It’s no secret I am in the midst of some serious deep-diving through the micronutrient evidence base & at a depth of about 30 metres I struck Boron! Don’t yawn! I saw that. Thinking, ‘boring’, when we hear, ‘Boron’, is almost as bankable as watching everyone reach for their water bottles when you mention anything hydration-related 🤣 But I am here to restore your positive regard for this mineral and remediate its bad (& boring) rep! In preparation for the Nutrient Prescriber’s Program we started each nutrient review with the seminal contemporary nutritional texts and then launched ourselves headlong into the latest & greatest research. By the end of all the Boron bits in all my trusty texts the yawn was not gorn! But the moment I started reading the research I was like, ‘Are we even talking about the same thing?!’Turns out we’re not 😵🤦♀️
You see Boron has been a longstanding victim of identity theft. What we’ve been lead to believe is Boron is weed-killer and ant-poison and look it does give us some of the benefits of Boron but not all. And it possess a pharmacokinetic & toxicity profile that naturally occurring Boron simply does not.
Who decided that the Boron that is ubiquitous in our environment but almost exclusively consumed by us only after biotransformation by plants – could just skip that last bit and still be safe and optimally beneficial?! Probably the same guy that came up with folic acid, may I suggest? Anyway, enough is enough. We all need to relearn Boron – naturally occurring Boron – in the form of Sugar Borate Esters (SBE)- the evidence of benefits for which will blow all of our little minds! Well it certainly blew mine! Looks like this natural form of Boron is going to hit the Australian market in the not-too-distant-future 🐦 can’t wait to see which supplier is sufficiently progressive and research-aware that they bring this to market, having been available as a high grade supplement, employed in numerous RCTS OS for some time. But this little Update in Under 30 is not waiting around for that release date – there is much to be gained from SBEs right now – so make some noise as the real Boron at last takes the stage!🎤
Boron has been the victim of longstanding identity theft and we unknowingly have been interacting with its imposter. Contrary to everything you’ve ever been told about this mineral, naturally occurring Boron is full to overflowing with benefits for our gut, our bones, our brain, our management of other minerals and is safe in large quantities. That ‘bad guy Boron’ you were introduced to and is still present in many of your supplements is a form we never consume in food…and therein lies a world of difference! Come meet the real Boron so you and your patients can get the real benefits!
You can purchase The Boron Deception: How We’ve Been Fooledhere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
Heck yeah. It’s going to take a lot more than 1 push-back post to turn this ship around! Likewise, I was only getting started with my recent Update in Under 30 episode, ‘What’s Hiding Behind Histamine’ 🤓😂 & part 2 has just been released where we unpack the case of a 41yo female with chronic diarrhoea, multiple food reactions, very high stress and very high oestrogen. Sounds like she’s a walking Histamine Headline – except she isn’t.
Right now we really do need to keep this conversation going such that a healthy discourse can help us deconstruct the histamine dogma.
I know I’m showing my age here, but anyone remember when Candida was having a ‘moment in the 90s? Ok, so that ‘moment’ stretched to over a decade of a ‘Candida-contagion’. No one could eat melons or mushrooms, eat ferments or feel joy. It was a bleak time that did our profession some reputational damage. Not only because seeing an ‘alternative practitioner’ became synonymous with being put on an unbearable, unattainable restrictive diet and positioned practitioners as peddlers of punishment but also because it took some time for science, in the form of accessible (& always improving) assessment methods, to come along and save us from the folly of the 1-diagnosis-for-all mentality.
Let me ask you, how many times do you actually see Candida overgrowth on reports from stool testing performed using best practice modern methods?
In my experience – never – not as a stand-alone issue. Occasionally, as part of the overgrowth of a suite of opportunistic organisms where the real-take home is the need to ‘remove the opportunity’ via the promotion of more good guys. So not only was the diagnosis incorrect, the proposed treatment for it was a complete misdirection as well.
Can’t help thinking in the current climate of Histamine Hysteria that history is repeating itself.
How will we all individually, and as a profession, respond this time?
In this follow-up episode we observe how the 3 key elements often hiding behind a histamine intolerance diagnosis: Misunderstandings, Missed Messages & the potential for Mistaken Identity, have played out in the case of a 41yo female who presents with chronic diarrhoea, a long list of problem foods including now a suspicion of ‘histamine foods’. Rachel offers up new ways to approach the patient work-up that cut through the ‘noise’ and enable us to better identify what is hiding behind histamine in similar cases of marked gut dysfunction.
You can purchase What’s Hiding Behind Histamine? – Part 2here. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account. You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
You’re invited to attend acnem’s 2023 Annual Conference ‘Long COVID, Navigating the Complexity, A Clinician’s Roadmap’.
Saturday 29th & Sunday 30th July 2023, Melbourne. Both face-to-face and online.
To get 25% off acnem Annual Conference USE CODE: acnem25
What level of Serum Ferritin represents ’empty’? As in complete depletion of iron stores?
Is it any value below the minimum of the reference range? e.g. < 30 mcg/L Or does the bottom of the reference range allow for a buffer and ’empty’ is substantially lower than this? Could patients actually be ’empty’ but still have Serum Ferritin values within the normal range? Could the same Serum Ferritin value occur in one patient on ’empty’ but with adequate stores in another?
Have you been told somewhere by someone that the ‘perfect’ TSH is 1.5 mIU/L? This is a wonderful, terrible & wonderfully terrible example of ‘magical numbers medicine’. As a push-back against the published reference ranges we’re given, that are so wide you could drive a truck through them, there has been an over-correction by some, leading to the myth of ‘magic numbers’. We can narrow the reference range substantially for many parameters with good rationale, make no mistake about that but once we start setting ‘aspirational goals’ that are explicitly rigid…well we’ve done 2 things 1) forgotten about the patient to whom this result belongs and 2) disregarded viewing each result as part of a ‘pattern’, that we must piece together and make sense of.
Back to TSH then… if my obese patient had a value of 1.5 mIU/L this in fact would be woefully inadequate – so too a child at any weight.
And we expect a higher value as well in our elderly clients too and this level there may be, in fact, increased mortality.
But the same result would be excessively & worringly high in my patient who’s undergone thyroidectomy.
Realising the full value of any test result in terms of what it reveals about the person sitting in front of you, requires these more thinking and more thoughtfulness. Unfortunately, a list of ‘magic numbers’ will often lead you astray. And building your scientific knowledge about labs will not only help you avoid the pitfalls of pathology but will strengthen your pathophysiology prowess in surprising ways, saving your patients a packet in terms of additional extraneous testing and help you truly personalise your prescriptions…because the ‘invisible (biochemical individuality, oxidative stress, genetic probabilities, subclinical states, imbalanced or burdened processes etc) just became visible’. I started requesting lab results early in my career and years later was lucky enough to be taken under the wing of Dr. Tini Gruner. I found some of our shared notes, from 10 years ago, scribbled all over patient results recently and I was struck by just how lucky I was to have her encouragement to really pursue my interest and how she was a guiding force about learning to recognise pathology patterns over single parameters. A decade on I can concede, much of my clinical and educative success has come off the back of this foundational skill-set and I know, this is true for so many I’ve taught too.
