I’ve been ruffling feathers over here while speaking at AIMA in Auckland. While I am pretty familiar and comfortable with that role (& responsibility?) – this topic ruffled my own, arguably the most. In fact, I kicked off the presentation with, ‘What I’m going to say might make some of you uncomfortable but you know what, it makes me uncomfortable and if it makes you think a little less of me, well, to be honest, contemplating these issues has already made me think less of me!”
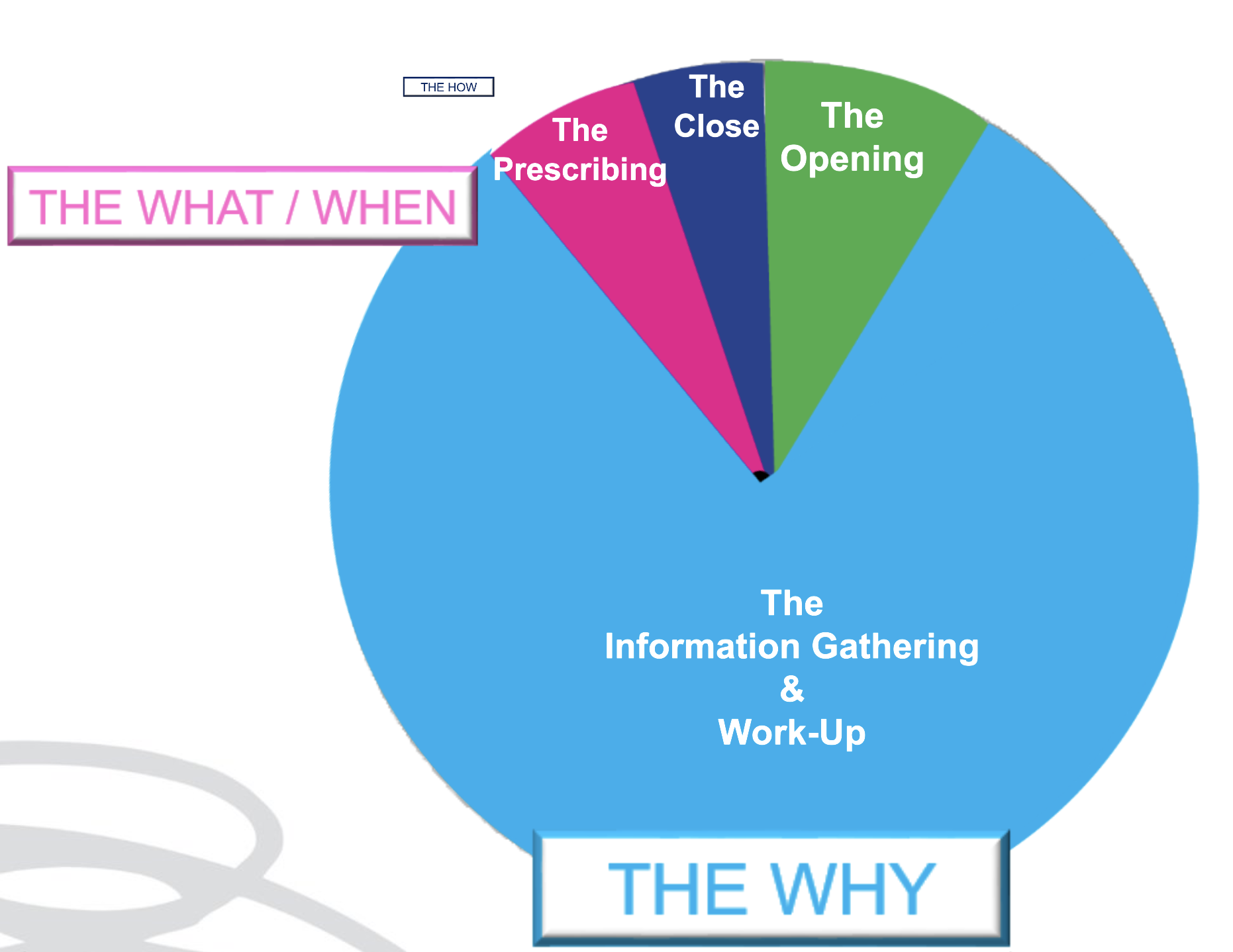
As an educator in integrative health, I have overwhelmingly been a peddler of knowledge and skills under the headings of: ‘WHY’ and‘WHAT’
Why – as in why does this patient present in this way, at this time. I am passionate about upskilling practitioners re our powerful contribution to the diagnostics & work-up of each individual. What – as in what changes (supps, herbs, diet etc) need to happen to correct for these very unique elements of imbalance in this patient to therefore aid resolution. We might label this, ‘personalised medicine’. But after so long in practice it’s patent that the best results don’t come from being the cleverest clinician nor the biggest biochemical brainiac. Knowing the ‘why’ and even the ‘what’, while enough for a minority of patients, fall short for the rest and can still fail to be truly about, & exclusively with, the most important person, in mind.
We’ve learned this before but it needs to be said again and again and again: much of any medicine is via the therapeutic relationship – and as part of this, our ability to PLACE the patient at the centre of their own SOLUTION. And therein lies the conversation we need to have in detail with them about the ‘HOW’ But how much time in your current consults is afforded to the ‘HOW’?
Being able to effectively negotiate with out patients the ‘HOW’ is an extension of Motivational Interviewing, Behaviour Change Theory & Patient Centred Care. It returns the humanity to our list of recommendations for each patient, pushing back against the autocracy that can tend to slip in with prescription writing. It powerfully reminds us that the prescription is only ever as good as the patient’s engagement & buy-in, and that’s only ever as good as our ability to write a prescription that is accessible & readily transplantable into their existing lives: to co-create with them Patient Centred Prescriptions. Someone in the audience had been my patient in the past – double awks right – because I absolutely know, I didn’t know this well enough back then. Back then when they were unable to do exactly as I had recommended – with their diet, their supps, their sleep, their work-life balance – they had, in turn, apologised for their ‘weakness’, ‘lack of willpower or diligence’ and me, being ever so gracious, accepted those apologies only to repeat the error of my ways and write yet more scripts that set them up to fail. 🤦♀️ I am committed to getting better at this and in this endeavour, giving both more attention & time in my appointments to the ‘HOW’ & yes I think we need to think creatively about how we use our appt time and between session touch points to achieve this – keen to hear about your perspective and experiences.
