Any steps towards inclusivity in societal & cultural terms are cause for celebration but in medicine, that can come in the form of a ‘diagnosis of inclusion’, the opposite, of course, of a ‘diagnosis of exclusion’ and potentially as slippery and loose as it sounds. That’s the somewhat precarious position we find ourselves presently in with perimenopause and menopause. With greater recognition of just how long health effects can kick in before there are any cycle changes [2-12 years for those of you playing along at home] and the widening lens now taking in the diversity of such health effects, women’s health has had a win. But, I would argue, this is not without a double edge. After all, aren’t we, as a result, more at risk, as women, of having everything attributed to “just ‘the change’, love”, and, in turn, going to be offered sex hormones more often as the solution?
Let’s play a word association game of minerals & their major roles
I say, ‘Potassium’. Maybe you say, ‘Sodium Potassium Pump’ I say, ‘Magnesium’. You say, ‘Muscles?’ I say, ‘Calcium’. You say, “Bones’….
But I say, Second Messenger. And arguably the most pervasive & potent one, at that. Remind you about second messengers? Well, sure. They are the ones who get sh*t done. Not like a boss (i.e. hormone or neurotransmitter) who shout directives from above but never step foot inside the dirty guts of the engine room itself. It’s the second messengers who run these messages from the outside of the cell to the inside and the engine room, to ensure that the directive is actually actioned! Amazing huh! And free calcium in the blood is, as I said, really a superhero even among the second messengers – with its regular responsibilities including: Insulin, TSH, Adrenaline, Oxytocin, Serotonin receptor activation etc etc
Does, it have a dark side? Well, sure. Don’t most superheroes?
If the available Calcium in blood and the extracellular environment is too high then basically bad sh*t gets done. Including vasoconstriction, clotting, deposition of calcium in the wrong place like arteries and joints and etc etc. That’s why the amount of Calcium in our blood is the MOST tightly regulated of all electrolytes and, in turn, has the NARROWEST of reference ranges. But will a Serum Calcium level always tell you when there is a problem with Calcium regulation? No. You’d need to have measured the major regulator itself, Parathyroid Hormone (PTH). Wait, am I seriously trying to tell you, that Serum Calcium alone can look completely normal in spite of really damaging Calcium dysregulation underway – leading to accelerated BMD loss, increased cardiovascular and renal risks etc.? I most certainly am.
So do you know which of your patients’ really need PTH assessment and why 1 dominant group amongst those, is any woman leading up to and following menopause?
No? Well you better pull up a pew and have a listen and a watch then! Yes this latest Update in Under 30 episode even comes with a little video tutorial!🤓🤯
Parathyroid hormone is a career criminal. In addition to buoying dropping blood calcium levels via legitimate means, it illegitimately achieves this by stealing it from our bones. But you wouldn’t know it – because like all career criminals this occurs completely under the radar. Elevated PTH, however, constitutes the most modifiable risk factor for bone mineral density loss & fracture risk and offers the biggest BMD gains secondary to its normalisation. In addition to this, even within range but ‘high-normal’ PTH correlates with a range of other cardiovascular and urinary presentations & if combined with elevated serum calcium can become a multi-systemic presentation (GIT, Mental health etc) frequently mistaken for other aetiologies. So how can we be alert to this ‘bone thief’? Which of our patients will benefit the most from PTH measurement and monitoring? This recording, resource & video tutorial on how to use a Ca PTH Nomogram answers all!
You can purchase Unmasking Hyperparathyroidism – Menopause & Morehere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account. You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
Ever feel like the universe has been preparing you just for this moment? Me neither really…but in this one weird way – yes!
So hear me out.