“The guidance I’ve received over the years from Rachel in relation to pathology interpretation has been one of the most valuable (and fascinating) investments I’ve made as a clinician. Her teachings have filled gaps in my knowledge base I never knew needed filling and have significantly enhanced my understanding of the inner workings of the body! Rachel has an incredible ability to make the numbers that patient’s so often present us with, both understandable and clinically meaningful. The knowledge I’ve gained by investing in this skillset has paid off in dividends and I’m certain will continue to do so into the future.”
Stacey Curcio – Cultivating Wellness
I hope you’ll join me for the most exciting up-skilling opportunity in learning labs yet. Oh…and all this talk about thyroid testing..this next MasterCourse series is focused on revolutionising your understanding of thyroid, adrenal, HPT & HPA markers based on the very latest research & findings & marry these together with everything you learned in MasterCourse I (ELFTs, FBE, Lipids & Glucose) to understand the ‘whole story’.
…an absolute treasure trove of free integrative health information about your patient!
DEEP DIVE INTO REAL CASE STUDIES TO DEMONSTRATE EACH PATHOLOGY PATTERN IN ACTION. ]\
There are limited places. To sign up for Rachel’s LIVE Series – MasterCourse II: Thyroid & Adrenal Diagnostics and for more information click here.
One of my dear friends told her husband several years ago that she had noticed he was now making, ‘old man noises’ upon standing up from couches & chairs. She told him that must simply stop. She pointed out that he was only 50 and that she neither could nor would listen to that for another 40 years!
He stopped!
But aging and old (wo)man noises are coming for all of us, right? And by the time we’re making those noises or excusing ourselves from certain activities due to sore, dodgy or NQR [insert joint or body part], we’ve spent several decades unknowingly right on course to get here! We don’t generally pay any attention to our ECM (extracellular matrix) which suffers in silence, slowly but surely losing its structural & functional integrity from the age of 18 on, until we reach the tipping point: joint degeneration, repetitive soft tissue injuries etc, and a problem that will never be silent again! Cue your choice of anti-inflammatories it seems – til death do us part!
The Ageing Matrix is a thing.
And no I haven’t seen the movie – I don’t need to – I’m living it.
When I was pregnant I thought I wanted to specialise in pre-conception & pregnancy care. Then my babies arrived and I took a fancy to paediatrics. Sound familiar to anyone? Now, unsurprisingly, I have a real thirst for knowledge expressly aimed at bettering this whole ageing-thing! So in preparation for this Update in Under 30 episode, I’ve relished the opportunity to put the Ponds Institute & all similar cosmetic companies on notice! Scrutinising their claims that every woman on the planet would do better with more Collagen, more Elastin, more Hyaluronic Acid, just more of every key ECM component really. Ok, but in accordance with my bias and my business, my lit review pertained to oral supplements, not outrageously priced magical middle-life-crisis rubs and the therapeutic action I had in mind was the integrity of our ECM, and the roughly 2kg of collagen, we rely on, for functions a lot less frivolous than stopping sag. I have to say, I started out as non-believer but the research was quite the awakening…still there’s a lot to unpack here in order to repack our ECM and prevent against the erosion of its integrity and everything we build, and rely on, upon it – to live well!
Osteoarthritis (OA), like osteoporosis, is a diagnosis made after decades of disease. Underpinning it all, is our aging Extracellular Matrix (ECM) with its characteristic compositional change that leaves us vulnerable, from the ripe old age of 18! The ECM, like all other tissues, is made from basic building block nutrients but presented in their most fanciest of forms with triple helix structures, aggregates and other large molecular weight components, that each possess remarkable physico-chemical properties & convey extraordinary functionality to structures like joints. But is prevention against, and effective intervention for, OA as easy as consuming more of these ECM biomaterials?
You can purchase Supplementing Collagen & ECM Biomaterials – What’s the story?here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
I’ve spent the best part of about 4 months recording my *NEW* Advanced Thyroid Assessment training. I told my team this would be easy and quick, given it was to be based on a great little 2-part, 2hr updated presentation I delivered just last year for ACNEM!! Sixteen weeks (like seriously…most of it) numerous rewrites and retakes later, our final product is 4 parts that goes for over 12hrs in total & has a bonus Adrenal recording! And yeah my team are impressed but unimpressed too if you know what I mean?!🙄🤪
Every time another, ‘Oh wow!’, or ‘No way!’, escaped my lips, it was a source of personal celebration, as another deeper layer of learning revealed itself.
But to the wonderful, somewhat weary and definitely wary Sally, who does all my powerpoints, it was met with, ‘Oh boy!’, because it meant many multiple new slides to build full of visual metaphors, animation acrobatics, if not an entire new Part!*#@^
Her sage advice along the infinite research road I’ve been travelling was : ‘Stop. You’re going to have to stop.’
So I didbut now I am this meme. Everything I see currently through the lens of thyroid health, I talk in tongues TFTs and my brain is one giant neural network of integrative endocrinological circuits! I have fallen in love with this topic, this neuroendocrine axis and its ‘first responder’ role all over again! Hence our little thyroid character below – all ‘antennaed’ up – is one of the many tools we’ve developed for this training, to teach us that ‘bad thyroids’ per se are extremely rare – but bad scenarios are common (too much or too little of any macronutrient, key micronutrients, a change in the internal or external environment etc etc) and this little fellow and his board of directors (no – not the hypothalamus or pituitary!) – well it’s their job to ‘read the room’, right?!
In the absence of this key understanding we risk: A lot of lazy labelling in thyroid health – ‘You have a bad thyroid – that’s why you…[can’t lose weight, feel tired, have SIBO etc]’ Misdirected treatment & especially a tendency to overload the butterfly with ‘thyroid’ nutrients – which can do more harm than good
I’ve said many times, ‘perfect number pathology is a myth’ but it runs rife in practitioners’ beliefs about TFT results with complete disregard of the person those labs belong too! Did you know, for example, that your TFTs should all be higher if your BMI is? That your T4:T3 ratio should never be 3:1 if you are on replacement, have hot nodules, are pregnant or are acutely unwell etc etc etc? How about how low your Selenium or Iron levels need to be before this factor will influence the actual levels of thyroid hormones measurable – & what the impact of these deficiencies are well before then that is far more sinister and serious? Yep…you see here I am, pouring just some of the tiny take-homes of Advanced Thyroid Assessment ALL over you!
Watch this space my new Thyroid training is just around the corner!
An increasing number of our patients have thyroid concerns but unbeknown to many of us the most likely explanation of all is thyroid nodules, whose incidence is on the rise globally. The development of nodules has always been primarily viewed as a nutritional disease. Traditionally attributed to chronic iodine deficiency but recently novel nutritional causes have emerged. Benign nodules come in 2 flavours: hot and cold and while patients can present with a mixture, it is the presence or absence of a hot nodule that radically changes what complementary medicines you can and can’t use and what an effective treatment plan looks like. The pointers, as is often the case, are there for us in the patient’s presentation and pathology, so knowing the difference is no longer a guessing game. This UU30 comes with a great visual clinical resource and includes key papers on the nutritional management of nodules.