At the end of an information & insight heavy appointment, formulating a list of products and doses for our patients to take can feel like a bit of a ‘tada moment’, like a magician pulling a rabbit out of the hat. “Here is the solution – now off you go!” Research tells us, however, that treatment-plans that are a co-creation between you and your patient – evolving from a discussion that not only allows them a voice, but a major role in the decision making – are far more likely to succeed. While we are the authority on our medicines, our patients are the authority on what makes them tick & what’s likely to succeed, in terms of taste, texture, temperature & timing! This is called Patient Centred Prescribing and together with some other tips tricks and hacks I share with you in this episode, can really increase patient buy-in, compliance and therefore bring your treatment plan to fruition and fulfilment!
This is not about body shaming nor body positivity. I understand the crudeness of the body mass index, as a measure of (un)healthy weight – let alone (un)healthy muscle mass, so I don’t use this as a stand-alone assessment of weight, nor rigidly adhere to the categories it allocates individuals. With only minor recognised racial adjustments for BMI, I also recognise our concept of ‘healthy weight’ is incredibly whitewashed with minimal regard and consideration for clear ethnic and racial differences in physique. Patient’s lab results tell the real story. It’s in their results that we can discover someone is thin-on-the-outside-fat-on-the-inside (TOFI) or FOTI. These are patients whose BMI, WC,WHR, Body fat% etc identify them as obese – yet there is not a whisper of what I call ‘Adiposity Patterns’: no subclinical inflammation, no reduced glucose tolerance or actual IR, no raised transaminases that we expect to correlate with girth and the corresponding fatty infiltration of their liver. In this, as in so many other aspects of clinical practice, we are reminded to see each individual, individually.
AND if we adhered to this always, listening unfiltered to the whole health story and letting the labs speak, we would not miss those patients in whom unhealthy weight really is the most important underpinning, & all impacting, issue. And we are not doing our job, when we don’t.
I mean – we all know the detrimental effects of excessive adiposity – that’s like Pathology Unit 1 topic 1, right? I know we know it. Yet there are so many reasons why we might down-play, step-around, or even ignore its enormous contribution in our patient work-up and certainly the discussion that follows with our patients. That too is a no-brainer. Who wants to say to someone whose come seeking your help, as an explanation for their complex health concerns, ‘There’s no zebras here just a horse – one really over-weight horse!’ Knowing too that unhealthy weight results from the most complex constellation of factors (biopsychosocial) unique to each individual and that change in this health determinant, is arguably the slowest and hardest to sustain. But how are we serving our patients if we don’t?.
A practitioner presented this case of a 48yo F seeking help with the work-up: Self-reported inability to lose weight after 1st pregnancy = ‘obesity’ ongoing – now BMI 33.1 –> 25yo Reflux & Hiatus hernia Tx Omeprazole initiated – ongoing –> 26yo Depression Tx Venlafaxine initiated – ongoing –> 30s Back and other musculoskeletal injuries Tx Surgery & Opiates – ongoing –> 40s Hypertension & elevated resting HR –> Last 12mo – changes in Mx cycles suggestive of perimenopause & substantial weight gain
This patient didn’t ‘have’ any lab results but I think I can make an educated guess about how they would look and in particular whether they show the characteristic ‘adiposity patterns’ I mentioned before. What was my first thought about the most impactful element of the case? Obesity. What was my second thought? Where is all the weight (diet & intervention) history that would help us to understand how she is where she is, right now? We didn’t have any. The practitioner informed me that the patient was ‘not very interested in talking about her weight’ – in fact, according to her, it didn’t seem like losing weight was one of her goals. Now this could be several things: the fear of judgement, even her own self-loathing, the paralysing awareness of the enormity of such a goal, the dashed hopes of the past, or it could just be that her weight, as the key negative determinant of the majority of her health concerns & quality of life, has just never been brought to her attention, nor the connections explained to her in simple accessible language. So over to us, right?
There were other health determinants at play in this patient but the centrality of the adiposity was undeniable & the practitioner said this was the greatest take-home. She’d been ready to don some jungle gear and go hunting some zebras – but there was a horse right here in front of her and that could not and should not, ever be ignored.
What else became apparent was the lack of knowledge & skills regarding how to take a comprehensive weight history & why this is crucial. Not only for this type of unhealthy weight, the underweight require exquisite attention, as do those with a more labile weight than expected as an adult. This brilliant article by Kushner et al from 2020 is a total gift in that regard and a must-read for every clinician. We feel uncomfortable asking about certain things when a) a patient feels uncomfortable which is usually because b) we are uncomfortable and this ultimately comes from not being clear about WHY this information is so important and HOW this will ultimately enable us to better help THEM.
This is the very latest, comprehensive review of the key aspects of thyroid assessment that will revolutionise your understanding of thyroid markers. Gain a clear understanding of how to provide the best, most individualised, thyroid management by learning to read the real story in each patient’s pathology patterns. Boost your knowledge and confidence looking at TFTs, rT3, thyroid antibodies & related nutrient patterns, as well as AITD, environmental EDCs, HPA driven HPT issues, thyroid nodules, the impact of dietary macro- & micro-nutrient imbalances and much more!
This 4 part series provides over 10 hours of the very latest research & findings, punctuated with real case studies, that will both contemporise and deepen your understanding of all things thyroid, with a bonus recording on Adrenal Assessment.
Are we doing ourselves out of a job? I’ve been talking treatment plans with my New Grads recently. Given, only recently these were major assessment items in their clinic units, they have been trained to create ALL-ENCOMPASSING (biopsychosocial) prescriptions and recommendations of utterly EPIC PROPORTIONS – to simply prove they know it all. Problem is this doesn’t work in the real world.
Emailing your client multiple pages of advice that covers: a whole sizeable supplement schedule that only a military-training could nail (2 tablets 1 XTID 1 X BID, a liquid, a powder, some with food, some definitely not with food) plus dietary advice, plus hyperlinks to exercise advice, mindfulness exercises and a request for follow up investigations before the next appointment…is…a L*O*T!!
It is also ineffectual – because it completely disregards the human on the other end. Let me ask you this, how much change are you capable of between a first and second appointment, roughly a period of 2-3 weeks? Personally, I gotta say not that much. It took my dentist years to get me just embrace flossing & I don’t think I am an exception! With all the knowledge we possess its hard not to see people as (a long list of) problems (& problematic behaviours) that we translate into, and solve via, a prescription.
Effectively we are saying to patients with this practice model, ‘Go change & come back when you’re done & then I’ll probably ask you to change some more!’ That’s both a big ask and a huge missed opportunity.
I hear from reliable sources over the ditch, that GPs are increasingly referring their patients to, or teaming up with health coaches, rather than naturopaths. Given what I’m observing, I get it. Doctors on the whole only have time (and barely then) for a finger-pointing prescription – certainly not the time and touch-points required to actually support patients with the very difficult thing that is, behaviour change. Nor the skills to truly facilitate patients making the necessary and desired changes – so they outsource this role. But we shouldn’t.
