Wow, menopause is really having a moment, isn’t it? Or is that just me (and my mates who are all somewhere on that perimenopausal path)?! But seriously, medical perception of this reproductive transition is undergoing a revolution right now—widening the lens to take in more diverse potential presentations and lengthening the period of impact recognised both ‘before, during, and after’ that last, last…no hang on…last period. But I fear we are at a crucial crossroads. Anything could be related to (peri)menopause, but not everything is or should be.
There are several other conditions whose onset tends to rise or peak at the same age and stage for women, and due to their shared features, they get missed & misdiagnosed, misattributed to that!(more…)
Any steps towards inclusivity in societal & cultural terms are cause for celebration but in medicine, that can come in the form of a ‘diagnosis of inclusion’, the opposite, of course, of a ‘diagnosis of exclusion’ and potentially as slippery and loose as it sounds. That’s the somewhat precarious position we find ourselves presently in with perimenopause and menopause. With greater recognition of just how long health effects can kick in before there are any cycle changes [2-12 years for those of you playing along at home] and the widening lens now taking in the diversity of such health effects, women’s health has had a win. But, I would argue, this is not without a double edge. After all, aren’t we, as a result, more at risk, as women, of having everything attributed to “just ‘the change’, love”, and, in turn, going to be offered sex hormones more often as the solution?
Over the years I’ve observed an increase in the incidence of practitioner paralysis. This occurs typically & understandably in the face of fearmongering. A good example is in the area of so-called ‘methylation medicine’ where we’ve been lead to believe that writing ‘the right’ nutritional prescription for patients requires a) their full gene profile, b) a knowledge of biochemistry that no one outside of a legit biochemist should have (!) and c) a bordering on perverse interest in in vitro research looking at how these pathways interact with different nutrients. And if we, as mere mortals (and naturopaths, nutritionists, herbalists or integrative pharmacists or GPs at that), are lacking in any of these WE WILL STUFF THIS UP GLOBALLY and put them on THE WRONG THING THAT WILL BE CATASROPH*C! Note: fearmongering always uses caps 😉
This stems from the misguided belief that ‘biochemistry alone maketh the man’ and ‘SNPs should write the ‘script!’
And the source of these falsisms are, what I refer to as, ‘Wallys with wall charts’. As impressed as we might be by individuals with brains for biochemistry or genetics, we should not let this overshadow the knowledge that health and disease are much more than 1 or 2 facets of your gene profile and how this may predict the pace of a few out of a million chemical reactions. Right? I mean I doubt any of us working in integrative health would intend to be so reductionistic and yet here we are with practitioners forgoing clinical (and RCT) evidence over that derived from in vitro with respect to supplements like SAMe and N-acetyl cystine, or worse still, taking as gospel, ideas that have come from pure hypotheses, based on 1 SNP out of an individual’s whole gene profile! This has infiltrated many areas of naturopathic and integrative medicine and certainly gotten the best of me at times too. But I am pushing back. Enough is enough. We humans are not our gene profile and holistic practitioners like us – know the manifold influences upon our health and wellbeing better than just about anyone else. And if you feel a bit lambasted by my little tirade – know that I have to give myself this very same talking- to every now and then – when I fall under the spell of Wallys and their wall charts!
In part one, we discovered the pro-drug nature of SAMe, revealing why evidence obtained from in vitro evidence can not be used to support either favourable claims or warnings. In the 2nd instalment we examined up close the misunderstandings about SAMe use in conjunction with antidepressants and clarified the real causes for concern in mental health clients. In this 3rd and final part we dissect claims and ideas about the success or safety of SAMe as a supplement with respect to methylation genetics and stages of pregnancy. All up this is indeed one BIG SAMe rethink that we reshape and re-inspire you about its prescription.
You know the saying, ‘If I had a dollar…’, well there’s so many ways I could finish that sentence, especially in relation to the most common questions I’m asked by praccies on a weeklybasis and ‘Can my patient on antidepressant ‘X’ take SAMe?’, would be in the top 10! While many of you might be mouths agape reading this, I bet the cause of that comical expression is not the same for everyone. Yes, like you, they’ve read the mandatory label warning: ‘individuals who are using prescription antidepressants or suffer from bipolar depression should not use this product unless under the supervision of a healthcare practitioner’ – but let me ask you, how do you interpret that? Turns out there are several interpretations and the most common is the most incorrect.
Yes you heard me. It’s time to remove that stain on SAMe’s reputation and take this nutraceutical, lauded amongst researchers and clinicians internationally for its excellent safety profile exactly in that scenario, in combination with antidepressants and other psych meds, out of the naughty corner – where it was mistakenly put in the first place! [No one puts SAMe in the corner 😂]
But I’m in no doubt many of you will take some convincing and while I am armed and dangerous ready with the answers, some will want to hear it from more than just me (and I 🙌 you ) Easy then – just read the research – take these for starters this one, that one, oh and this one – but there’s plenty more! Once you have, you’ll likely be scratching your head and asking yourself as I did, ‘How did we come to be so misinformed and come to a place where SAMe is so misunderstood?!’
I can answer that too 😉 And then for good measure I hope your brain pings you straight back to that warning on the SAMe label to follow up with – and what is the actual correct meaning and take-home of that label warning then?!🤔
In the previous Update in Under 30 episode we established where are lot of the misunderstanding originates with SAMe, in particular from lab based research that has little-no relevance on the effects of taking SAMe as a supplement, given what we understand now about its bioavailability and pharmacokinetics. While this helped us contextualise such ideas and get some serious perspective on the camp that exudes mild-moderate SAMe hysteria (arms flailing like the robot from Lost in Space, ‘Danger Will Robinson!”), supplemental SAMe is not right nor safe for all. And that is indeed something we need to sharpen our tools and our skills in recognising, monitoring and managing. Just a little somethin’ for your Christmas stocking & all those lazy hours on the beach you’re banking on over the break 😉
You’re welcome🤶
The Big SAMe Rethink Part 2
In part 1 we established where a lot of the misunderstanding originates with SAMe, in particular from lab-based research that has little-no relevance regarding the effects of taking SAMe as a supplement, given what we now understand about its behaviour in the body. In this instalment we go on to examine the evidence that led to the mistaken belief that SAMe was not safe in combination with pharmaceutical antidepressants and explore what the real safety concerns are with respect to its use in mental health patients. This audio comes with a great resource that helps you to both prescribe and supervise the taking of SAMe in your depressed patients, minimising risk and optimising outcomes.
Recently a very experienced practitioner who uses SAMe frequently and successfully in her patients and also delivers education said to me, “I don’t know what I am doing wrong – practitioners still come back to me with cases where they’re throwing 8 different products at a patient to ‘lower histamine, improve mental health and support methylation’ instead of using just one – SAMe!” I laughed and said, whatever you’re doing WRONG in trying to teach people about SAMe I am doing WRONGER and for LONGER!! I’ve been trying to encourage and inspire confidence in prescribing SAMe for 2 decades now and still some of my most loyal listeners, are like, ‘I still haven’t prescribed it, I am too scared.’ 🤯
But I think the fear factor around SAMe occurs for several reasons: Misinformation – there is a LOT of misinformation about HOW SAMe works and WHAT kind of power it wields therapeutically Misunderstanding – this comes from a couple of key misunderstandings about drug interactions and SAMe pharmacokinetics & pharmacodynamics Mystery – even for me, SAMe has had an air of mystery about it, nagging, seemingly unanswerable questions that can undermine our confidence and certainty about its appropriate use and safety
I get it. And given the studies employing SAMe as a therapeutic agent date all the way back to the 1970s and continue to today – in psychiatry, hepatobiliary disease, cancer etc – there is a LOT of information that has been gathered overall and a LOT of old ideas/theories/speculation replaced by understanding thanks to better methods and models of scientific enquiry. So I decided it was time for me to confront this ‘man/molecule/medicine of mystery’ head on, conduct a completely updated literature review of SAMe and along the way – challenge many of my long held beliefs.