There are some things we say so often to patients we could record them and just press <PLAY> Like this daily dogma: ‘When you’re under stress, your demand for Magnesium rises and then in turn that can make you more susceptible to further stress, so we’re going to give you some to support you’. But is this actually the whole story? You guessed it, no. (I know I am fairly predictable like that 😅)
Recently, a personal new record – a patient reported ongoing daily use of a very high dose Magnesium ‘practitioner only’ product 8 years after it was prescribed by her then naturopath – and guess what, the patient still hadn’t reached nirvana* not the band! – a transcendent state in which there is neither suffering, desire, nor sense of self
Jest as I may – I think this raises some serious questions. The pervasiveness of our prescriptions when patients are not given an end-date coupled with ongoing access. How (not) effective this intervention was if someone perceives ongoing undiminished dependency on it. And specifically with Magnesium – whether our prescriptions (form, dose, adjuvants, advice) are the problem? If stress is synonymous with a shortfall of this mineral then Magnesium is not a solution to stress itself but the amplified stress response and the stress still requires its own redress, right? But do our patients hear this as well when we press <PLAY>?
Likewise – the BIG doses per serve being recommended might make sense for the minority (seeking potential NMDA antagonism) but are a real mismatch with the majority, who are just stuck in the stress loop and weathering a perfect storm of Magnesium under-supply and increased demand.
I love my minerals as much as, ok more than, the next practitioner but I’m always keen to refine my repletion approaches and oh yes, by the way, there is good data, a meta-analysis in fact, examining how long it takes to achieve repletion using oral Magnesium – and guess what, it’s not 8 years! The latest Update in Under 30 goes into all this and much MuCh MUCH more…you’re welcome 😂
Practitioners working with nutrition appreciate that Magnesium is vulnerable to depletion by the stress response and that in turn, can make people more prone to stress & keep patients stuck in a so-called ‘stress loop’. But do we understand the intricacies of this and how we, as practitioners, can get stuck in another kind of loop – one of endless Magnesium prescribing without reaching repletion? We discuss ways to improve your Magnesium prescriptions – in particular, ‘doping Vs drip-feeding’ and other things to assess & address if the long road to repletion risks becoming an endless one!
You can purchase Magnesium – Stuck in the Stress Loophere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
If I could be granted 1 wish regarding all health professionals, it would be that we were all competent in reading Iron Studies. Think that’s overstating the issue? Or not a bodacious enough way to ‘spend’ my wish? I don’t. Especially when you consider the impact of GPs in this space.
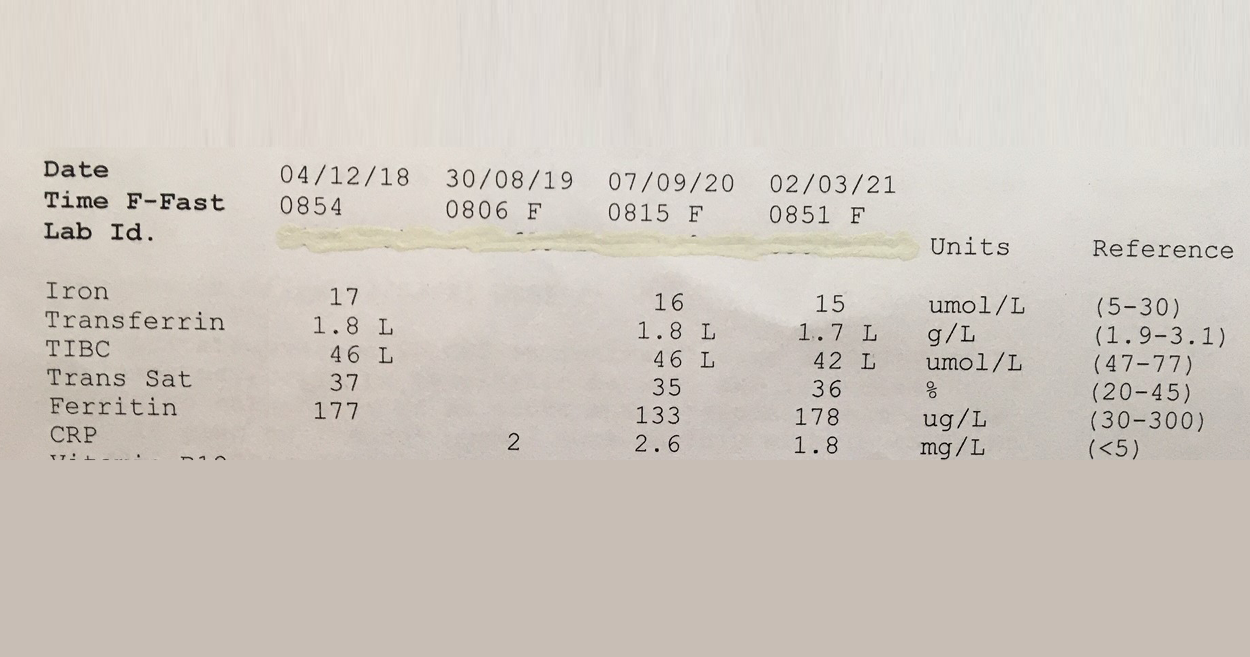
This 57Y male was asked to make a follow up appointment with his doctor, to discuss his ‘abnormal’ results which he was informed constitute Iron deficiency. Consequently he was was advised to start an iron supplement! #@!*
Your thoughts? Revoke this doctors medical licence? Insist on some very du jour ‘re-training’ at the very least? I mean, if you think this Iron pattern flags a deficiency or shortfall, then you’re as good as reading a map upside down and back to front…and written in a foreign language!! The ‘Ls’ in his latest labs flag he has suppressed transferrin, indicative of negative feedback inhibition of GIT uptake of this mineral, secondary to healthy stores or inflammation. And it’s not just that more iron is not indicated but that more iron in fact presents a patient like this with increased and unnecessary risk: to their microbiome, intestinal wall health, even according to the larger longer studies a potential correlation with colorectal cancer risk, if taken long term. Let alone the whole cardiovascular conundrum. Better still this same patient was told a few years back that he might have iron overload! Again the ‘map’ could only have been being read, upside down, back to front to reach such a conclusion!
So the one patient in just a few years by 2 different doctors has been diagnosed incorrectly with 2 different iron issues. Yep.
And sadly I have sooooo many more cases of missed and mis-diagnoses with regard to this mineral. The latest RCPA Position Statement on the Use of Iron Studies, underscores that assessment of iron status and GPs competence in knowing when to do this and how to interpret, is an important part of core general practice. Given it “is the commonest nutritional deficiency state in Australia and is significantly under-diagnosed” This succinct document offers a quick crash course in Iron nutrition for doctors and it hits all the right marks with advice about not ordering ferritin as a stand-alone because “the interactive nature of the three components allows for more accurate interpretation”and this simple but sage advice:
“Transferrin, iron transport protein, tends to increase in ID… A better strategy (than being tricked by Serum Fe) is to report transferrin saturation. A low transferrin saturation in the setting of an equivocal ferritin level is suggestive of iron deficiency. An elevated transferrin saturation is the first manifestation of iron overload.“
I mean seriously, do doctors read these RAGCP resources & recommendations, or is it just me? 🤓😂
Need a rip-roaring review on how to really read iron studies? Or know another health professional who does?!! Consider this Easter Educational Gift Instead of Eggs!! So You Think You Know How To Read Iron Studies?