Thyroid disease as a result of a viral infection was first described in 1902 by Dr Fritz De Quervain and of course he and his ego called it De Quervain’s subacute thyroiditis. For some historical context, this predates the recognised role of iodine deficiency in thyroid disease! Skip ahead almost a century to deep in the 1990s and mini-me was sitting in a uni lecture room [front row & wearing fluro of course🤣] and over hundreds of hours (no scrap that zillions*^# of hours) of lecture content I was exposed to, the description of De Quervain’s Subacute Thyroiditis stood out and stayed stuck to me. I’ve brought it out for a twirl from time to time in the interim with some of my patients & in particular in correspondence with their docs.Skip ahead to the 2020s when we had this thing called. ‘a global pandemic’, and now everyone wants to talk viruses and their broader health implications & as a result, good ol’ Fritz, me and our buddy, De Quervain’s subacute thyroiditis, are all having a moment.
But just to recap – this is (clearly) not new.
What is new is the way this ‘virus of the moment’ has brought this Thyroid V Virus battle to the forefront. We are living an important chapter in history where all the textbook entries on De Quervain’s Subacute Thyroiditis are madly being rewritten to reflect the veracity of this viral attack on the gland and the wide-scale & varied damage that ensues over the months and years that follow. And so many of our patients are the walking embodiment of it – whether that be in the form of low or high thyroid hormones, nefarious changes to gland anatomy only evidenced on US. So what do we need to know? in short, that pathogens as goitrogens have never been more of an issue than right now for ourselves and our patients. And that compared with just our usual desire for comprehensive investigation of the HPT, taking a complete look ‘under the hood’, not only by way of a full TFT and Ab titres but also, wherever there is an additional suspicion – by way of a thyroid US – has become non-negotiable. But regardless of what you find there, once you look, do you know what to do next?
Biopsies and autopsies of diseased thyroid glands alike reveal the prevalence of many common viruses within, setting the scene perfectly for the Thyroid V Virus battle. So, what happens when a virus takes a specific liking to this gland? While there are several different possibilities, one brought to the forefront in recent years is viral thyroiditis wherein stage 1 is ‘spill’, stage 2 constitutes a gland that is now ’empty’ and while stage 3 is reported to be ‘recovery’, this is increasingly scarce – replaced with chronic or recurrent thyroiditis, relapses of previously remitted GD and a doubling of new AITD diagnoses – not to mention the wide variety of unfavourable anatomical changes being found on ultrasound. Comes with a great desktop reference with prescription examples.
You can purchase ThyVIRoidhere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account. You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
The debasing of BMI as a stand-alone assessment of weight is long overdue given its significant limitations and lack of meaningfulness with respect to overall health. This coincides with a bigger societal and cultural shift towards inclusivity which involves redressing bias against people with diverse body sizes and compositions.
And how do we, as integrative health professionals, continue to uphold our principles of prevention and treating the cause when excess adiposity may be a very real contributor? While ensuring we ‘see’ and treat each individual in front of us, not our assumptions about adiposity, not our body size bias nor blind spots?
One part of the answer: read and be led by their lab results – because pathology is nothing if not personalised.(more…)
The builder responsible for my reno arrived one day with a frown. When I asked him what was wrong – he said he’d just had his second high PSA result and now the doctor wants him to see a specialist. It was apparent that he felt this was a real cause for concern. Talk about raising a red flag to a bull 🚩🐂 Yes, of course you know what followed. I insisted on reviewing the results myself only to find the reference range provided on his report was not specific to his age – and if we adjusted up for this (as the science supports) his result is just 0.5 ng/mL above the expected value!
Now, remember he is a builder so, ‘0.5’ in his mind might well be on par with 5mm which apparently is a big deal…or so he keeps telling me every time I try asking for some weird unconventional thing for my roof, windows, walls, whatever!! So I still had to provide a little bit more detail for him to get perspective and to understand the true meaning (and lack of scary meaning) of his results.