I thought about calling this latest episode, ’30 Things You Don’t Know About SAMe’ – and calling it like a horse race because in all honesty I learned THAT MUCH!
But I settled for: The Big SAMe Rethink – inspired by one of many pivotal papers which helped to revolutionise my understanding & approach to this nutraceutical which you can read yourself here. Misinformation, misunderstandings and mystery be gone (ok well most of it anyway!) – by filling in the gaps in our information that previously fuelled these – we can move forward with much greater confidence and clarity and we now know where the real safety concerns exist.
The Big SAMe Rethink Part1 Do you feel like you need to pick a SAMe side? Researchers and clinicians, alike, seem divided in their opinion about its therapeutic capacity and certainly its safety. One side are the ‘naysayers’: ‘SAMe can’t possibly be effective for both depression and in hepatobiliary conditions and and and’. Keeping them company are the ‘doomsayers’, preaching danger and destruction should we prescribe this ‘universal methyl donor’. But the other camp can seem just as fanatical and far-fetched at times: ‘it’s good for just about everything with zero safety concerns’. The divide and differences come down to origins of evidence and, once again, the truth lay somewhere in the middle. This new information on SAMe’s behaviour as a supplement will prompt you to rethink so much of what you thought you knew, whatever side you’re on!
Gone are the days, thankfully, when we could all easily identify any individual taking an antipsychotic 1) because they were the marginalised ‘mad’ and 2) stigma and shame were rife. With the seismic shift that has occurred both in psychiatry & society we now know so many of the people we live or work with just might be taking ‘something’ & under any number of diagnostic labels. And increasingly the ‘anti-psychotics’ are not reserved for the psychotic nor the ‘mood stabilisers’ for the manic. Which can complicate things – especially when it comes to their thyroid.
You see it’s a mistake to think that only Lithium spells trouble for thyroid function
The latest piece of evidence from a study of over 25K BPAD patients in the US tells us this common misunderstanding makes us prone to not recognise all the other patients in whom their psych meds are disrupting and in fact driving thyroid (dys)function. Though Lithium carbonate remains the most noxious goitrogen due to its multiple disruptive mechanisms – the rest of a large group of Psych meds (yes even antidepressants!) are impacting to the point of effecting the thyroid function test results you are likely to see in patients taking these. And this is something we need to be alert to – these medications are essential, non-negotiable in most scenarios, but a secondary hypothyroidism is not their intended goal and can make matters worse.
Cue our growing understand of psychoneuroendocrinology, of course. Your HPT is influenced by your mood & vice versa
I told you I’ve rekindled my love and passion for thyroid pathology and this is one of the many elements I got to include in our latest updated training * Advanced Thyroid Assessment* and the upcoming MasterCourse. But I just had to hit record on this one aspect immediately – because if we don’t recognise the cause we are likely to be throwing all the wrong things at the thyroid – to no avail. This kind of subclinical or overt hypothyroidism is not due to nutrition per se, or due to some other kind of HPT re-setting influence like inflammation…it’s the meds & that necessitates different solutions & a much bigger conversation…so join me…
Many of us recognise the bidirectionality between thyroid function and psychiatry wherein ‘stress’ and mental illness can produce a predictable pattern and shift in TFTs and vice versa but regarding the question of psych meds as potential goitrogens, many of us are mistaken in thinking this issue begins and ends with the use of Lithium carbonate. As it turns out, an increasing number of these pharmaceuticals are recognised to disrupt thyroid health & activity via a variety of mechanisms both centrally and peripherally & as a result many patients may get stuck in a vicious loop of worsening thyroid function and mental wellbeing. – until someone calls it – someone like us.
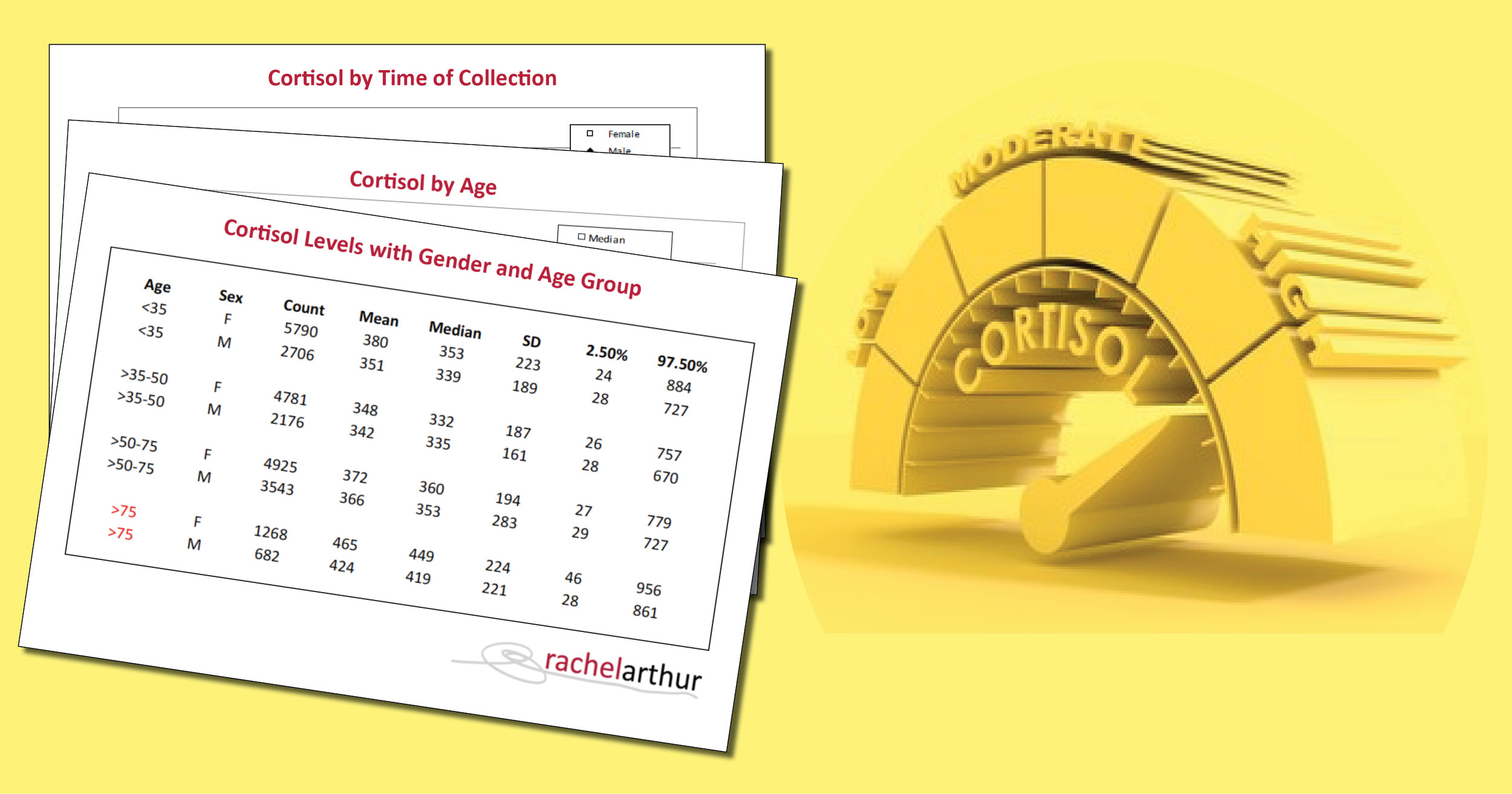
And all 35K results have been collated, analysed & made available so we can be better informed regarding expected Cortisol values based on sex (spoiler alert: women win & when I say win I mean track higher generally🤷♀️), age & life-stage. This month in our Mental Health Primer program I’m talking about how to look at labs through a mental health lens – from the most routine (ELFTs, FBE etc) to those 2nd tier assessments that we might sometimes recognise to provide essential information about our patients. HPA assessment is such a big one in mental health and depression, specifically, because of the 2 major subtypes: typical (can’t sleep, can’t eat) and ‘atypical’ (over-sleeps, over-eats). We all know that in ‘typical’ depression – the subtype we tend to over-focus on due to its dominance (and sometimes therefore miss the atypical patient at our own peril), there is most characteristically a hyper-cortisolism, with poor negative feedback at the HP, allowing for these higher circulating levels. But is your depressed patient with sleep disturbance experiencing higher than healthy or expected cortisol release? No, not necessarily.
