caped crusader’… but I thought that would get your attention…. oh look it did! 😉
I’m off to Melbourne for the ACNEM Conference May 5-6th and Batmania was one of the interim names of this very cool and happenin’ town before it became known as Melbourne in 1837! Things have certainly changed in nutrition and the environment since then and as practitioners we now need to address sometimes very complex dynamics between genes, gut, nutrition and environmental health. Which, luckily enough this conference is all about!
This year’s theme for ACNEM is Health for Life – Mastering the Integrated Approach.
I am fortunate to be included in the exceptional speaker line-up (thanks for lovely sentiments many of you have expressed so far about that 🙂 ) I am presenting on ageing..which many of you know that I am suddenly now very interested in…getting old and all.
Can you help me out here? My memory has failed me. Someone, somewhere (Mel? Syd? Auckland? Online during a mentoring session? In a Mullumbimby supermarket?!), in the past month asked me for this paper documenting the increased pain perception reported by subjects given IV saline with a slightly acidic pH compared to a neutral preparation. Quite an extraordinary illustration of the potency of small pH changes in the ECF and the impact this can have on our pain perception.This study is one Professor Vormann has previously talked about and as I’m touring with the fabulous German Professor right now I said, ‘Sure!’…then seemingly instantly erased from my mind who made this request! Is it you?
This month is a fabulous blur of travelling & speaking, getting back face to face with everyone at a bunch of seminars & conferences, which I love but I do forget some days where I am, who I am and exactly what I have promised and to whom!(more…)
…Chronic Kidney Disease (CKD) that is! That’s the ad we really need broadcast on prime time tv. On par with osteoporosis and other conditions that ‘seemingly appear out of nowhere’ in people’s 60s and beyond, there’s a potent combination of ignorance (patients) and denial (health professionals) at play it seems, when it comes to discussing the earliest signs of CKD that typically start decades before you’ll ever get a ‘diagnosis’. Being specialists in preventative health care – this is something we need to have firmly on our radar in terms of early identification and also in our repertoire when it comes to risk reduction. Most of us know about water intake and all the medical risks for renal impairment but are we equally onto the critical role that mild acidosis plays in driving this condition?
I’ve been travelling a lot for work lately, so in my absence my teens have been under the influence of others and as a result they’ve returned with new & improved habits. This one is gold:
1 egg + 1 banana
beat egg & add to mashed banana
pour into a hot pan, coated with small amount of oil
flip and serve with youghurt and fresh berries(more…)
Ever got to the end of a day or a week and felt like this? Or woken up to find your skin looking like this?! Just quietly, me too. When my son was about 3 he was sitting in the back of my car with my mum (she would have been in her early 70s) and he asked how people get wrinkles. We told him it was from having a fun life with lots of laughter, to which he replied out loud while still staring intently at my mother’s face, ‘Wow Grandma! You must have had the best life ever!’ I digress.
I personally am not a crusader of anti-ageing (seen my pics recently?!!) but my recent research into effectively reducing Advanced Glycation End-products (AGE) via the diet, to in turn potentially lower both my risk of tuckshop arms AND just about every other disease you can name (cardiometabolic, neurodegenerative, psychiatric, malignant, you name it), got me sitting up and paying attention!(more…)
My partner and I have a well rehearsed script whenever he is suffering from man flu, he says, “Am I going to die?” and I say “Yes, just not today.” First world peoples tend to specialise in the denial of several absolutes: like time & death. As Professor David Cameron-Smith, from the University of Auckland says, ‘old’ is something we always define as ‘other’. We are not old but we know people who are!I personally used to define ‘old’ as over 50 until that became rather close and uncomfortable at which point I noticed a completely unconscious increase in the lower limit! Now old is over 75 yrs…and stay tuned for more updates 😉
Scenario: Run into friends of friends who join us in the sunshine for a cuppa & we’re discussing the finer details of chai (western version V the real streets of Delhi stuff), tumeric lattes etc etc. as you do. I comment on how unpleasantly strong I found the cow’s milk in those downtown Delhi chais we had when we were there.
50 something man: Oh I LOVE that – I just LOVE cow’s milk. I drink loads of the stuff. I used to drink 2L a day but now it’s more like 1L a day.
Me: Seriously?
50 something man: Absolutely. Then there’s the cheese as well – I would eat at least 1kg of that a week. But it’s good for my bones, right? I have that thing, you know, before osteoporosis…brittle bones.(more…)
Recently, while I was touring around the country talking all things Acid Base (!), I spent a bit of time talking to practitioners about the limitations of our current protocols and assessment tools for detecting ‘Bad Bones’. I was surrounded by a sea of nodding heads and when I offered a solution in the form of additional bone health markers, I could see light bulbs going on all over the room 🙂
We all appreciate that osteoporosis develops over a lifetime not overnight, yet the current screening recommendation in most countries suggests that women at the ripe old age of > 65yrs and men >70yrs undergo their FIRST (!) BMD scan! The only exception to this rule is that they recommend an earlier scan in those individuals at high risk…ahem….does anyone here not have their hand up?? (more…)
You might have heard me talk about using an ‘upstream’ rather than ‘downstream’ approach in nutrition – the concept is very naturopathic… look at the water source and address things there rather than just tweak things downriver! One of the most important upstream influences on patient health & wellbeing I can think of is systemic pH – the body’s constant struggle to neutralise its overwhelmingly acidic input, which comes from both metabolism, inflammation, stress and of course unbalanced diets.
It’s a war out there and most of our patients aren’t winning! (more…)

















 Recently, while I was touring around the country talking all things Acid Base (!), I spent a bit of time talking to practitioners about the limitations of our current protocols and assessment tools for detecting ‘Bad Bones’. I was surrounded by a sea of nodding heads and when I offered a solution in the form of additional bone health markers, I could see light bulbs going on all over the room 🙂
Recently, while I was touring around the country talking all things Acid Base (!), I spent a bit of time talking to practitioners about the limitations of our current protocols and assessment tools for detecting ‘Bad Bones’. I was surrounded by a sea of nodding heads and when I offered a solution in the form of additional bone health markers, I could see light bulbs going on all over the room 🙂