This however is just a micro-illustration of a big problem in pathology – we all risk a lack of perspective but if we can get it back, aids us to see that seemingly ‘normal’ results are sometimes a concern, and so-called ‘concerning’ ones, non-significant. The incredible patient insights that can be gained from being able to measure & monitor actual quantities of things in our patients; nutrients to novel disease markers, precursors to end-products, all comes down to understanding how their values compare with…with what? With someone of a different sex and age? With ‘all adults 18-108!’? With any other pre-menopausal woman regardless of reproductive or cycle stage? With ‘the average’ adult given that this current definition is overweight & unwell? Who are we comparing ourselves and our patients to?
When I undertook my undergraduate training many moons ago – there was no education in blood test interpretation. But as soon as I got out into practice I found my patients had all these bits of paper filled with magic numbers that I felt certain might offer me insights and a deeper understanding of their whole health – and how to best help them.
I desperately wanted to decipher this foreign language and made it my mission to do so. I was lucky enough to meet and be paired with a kindred spirit, Dr Tini Gruner, who happened to be my supervisor when I returned to undertake my honours thesis. Together we pooled our knowledge, sought out & shared with each other yet more and found that, together with comprehensive case taking, it provided excellent scaffolding to our work-up of patient cases. Better than that, it created this baseline for patients, identified clear treatment objectives and we could measure the success of our interventions based on how their results did (or didn’t) respond to our interventions. It was (and still is) a totally thrilling way to practice.
We talk about there being both an art & science to medicine generally and certainly an integrative approach. Without the benefit of pathology interpretation, I felt too at sea at times, without quite enough of the science to check the accuracy of the ‘art’ and my speculation.
Being able to understand what each individual result represents and reflects, to know how to form meaningful comparisons – with external reference ranges that speak to healthy individuals of the same sex & life stage, derived from rigorous research – and also form a comparison with the patient themselves, to pick up on the most subtle and significant early alerts to an emerging pathophysiological or healing process – is the skill, I believe, we all need in health to complete the toolkit. That’s why I made it my mission to learn the language of labs, from a conventional & integrative interpretative perspective, and then to share this learning with everyone wanting and willing to take this baton from me (& Tini) and run with it 🏃♀️🏃
MasterCourse I: Comprehensive Diagnostics. Click here to read more and here to purchase it.
*Please note that this is the place to start for everyone wanting to add preventive diagnostics to their tool kit. It is also the pre-requisite for MasterCourse II, so make sure you have completed this before continuing with MasterCourse II: Thyroid and Adrenal Diagnostics.
MasterCourse II: Thyroid & Adrenal Diagnostics. Clickhereto read more and here to purchase it and sign up for the Free Watch Party commencing tomorrow, 3rd August 2023 with is included with each purchase of the MasterCourse II.
Rachel: And sometimes emails from practitioners provide me with both the question and their own answer to their question even!
Cameron Barker’s (Ex-student long-term learner & mentee)email arrives titled:Unexpected Source of Iodine in Placenta Caps?!
A 32 yo female with a 12-week-old daughter came to me as she was not feeling well, in particular, she reports fatigue, racing heartbeat, anxiety and loss of appetite. Previously, 2 years ago, I had helped her with her Hashimoto’s. I did not hear from her for a year or so and she fell pregnant and was recommended to take a well-known iodine-containing pregnancy multi.
Just as optimal integration of lab results into our patient work-ups makes ‘the invisible visible’ we thought we might make visible some of the everyday Q & A that we engage in with wonderful practitioners who are fast becoming Diagnostic Divas & Divos.
Praccie email arrives with subject header ‘Graves Help’ (or is that ‘Graves…HELP!’🤔)
Practitioner: I have a Grave’s patient who required Propylthiouracil (PTU) for a few months from late 2022 until Jan 2023 which obviously took her thyroid in the opposite direction (see labs). Following a miscarriage last year, she has conceived and is around 6/40 and her current TSH result has come in at 3.3mIU/L, her TPO Abs > 1000 and she also has low-level Tg Abs (TRAbs not measured this time) and this is what she just said to me:
“I just had my specialist session this morning – and she has put me on thyroxine (50mcg) as my thyroid is quite low. I also asked her about the prenatal vitamin and she said it was safe for me to be on iodine at this time, as the Graves isn’t present and baby needs it for the development of its own thyroid.”