Overt Iron Deficiency Anaemia or Haemochromatosis aside…do you understand the critical insights markers like transferrin and its saturation reveal about your patients iron status? Most practitioners don’t and as a result give iron when they shouldn’t and fail to sometimes when they should. This audio complete with an amazing cheat sheet for interpreting your patients Iron Study results will sharpen your skills around iron assessment, enabling you to recognise the real story of your patients’ relationship with iron.
When I deliver foundational nutrition training to GPs I talk tough. It’s a tough field, right? Compared with the relative certainty of pharmaceuticals, their established pharmacokinetics, their sophisticated delivery systems to ensure high bioavailability…trying to fix micronutrient deficiencies in patients can feel a lot like you’re trying to perform minor miracles. Take iron for something different, its homeostasis pivots on its tight regulation at the gut wall – and this is a wall that is very tight!! At best you get about 10% of a supplement taken up, at worst you get none and the harder you push & the higher you go with your dose…the lower the fractional uptake. Tough stuff, right?!
It’s about at this point in my talk I read their collective minds and say, “I know, you’re thinking, oral supplementation is for suckers – what about we bypass that road block and use IV?!” [Ok, I definitely use nicer words than this]
And then I put up a list of pros and cons about IV micronutrient repletion: ‘100% bioavailable’ & ‘Bypasses the body’s regulatory systems’, go on both! You see, time & time again we discover, when we think we’re outsmarting the body, it still manages to outsmart us. There are some exceptions to this – some nutrients (Vitamin C) and some contexts (late pregnancy iron deficiency) but the broader promise of ‘rapid replenishment’ for everyone, in your lunch break, via an IV infusion..is not realistic, responsible nor without risk. Don’t get me wrong, I am an advocate of appropriate IV Fe use and have encouraged a small fraction of my patients to take this path. However, given the dramatic rise in prescriptions for this since 2013, I think it’s time to stop and seriously review each element: In reality what does it achieve and in whom is it a responsible recommendation; Was a risk benefit analysis performed for & communicated to each individual & was the remaining risk mitigated?
Think anaphylaxis is the major concern? It might be the most lethal but there are more serious concerns due to higher incidence with newer preparations.
So, how well do you know your different IV iron forms, and their predilection for potential problems? And have your answers ready to all the questions raised above? In order for all involved to make an informed choice (both practitioners and patients), we must.
You’re welcome 😉 and hey welcome back to tough talkin’ Tuesday…
While rates of iron deficiency and related anaemia continue to grow, the increase in prescriptions of IV Fe have expanded exponentially in western countries. What is behind this change in practice regarding how we treat iron deficiency and does it match with responsible prescribing? Do the benefits always outweigh the risks? And while we’re on the topic, who is most likely to benefit and what are all the risks? In light of a current class action in the US, relating to a lesser talked about adverse event associated with IV Fe and recent complaints here in Australia against GPs, allegedly due to inadequate information to enable informed patient consent…it’s time to answer these questions and more. When is IV Fe a means of rescue and when is it a risky repletion strategy with no evidence of advantage?
You guys know I can’t help myself. For the last year or so I’ve been immersed in developing and redeveloping and redeveloping 🤓 [ahem apologies to my team!!] teaching tools for all practitioners to better understand what the routine renal markers can offer us in terms of understanding our patients…and it is far above and beyond renal function, promise. Just one example of this, is the sophisticated yet incredibly simple urea to creatinine ratio calculation that I was originally taught by Professor Mel Sydney-Smith. In adults with preserved renal function, this is the key to the kingdom, in terms of being able to objectively quantify whether patients are truly meeting their own individualised protein requirements. The Marvellous Mel (well he is, who can argue with that?!) added this one to my toolkit a long long time ago and in turn, I’ve been using it and spruiking it ever since.
In fact, I just lost 30 mins of my life listening to myself (ewww) in an old Update in Under 30 from 2013 that I recorded on this very topic.
[Sigh] I sounded so youthful…and…about 7 years younger too in terms of experience with this crafty calculation in the hundreds of labs I have encountered since!
My reliance on this ratio has remained but my wisdom regarding how to apply it has widened….and so, as I prepare to initiate another hundred or so practitioners into this secret sect 😉 via our current MasterCourse in Comprehensive Diagnostics, I couldn’t help myself and decided to re-record this UU30 episode: Using Urea & Creatinine as Markers of Protein Adequacy and also throw in a new pdf resource to boot [once again, ahem,apologies to my team!!] You see our ability to identify protein adequacy without this tool relies on the rather-rudimentary-‘rule’ that your protein requirements increase linearly with your weight…that’s the whole g/kg body weight thingo, right? But what if your weight gain is ‘all adipose’ Vs ‘mega muscle’ – are the protein requirements really the same for both people? Absolutely, not! This calculation enables us to step away from the rough approximation of the RDI and be able to determine if each individual is meeting their genuine requirements as driven by their own unique muscle mass hunger…oh and it reveals a few other very helpful things along the way to boot!
But this simple calculation comes with some caveats: 1. there are people and presentations in whom this calculation is not appropriate or accurate 2. because there are no magic numbers, right, it is about matching your labs with the patient in front of you and 3. looking (as always) for patterns.
…and a word of warning to the uninitiated: You’re going to love it!
So for those of you who are already Update in Under 30 Subscribers…happy Wednesday! Because you always benefit from any updated recordings etc. you’ll find this rejigged resource is already in your Active Content and for those of you who may have purchased this as an individual recording in the past, the same applies. And for anyone else keen to make some real meaning out of the most routine labs we see over and over again, and understand a whole world more about what they tell us about our patients’ muscle mass health, trajectory and the dietary protein piece of this puzzle…you might want to check this out too! And for those of you who think ‘total protein’ on a patient’s blood test results reflects ‘total protein’…boy have I got news for you!!
This comprehensive analysis of two standard indicators, urea and creatinine, that are often part of the patient’s standard blood chemistry tests. These commonly available results can provide insight into protein ingestion and uptake as well as muscle mass and, in extreme cases, kidney and liver function.
Have you been told somewhere by someone that the ‘perfect’ TSH is 1.5 mIU/L? This is a wonderful, terrible & wonderfully terrible example of ‘magical numbers medicine’. As a push-back against the published reference ranges we’re given, that are so wide you could drive a truck through them, there has been an over-correction by some, leading to the myth of ‘magic numbers’. We can narrow the reference range substantially for many parameters with good rationale, make no mistake about that but once we start setting ‘aspirational goals’ that are explicitly rigid…well we’ve done 2 things 1) forgotten about the patient to whom this result belongs and 2) disregarded viewing each result as part of a ‘pattern’, that we must piece together and make sense of.
Back to TSH then… if my obese patient had a value of 1.5 mIU/L this in fact would be woefully inadequate.
Also too low for any patient, no matter their size, if their T4 is low and we’d like a higher value as well for risk minimisation in our elderly clients too.
But the same result would be excessively & worringly high in my patient who’s undergone thyroidectomy.
Being given a list of ‘magic numbers’ will never replace learning labs correctly. When we do this, we come to truly know that meaning can only be made of the markers when you can answer the following questions:
What is this (metabolite, analyte, binding agent, plasma protein etc)?