You see even the 2 subtypes can have sub- sub- types. Patients can have a diagnosis of either form of depression but have PTSD features or other psych and non-psych comorbidities that make it more probable that their adrenals and Cortisol are turned to ‘low’. As in unhealthily & unhelpfully low.
And that would then necessitate a very different approach to treatment – a different choice of herbs and nutrients etc., right? As we’ve discussed before, accurately capturing cortisol is a task not for the faint-hearted! Cortisol demonstrates such dynamism – not just regarding time of day and pre-test and test exposures & experiences, but also your geographical location in the world (!), not to mention choice of medium and which aspect of the HPA story that specifically reflects. But for some patients it is essential for best management that we ‘feel the fear & undertake an assessment of their HPA function anyway’! But we need to ensure we get results we know how to accurately interpret.
I use different cortisol captures (saliva, urine, blood) to answer different questions – but if I want to understand the HPA functionality and performance and feedback…then measuring cortisol alone is not adequate – and we are back at blood, which offers us, as always, to go beyond a simple numerical: ‘adrenal output’ & also answer the question: “What were the adrenals TOLD to do?” aka where does any actual mismanagement lie & likewise, the key to correction.
I have! And just recently a stark contrast between the results from 2 different methods of cortisol capture in the same patient illustrated just how likely this is. How do we ‘capture’ something so ‘dynamic’ and interpret anything of substance from a ‘static’ assessment technique? But rather than throw up our hands and throw out the whole attempt to measure cortisol, we can improve the rigor, reliability, and real-world meaningfulness of our patients’ results by refining our timing of tests, choosing the medium wisely & manipulating test conditions to answer specific questions about their HPA function. Great ready reference resource included!
Did I say, ‘Our Brain’? 🙄 Maybe it really should be, ‘Their Brain…on Drugs: what recreational substances reveal’. While infinite self-analysis is an occupational hazard for health professionals, when we use our detective powers for good not evil, our patient work-up benefits. But of course, it is impossible (and not desirable) to avoid all self-reflection. Let me introduce myself: I am a high dopamine gal. How do I know? Because a valid accurate test of my neurotransmitters told so? Heck no – outside of lumbar puncture there isn’t one! Because my reactions to recreational drugs did.
A self-proclaimed ‘cheap date’, with amplified & protracted intoxication experiences from small amounts of any psychoactive & no, sadly, not always pleasant. I specialise in visual trails, a known trademark of dopamine surges, when under the influence of even just a few drinks – much to the bewilderment of my loved ones.
Some even famously once questioned whether I was, in fact, safe to ride a push-bike 500m on Lord Howe Island after 2 glasses of prosecco. Stop! I heard that murmur, this has nothing to do with my liver & its handling of such substances. [How rude!😆] I can cite ample other evidence in support of this. This is also not simply due to being a teetotaller and therefore having not (yet) developed tolerance. This high dopamine diva-stuff is echoed by my non-intoxicated ‘normal’: vivid dreaming, impulsivity, and bankable bad reactions to Vitex: ANGER (capitals intended). TMI? 🙄🤐
When you know the questions to ask, the answers to lean in further to, and then the way it can all come together, to create a neat little trail of breadcrumbs we can follow all the way to our their neurochemistry…you can find the gold.
The thing is – and I remain annoyed and frustrated by this to this day – our ‘schooling’ was not very ‘sex, drugs and rock’n’roll’. New grads tell me nothing has changed. In fact, these kind of topics were absolutely omitted, in spite of the claim we consider the ‘whole patient’, the whole health story! Interesting, hey? Nod to those working on the ‘sex’ bit in holistic health: Moira Bradfield-Strydom, Sage King, Monica Francia, Daniel Robson…love ya work! Now for the drugs! Do you know what recreational substances can reveal about your patients’ neurochemistry?
Finding out about your patient’s historical or current psychoactive appetites and adventures (and yes that could be as commonplace as alcohol), is not purely for the purpose of collecting yet more data on their ‘health behaviours’. Nor yet another cue for casting judgement! It is an opportunity to take a can-opener to their cranium, open that baby up & take a look inside. Without making a single incision!
But there’s a bunch of background knowledge you need to polish up on re psychoactive MoA and what each part of your patients’ experience (1st vs subsequent exposures, threshold for intoxication, the nature of the intoxication itself, & the possible aftermath) can reveal – as an inventory of their CNS materials and machinery. All the while having a process to follow to ensure your evidence is leading you to the right and reasonable conclusion. Come with me and let’s follow the trail of breadcrumbs your patients recreational substance experiences have laid out for you…🐓
Our Brain On Drugs – What Recreational Substances Reveal Part 1
Ever wondered why not everyone loves MDMA given it’s the ultimate love drug? Or why some of your clients are exquisitely sensitive to the aftermath of psychoactives and routinely, reliably experience ‘rebound’, in the following days while others ‘bounce’ seamlessly from a big night into the boardroom the very next morning? What do these things tell you about the state of play of their neurotransmitters & their neurochemistry? So much more than you expect and given the only validated accurate assessment of an individual’s neurotransmitters is via lumbar puncture…with far less pain and inconvenience. This is the first of a 2 part discussion.