Oh gawd! Preg? Iodine? Graves? Antibodies? Antenatal or postnatal aggravation?!
Is there an UU30 I can listen to to help me understand this?… sorry for the panicked email…
Gone are the days, thankfully, when we could all easily identify any individual taking an antipsychotic 1) because they were the marginalised ‘mad’ and 2) stigma and shame were rife. With the seismic shift that has occurred both in psychiatry & society we now know so many of the people we live or work with just might be taking ‘something’ & under any number of diagnostic labels. And increasingly the ‘anti-psychotics’ are not reserved for the psychotic nor the ‘mood stabilisers’ for the manic. Which can complicate things – especially when it comes to their thyroid.
You see it’s a mistake to think that only Lithium spells trouble for thyroid function
The latest piece of evidence from a study of over 25K BPAD patients in the US tells us this common misunderstanding makes us prone to not recognise all the other patients in whom their psych meds are disrupting and in fact driving thyroid (dys)function. Though Lithium carbonate remains the most noxious goitrogen due to its multiple disruptive mechanisms – the rest of a large group of Psych meds (yes even antidepressants!) are impacting to the point of effecting the thyroid function test results you are likely to see in patients taking these. And this is something we need to be alert to – these medications are essential, non-negotiable in most scenarios, but a secondary hypothyroidism is not their intended goal and can make matters worse.
Cue our growing understand of psychoneuroendocrinology, of course. Your HPT is influenced by your mood & vice versa
I told you I’ve rekindled my love and passion for thyroid pathology and this is one of the many elements I got to include in our latest updated training * Advanced Thyroid Assessment* and the upcoming MasterCourse. But I just had to hit record on this one aspect immediately – because if we don’t recognise the cause we are likely to be throwing all the wrong things at the thyroid – to no avail. This kind of subclinical or overt hypothyroidism is not due to nutrition per se, or due to some other kind of HPT re-setting influence like inflammation…it’s the meds & that necessitates different solutions & a much bigger conversation…so join me…
Many of us recognise the bidirectionality between thyroid function and psychiatry wherein ‘stress’ and mental illness can produce a predictable pattern and shift in TFTs and vice versa but regarding the question of psych meds as potential goitrogens, many of us are mistaken in thinking this issue begins and ends with the use of Lithium carbonate. As it turns out, an increasing number of these pharmaceuticals are recognised to disrupt thyroid health & activity via a variety of mechanisms both centrally and peripherally & as a result many patients may get stuck in a vicious loop of worsening thyroid function and mental wellbeing. – until someone calls it – someone like us.
Have you been told somewhere by someone that the ‘perfect’ TSH is 1.5 mIU/L? This is a wonderful, terrible & wonderfully terrible example of ‘magical numbers medicine’. As a push-back against the published reference ranges we’re given, that are so wide you could drive a truck through them, there has been an over-correction by some, leading to the myth of ‘magic numbers’. We can narrow the reference range substantially for many parameters with good rationale, make no mistake about that but once we start setting ‘aspirational goals’ that are explicitly rigid…well we’ve done 2 things 1) forgotten about the patient to whom this result belongs and 2) disregarded viewing each result as part of a ‘pattern’, that we must piece together and make sense of.
Back to TSH then… if my obese patient had a value of 1.5 mIU/L this in fact would be woefully inadequate – so too a child at any weight.
And we expect a higher value as well in our elderly clients too and this level there may be, in fact, increased mortality.
But the same result would be excessively & worringly high in my patient who’s undergone thyroidectomy.