What do I know about its physiological and biochemical context – what is its role and regulation in the blood, what moves it and to what magnitude?
How have the reference ranges been determined for this lab – who am I comparing my patient to?
Therefore, what is the significance of a result that is: ‘normal’, ‘low normal’, ‘high normal’, below or above the range?
Does this value ‘fit’ with my patient?
What else could explain an unexpected result?
How strong is my level of evidence?
What do I need to do from here to confirm or refute this?
And a few more 😉
Realising the full value of any test result in terms of what it reveals about the person sitting in front of you, requires these skills. Unfortunately, in contrast a list of magic numbers will often lead you astray. And building your scientific knowledge about labs will not only help you avoid the pitfalls of pathology but will strengthen your pathophysiology prowess in surprising ways, saving your patients a packet in terms of additional extraneous testing and help you truly personalise your prescriptions…because the ‘invisible (biochemical individuality, oxidative stress, genetic probabilities, subclinical states, imbalanced or burdened processes etc) just became visible’. I started requesting lab results early in my career and years later was lucky enough to be taken under the wing of Dr. Tini Gruner. I found some of our shared notes, from 10 years ago, scribbled all over patient results recently and I was struck by just how lucky I was to have her encouragement to really pursue my interest and how she was a guiding force about learning to recognise pathology patterns over single parameters. A decade on I can confess, much of clinical and educative success has come off the back of this foundational skill-set and I know, this is true for so many I’ve taught too.
“The guidance I’ve received over the years from Rachel in relation to pathology interpretation has been one of the most valuable (and fascinating) investments I’ve made as a clinician. Her teachings have filled gaps in my knowledge base I never knew needed filling and have significantly enhanced my understanding of the inner workings of the body! Rachel has an incredible ability to make the numbers that patient’s so often present us with, both understandable and clinically meaningful. The knowledge I’ve gained by investing in this skillset has paid off in dividends and I’m certain will continue to do so into the future.”
Stacey Curcio – Cultivating Wellness
I hope you’ll join me for the most exciting up-skilling opportunity in learning labs yet. Oh…and all this talk about thyroid testing..that’s just a serving suggestion 😉 this year my MasterCourse is focused on the most routine labs of all: ELFTs, FBE, WCC, Lipid and Glucose Panels…an absolute treasure trove of free integrative health information about your patient!
This skillset has been found by many to be biggest ‘game-changer’ in Integrative Medicine!
There are limited places. To sign up for the MasterCourse: Comprehensive Diagnostics click here. For more information about the program click here.
Listen to me, I’m sounding all sporty 😂. I’m not though, just in case you suffer misguided visions of my virtues! But it’s not just the self-declared serious athletes that we need to have on our radar in relation to optimising their oxygen carrying capacity (aka window to winning). Our clinics are full of people, regularly running, doing triathlons for fun (!), riding vast distances clad in Lycra to drink coffee in other town’s cafes etc. etc. whose FBE might be feeling the pinch! That’s right! All these individuals, depending on the frequency and intensity of their exercise, could have the so-called, anaemia of an athlete.
Long gone is the idea that exercise-induced changes to your haemoglobin and red blood cells and perhaps even your iron, would only affect the ultra-marathon runners among us. It’s the swimmers, the cyclists, the Roller Derbyists, the CrossFitters, the basketballers, the Gym Junkies, the lawn bowlers..ok I may have gone too far now…they all are at increased risk.
Why? Isn’t exercise good for you? You know I so want to say, ‘Surprise! It’s not!’ but alas. Of course it is good for us BUT there are some fascinating challenges regular exercise can throw at your dear old blood and its bestie, iron. These challenges are incredibly dynamic – having one effect during exercise, a different one immediately following, and yet another in the days of rest in between. And sometimes, in fact, often, our patients can end up on the wrong side of these seismic shifts. Here’s how the story usually goes
“Oh yeah..I’ve had anaemia for ages! You know and it doesn’t matter how much Iron I take or how I take it – it never budges. But I’ve been told to stay on the Ferrograd anyway”
Typically, being told it’s ‘Athlete’s Anaemia’ is the first, in a series, of many many errors to follow. Because in fact, there is no such thing. That’s right. Anaemia is a symptom not a disease and exercise induced anaemia comes in 4 common flavours: Dilutional, Heamolytic, Iron Deficient & Acute Anaemia of Exercise, and knowing the difference is critical to correct management. Only 1 of them will reliably improve with iron and it needs to be prescribed in a totally novel way. Others will get worse with more iron. Yep. And one is a complete illusion. So when we don’t make the right diagnosis, which of the 4 types your patient actually has, we fail to find the fix. And while all of our patients may not be overly obsessed with improving their performance or even winning, let’s face it, they all want to achieve their PB, that’s why they came to see you. So can you tell the difference?
WARNING: I got so enthused about this topic that I went over. The current ‘Update in Under 30’ is a ‘serving suggestion’ only! And you may need to speed up your playback to squeeze in another bonus 10 min, if you can only afford your usual 30 min car trip to listen!
Outrunning ‘Athlete’s’ Anaemia
Persistent ‘hard-to-resolve’ anaemia is a common presentation for anyone participating routinely in sport and that can be at any level, not just among the professionals. From our lovely ladies who take up running or CrossFit in their middle-age, to our MIL (men in Lycra) and ‘weekend warriors’, they may love it but their haemoglobin and their iron doesn’t! Anaemia equals reduced oxygen carrying capacity, a concern for anyone interested in optimising their performance but equally relevant to patients just trying to manage their energy throughout the day. In this important episode we identify 4 different types of anaemia seen in patients as a result of exercise, incorrectly lumped together as ‘Athlete’s Anaemia’. Each type is easy to recognise once you know how and effective treatment of each is remarkably different. This summary and the super handy clinical resource that accompanies it will help you and your patients absolutely outrun it, at last.
For all Update in Under 30 Subscribers, you will find it waiting for you in your online account and don’t forget the **EXTRA BONUS LIVE CALL WITH RACHEL.
**This live Zoom call with Rachel is for current Update in Under 30 Subscribers ONLY. A Q&A session for subscribers on the UU30 episodes released in 2020. Contact the RAN Team to reserve your spot!
Ever suspect you’re being gaslighted by your patients’ results? Especially when their CRP result says, ‘nothing to see here’! But every other piece of information and every one of your senses tell you they’re inflamed and their immune system is up to something!!Me too. You probably then look at their other results, their ESR or their white cell count searching out something that supports your hunch, but they too can look disappointingly unremarkable. That’s the moment when you wish life was like a televised sports match and you could check the video evidence rather than believe the mere mortal (and clearly blind!!) man in white on the pitch. Well guess, what…you can.
Albumin
÷
Globulin
As long as you know how to divide one figure by another using a calculator. I’ve found it requires the same digital dexterity as pushing the ‘on’ button’ on my blender…so if you can make a smoothie, you’re sorted! So while almost every lab routinely reports these two as separate parameters that are also routinely in range…I haven’t seen many that actually do the calculation for you and give you the Albumin:Globulin (AGR) on a platter. Yet this one step maths transforms the mundane into magic and can reveal almost all to you regarding your patient’s level of immune activation, inflammation and oxidative stress, from the largest number and variety of drivers. That’s why I call it, 📣The Master Inflammatory Marker 👑
When factoring in your patients pathology results is at its best – it makes the invisible suddenly visible to us. We could have sat and eyeballed that patient all month and never suspected that their Hcy was too high, or they had antiphospholipid antibodies or, or etc.