&
Our Brain On Drugs – What Recreational Substances Reveal Part 1 Part 2
The 2nd part of this discussion goes into the detail of the MoA of each recreational drug class and what our patients’ encounters with these reveal about their neurochemistry. It also includes a resource we’ve developed to help you follow a process, in your review and rate the quality of evidence you have, to ensure your extrapolation and interpretation are well-founded. **WARNING OVERSIZE LOAD AHEAD** There is a bonus case discussion that puts into action everything outlined in both parts and the process of qualifying the evidence.
You can purchase individually Our Brain on Drugs – What Recreational Substances Reveal Part 1here and Part 2 here
or become an Update in Under 30 Subscriber to access both episodes plus the entire library (100+ episodes) of Update in Under 30 audio’s and resources here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
When was the last time you ‘got on the gear?’. Wait, am I showing my age?🙄 The afore mentioned ‘gear’ could be beers or GnTs, weed or hooch, eccies or pingers, ‘nose candy’ or blow. I could keep going! While, anything beyond alcohol, might be purely a historical tale for many of us – during a [ahem] ‘very different phase of our lives’, Australian research tells us that the patients who come to see naturopaths are just as likely to drink alcohol as those that don’t and are in fact about 40% more likely, to have used marijuana or other illicit drugs in the past 12mo. And this was the women in their 30s! You heard me.
Now, this is not a call to action, to dob in a dabbler.
This is instead a wake-up call for all of us, regarding the best insight into our patient’s neurochemistry, that is right there in the patient’s psychoactive substance encounters.
Because let’s get 1 thing clear, straight up – the ONLY valid, accurate, reliable pathology test for the measurement of neurotransmitters is a lumbar puncture. Correct. And anyway, if you’ve been following psychiatric research this millennium, you’ll know that the belief that neurotransmitter quantities are the whole story (or even main players) in neurochemistry, is fatally flawed. So, whether your patient’s ‘alcohol or other’ is purely in the past or in the present, this line of questioning and what it can reveal to you about their neurochemical nuances (high or low dopaminergic tone, shortfall in serotonin, high or low histamine etc) is gold.
Because no recreational substance BYO
Instead they raid your stocks and supplies, get your brain to develop ‘bigger ears’ for some signals over others. Their effects are purely a manipulation of the patient’s existing materials and machinery. And accordingly, here is the great reveal. So, a 30 something patient of mine reports dabbling in all sorts during her teens and twenties. She relays pretty ‘expected experiences’ with each substance – remember these psychoactives are known quantities, we know a lot about which buttons they push and I so I concur that her responses were anticipated & typical. Maybe if anything, she is able to recognise that she had a lower threshold for intoxication compared with other first time users. “But MDMA,” she says, “I don’t get it and boy I tried! Several times!” So, while everyone else felt the love in the room, danced all night to the fantazzmical beats and the orgasmic-optic light show…she felt like she’d taken nothing at all. Aha! This of course would prompt me to ask more questions to help clarify both her serotonergic tone & other instances where she might have encountered oxytocin. And the real insights about her neurochemical milieu (strengths, weaknesses, balance and imbalance) start to form, so too the best way to support her. Don’t miss the real reveal in your patient’s story – that offers to lift the lid on their cranium and let you take a look inside.
Our Brain on Drugs – What Recreational Substances Reveal Pt 1
Ever wondered why not everyone loves MDMA given it’s the ultimate love drug? Or why some of your clients are exquisitely sensitive to the aftermath of psychoactives and routinely, reliably experience ‘rebound’, in the following days while others ‘bounce’ seamlessly from a big night into the boardroom the very next morning? What do these things tell you about the state of play of their neurotransmitters & their neurochemistry? So much more than you expect and given the only validated accurate assessment of an individual’s neurotransmitters is via lumbar puncture…with far less pain and inconvenience. This is the first of a 2 part discussion.
You can purchase Our Brain on Drugs – What Recreational Substances Reveal Pt 1here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
There’s probably some poignant lines from a rap song everyone knows that I could insert here but, alas, Gold FM doesn’t play anything produced after 1999, so I’m none the wiser. What I’m trying to bring to mind, is the potential clash between our reality & our response: we’re not all gonna get instafamous, so the majority of us should probably curb the buy-now-pay-later spending and establish some contingency plans. And while it might seem like I’m just picking on the young folk, this can happen at any age and stage of life. These, in psycho-speak are called Positive Illusions, and are one of the concerns psychologists have about the potential impact of exclusively focussing on ‘the positives’, aka Positive Psychology (PP).
There’s a lot to like about this Gen Z offspring of psychology. And perhaps, as integrative health professionals, a ready-made romance, given both tribes (them & us) believe in health being something beyond the mere absence of disease. That and the fact they give due recognition to the role diet & exercise play in our mental wellbeing…how truly thrilling! Over the last 20 years PPIs (Positive Psychology Interventions not the other ones!) have become so pervasive: schools, workplaces, we’re in an age of the National Happiness Index, we’re overflowing with positivity, spilling over the lip of your coffee mug, emblazoned with ‘You’re Awesome!’ or ‘You’ve Got This!'(Just in case we forget momentarily) But we need to explore the science for and against, to better discern when these messages and tools are a help in clinic and in our patients, and when potentially a hindrance, worse still, a harm.
😁POSITIVITY😁
is extremely popular right now, but an obsession with it & rejection of all things negative (thoughts, feelings, experiences pasted over by something nicer and brighter!) is not necessarily a balanced recipe for mental wellbeing, according to the science.
PP has made a wonderful contribution to how we think and talk about our mental wellness as opposed to just our mental illness. However, there is a critical context in here that’s important for clinicians to understand, in order to use it well, and some thought-provoking criticisms and counter-balances that will help us all avoid becoming as (in)effective as a slogan on a coffee mug. Oh and guess what guys? Assessment first 🤓💪 this takes the guess work out of whether your patient is a good candidate for PPIs and we’ve included two in this latest Update in Under 30 – even a validated mental health screen that only uses positive language for those averse to those nasty negative thoughts and feelings!
UU30 Positive Psychology Its likability & limits
The ideas behind Positive Psychology may resonate deeply with integrative health professionals, for good reason. We have in common a belief that ‘the absence of disease’ does not constitute health & that prevention is better than cure. And PPIs have become so popularised they have permeated into schools, workplaces and most people’s therapeutic interactions, e.g. gratitude exercises, identifying our strengths via a strengths wheel, self-compassion. But do we know the limits of positive psychology? Do we know who it works for and what it means when it ‘doesn’t deliver’ mental wellness?
You can purchase Positive Psychology Its likability & limitshere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
I’ve been hatching this passion project for quite some time. In truth, I can probably trace its beginning back 2 decades, when I returned to practice, after working in psych meds for big pharma. I knew then I had something to say. Because even then I knew that we, as integrative health professionals, could see that food must matter, nutrition must play a part, in the difference between mental illness and wellness and that the solutions were unlikely to be all pharmaceutical, or even that the likelihood of a ‘pharmaceutical fix’ would be improved by adequate attention our nutrition. For those of you too young to know, this was about a decade before the ‘Inflamed brain’, as a model for mental illness, got wings. About 5 years before the psychiatrist, Michael Berk, first took NAC to the world & about 5 years after the first links between methylation & mental health were just being muttered. It was before this extraordinarily expanding field of research even had a name: Nutritional Psychiatry, circa 2015 (thanks in part to Jerome & Felice)
And now it has a name And the evidence is irrefutable But we still need to get the message out, further, louder.