After all – I want to be on my patients’ support bench & health care team always – not a flash in the pan, that blinded them with science or my ‘smarts’ and proved to them in one over-stretching prescription – that naturopathy is not for them, or at least, they’re not fit for the task.
At the end of an information & insight heavy appointment, formulating a list of products and doses for our patients to take can feel like a bit of a ‘tada moment’, like a magician pulling a rabbit out of the hat. “Here is the solution – now off you go!” Research tells us, however, that treatment-plans that are a co-creation between you and your patient – evolving from a discussion that not only allows them a voice, but a major role in the decision making – are far more likely to succeed. While we are the authority on our medicines, our patients are the authority on what makes them tick & what’s likely to succeed, in terms of taste, texture, temperature & timing! This is called Patient Centred Prescribing and together with some other tips tricks and hacks I share with you in this episode, can really increase patient buy-in, compliance and therefore bring your treatment plan to fruition and fulfilment!
We all (inaudibly🤞) sigh when patients utter this & adopt the brace position for whatever mis- or dis-information may follow.
So how would you feel, if instead, these were the words of the health professional you’re seeing?
We could debate forever the pros and cons of FB and its forums – & indeed it offers both – but one thing we must never lose sight of is what it has in common with the ‘wild west’: unregulated, unvetted, and with plenty of cowboys – often sadly, masquerading as experts, or just ‘very “generous” very very active group members’, with hidden agendas. I don’t generally engage with the naturopathic forums but occasionally I catch sight of things that I can’t look away from, and I can’t not speak up. Recently, someone (with a not-so-hidden-at-least-to-me-agenda) was raving about the dangers of N-acetylcysteine as a supplement & the way it was spoken about made it seem like it would be *poison* at any dose. Wha? As you may have learned from me it is definitely potent and in turn, demands our respect as a powerful therapeutic agent – directing our decisions about timing and reminding us, yet again, that least dose is best dose. But what this individual was purporting were adverse effects I’d never heard of in relation to this nutraceutical. So I simply asked, ‘Can you please share your reference(s)?’
Prior to me inserting myself into the comments – there had been enormous engagement specifically with this individual’s claims- which mostly went like this: ‘Oh wow! I didn’t know this!!’ ‘Thank you – that’s so interesting!’ “Oh that explains why Tom doesn’t like it, and Dick won’t take it and Harry says it’s horrible!” 🤦♀️
FB forums – seeking out the support & opinions of our peers can be truly wonderful but it can totally derail our knowledge too if we don’t keep checking the quality of that information. A simple: Can you share your references, or, where did you learn this? Should be part of the respectful and expected scientific discourse in our profession. I’ve asked that before when I’ve found myself yet again in a forum thread and had a truly fabulous response – with the practitioner generously sharing a number of high quality published articles that would have taken me ages to find myself! 💪Not the case in this recent episode. The 3 distinct claims, which all centred on NAC being bad for high histamine individuals, were ‘substantiated’ by just 1 primary reference & that was a Poster Presentation: “Human placental tissue was minced and subjected to a fractionated ammonium sulphate precipitation (35% / 65%). A fraction high in DAO activity was purified using hydrophobic interaction chromatography (HIC), and incubated with the drugs in prescribed concentration” . The full research has never actually been published in its entirety and the brevity of detail on a poster means you know barely any of the important details regarding the methodology. I also looked for any other research that emulated these methods or findings or even cited this paper – nada. And if you lead with your best – this was appalling low level evidence that is really unlikely to be relevant. But hey – here’s the 1 provided reference – make your own mind up! (see how easy that is?!)
I asked for clarification and for papers to support the other 2 claims. Silence.
But actually before silence a bit of ‘How dare you ask!’
That’s when I got a different insight into this forum & arguably a culture that doesn’t foster curiosity & questioning, if that risks challenging the ‘poster’s’ position. And when several incredibly intelligent, kick-arse clinicians quietly contacted me on the side to say, ‘THANK YOU!~ This person posts comments like this all the time & it’s so misleading & someone needed to say something, but it probably had to be you.’ Well that really made me 😥 because it didn’t, you know – any one of us can ask, “Can you share the reference(s) for that?” and clearly we need to more often 🤓
Why are we afraid to question information or ask for references and why are people afraid of the question? This should not be a competition or hierarchy of who can ask or not ask questions. And if the forum that you’re a member of makes it seem that way – then ask yourself, if its doing you more harm than good.
Aren’t we on the same team here? We all have a professional duty of care to our patients to ensure that in looking for quick answers we don’t get incorrect ones that misinform us, our patients and our treatment decisions.
Have you ever noticed that our products don’t work if our patients don’t take them?!🙄
The reasons for non-compliance, dis- or non-engagement, poor patient buy-in & follow through are many:
*My dog ate the instructions * My inbox swallowed the instructions *As soon as I left your clinic, your instructions left my brain
Reasons also include far more credible things such as non-patient centred prescribing. This is what most of us do when we’re full of good intentions but short on time at the end of a consult, so we just throw a bunch of products and a script with them out the door. Arguably many of us make this mistake also because our training perpetuated this relic of conventional medicine and paid insufficient attention to the therapeutic relationship. In contrast, patient centred prescribing recognises the patient as best-placed to find personalised solutions to their very individual challenges, including, decision making around dosing regimes. So while we continue to ensure & oversee that therapeutic doses are used and that best conditions for taking certain things are adhered to – your patient remains the expert in the room about how to actually achieve this – both in terms of when & where in their very real lives – with a little help from us – and what ‘works for them’, in terms of taste, texture & temperature.
That’s right, I said temperature…are you telling patients to take everything at room temperature??
You need to think again – this is something we can safely manipulate with many powdered & liquid remedies (some exceptions of course!) to match patient preferences & radically increase palatability, pleasure and ultimately patient compliance.
Are you like me? I have supplements scattered all over my house – in places that correlate with an action or moment in the day when I am most likely to take them. This is another important element of Patient Centred prescribing, so I work with my patients to identify these easy solutions too. After the gym? In the gym bag. After breakfast as you leave for work? In the key bowl. At work? On the desk beside the computer screen. Keeping taurine in the drinks cupboard in front of the alcohol is another nifty reminder and trick for those looking to ‘pre-load’ and cut down! Tips and tricks like these save our over-loaded memory. They remove or minimise barriers. They make compliance less effortful. And as a result, you know what? They might just get the results we would have expected!