Realising the full value of any test result in terms of what it reveals about the person sitting in front of you, requires these more thinking and more thoughtfulness. Unfortunately, a list of ‘magic numbers’ will often lead you astray. And building your scientific knowledge about labs will not only help you avoid the pitfalls of pathology but will strengthen your pathophysiology prowess in surprising ways, saving your patients a packet in terms of additional extraneous testing and help you truly personalise your prescriptions…because the ‘invisible (biochemical individuality, oxidative stress, genetic probabilities, subclinical states, imbalanced or burdened processes etc) just became visible’. I started requesting lab results early in my career and years later was lucky enough to be taken under the wing of Dr. Tini Gruner. I found some of our shared notes, from 10 years ago, scribbled all over patient results recently and I was struck by just how lucky I was to have her encouragement to really pursue my interest and how she was a guiding force about learning to recognise pathology patterns over single parameters. A decade on I can concede, much of my clinical and educative success has come off the back of this foundational skill-set and I know, this is true for so many I’ve taught too.
“The guidance I’ve received over the years from Rachel in relation to pathology interpretation has been one of the most valuable (and fascinating) investments I’ve made as a clinician. Her teachings have filled gaps in my knowledge base I never knew needed filling and have significantly enhanced my understanding of the inner workings of the body! Rachel has an incredible ability to make the numbers that patient’s so often present us with, both understandable and clinically meaningful. The knowledge I’ve gained by investing in this skillset has paid off in dividends and I’m certain will continue to do so into the future.”
Stacey Curcio – Cultivating Wellness
I hope you’ll join me for the most exciting up-skilling opportunity in learning labs yet. Oh…and all this talk about thyroid testing..this next MasterCourse series is focused on revolutionising your understanding of thyroid, adrenal, HPT & HPA markers based on the very latest research & findings & marry these together with everything you learned in MasterCourse I (ELFTs, FBE, Lipids & Glucose) to understand the ‘whole story’.
…an absolute treasure trove of free integrative health information about your patient!
DEEP DIVE INTO REAL CASE STUDIES TO DEMONSTRATE EACH PATHOLOGY PATTERN IN ACTION. ]\
There are limited places. To sign up for Rachel’s LIVE Series – MasterCourse II: Thyroid & Adrenal Diagnostics and for more information click here.
I’ve spent the best part of about 4 months recording my *NEW* Advanced Thyroid Assessment training. I told my team this would be easy and quick, given it was to be based on a great little 2-part, 2hr updated presentation I delivered just last year for ACNEM!! Sixteen weeks (like seriously…most of it) numerous rewrites and retakes later, our final product is 4 parts that goes for over 12hrs in total & has a bonus Adrenal recording! And yeah my team are impressed but unimpressed too if you know what I mean?!🙄🤪
Every time another, ‘Oh wow!’, or ‘No way!’, escaped my lips, it was a source of personal celebration, as another deeper layer of learning revealed itself.
But to the wonderful, somewhat weary and definitely wary Sally, who does all my powerpoints, it was met with, ‘Oh boy!’, because it meant many multiple new slides to build full of visual metaphors, animation acrobatics, if not an entire new Part!*#@^
Her sage advice along the infinite research road I’ve been travelling was : ‘Stop. You’re going to have to stop.’
So I didbut now I am this meme. Everything I see currently through the lens of thyroid health, I talk in tongues TFTs and my brain is one giant neural network of integrative endocrinological circuits! I have fallen in love with this topic, this neuroendocrine axis and its ‘first responder’ role all over again! Hence our little thyroid character below – all ‘antennaed’ up – is one of the many tools we’ve developed for this training, to teach us that ‘bad thyroids’ per se are extremely rare – but bad scenarios are common (too much or too little of any macronutrient, key micronutrients, a change in the internal or external environment etc etc) and this little fellow and his board of directors (no – not the hypothalamus or pituitary!) – well it’s their job to ‘read the room’, right?!