Since then, I’ve mostly shared my ‘something to say’ with you. Entrusting you with passing on the message and the medicine further & it has been an honour and something I work to improve all the time. But every year or so along the way, I had the opportunity to speak to the uninitiated, the non-believers. At medical conferences, to doctors and pharmacists, via in-hospital training of psychiatrists, on large public platforms and each time I did, the same thing happened. The room went quiet, people listened, crossed arms before I began, unfolded by the time I finished, with even the staunch non-believers at the outset, approaching me afterwards, to speak to the impact, the revelations. I had hit a nerve & built a bridge, simultaneously.
So I decided it was time, to indeed ‘say something’ , to more people and more loudly than ever before & I created this video: How Could Nutrition Improve Your Mental Health?
This is something so many need to hear right now. I hope you might share it with your patients and save yourself some precious time in your already over-crowded appointments. Use it as an educational offering, a soil tiller, a ready rationale, maybe even, a ‘step 1: watch this’, for those you’re about to help. With the other health professionals you share these patients care with, so they can better understand the place and potency of your contribution. Family and friends – so they too can benefit and better understand. It doesn’t feature me, outside of my voice to carry the message & it refers them back to you – to ‘us’, those of us passionate about wellbeing, skilled-up in nutrition, who take the time and know that not all mental health solutions are outside of ourselves & an individualised approach that takes the best of each modality is ultimately best for the individual.
Introduction to Nutritional Psychiatry can be viewed here. This 30 min video is an introduction to Nutritional Psychiatry. It is especially beneficial for integrative health practitioners and people working in mental health related industries. We encourage you to use this engaging ‘visual’ presentation to educate your clients by giving them this link. Contact [email protected] if you would like to receive a digital copy to add it to your website or other online platforms.
There are some things we say so often to patients we could record them and just press <PLAY> Like this daily dogma: ‘When you’re under stress, your demand for Magnesium rises and then in turn that can make you more susceptible to further stress, so we’re going to give you some to support you’. But is this actually the whole story? You guessed it, no. (I know I am fairly predictable like that 😅)
Recently, a personal new record – a patient reported ongoing daily use of a very high dose Magnesium ‘practitioner only’ product 8 years after it was prescribed by her then naturopath – and guess what, the patient still hadn’t reached nirvana* not the band! – a transcendent state in which there is neither suffering, desire, nor sense of self
Jest as I may – I think this raises some serious questions. The pervasiveness of our prescriptions when patients are not given an end-date coupled with ongoing access. How (not) effective this intervention was if someone perceives ongoing undiminished dependency on it. And specifically with Magnesium – whether our prescriptions (form, dose, adjuvants, advice) are the problem? If stress is synonymous with a shortfall of this mineral then Magnesium is not a solution to stress itself but the amplified stress response and the stress still requires its own redress, right? But do our patients hear this as well when we press <PLAY>?
Likewise – the BIG doses per serve being recommended might make sense for the minority (seeking potential NMDA antagonism) but are a real mismatch with the majority, who are just stuck in the stress loop and weathering a perfect storm of Magnesium under-supply and increased demand.
I love my minerals as much as, ok more than, the next practitioner but I’m always keen to refine my repletion approaches and oh yes, by the way, there is good data, a meta-analysis in fact, examining how long it takes to achieve repletion using oral Magnesium – and guess what, it’s not 8 years! The latest Update in Under 30 goes into all this and much MuCh MUCH more…you’re welcome 😂
Practitioners working with nutrition appreciate that Magnesium is vulnerable to depletion by the stress response and that in turn, can make people more prone to stress & keep patients stuck in a so-called ‘stress loop’. But do we understand the intricacies of this and how we, as practitioners, can get stuck in another kind of loop – one of endless Magnesium prescribing without reaching repletion? We discuss ways to improve your Magnesium prescriptions – in particular, ‘doping Vs drip-feeding’ and other things to assess & address if the long road to repletion risks becoming an endless one!
You can purchase Magnesium – Stuck in the Stress Loophere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
I’m intrigued by the silence. Hair loss in women is frighteningly common, following pregnancy, menopause & with extreme stress (wait is that a tautology? 🙄) In fact it can strike at any age and for a multitude of reasons. When it happened to me a few years back I also initially responded with silence, terrified that if I said it out loud it would make it real, but when my daughter suddenly asked, ‘Mum are you losing your hair?’ with her trademark attention to detail & exquisite empathy, she gave me the words & a good kick into gear, simultaneously. Now I am fascinated by women’s silence around this generally, how little we share our stories & forewarn others, & as practitioners, the lack of adequate training we’ve had identifying the different types (hint: it involves donning gloves or if restricted to online consulting, knowing how to organise correctly positioned pics) & from there finding the right solutions.
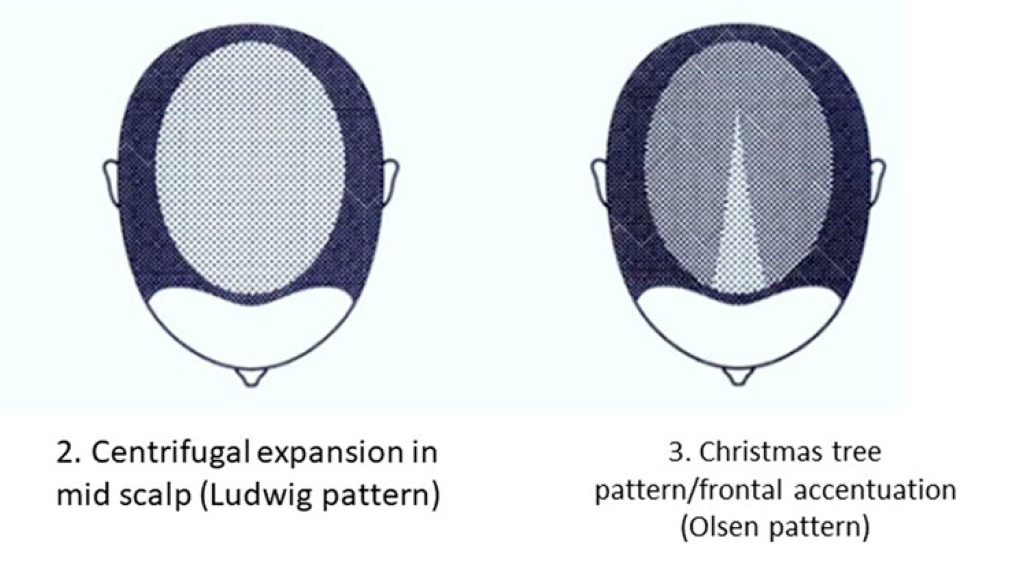
While Female Pattern Hair Loss (FPHL) is the dominant type in women – it only applies to the following pattern:
But alopecia due to stress, thyroid disorders, autoimmunity, contact dermatitis etc will affect different regions of the scalp and with a different onset & progression.