Compliance Changers – Strategies for Success
At the end of an information & insight heavy appointment, formulating a list of products and doses for our patients to take can feel like a bit of a ‘tada moment’, like a magician pulling a rabbit out of the hat. “Here is the solution – now off you go!” Research tells us, however, that treatment-plans that are a co-creation between you and your patient – evolving from a discussion that not only allows them a voice, but a major role in the decision making – are far more likely to succeed. While we are the authority on our medicines, our patients are the authority on what makes them tick & what’s likely to succeed, in terms of taste, texture, temperature & timing! This is called Patient Centred Prescribing and together with some other tips tricks and hacks I share with you in this episode, can really increase patient buy-in, compliance and therefore bring your treatment plan to fruition and fulfilment!
You can purchase Compliance Changers – Strategies for Successhere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
“How much can you misbehave & get away with it?” I listened with fresh ears, as a practitioner asked my son this question recently. I use similar ones with my own patients but hearing it from someone else, I could sit back and appreciate its true purpose and how well it achieves this. Most of us adjust our behaviours, when we can, to ‘manage’ things that cause us problems.
Sure I can eat food I haven’t made myself
………..but once a week is my max. or ‘X’ flares
My energy is pretty good …… but 1 night of poor sleep & I’m back on ’empty’
No impaired alcohol tolerance
………I just never have more than 1
My [insert: gut, skin, energy, immunity, mood] is not a problem
………as long as I don’t miss a dose (of supplement/medication etc)
And sometimes this ‘adjustment’ (or avoidance) is unconscious. Hence the beauty of the question: How much can you get away with, coupled with our understanding of how much ‘room to move’ there should be in a patient who is truly well. So the teenage to early 20s patient sitting in front of us, theoretically, should be in their prime of wide mischief margins, and we are alerted to individuals in this age group who are having to live like an older person, needing to exhibit vigilance around early bedtimes and allowing themselves almost no indiscretions. In contrast, as we age, we understand too, the margin for mischief narrows. Our over-50s selves are unlikely to get away with half as much as did in years gone by but we shouldn’t require the stricter self-care hypervigilance of our senior selves.
And for the patient who answers ‘no’ to everything on your GIT or stress/mood screening questions, for clarification, follow them up with, “and how much can you get away with and still have no issues?”
You may very quickly get a different understanding of what lies beneath and how much ‘management’ is required to maintain ‘balance’ or ‘no symptoms’ or ‘health’ 🧐
The primary objective of MasterCourse I is to realise the true value we can extract from the most commonly performed labs (ELFTs, FBE, WCC, Lipids & Glucose) which constitute the largest biochemical dataset we have on almost every patient. By learning how to comprehensively interpret these labs in an integrated medical framework, using the very latest science, we can extract the gold often buried in this goldmine. Accordingly, we prove ourselves to be the greatest asset to our patients, to other health professionals we are sharing care of patients with and we cut the cost of additional expensive testing, that is less well understood and validated.
MasterCourse I will help you access that gold and has been intentionally designed to match each lesson with real learning– with the time spent in theory and in application. Delivered across 24+ hrs of streaming video sessions with bonus pre-sessions, audios, resources and tools – this MasterCourse is likely to be a genuine game-changer for the way you practise and the potency of your patient prescriptions.
If I could be granted 1 wish regarding all health professionals, it would be that we were all competent in reading Iron Studies. Think that’s overstating the issue? Or not a bodacious enough way to ‘spend’ my wish? I don’t. Especially when you consider the impact of GPs in this space.
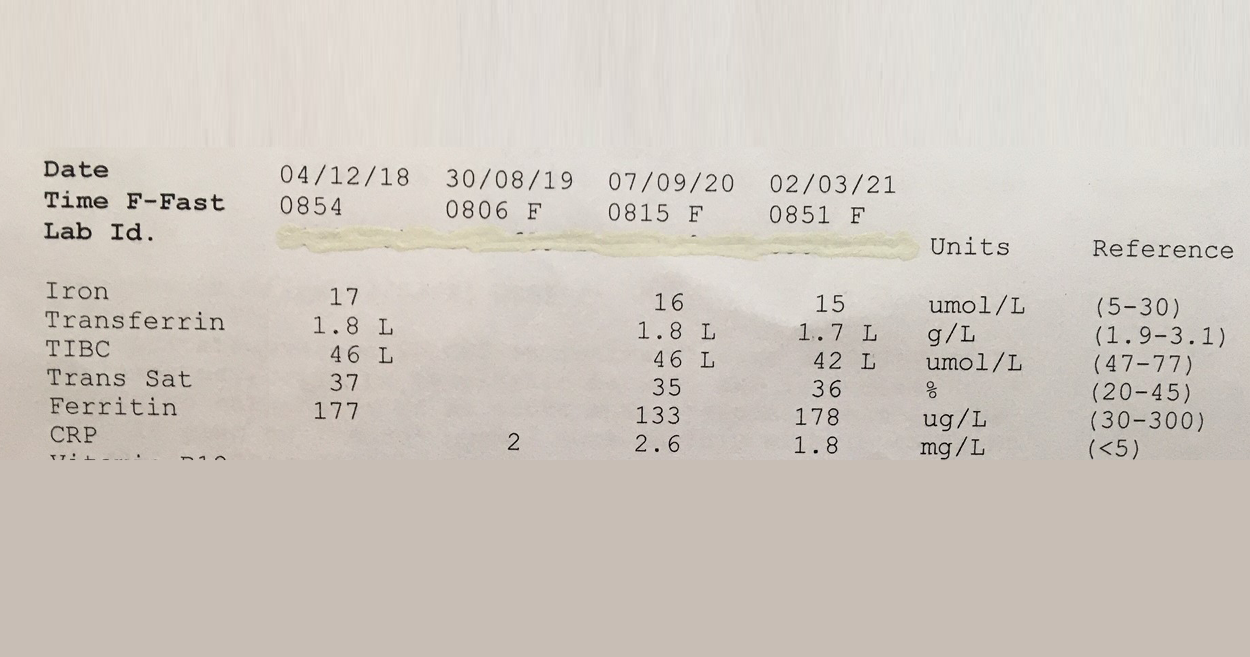
This 57Y male was asked to make a follow up appointment with his doctor, to discuss his ‘abnormal’ results which he was informed constitute Iron deficiency. Consequently he was was advised to start an iron supplement! #@!*
Your thoughts? Revoke this doctors medical licence? Insist on some very du jour ‘re-training’ at the very least? I mean, if you think this Iron pattern flags a deficiency or shortfall, then you’re as good as reading a map upside down and back to front…and written in a foreign language!! The ‘Ls’ in his latest labs flag he has suppressed transferrin, indicative of negative feedback inhibition of GIT uptake of this mineral, secondary to healthy stores or inflammation. And it’s not just that more iron is not indicated but that more iron in fact presents a patient like this with increased and unnecessary risk: to their microbiome, intestinal wall health, even according to the larger longer studies a potential correlation with colorectal cancer risk, if taken long term. Let alone the whole cardiovascular conundrum. Better still this same patient was told a few years back that he might have iron overload! Again the ‘map’ could only have been being read, upside down, back to front to reach such a conclusion!