But the albumin to globulin ratio goes one step further & trumps the other inflammatory markers we’re so familiar with, because it even sees what they can’t!
And a low AGR (≤1.2) signals just that to you. So when the patient with joint pains, or just a little bit of belly fat or an emerging yet unnamed autoimmune condition presents exasperated saying, ‘but apparently I’m not even inflamed!’…you can let them know you do see it, and it’s just that others weren’t looking in the right place, then get busy rolling your sleeves up to move those markers! That’s right, a low AGR is a clear call to action for practitioners engaged in risk minimisation, prevention and for working towards best outcomes in established disease and monitoring a patient’s AGR is a series of clear sign-posts about whether you’re leading them in the right direction or not. There’s a lot more to say on this this third umpire & ripper of a ratio – about kids, the contraceptive pill, confounders, a role in cognitive impairment prevention and what optimal might look like but hey…the cricket’s back on…gotta go 😂
Patients’ labs lie, not often, but sometimes and the inflammatory markers performed routinely like CRP and ESR have been known to tell a few. Like when everything about a case screams inflammation but both of those say there’s none there. Why do they miss it?…well basically it’s not their lot. CRP and ESR have specific signals they only respond to and therefore reflect only certain immune reactions and at specific stages of that response. But there’s a nifty little calculation you can perform with all of your patients labs and suddenly see the immune activation, inflammation and oxidative stress that was lurking beneath. It’s called the albumin to globulin ratio and it’s going to change your understanding of what’s going on in your clients and your ability to monitor the efficacy of your management.
Sometimes I think I must be psychic..or is that psychotic? Don’t answer that, it’s a bad Byron Bay in-joke. I had literally just recorded my Update in Under 30 Copper in Kids and this excellent new study was published that same week, assessing and comparing trace minerals in age-matched ADHD and neurotypical kids. Snap! ✨ First, a moment of panic…because believe it or not, there are very few rigorous studies that have looked into this and so I had already read them all cover to cover and could confidently say, I had a grip on the literature. Gasp…’ will it have a different finding and challenge the much broader story about the excessive demonising of this mineral in kids health?’ Everyone take a big breath out…no.
But if you’re someone who thinks you’re seeing Copper toxicity in kids, you can keep taking a big breath in and while you’re at it a huge bit of new information:
Copper Excess is Normal in Children.
Every investigation of blood Copper levels in kids has reached the same conclusion and this latest one by a Russian group of researchers renowned for their work in Copper agrees. So the ideas that we have about optimal in terms of mineral balance for adults may stand, but can not and should not be applied to children. The elusive 1:1 relationship between Cu and Zn, for example, considered aspirational in optimising the mental health of big people, is absolutely not desirable or even healthy, in little ones. Why is it so? I hear you ask (…because you loved those old Cadbury chocolate ads with the crazy Professor as much as I did) Well, essentially because kids need more Copper than us, as a simple result of their increased growth requirements: blood vessels, bones, brains…Cu is a critical player in them all and more. And while we (and when I say ‘we’ I mean ‘I’) may be passionately passionate about Zinc’s importance, turns out, in paediatrics, it really does play second fiddle to Cu and should.
This new contribution to the Cu & Zn in ADHD kids debate did find that compared with neurotypical kids, their Cu:Zn was higher BUT – **and this is the really important bit **- as has been shown in a similar cohort before, the shift in relationship between the two was due in fact to lower Zinc levels NOT higher Copper.
So, I guess when you think about it…Zinc perhaps really does still deserve all our loving attention we give it 😂…we just need to rethink the whole negative attention we tend to mistakenly give Copper!
Copper, as a kingpin in angiogenesis, brain & bone building & iron regulation is a critical mineral during paediatric development. So much so, the kind of blood levels we see in a primary schooler might cause alarm if we saw them in an adult. So too their Zn:Cu. But higher blood Copper and more Copper than Zinc are not just healthy but perhaps necessary during certain paediatric periods. This recording redefines normal, low and high with a great clinical desktop tool to help you better interpret these labs, as well as reviewing the top causes and consequences of both types of Copper imbalance in kids.
The latest Update in Under 30 has landed. You can purchase January’s episode, Copper in Kids here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
-Your RAN Online Account has a NEW LOOK!!-
Next time your log in, you will experience a more user friendly way to search, view, listen and download your resources. Find out what’s new here.
Copper deficiency happens in kids, so does copper toxicity and both are serious concerns, but do we know when to accurately call either? First, we have to know ‘normal’. If we know what normal Serum Copper values look like in children, then we can easily spot those falling below or above this, right? That’s the first hurdle we tend to knock over and break a toe on! Being a mineral whose levels vary widely in soil from country to country, globally, the differences in reference ranges are breathtaking & absurd. Add to that, that copper is a key mineral in kids, driving huge demand for it during key periods of development, so the range for pre-schoolers isn’t the same as the primary or high schoolers – not that your lab is flagging that. Unhelpful? Yes. Dangerous, even? Potentially.
To diagnose ‘Copper Excess’ in a child is a big call to make.
One, because most practitioners are unaware just how much Copper a child really needs at each age & two, high copper is often a messenger for something else going on and then three, the primary objective based on this diagnosis becomes to lower their Copper but we could be either shooting the messenger or missing the mark all together…right?
Copper excess does happen but not nearly as often as practitioners believe it does. And in kids, the fall-out from such misdiagnosis is bigger. And missing a Copper deficiency? (because we’re not as well-trained to recognise it and because Copper has been sadly demonised) Likely to have myriad negative impacts at this vulnerable age…almost none of which generate symptoms or a distinct clinical picture e.g. secondary iron deficiency, low neutrophils without necessarily compromised immunity. But what about the holy grail get-out of jail adjective: ‘relative’. You know, ‘this is at least a Copper excess relative to their Zinc?’
Well, to form this opinion you’re likely calculating the Zn:Cu ratio and applying an ideal adult value of 1:1 but show me the primary evidence that supports this for kids…anywhere? The Zn & Cu relationship shifts as we move through life-stages and in fact Copper is supposed to dominate through a lot of our childhood so…ummmmm…no.
HTMA Copper side-steps all of this?..double no.
I used to make the same mistake re Zn:Cu, I may have even taught you this?!🤦♀️ But as so often happens, a week spent in all the original scientific data and I’ve emerged a changed practitioner! Having been part of perpetuating this problematic premise in the past, I am determined to get the correct message out there to as many practitioners as possible. So help me spread the word on Copper in Kids – by telling others that this mineral is so critical to kids compared with adults, they will often have higher levels than ‘us’ and that until you’ve applied the right age-appropriate reference range and ruled out confounders you can’t possibly make a call on Copper. I mean, we kind of knew this all along, with healthy pregnancy Copper values being exponentially higher being a giant clue. Turns out kids’ ‘Copper Age’ extends way beyond the womb.