And remember, by the time YOU, the practitioner, can spot a patient is losing hair when they simply walk into the room, they have ALREADY LOST 50%😢 This is why I think we need to push back against the silence. The research is unflinching about the serious psychological impact this has on women – especially in cultures which place so much emphasis on looks generally, and hair, specifically as a commodity of very high value in women. The diagram above comes from a 2019 update on the phenomenon of FHPL and it’s a good articulation of the knowns and unknowns (pssst spoiler alert…it ain’t about androgens!) but let’s never forget the other causes and cures. So let’s make sure as the trusted practitioners women present to so often, we are sensitive enough to have this tricky conversation & skilled enough to help 💪
Stop Pulling Your Hair Out – The FPHL Answers You Need
Female Pattern Hair Loss (FPHL) is everywhere, perhaps you just haven’t been looking. As the leading cause of alopecia in women globally and with 1 in 5 women affected at any age, we’ve all got clients who have FPHL to different degrees. We need to be better able to recognise the early features of this condition which profoundly impairs quality of life and induces depression in its sufferers and that begins with validating patients’ concerns when they report “thinning” or “increased losses”. But what do we do from there? This recording talks you through the assessment, diagnosis and management of FPHL based on a combination of the most recent research and Rachel’s clinical experiences. Once you’ve ‘seen’ FPHL.., you won’t ever ‘unsee’ it and your patients will thank you.
Ok, so maybe I don’t quite look like this after 100 episodes & almost a decade of our Update in Under 30 series but sometimes, in the depths of researching & developing each episode I can feel like this! The idea for this subscription series came out of a desire to share little monthly snippets from my patients and was called, ‘From my desk to yours’, but over time as its following grew, I came to realise how large and valuable a resource – a library of sorts – this was to practitioners. In particular, those hungry for answers, rich in critical thinking but time poor. And so, it evolved to become ‘Update in Under 30’. The topics are remain typically ‘home-births’, from my patients or those shared with me through mentoring but I realised recently, each episode goes through 3 stages of development, something like:
1. Answer a key Clinical Question that’s out there in our professional community generally 2. Answer the often more complex questions clinicians, with significant first-hand experience, have directly asked me about this same aspect of practice 3. Then, last & most challenging, is endeavouring to answer all the questions that I have now after reading the first 50 or so articles to answer the first two questions!!
And let me tell you – that last one can take weeks!!🧐😵🧐 often stalling or stopping all together, the recording or release of an otherwise near-complete episode 🙄 Ask my team – I drive us all batty. But that’s because I recognise the great responsibility I have so wonderfully been awarded and I take that to heart. And I have these questions of yours, of ours, in the driver’s seat when I research (and research again), write and rewrite, record and re-record these [messing with the myth, hey…did you think was my passive income?!^#@}
Take this month’s topic – to celebrate our 100th episode it seemed fitting to pick a BIG one!:To NAC or Not to NAC (that is the question!):
1.In integrative medicine opinions on NAC are divided – among all the fans it has its dissenters – why? 2.If such concerns about NAC are well-founded (and they are) how do we mitigate these? 3.What risks are real & relevant to the kind of plasma values we are likely to see? How precise can we get with our prescription through changes to form, dose, dosing regime etc to ‘accentuate the positives, eliminate the negatives & not mess with Mr In-between,’ as my bestie, Bing Crosby says?
Relax – I refrained from singing this line in our latest update!! But what I do let loose on is a whole lotta juicy answers to our collective questions about a much loved nutraceutical! Happy 100th UU30 🥳
That is indeed the question for most of us working in integrative medicine. While there is hardly a nutraceutical with more therapeutic flexibility and potency – with potency comes risk and responsibility – hence NAC’s dissenters. Many of the concerns regarding the use of NAC are well-founded and come down to its dynamic chemistry in both the gut and blood together with its specific pharmacokinetics. With improved understanding of both, however, to direct dose, dosing regime & duration for more precise NAC prescribing – we can accentuate its positives, eliminate its negatives and not mess with Mr In-Between, so to speak!
And for our 100th session this is of course a SUPER SIZE ME SERVE coming in at about the 40minute mark 🙄🥳
You know when you learn about a ‘new’ dis-ease driver and then you actually have to stop yourself from diagnosing every patient with it? I’ve done this dance with Gilbert’s Syndrome for over a decade, so too maybe have some of you? And while there have been many, many occasions when I’ve been certain it’s Gilbert’s (clear robust & reproducible patterns of high bilirubin without other explanation) there are other times when I’ve been left wondering, and with questions. Like – what about a fluctuating pattern – sometimes ‘within range’ sometimes above or at least high-normal – with no other explanation? What about the patient whose symptom-story is a perfect fit – prone to nausea, early satiety, gut issues, food reactions and anxiety all worse for increased oestrogen…but the total serum bilirubin is 14 micromoles/L? I mean, 14, right? that’s well below the top of that range, but remarkably higher than the majority of women of the same age, eating the same diet. And you ask yourself…could it…be??
It could.
The latest UU30 offering on Gilbert’s Syndrome constitutes a complete overhaul of everything we’ve previously been told about how to recognise and diagnose this polymorphism & it’s going to answer a lot of those ‘could it be’ questions we’ve all had! Known also as familial non-haemolytic jaundice and episodic hyperbilirubinaemia under stress – is everyone with Gilbert’s prone to jaundice? Uh, no. Total bilirubin levels typically have to get to 45 micromoles/L to evoke this effect – many of our GS patients won’t ever get there, some will with increased illness or other stress and may yellow a tad (like a fading bruise), while other patients of mine routinely have a bilirubin at this level but won’t experience jaundice unless they impair their UGT further via doing what they know they shouldn’t: extreme exercise or excess alcohol. The latest deep dive into GS diagnostics
But as much as we don’t want to miss this diagnosis we don’t want to mis-diagnose patients with it either!
Can you spot the difference? Don’t forget total serum bilirubin levels are the net result of haem catabolism – so you need to account for rate of blood production, destruction and of course rule out any biliary dx before you can take a guess at Gilbert’s. Oh and watch out for expected high bilirubin values in the fasting fan(atic)s!
For those people living with Gilbert Syndrome at last the research world & the real one are uniting – with greater detailed documentation of how this very common polymorphism presents and the mark it may make in their health story. However, given only 1/5 with Gilbert’s syndrome actually know they have this condition, who are we missing? This latest instalment rewrites our diagnostic criteria and corrects our past misunderstandings based on the very latest science, while shedding further light on what it’s like to live in Gilbert St.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
[Ahem] Ok let me explain…Several catch-cries from Australian ads have earnt themselves a lifelong place in my head and heart, taking up space where something more important should be, no doubt, but does anyone remember this SPC canned fruit (REALLY showing my age now!!) one, where the little boy chases the grape around the bowl and declares it a, ‘Slippery Little Sucker!’? Ok so this little boy is every one of us when we’re trying to ‘capture someone’s cortisol’ and just like the boy we will eventually achieve a ‘result’ – get a ‘number’ but what in fact does this mean in relation to your patient’s HPA axis, stress perception, responsivity, recovery etc etc?
Recently I was presented with 2 cortisol results for a patient taken within the same 24hrs – her blood am result was above range, while her 24hr urine flagged under-functioning of her HPA axis generally. Both were accurate.