So the one patient in just a few years by 2 different doctors has been diagnosed incorrectly with 2 different iron issues. Yep.
And sadly I have sooooo many more cases of missed and mis-diagnoses with regard to this mineral. The latest RCPA Position Statement on the Use of Iron Studies, underscores that assessment of iron status and GPs competence in knowing when to do this and how to interpret, is an important part of core general practice. Given it “is the commonest nutritional deficiency state in Australia and is significantly under-diagnosed” This succinct document offers a quick crash course in Iron nutrition for doctors and it hits all the right marks with advice about not ordering ferritin as a stand-alone because “the interactive nature of the three components allows for more accurate interpretation”and this simple but sage advice:
“Transferrin, iron transport protein, tends to increase in ID… A better strategy (than being tricked by Serum Fe) is to report transferrin saturation. A low transferrin saturation in the setting of an equivocal ferritin level is suggestive of iron deficiency. An elevated transferrin saturation is the first manifestation of iron overload.“
I mean seriously, do doctors read these RAGCP resources & recommendations, or is it just me? 🤓😂
Need a rip-roaring review on how to really read iron studies? Or know another health professional who does?!! Consider this Easter Educational Gift Instead of Eggs!! So You Think You Know How To Read Iron Studies?
Overt Iron Deficiency Anaemia or Haemochromatosis aside…do you understand the critical insights markers like transferrin and its saturation reveal about your patients iron status? Most practitioners don’t and as a result give iron when they shouldn’t and fail to sometimes when they should. This audio complete with an amazing cheat sheet for interpreting your patients Iron Study results will sharpen your skills around iron assessment, enabling you to recognise the real story of your patients’ relationship with iron.
‘Hey Alexa, What’s that formula for correcting urinary iodine for hydration status?’ Oh yes, if only she could answer these kind of questions!
There’s no one here by that name but we get these kind of emails all the time [Oh and also for Freya who hasn’t worked here in like 5 years!!😂] But we love them because it means our blogs provide useful, sought after and (we like to think!) really really hard to get anywhere else answers . But hey try it, Ask Siri! We’re always forthcoming with references – not just citations but the full low down and dirty full texts (as long as we’ve managed to get our hands on it!!) and we know which topics particularly hit a spot across our professional group by not just the number of enquiries but how far the actual blog they’re referring to, dates back. So we’ve just received more comms regarding one that’s often on high rotation…a post I wrote on urinary Iodine Assessment & how and why we should adjust for hydration! That was 2014…what a vintage 🤩 Show’s though how topical and tricky this little test is.
The iodine landscape has undergone radical change recently. We’ve moved from recognising the resurfacing of a widespread deficiency, to large-scale food fortification that has failed to correct deficiency in most and produced excesses in a few. Parallel to this, we have the ever growing incidence of thyroid disorders and some radically contrasting ideas regarding iodine’s role in both aetiology and treatment. Micrograms V milligrams? Random urinary iodine or iodine loading test? Important new evidence and clinical experience helps us understand more about how to accurately assess patients’ need for iodine and know when & how to use it therapeutically & when not to!
I’ve seen two 20-year-old young men in my practice this last month who’ve already made a lasting impression on me. The first, is buff, full of cheek and humour while deeply engaged with his health, earnest in his desire to understand his 7 years of daily upper gastric pain, for which he has read much, changed his diet & given up what most 20 year olds would consider their rite of passage and right (late nights and alcohol). The second is pale, gaunt, neuro-atypical, full of tics and avoiding eye contact at the beginning of each consult, only to look me solidly in the eyes as he reveals incredible insight about ‘being different’ & his desire to be able to engage with something/anything so that he can live a more normal life, by the end. What do they have in common?
They’re 20 & trying to make their way in the world. Undertaking all these newly autonomous actions, previously taken care of by parents, including fronting up to a health professional with concerns, seeking understanding and support.
The first, in spite of 7 years of gastric pain and irritation (I can see mum took him to a GP with similar concerns at 13 years & again at 15!!), self-reported extreme worsening with gluten exposure and a family history of similar GIT issues, was not offered a single investigation by the GP they visited but was given a month long trial of a PPI. I caught him 3 days in. Was he feeling less pain? Yes? What does this mean? He has gastritis at best, something more sinister at worst? Does it reveal the cause? Not one iota. But tests for H.pylori, coeliac disease and a few other basic labs, might. Does it offer a long-term solution? Nope – even the GP said , ‘Now this will probably help but you won’t be able to stay on this too long!” While up to 80% reductions in gastric acid, will definitely lessen gastric irritation and pain for most, will a month ‘fix’ anything? Unlikely. Especially when the well-documented withdrawal rebound effect kicks in, once he stops! After a month of actual stomach repair work, he’s feeling dramatically better and yes, we’re still pushing for those test results.
The second 20yo, was seeking a mental health care plan from a GP he’d never seen before. He walked out after 15minutes instead with an SSRI.
With a diagnosis of Asperger’s at 12, ADD at 13 and a series of high level neurocognitive assessments and stimulant trials – how could anyone make an informed decision about appropriate medication for this neurobiologically complex individual in 15mins, while simultaneously ignoring his request for hands-on psychological support? I was a bit stunned. He was too. How long, and how much effort and courage, will it take for him to make another appointment, get himself back to a medical clinic and ask again? He struggles to remember to eat. I’m glad he came. I can’t offer all of the services and support he needs, far from it, but I can listen long enough to ‘see him’, acknowledge that his personal priorities and values are valid and in turn, direct mine in terms of how best to support him. I can also try to encourage him not to give up on getting the support from others he desires and desperately needs. This is not gender specific of course – I’ve heard similar stories from young women. I remember being 20 – perhaps all health professionals need to take a moment to remember what that was like too? 🤔🤗
I know, timing, huh?! It’s almost like I’ve been sniffing around your recycling bins but I didn’t need to of course, at this time of year it’s a fairly safe bet you’re madly winding it back a tad from your most outrageous annual alcohol imbibing. And so are all our patients. To me, extracting accurate information succinctly from patients regarding their alcohol use can be one slippery little sucker. It’s one of the questions people tend to give you a very tidied up answer to, or in fact they’re in such denial they can’t be considered a reliable witness. Think about it. Being a non-habitual drinker myself, I can appear almost saintly when reporting my daily consumption, “None”…but that omits the ‘other me’ that might show up at a conference gala dinner or some live music event, with my volume controls adjusted significantly up…ergh…firsthand accounts anyone? And how often does that happen? Well anywhere between 4 times a week and once a month. See what I mean?