Copper, as a kingpin in angiogenesis, brain & bone building & iron regulation is a critical mineral during paediatric development. So much so, the kind of blood levels we see in a primary schooler might cause alarm if we saw them in an adult. So too their Zn:Cu. But higher blood Copper and more Copper than Zinc are not just healthy but perhaps necessary during certain paediatric periods. This recording redefines normal, low and high with a great clinical desktop tool to help you better interpret these labs, as well as reviewing the top causes and consequences of both types of Copper imbalance in kids.
The latest Update in Under 30 has landed. You can purchase January’s episode, Copper in Kids here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
-Your RAN Online Account has a NEW LOOK!!-
Next time your log in, you will experience a more user friendly way to search, view, listen and download your resources. Find out what’s new here.
Remember the days when we had the brain all back-to-front & upside down? Anatomy & physiology told us it was an island, completely protected by the blood-brain-barrier from pathology in the rest of the body, that it was incapable of regeneration after damage and that it didn’t have its own lymphatic system. All wrong. Which presents a problem, the CNS is absolutely in trouble if other parts of our body are (!), but also some solutions: plasticity and the brain’s own capacity for cleaning up after itself. New research has revealed more about this critical CNS cleansing and what is likely to get in the way of this
The latest Medscape update on this is quite poetic, speaking to the movement of body fluids like tides within the human body.
“They found that the blood flow to the brain diminishes, allowing for an influx of cerebrospinal fluid (CSF), washing away the day’s detritus of proteins and other waste substances that might harm the brain if they aren’t cleared out.”
But these particular tide times are restricted to sleep – having never been identified during awake states & even more specifically only during our Deep Sleep, the period of slowest brainwave activity. The speculation is, of course, given sleep issues predate or are a feature of neurological and mental health conditions, that perhaps this comes back to the impeded process of waste removal that accompanies this and how this may contribute to accelerated negative neurological change. For example, beta-amyloid proteins are well known to be removed most rapidly during our sleep and this week I’ve been faced with a small mob of patients who have substantial cognitive impairment risk from a genetic standpoint (e.g. Apo E 4 carriers in families riddled with dementia) but their unmanaged long-standing insomnia plus or minus OSA is likely just AS risky. So here we are again back at one of the key non-negotiables for health: Sleep.
I often say to my patients, ‘There is nothing I can give you in a bottle or a blend than can do one 100th of what healthy (quantity & quality) sleep can do for your wellbeing today or for preventing health issues for you in the future’
And then I say it out loud again when no one else is around just to ensure we’re all aware of that 😉
The brain is no longer considered an immunoprivileged organ separated from immune cells by the blood-brain barrier, with research revealing numerous interactions between the neurological and immune systems. A large body of evidence now shows that these interactions, in particular an imbalance in pro-oxidant & antioxidant systems, play a clinically relevant role in the mental health issues of our patients and may go some way to explain why patients with chronic inflammation frequently present with mood and cognitive issues. Identifying and addressing the source of the inflammation (musculoskeletal, gastrointestinal etc.) therefore potentially addresses the underpinning cause and creates a ‘win-win’ scenario for patients. This updated recording aptly named: The Inflamed Brain, covers all this and more!
With the increasing weight of evidence pointing to a potent pathogenic portal between our mouths and every other part of the body, whether that be in terms of cardiovascular disease, rheumatoid arthritis, appendicitis, even a growing case for Alzheimer’s disease, we need to ensure we’re not overlooking the condition of each patient’s oral cavity. I got very excited about the recent Medscape article: A rapid non-invasive tool for periodontitis screening in a medical care setting. It’s true, I live a quiet life 😉 But seriously, a validated tool for all non-dentists to accurately pick up on the likelihood of this condition would be a nifty little thing indeed, so we can narrow down just who we quick-march off the dentist as well as understand their whole health story. But then I read the 8 actual questions which included gems such as: Do you think you have gum disease? and Have you ever had treatment for gum disease such as scaling and root planing, sometimes called “deep cleaning”? I thought, ok, this is not rocket (dental) science.
But that’s the point, I guess, right?
So while I encourage you to check out & employ this screening tool by all means, we can also be reassured that just by ensuring that when we ask about someone’s digestion (and when don’t we?!) we start at the very top of the tube, we’re doing a good job!! As my new grad mentees learnt this year…following the patient’s GIT from mouth to south anatomically, is my rather simplistic way of guaranteeing I cover everything digestive..without using formal consultation script. So in the case of the mouth, my questions include things like: last trip to the dentist; any prior dental diagnoses, number of amalgams, implants, root canals etc & their routine dental care techniques, any signs of bleeding on brushing & all foods they avoid for dental or oral reasons? Look, it hasn’t undergone the rigorous validation that the Self-Reported Oral Health Questionnaire has..but I think it’s a good start.
Whether we’re being picky about pathogens and exactly how they got access to the rest of the body (and gums make a great entry point!!) or just concerned about chronic low level inflammation, a ‘gurgling’ CRP between 1-5 in an otherwise ‘healthy adult’, picking up on periodontitis is a pivotal.
Oh and if you’ve ever wondered about possible health implications from mouth metals other than amalgams…don’t worry, soon I’ll be getting to that with a forthcoming UU30.
Want to hear more about how certain microbiota (from the mouth to the south) are being implicated in joint diseases such as rheumatoid arthritis and ankylosing spondylitis and how we can investigate these individuals?Getting to the Guts of Women with Joint Pain is a recent UU30 instalment that gets down & dirty on the detail.
No you’re right, it’s not long enough to be a Hemsworth’s mobile number but actually it’s more sought after 😉 If you’re up to date with reading & recognising all the different patterns of Iron Studies & the stories they tell, which is a daily business for most of us, then you will know by heart the striking pattern we call, ‘Pseudo Iron Deficiency’. You know the one where your patient’s serum iron & transferrin saturation are mischievously trying to trick you into thinking you need to give this patient iron…when in fact this is absolutely not what they need!
This is of course the result of the redistribution of iron during inflammation – iron is actively removed from the blood and sequestered in the liver instead. It’s designed to protect us from bacterial bogeymen, which is how our stone-age bodies interpret all inflammation of course.
Doesn’t sound familiar? Ok you need to start here or even embrace a full overhaul of all things iron here.
But for those of you nodding so hard you’re at risk of doing yourself an injury, this number is for you. We’ve often talked about the redistributional increase in patients’ ferritin levels in non-specific terms: it goes up..but by how much? Of course we would like to know because no one is fooling us with this transiently inflated value…but can we make an estimation as to what this person’s ferritin will drop to once this inflammation is resolved? Yes.
X 0.67
Write it down. Consider a tattoo, perhaps?
This glorious magic number comes from Thurnham et al paper in 2010 who did the number crunching on over 30 studies involving almost 9,000 individuals to determine the mathematical relationship between inflammatory states & markers and the reciprocal increases in ferritin. Their work is exceptional in that it also differentiates between incubation (pre-symptoms), early and late coalescence periods (if you want to differentiate your patients in this way and get even more specific then you need to read the paper), however, overall when we see a patient who has a CRP ≥5 mg /dL , we can multiply their ferritin by 0.67 and get a lot closer to the truth of their iron stores. Oh and another important detail they revealed, this magnitude of ferritin increase is more likely seen in women or those with baseline (non-inflamed) values < 100 ug/L..so generally more applicable to women than men. Thanks Thurnham and colleagues and the lovely Cheryl, my previous intern who brought this paper to my attention…you just took the guessing out of this extremely common clinical scenario 🙂
We’re not deaf…we heard that stampede of Iron-Inundated Practitioners!The Iron Packageis for you!