Had I have only have seen one, I would have formed the wrong opinion and only gleaned part of her overall HPA story. Every different type of cortisol capture – from different mediums: blood, saliva & urine – to different collection conditions: time of day, fasting V fed, specific stressor exposure etc answers a different question about our patient’s HPA axis. So to use any form of cortisol assessment well we need to start with 2 understandings: 1) it is a slippery little sucker indeed and no one test can answer all our questions – or as Miller & colleagues more eloquently put it, “Remember, all models are wrong; the practical question is, how wrong do they have to be to not to be useful” and 2) be clear about the most important question you have about your patient you are trying to answer and that will make your choice of test (& timing & & &) patent. But do you know enough about cortisol regulation to be clear about the ‘sweet spot’ of each test?
The Cortisol Awakening Response has understandably attracted the bulk of the research focus over the last decade and accordingly has risen in popularity in practice & while it remains a very valuable way to answer certain questions about patients, our understanding of its limitations continue to grow. For example there is a disconnect between CAR & diurnal cortisol secretion – so in essence your CAR can look woke but your ‘Slope’ may be broke! If you’re a fan of this method, make sure you catch up on the CAR-Expert Consensus Guidelines by Stalder et aland if you’d like to get clear about which test and when, when it comes to all the key options for Cortisol Capture..
then let’s dive in together with my latest Update in Under 30 instalment
I have! And just recently a stark contrast between the results from 2 different methods of cortisol capture in the same patient illustrated just how likely this is. How do we ‘capture’ something so ‘dynamic’ and interpret anything of substance from a ‘static’ assessment technique? But rather than throw up our hands and throw out the whole attempt to measure cortisol, we can improve the rigor, reliability and real-world meaningfulness of our patients’ results by refining our timing of tests, choosing the medium wisely & manipulating test conditions to answer specific questions about their HPA function. Great desktop reference included!
You can purchase Cortisol – Have You Been Caught Out?here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
The average woman & her dog (& likely every other member of her household, be they furred or otherwise), can tell you that sudden changes in sex hormones can undermine, derange, psychopathise, impact her mind and mood. Hey, for me most days reverse parking is my mild super power, the envy of all, but on day 26 of my menstrual cycle, I can struggle with a ‘nose-to-kerb’! But if we are quick to attribute this to the fluctuating sex hormones produced by our ovaries, alone, we’d be making a mistake. A portion of these peripheral steroids do cross the BBB and act in our brain, so changes to these levels during any kind of transition: follicular to luteal, pregnant to post-partum, menstruating to menopausal, early adulthood to andropause, will be ‘felt’ but the sex (hormones) we have on our brains at any given time, are far more abundant, potent and complex than this, thanks to the brain’s ability to make its own.
So in fact, the amount of sex hormones active in the brain represent an intersection between peripheral and central steroidogenesis. These Neurosteroids, made ‘on site’, are as much produced in response to our mood, our neurobiology, our psychological and environmental stress, to help us navigate these, as they are the creators of mood itself.
Yes, these particular sex hormones, due to their actions in our brain, belong to that growing list of CNS celebrities: the Non-Classical Neuromodulators. Which, for the otherwise neurotransmitter-centric & obsessed among us (that’s everyone), makes mental health and illness much more complex than ‘serotonin deficiency’ or ‘glutamate excess’ and a whole lot more real. We now need to consider other entities like: ‘suboptimal LDLs’, 5 alpha reductase over or under-expression & ‘xs inhibitory tone via progesterone’.
The ‘sex on the brain’ of any patient therefore is impacted by both their Endocrine (ovaries, testes, adrenals) and Synaptocrine (neural) contributions – and these demonstrate some shared dependence (for cholesterol & healthy mitochondria etc) and independence.
We all know the depressing stats in support of the ‘ovarian withdrawal hypothesis’ and the risk to women’s mental health with each reproductive transition, and also in andropause in men, but the time has come to now deepen our understanding and to recognise we can have an imbalance of ‘sex’ on the brain – regardless of the ‘balance’ we might see in the periphery and put our thinking caps on about the options we have to address steroidogenesis either side of the blood brain barrier.
When it comes to a modern take on how sex hormones impact both the structure & function of our CNS, we need to blend the ‘old’ with the ‘new’. The ‘old’ tells us, production of sex hormones is in the gonads and action at a distant target anywhere else in the body, including our brain. And the ‘new’ is in the form of the ‘Synaptocrine’ – where production of these sex steroids is actually within neural tissue itself and their immediate actions occur close-by, in the synpase and at the post-synaptic neuronal membrane. These two contributive pathways show some shared dependence but also independence from one another and the balance of both has now been recognised to be integral to the overall health of the nervous system.
Well, this is different, now I’m watching you! 😆 In early 2021 we released our very popular MasterCourse I: Comprehensive Diagnostics, as a ‘self-paced’ online offering for the many who missed out on attending live in 2020. Many have grabbed this opportunity with both hands (& a headset and some hardcore Do Not Disturb! signs) but we know that for some, doing the entire course on your own, >24hrs of video presentations, can be a tad onerous & overwhelming. We want to remove these barriers and empower & upskill as many practitioners in pathology interpretation as are keen, and as a means to achieve this, we’re offering the MasterCourse I Watch Party. So bring your bhujia and a beverage and let’s do this!!
Practitioners who sign up for this will be able to watch each session’s video replay live with other practitioners and have the opportunity to ask Rachel questions & participate in case discussions at the end. Another key detail is that we will run the sessions weekly, so that the full course is covered in just 6wks, from July 8th to August 12th.
MasterCourse I: Comprehensive Diagnostics LIVE WATCH PARTY 24 hours of live Zoom sessions + Bonus sessions! 8, 15, 22, 29 July & 5, 12 August on Thursday at 3.30pm to 7.30pm AEST.
Each Thursday, the video presentation for that week will be played so we can watch it together. Then Rachel will open up her webcam and mic, inviting you to do the same, to participate in a Q&A as well as set case discussions. When you register, you get immediate access to watch our preliminary/preparatory sessions, prior to 8 July: Accurate Pathology Interpretation Starts Here and the RAN Patient Pathology Manager Tutorial.
Below is an overview of the Watch Party schedule.
Week 1 – 8 July | SESSION 1: Acid Base Balance & Electrolytes
Week 2 – 15 July | SESSION 2: Renal Markers Week 3 – 22 July | SESSION 3: Liver Enzymes
Week 4 – 29 July | SESSION 4: Lipids & Glucose
Week 5 – 5 August | SESSION 5: Immune Markers
Week 6 – 12 August | SESSION 6: Haematology
“I thought my pathology skills were pretty up there until I did Rachel’s Diagnostic Masterclass course! Nothing like being knocked off my perch by a literal avalanche of new information, especially when it comes from the most commonly tests that we all use so often. The course has been a fantastic learning opportunity for me, and has since helped me pick out many intricacies in cases that have previously been missed.
The course structure was great, the level of detail was right up my alley, and the case studies were entertaining (in true RA fashion). Once again Rachel has increased my knowledge base, and help me provide way better service to my patients.” – Rohan Smith, Naturopath
Join Rachel on MasterCourse I: Comprehensive Diagnostics Watch Party and register here.
MasterCourse I is a pre-requisite to join MasterCourse II which will be delivered live in 2022.
Don’t know why on earth I would be discussing ‘Glassing’?I have a hunch. I was supposed to be doing a deep dive into Taurine & Glycine & their CNS effects for the latest Update in Under 30 and due to a technical glitch we produced a software generated transcript from my first attempt at the audio recording. We’ve never done this before and it seems to suggest, I have an accent and I’m a little mortified. I wasn’t under some delusion that my utterance was universal…my speech narrows my origins to certainly the ‘bottom of the globe’, but, ‘Strewth Sheila, how does any of yous guys understand me??!’