While I’m sure you’ve probably heard me say before, I ask every patient who does drink, what kind of drunk they are because it can hint at their underlying neurobiology, there is a new study that suggests, using a very short 4 item UCLA RRHDS survey, we can categorise patients alcohol use and misuse into 3 types:
Reward ReliefHabit
and in doing so, also be better able to identify the best way to manage them as well.
I’ve been interested in addiction neurobiology for a long time and very much resonate with the work of Koob, which in layman’s terms proposes that we seek intoxication initially for the ‘high’ and then with dependence, we continue to seek it to appease the terrible lows of withdrawal. It has long been known that alcohol use disorder is heterogeneous – there are different types and accordingly the kind of generalised treatment of these individuals proves extremely hit and miss. But articulating the different types and their distinct drivers and solutions has been fraught. Like what makes one alcoholic the functional type who in addition to their long-lunches is a CEO and the one who can’t keep their job? Is it just socioeconomic context or something more? Why are some types of alcoholism deemed also to run more in families and while others aren’t? There are clearly major difference in pathophysiology but what are they? More recently these 3 groups have emerged and this recent study confirms the value particularly in the distinction between those who drink driven by reward and those for relief + habit. It’s a great read but here are some key take-homes:
ReliefHabit
Relief/Habit: You predominantly drink to cope with, or resolve a negative physical and emotional experience (negative reinforcement). You have more depressive features and have more anxious traits than those ‘reward drinkers’.The key to managing this type of pattern is to target negative physical and psychological experiences with ‘downers’ (they calm down an overactive brain that’s on ‘alert’) such as sedatives, anxiolytics, and glutamatergic modulation. (Hint for practitioners: this is where Taurine & Glycine really shine)
Reward
These individuals drink to feel good so they are driven by positive reinforcement and therefore the approach to the helping them should be quite different, with lifestyle recommendations that offer other options for mood elevation such as exercise etc as well and herbal and nutritional approaches.( Hint hint…not the key group for Taurine, more like Tyrosine and Saffron etc)
So…back to my question…what kind of drunk are you & what drives you to drink? As a nation of over-consumers by nature, this is a question we need to ask all our patients
Rachel introduces you to new clinical tools that has been developing to help us all better master the maze of mental health. With so many possible biological drivers: from methylation to inflammation and from gonads to gut, these tools can help you quickly identify those most relevant to each patient and also outline the strategies necessary for redressing these. This presentation comes with an extensive library of resources including pdf of Assessments Tools and Case Study Notes.
I take my job to heart. When someone asked me recently to choose the single value that spoke most to me personally I couldn’t seem to go past, ‘Purpose’. I feel very honoured to have contributed to the learning of so many health professionals in their undergraduate and so many more in their professional careers following graduation and I know that with this comes huge responsibility. Second on my values list (again, possibly unsurprising) is Empowerment & coming in with a photo finish at 3rd:Integrity. Discernment and critical thinking (about information, about research, about reflective practice) are perhaps the eggs in this souffle, helping us all to rise up.
As part of our critical thinking we need to accept a few truisms:
Research changes Experience changes Knowledge changes
Information is not static. So we need to ask ourselves, how long ago did I learn this? How long since I’ve checked it is still correct? And just because perhaps this information came out of the mouth of our mentors or teachers, makes it no less up for regular review. I’m trying to undertake these internal audits on a regular basis. Typically they’re prompted by bloody good questions my mentees have asked me. A question I can’t answer or, more to the point, I can’t answer with full confidence I’ve double-checked my old beliefs and understandings against new evidence recently…these almost always provoke a lost night of sleep for me. Not from sleeplessness per se but due to immersing myself in the latest research and performing a mini informal lit review, bringing out all my old beliefs/evidence etc. Marie Kondo style and asking do they still spark joy✨ (in light of the latest evidence)?! And yes sometimes there’s a little bit of heartache when you have to let your old tightly held beliefs and understandings go 😢
The 1st update is about N-acetyl cysteine. Some of you may have heard me previously question the efficacy of the vegan form. Now that all but 1 Australian product is vegan, produced from bacterial fermentation or purely synthetic, I was wayyyyyyyy overdue to check the validity of my old ideas. Let the record show, I was wrong. Unlike some other nutraceuticals like chondroitin sulphate, wherein the source radically changes the overall structure of the molecule and therefore its uptake and actions – the same is simply not true for NAC.
So those ducks, & their NAC rich feathers, can all sleep a little easier at last…phew! Now the 2nd internal audit well that did cause some tears for me…
We often identify patients who could do with a little glucuronidation first aid: marked dysbiosis, Gilbert’s syndrome, oestrogen excess, cancer risk (especially bowel, breast & prostate) and one of our nutritional go-to’s has typically been Calcium D Glucurate. While there is ample evidence that one of CDG’s metabolites: 1,4 GL – inhibits beta-glucuronidase, is an antioxidant, platelet activation inhibitor and generally all-round good guy to have onboard, new research strongly challenges that oral CDG will convert to this at levels sufficient to support this detoxification pathway. Sounds like we’re overdue for an update on this supplement and when and where it might be useful in addition to how to find the real deal in real food!
My current count is about 13. Lucky for some? Patient advocate, referral point, primary prescribing practitioner, behavioural change motivator, wise business counsel, good empathetic listener, fearless myth buster, researcher, head chef to a group of nats…that’s the toughest hat right there, right?! 🤣
While there is a concern in naturopathy and integrative health that we increase our own load due to our eclecticism – I see this as a strength & part of the appeal.
But it does warrant regular review.
I semi-regularly cry-out, “I just want a normal job, you know 9-5, clock on, clock off.” To which anyone who knows me tends to drop to the floor in a fit of uncontrollable laughter. They’re right of course, I do not have the temperament or the ability to be sufficiently single-minded to work at Coles. And the reality is I do feel privileged and satiated by wearing all my different hats bar just a couple…but this is par for the course and part of the important reflective process we should all continually undertake in our careers: Which hat no longer fits me? Which gives me a bit of headache? We can then re-orient our work and our businesses in a way that tries to reduce, or remove altogether, our time spent in these roles.
“I am completely over giving 101 dietary advice!” I wish I had a holiday for every time I’ve heard a nat with more than 10 yrs experience say that!
“Oh the never ending story of answering my inbox!!!!!!!!!!!!!!!!!!!!!!!”is another one on high rotation in our ranks.