Our recordings and clinical resources for improving your skill-set in all things iron including, your accuracy of diagnosing deficiencies, pseudo-deficiencies & excesses, plus radically rethinking the best treatment approaches for each scenario…have been some of our most popular. Because nailing iron (pardon the pun) is harder than we were all lead to believe and at least 1 ‘iron maiden’ or ‘iron man’ walks into our practice every day, right? So we’ve brought together 5 extremely popular UU30’s on Iron into one bundle for the price of 4! So if you’re more than ready to graduate from ‘iron school’, now’s your best chance!
How often were we told this in our training? And how often have we found this to be true in practice? And now suddenly, it seems, the medical researchers (at last!) are rapidly coming around to this core concept?? Our microbiome is suddenly the hottest property on the body block, and it seems every interested party is shouting, ‘Buy!Buy!Buy!’ As integrative health practitioners, of course, we had a major head-start, not just by appreciating the gut’s central positioning in the whole health story (iridology beliefs, maps & teasers aside!!) but also a heads-up about the damage the western diet, our medication exposures and lifestyle tend to wreak upon it. A favourite quote of Jason Hawrelak’s by Justin Sonnenburg, “The western diet starves your microbial self”, underscores the significance of just one element of this impact. And…are we all clear that the increasing number of patients reporting adverse food reactions, once again, overwhelmingly are a response to aberrant processes in the GIT?
Sounds silly it’s so obvious right, but it’s easy to get distracted & misattribute blame…for example, it’s the food that’s the problem. Well yes in a minority of situations interactions between someone’s genes, immune system and a particular food turns something otherwise healthy into something pathological, but for the majority, the food itself & in others is healthy, & could be beneficial to this individual, if only we could resolve their GIT issues…like FODMAPs for example.
Not the problem, just the messenger.
So if the ‘problem food’ is just the messenger, what’s the actual message we need to understand? Is it that this patient has medication, disease or otherwise induced hypochlorhydria, impairing ‘chopping up’ of potential antigens implicated in immune mediated food reactions? Or is that this person’s got fat maldigestion &/or malabsorption so that in addition to not tolerating fats, they may experience dietary oxalate intolerance to boot? Or are the food reactions the result of altered microflora changing what we can and can’t digest (via their critical contribution) & absorb?
So what message does the presence of IgG antibodies to consumed foods send us about the state of someone’s gut? It’s telling us 2 things: this individual exhibits abnormal intestinal permeability & currently in the context of this leaky gut, these foods may constitute a barrier to resolving this & other symptoms as well.
We’ve recently released the mp4 (that’s audio plus the movie version of the slideshow so grab your popcorn…that’s if you don’t have a corn issue!) of A Guide to Investigating Adverse Food Reactions – What’s IgG got to do with it? which details the science behind IgG, including debunking, the incorrect debunking of IgG food antibody testing!! But more than this, it overviews the whole maze of adverse food reactions, articulates a logical investigative path for practitioners through this maze, and helps us to really understand that finding the food(s) responsible for a patient’s symptoms is not the final destination..and can be in fact a distraction, if we don’t cut to the chase and find out the why…and funnily enough…my dear old iridology teachers and colleagues...it almost always comes back to the gut 😉
Confronted with the possibility of adverse food reactions in an increasing number of our patients can be an overwhelming prospect, in terms of accurately identifying and understanding the faulty mechanism underpinning these aberrant responses to healthy foods. Elimination of culprits in most situations is only a short term reliever, not an appropriate long term solution, so to optimise results we need to know the real mechanism of action. The majority of these, of course, stem from the gut, but being able to elucidate exactly which of the many things that can go wrong there, is going wrong and therefore what foods are problematic until we address this, is the key. This 2hr mp4 is all about the bigger picture and helping you find method in the madness that can be the AFR landscape. Along the way, we detail the science of where IgG reactions fit into this and it’s a fascinating story that just might be the missing puzzle in your leaky gut patients.
b. Every herbalist’s jaw at my table at the NHAA conference gala dinner, when I got almost all my Latin binomials right during the trivia quiz?…and after some champagne, that’s a particular achievement
c. My jaw, when I saw firsthand how much those herbalists could drink of ye-not-so-olde herbal extracts!!
d. The latest Update and Under 30 – Milk Madness Part 2
e. All of the above
If you answered, ‘e’…. you must have been one of those herbalists at my table, otherwise you have way too much insider information! But yes you are correct on all accounts. So this latest UU30 is an extension of our discussion last month about the potential contribution from to mental health from dairy intake in a subset of patients. This whole topic, the research for which dates all the way back to the 70s, was too big to fit into one – given the current evidence base that now depicts at least 2 different mechanisms that might be at play, and the different types of mental health problems, each has been linked with. Last month was all about retracing the ‘dietary exorphin’ path, this month it’s about the propensity for some individuals to make antibodies to casein and the significant growing data that suggest this happens to a larger extent in patients with certain psychiatric diagnoses. More importantly, we talk about the ‘why’.
What compelled me to make time to look through all the literature on this was that there is some. No seriously. When I initially learned of the GFCF dietary approach to ASD patients I was told that in spite of a lack of supportive research, the empirical clinical evidence was irrefutable, which I later saw with my own eyes. In the couple of decades since, I only really heard about negative findings, short trials of the elimination diet specifically in ASD kids, that failed to produce significant change. Funny how the bad stories rise to the top, right? But when I spent the time doing a thorough literature review, I found these negative findings were far from the whole story. In fact, I was really surprised by the high level of evidence employed by researchers of late, who have repeatedly found associations between either exorphin or antibody levels and patients with particular diagnoses, in addition to really progressing our understanding of why these measurable differences (urinary exorphins, plasma IgG and to a lesser extent IgA casein antibodies) are meaningful. Do we know everything? What do you think? The answer, of course, is always no. But we know enough to consider this aspect in our comprehensive workup of mental health patients and all their biological drivers and we know dramatically more than anyone in mainstream medicine, or the dairy industry for that matter, is ever going to let on!
If you want to hear a synthesis of the casein antibody link with mental health then download the latest UU30 – Milk Madness – part 2. If you can’t go that far, then “do yourself a favour” and read a couple of seriously important articles on this topic – and why not start at the deep end with this study by Severance in 2015.
Could dairy intake in susceptible individuals be a risk promoter for mental health problems? In addition to evidence of the exorphin derivatives from certain caseins interacting with our endogenous opiate system discussed in part 1, we now look at the evidence in support of other milk madness mechanisms. Specifically, the IgG and, to a much lesser extent, IgA antibodies about what this tells us about the patient sitting in front of us about their gut generally and about their mental health risks, specifically. The literature in this area dates back to the 1970s but the findings of more recent and more rigorous research are compelling.
 You can purchase
You can purchase