So we’re giving away 3 free copies of this recording to the first 3 individuals who can correctly translate the following from that transcript!:
“In fact, if we go back to their chemistry, you might recall that Glassing, well I refer to it as the naked amino acid. It refers to the fact that Glassing is the amino acid in its most stripped back form. It actually doesn’t have a side chain, which of course all other aminos do. So therefore it doesn’t have eyes and ears. It doesn’t have an Alan O’Day form.”
🥴😵😬
What?! Yes it took me a while to work it out…and I WAS THE PERSON IT WAS QUOTING!! So while I am currently using a medium released from my regional rhino-challenged speech, let me tell you why I am right into ‘Glassing’ as CNS support and as a sleep aid for many patients. Ever listen to the long list of enviable actions Melatonin has on the brain and think…’gee I wish we had something that wasn’t a hormone that could do that?’…hello Glassing, I mean Glycine. SCN sensitising, circadian entrainment, sleep architecture improvement without being a sedative or hypnotic…just to name a few. And guess what? The overlap between these two even extends to their behaviour within the upper GIT! Both of course being shown to be helpful in aiding the healing and recovery of function and integrity in the stomach. What else dose it do and how can we use it to its fullest benefit? The answers are in our latest instalment, A Fresh Look: Taurine & Glycine In The CNS.
And you’ll be pleased to know, the transcript experience has certainly got me paying more attention to my enunciation than ever before. So you’ll understand every word!
Maybe my parents really were just being kind when they said, ‘Everyone sent their kids to elocution lessons back then, it wasn’t because we thought you specifically needed help” 🤣😂
Both taurine & glycine have a claim-to-fame as amino acids that effectively calm an over-revving brain, via their net inhibitory actions within the CNS. They achieve this via different means and while in some circumstances, one, either or both will is the result of differences in the regulation of their BBB transfer, pharmacokinetics, as well as add-on benefits or detractors, unique to each. Learn how to use both of these powerful and affordable mood-modulators, to their fullest, and be more able to know ‘which one when’, by listening to this latest narrative review.
The latest Update in Under 30 has landed!!!
You can purchase Take A Fresh Look: Taurine & Glycine in the CNS here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
There’s enormous potency in nutritional medicine for mental health but it ain’t in the form of a ‘dash of precursor here and a sprinkle of co-factor there’, like some may have you believe. Many nutritional prescriptions can look good on paper but that’s the extent of it, take the suggested use of glutamine for GABA production, for example. Sure it can be said to be a precursor (so is glucose!) – so will higher intake of this equate to higher production of this neurotransmitter? Ah, no. The reasons relate to distribution and hierarchy of use for this amino acid, as well as determinants of glutamatergic neuron activity.
Why would we limit our prescriptions to precursors, anyway, when we have 2 amino acids at our disposal, whose oral supplementation is known to translate to higher CNS levels and their actions and efficacy as major inhibitors of neuronal firing (akin to GABA), involves no modification nor maybes?!
Hello, Taurine & Glycine, where have you been all this time?
While, many of us may have been using taurine in combination formulas for mood, chances are you’re not entirely clear why sometimes those work and sometimes they don’t. The answer may be in the regulation of CNS taurine transfer & balance- sometimes the people who need it most, have the least capacity for its uptake across the BBB. This is well-established in neurobiology, but news to many nutritional and integrative health professionals, who have been using it in patients where Glycine, in fact, makes more sense. So while taurine has myriad impressive strings to its bow in relation to mood-modulation and powerful protection of brain structure & function, Glycine, has an extensive network of receptors throughout the brain and spinal chord, enabling it to exert inhibitory effects, second only to GABA itself. And, most importantly, BBB transfer of this amino is not subject to the same impediments that we see with taurine. These are two of my most frequent and favourite mood-modulators, affordable and accessible when used as single ingredients, for patients, with anxiety, addiction & sleep disorders etc but understanding how they work (and when they won’t) is essential in choosing which one to use, when.
For example, do you know the Tmax for either of these oral supplements? How long it takes, to create a spike in patients’ plasma, better still their CSF, and therefore speed of onset of action? What about their elimination half-lives to guide your understanding their duration of action and therefore the timing of follow-up doses?
When we’re trying to realise the full potency of our medicines – these are important details to know that convert our ‘prescription potential’ into something powerful. Just like die-hard herbalists will tell you, its an art and a science and this is true in nutritional medicine as well. Don’t skimp on the science!🤓
Both taurine & glycine have a claim-to-fame as amino acids that effectively calm an over-revving brain, via their net inhibitory actions within the CNS. They achieve this via different means and while in some circumstances, one, either or both will is the result of differences in the regulation of their BBB transfer, pharmacokinetics, as well as add-on benefits or detractors, unique to each. Learn how to use both of these powerful and affordable mood-modulators, to their fullest, and be more able to know ‘which one when’, by listening to this latest narrative review.
The latest Update in Under 30 has landed!!!
You can purchase Take A Fresh Look: Taurine & Glycine in the CNS here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
 Wow, menopause is really having a moment, isn’t it? Or is that just me (and my mates who are all somewhere on that perimenopausal path)?! But seriously, medical perception of this reproductive transition is undergoing a revolution right now—widening the lens to take in more diverse potential presentations and lengthening the period of impact recognised both ‘before, during, and after’ that last, last…no hang on…last period. But I fear we are at a crucial crossroads. Anything could be related to (peri)menopause, but not everything is or should be.
Wow, menopause is really having a moment, isn’t it? Or is that just me (and my mates who are all somewhere on that perimenopausal path)?! But seriously, medical perception of this reproductive transition is undergoing a revolution right now—widening the lens to take in more diverse potential presentations and lengthening the period of impact recognised both ‘before, during, and after’ that last, last…no hang on…last period. But I fear we are at a crucial crossroads. Anything could be related to (peri)menopause, but not everything is or should be.

 You know the saying, ‘If I had a dollar…’, well there’s so many ways I could finish that sentence, especially in relation to the most common questions I’m asked by praccies on a weekly basis and ‘Can my patient on antidepressant ‘X’ take SAMe?’, would be in the top 10! While many of you might be mouths agape reading this, I bet the cause of that comical expression is not the same for everyone. Yes, like you, they’ve read the mandatory label warning: ‘individuals who are using prescription antidepressants or suffer from bipolar depression should not use this product unless under the supervision of a healthcare practitioner’ – but let me ask you, how do you interpret that? Turns out there are several interpretations and the most common is the most incorrect.
You know the saying, ‘If I had a dollar…’, well there’s so many ways I could finish that sentence, especially in relation to the most common questions I’m asked by praccies on a weekly basis and ‘Can my patient on antidepressant ‘X’ take SAMe?’, would be in the top 10! While many of you might be mouths agape reading this, I bet the cause of that comical expression is not the same for everyone. Yes, like you, they’ve read the mandatory label warning: ‘individuals who are using prescription antidepressants or suffer from bipolar depression should not use this product unless under the supervision of a healthcare practitioner’ – but let me ask you, how do you interpret that? Turns out there are several interpretations and the most common is the most incorrect.