These ‘lost loves’ and potential disproportionate time wasters should never be ignored & simply endured but should instead be met…head on. The more I hear about different practice models & observe my own business over 20+years, the more I can see that when a practitioner is losing too much time or job satisfaction, wearing some of these hats that no longer fit, the less financial growth and sustainability their practice model holds. I know…them’s fighting words! Anyway, I’ll be talking about this and the delicate balance of our mild super-powers V our soft underbelly at Vicherbs monthly meet-up Sept 26th if you live in Melbourne and want to come along the join in the conversation. I think it’s a good one that we need to keep having.
The Group Mentoring program provides integrative nutrition practitioners with monthly sessions of the most accelerated form of post-graduate education and clinically relevant skill development. Join this online 12 month program of like minded professionals and work with Rachel through real clinical cases and questions presented by each member in a collegiate setting. If you know you want in for next year already, get ahead of the queue and email us: [email protected]
“Rachel’s mentor program is something I look forward to each month and I feel very privileged to be one of her mentees (or mintees as she likes to call us). Each session is action packed with so much information shared that my brain gets a lot of dopamine hits! Rachel has a rare talent of teaching in a way that makes the most complicated information easy to understand, and even fun! The learning doesn’t stop after each mentor session. The group, including Rachel, will share research and continue to follow the cases shared. Amazing value for money. I know this is something I will want to do my whole career…there is always something more to be learned.”
Breaking up is hard to do (sounds like the name of a song!) but it shouldn’t be! I got an email this week from one of my gorgeous long-term mentees in the vein of a ‘Dear John’ letter. She carefully, beautifully gently let me know… “I’ve found someone else…”
“This is not an easy decision as I have major Rachel Arthur FOMO and visions of my knowledge falling down a deep crevice and never coming back. My motivation for this decision is related to my strong interest in women’s health. I have an increasing number of complex cases around this topic and have sought extra mentoring and I am turning into a mentoring junkie. Now there is nothing wrong with this in theory and a recent post you did about all the mentoring you do and mentors having mentors I saw as sign to keep on seeking mentorship but again that was the RA FOMO speaking… Anyway, I have struggled with the perception this might relay – that I think I’ve got it all covered and I simply don’t but I do think this is the right thing for me at this time.
Thank you Rachel for the exponential help you have provided me since I started mentoring in 2017 and for the level of knowledge and commitment you bring to our profession. I am truly grateful and proud to have been a RA mentee.”
This email really made me really smile – how can this not be good news??? This type of letter or break-up email can have the sender feeling a bit apprehensive about a possible negative response but as I read the email I couldn’t suppress a smile from ear to ear! Not because I’ve got one less person to mentor and more time for lazing around Byron’s beaches with all the instamummies 😉 but for me there was nothing but good news in this development… I love witnessing this practitioner’s growth, their movement into a new field of specialisation and I celebrate this decision. I still have my own mentors…and not just one by the way, but several due to the expertise of each – mental health; herbalist; heavy metals etc. It’s always about finding the best brain’s trust for the job at hand.
I want everyone to find their best mentors to support them in each & every stage of their career
as an integrative health practitioner.
Over the years I’ve received amazing feedback on my mentoring services and often the misperception that my knowledge infinite! Yes I am a journal junkie and I do have 20+ years practice under my belt but…I believe a good mentor has their own mentors. Your mentors may change over time to strengthen different muscles or skill sets and it’s knowing where to look for answers, how to always apply critical thinking and developing your own brains trust tha.
Rachel’s hugely popular New Graduate Group Mentoring, which launched this year, is designed to help anyone who wants support transitioning from student (or lapsed practitioner!) to Naturopathic or Nutrition clinicians with a difference! This online 11 month program is a great way to develop your confidence, skills and knowledge. The bonus with these sessions is you’ll find your tribe, gain support and radically build your toolkit. Applications for 2020 open in October – you can put your name on our wait-list now for this and all other groups by emailing us at [email protected].
I’ve had a bit of ‘a bee in my bonnet’ this year. I heard that! Ok, arguably it extends a little further back…like my whole career! But if you’ve seen the topics I’ve been speaking on at conferences in recent months, you’ll know exactly the soapbox I’ve climbed up onto. Inter-professional communication & collaboration. My particular focus (naturally 😉 ) has been current issues regarding the sharing of, and access to, pathology results for our shared-care patients. However, in the face of several distinct threats to the practise of both naturopathy and medicine in Australia of late, especially in the form of anti-collaborative rhetoric/push affecting both professions right now (read PHI reforms, promptly followed by proposed MBA review..if you haven’t read this regressive and repressive set of recommendations you seriously must), the question of how to improve collaboration in order to ultimately serve our patients better, has never been more urgent.
Last week, at the ICCMR conference, I outlined the current barriers for naturopaths to accessing patients’ pathology results (current and historical) and the heightened risks that this results in, either because of incomplete information or because of the subsequent direct pathology referring by naturopaths. Yes, bypassing the GP and another set of trained eyes on your patients labs comes with risks. I also spoke to the opportunities that await us if we can overcome this: in terms of improved patient outcomes, reduced risk, more economically responsible public health budget spending etc. etc. need I go on?! In the Q & A following my presentation, a doctor in the audience made two very important contributions, which deserve some additional air…she said:
“Shouldn’t the patient ultimately own their own pathology results? Then it would be a case of them electing who has access to these: their GP, their naturopath, their osteopath. Rather than the other way around – after all, we are all supposed to be members of their health care team, right?”
She said it. Not me. But I applaud her. She’s right of course. Right now, under the current proposed changes, we and integrative health care delivery and patients’ right to choose and self-direct their healthcare and public health budgetary burden…are all under threat of de-evolving. Right at the time when, with the current chronic disease burden and predicted public health budget blowouts, it should be all hands to the pump! Who has ever conducted a cost-benefit analysis of what integrative health care (successful patient sharing between naturopaths and GPs /specialists) saves the government? No one is my guess and when I proposed I do exactly this for my PhD on a particular parameter some years back, I was not so subtly told, that in spite of a great application, given the primary funding of the research group was from government, and a clear conflict of interest with the head researcher who was also a government advisor, ” my proposal was not in line with the current directives”. Yep.
Last week, a dear mentee of mine mentioned that a GP one of her patients sees responded to her respectful correspondence regarding their shared patient with absolute terror, citing possible de-registration if they are seen to be collaborating or interacting with her in any way…assuming the MBA changes go through. This doctor then decided the lesser risk, was to cease communication with this other key member of the patient’s health care team, not refer the patient for any follow up investigations (including those representative of basic duty of care) and certainly not enable access to any pathology results for this patient from the past or in the future. My mentee’s exemplary response to this doctor:
“My apologies for placing you in an uncomfortable position. I do understand the restrictions and guidelines GPs must work within for Medicare and AHPRA and understand that as you are the requesting practitioner you are liable for any pathology referred for. I make this clear to all my patients and that my referrals are on a request base only and it is up to yourself or the requesting GP for the final decision. I only try and request pathology through a GP or other medical practitioner to try and minimise both risks (of only myself viewing these labs) and unnecessary costs to the patient.
…’X’ has currently been seeking medical and alternative treatment for over 2 years and yet has had no change, if not a worsening of his condition and when I saw them 2 weeks ago, it was my understanding that not even basic assessment of full blood count, liver function and other general health markers had been completed. I had advised X that not all pathology may be covered under Medicare, and to come back to me so I could send him privately for those tests not able to be completed under Medicare. My apologies this was not made clear to you at the time of his appointment.
I take pride in my evidence-based approach to nutritional health in my practice, and work frequently with other patients’ medical practitioners in supporting their health. Thank you for your time and I appreciate your thoughts on this matter”
If the patients’ best interests are no longer the primary goal, as decided by bureaucrats, both government and organisational, is it time to ask the actual health professionals to please stand up?! Is it tipi-talk time for practitioners from all disciplines? Growl over.
Want to ensure you are writing professionally to other health care practitioners? Then our recording and resource Dear Doctor, is for you!
In this 45min podcast Rachel succinctly covers the serious Do’s and Don’ts for your professional letter writing. Rachel gives step-by-step instructions and examples for key phrasing and clear medical justifications, what terms to use when in order to come across respectfully, and how to present urgent red flags without sensationalising. This podcast is will help your professional letters improve collaboration for you and your patients need.
Help!!! I’m about to share the stage at the 3rd International Acid-Base Symposium on the 25th-27th Jun, with the best acid-base researchers in the world, all of whom I actively stalk (well read and recite everything they’ve ever published but close enough!) I’m terrified and excited in equal doses…but urgently need to change my presentation approach because until now I’ve had the privileged position of simply fulfilling the town-crier role, announcing far and wide the findings of theirincredible research into acid base physiology and their findings about impact of chronic mild metabolic acidosis. But I can’t quote Arnett to Arnett! I can’t tell Dawson-Hughes about the incredible insights of Dawson-Hughes’ large body of work in this area! Oh my Goodness (cue, shaking knees), I’m going to meet Thomas Remer…of Potential Renal Acid Load Formula Fame!!
Yes, my partner is a musician and through him I have brushed shoulders with all kinds of famous…but nothing that has made my heart beat quite this fast!
Quite the month for it, I hear. My inbox has run hot with practitioners deeply concerned about some serious finger pointing that’s been going on.
The fingers in these instances have belonged to medical practitioners and the direction they’re all pointing, is seemingly at any complementary medicine their shared patient is taking.
Here’s a couple of good examples: “Your high blood pressure is the result of the combined mineral formula you’re taking!” These were the words of a GP to a 50 something female patient when he discovered she was taking a calcium, magnesium, potassium containing formula. The patient was hypertensive at the initial appointment, at which time the naturopath encouraged her to actually seek review, assessment and prescription of an anti-hypertensive, however the patient declined. The nutritional prescription was recommended in response to high acidity (raised anion gap) and prematurely low GFR (impaired renal function). Patient’s HBP continued to be problematic so the next doctor she sees, points the finger and says, it must be this product!
Would anyone like to explain that to me? In fact, that was my advice back to this very concerned and understandably rattled practitioner…just to cordially request the GP to outline the mechanism by which this might occur. (more…)
Ever wondered where on earth (or Mars?!) I came from? As much as I can’t keep quiet on some topics, my personal journey to here has been a bit of closed book to many. Recently during an interview with Andrew Whitfield-Cook from FxMedicine, which was supposed to be strictly about postgraduate education paths and the desperate need for mentoring, internships etc for naturopaths, the sneaky devil got me to spill the beans on a whole lot more!
Having been involved in so many aspects of naturopathic and integrative health care education over the past 15 years, of course I do have a lot of ideas about how practitioners can best accelerate their learning and development, the need for more independent education and the importance of fostering critical thinking.
I think you already know that I feel passionately about this but do you know the whole story? Who I have been mentored by and how I continue to tread the path of the ‘student’?(more…)
May was the month of teenage girls presenting with severe digestive problems, especially ‘food intolerances’, leading to avoidance of specific foods and at times significantly reduced food intake overall. As integrative health practitioners, validating and creating insight for clients on the nature and source of their food reactions is our bread and butter, right? Is it wheat? Dairy? Gluten? FODMAPs? Salicylates? Oxalates? We are not surprised by how many ‘sick’ patients we see in spite of a theoretically ‘healthy diet’ – healthy for others perhaps but not for the individual in front of you, right? But what if I told you that each of these teenage girls had a BMI < 18 kg/m2, does that change your opinion about your role? Would you assess, monitor and manage these teenage girls differently? You should.
Take the example of one of my clients: 14yo female with a BMI 16.3, who had her first confirmed food reaction under 2yo with failure to thrive, which was attributed by a paediatrician & dietitian at the time to severe salicylate sensitivity. She underwent jejunal biopsy at 3yo for suspected coeliac disease, due to ongoing concerns and a primary relative with CD but it was NAD. In the 11 years since, there have been a couple of other digestive diagnoses based on solid evidence, such as mainstream stool PCR testing. So surely, the fact that she is underweight & that she skips lunch at school due to digestive discomfort is proportionate and explained by her organic digestive issues. Or is it?(more…)
Recently, I posted about my very positive experience of the AIMA NZ conference, prior to that I was gabbing on about the upcoming ACNEM Brain Health conference in Melbourne in May and now I am going for the conference hat trick! I want to revisit a really impacting lecture for me at last year’s Australasian Society of Lifestyle Medicine (ASLM) conference, delivered by the Emeritus Professor Mark L. Wahlqvist AO, BMedSc, MBBS, MD (Adelaide), MD (Uppsala),on the relationship between ecology and human health.
Why did I find his talk so impacting? Why should every integrative practitioner take the time to watch this?(more…)
Just back from a truly wonderful Australasian Integrative Medical Association (AIMA) conference in NZ. I don’t know what it is about the land of the long white cloud but they seem to produce some of the loveliest, most earnest health practitioners and this conference reflects this, setting itself apart each year as a result of its very organic mix of speakers (general practitioners, naturopaths, nurses, specialists) who are all equally embraced and lauded. To boot we had medical students invited to attend this year and guess what, these 20 or so med students…they stayed for the full weekend much to everyone’s surprise(!), loved it and want more. Really. At the AIMA NZ conference, on the two occasions I have spoken, I feel a sense of coming home…no I don’t mean I am about to move there (too cold!!) but I mean coming home to integrative medicine.(more…)