In the absence of this key understanding we risk: A lot of lazy labelling in thyroid health – ‘You have a bad thyroid – that’s why you…[can’t lose weight, feel tired, have SIBO etc]’ Misdirected treatment & especially a tendency to overload the butterfly with ‘thyroid’ nutrients – which can do more harm than good
I’ve said many times, ‘perfect number pathology is a myth’ but it runs rife in practitioners’ beliefs about TFT results with complete disregard of the person those labs belong too! Did you know, for example, that your TFTs should all be higher if your BMI is? That your T4:T3 ratio should never be 3:1 if you are on replacement, have hot nodules, are pregnant or are acutely unwell etc etc etc? How about how low your Selenium or Iron levels need to be before this factor will influence the actual levels of thyroid hormones measurable – & what the impact of these deficiencies are well before then that is far more sinister and serious? Yep…you see here I am, pouring just some of the tiny take-homes of Advanced Thyroid Assessment ALL over you!
Watch this space my new Thyroid training is just around the corner!
An increasing number of our patients have thyroid concerns but unbeknown to many of us the most likely explanation of all is thyroid nodules, whose incidence is on the rise globally. The development of nodules has always been primarily viewed as a nutritional disease. Traditionally attributed to chronic iodine deficiency but recently novel nutritional causes have emerged. Benign nodules come in 2 flavours: hot and cold and while patients can present with a mixture, it is the presence or absence of a hot nodule that radically changes what complementary medicines you can and can’t use and what an effective treatment plan looks like. The pointers, as is often the case, are there for us in the patient’s presentation and pathology, so knowing the difference is no longer a guessing game. This UU30 comes with a great visual clinical resource and includes key papers on the nutritional management of nodules.
Over years of delivering independent education in integrative health I have spoken to some diverse audiences. This has included health professionals from very different backgrounds: from hospital-based psychiatrists & mental health nurses, to whom I presented on site in hospitals both in Australia & NZ, to a national sparkle-arkle speaking tour, in front of large groups of aesthetic practitioners. They’re the doctors & nurses for whom botox and fillers are their tools of trade, and yes I got to see actual demonstrations of their work performed live!!!😶 More recently, I’ve had several opportunities to deliver evidence-based independent education on nutrition to pharmacists en masse – which I always enjoy because they ask some of the best questions!
Underpinning each decision to accept an invitation from a 3rd party, be that a company an organisation or an institution, to speak, is: 1.The realisation of an opportunity for nutritional medicine to reach more people, a wider audience, & ultimately expand the circle of influence amongst health professionals, who interact with & advise the public at all different levels 2. An agreement and/or contract that ensures my independence, the correct use of my materials, image, brand and IP & removes any expectation to promote their products/services etc
And my ‘door’ is open to any invitation which meets these 2 criteria. So you might have seen my name, previously associated with some brands or organisations, in the last few years disappear off their speaker announcements, or no longer connected, and in turn you might see my name pop up in new places! Like….Metagenics Congress on Autoimmune Disease!! After many invitations from this company, that I wasn’t able to previously accept, I am pleased to be speaking at this face to face event on the Gold Coast in August. What a novelty, hey? Face to face?! My talk is about the 4 Mistakes not to Make in Hashimoto’s and as always, I’ve completed a full mini-literature review in order to speak to the very latest on diagnostics and nutritional management, in this condition. Yes, to quote a Costanza, “We’re back baby, we’re back!” And to see my full current smorgasbord of speaking commitments & all the people I am ‘spreading the (nutritional) word’ to – just click here.
This previous training will take your understanding of the interplay between food, nutrition, environment and the thyroid several steps further. With more supportive research and a greater focus on the mechanisms behind the relationships between these macro- & micro nutrient & environmental factors, this presentation is for the true thyroid die-hard.
Ever been guilty of having a ‘man’s look’ for something? I have. Particularly when it comes to the online omniverse! I can be a bit flaky at finding things right there on the page…allegedly! So for those of you who have a similar experience with my website & endless educational offerings, I FEEL YOU! We do have a tonne of training options and a whole lot of (love 😉 couldn’t resist the Led Zepplin reference)… lab & diagnostics resources! This has come up in conversation a lot recently, following the release of our RAN Student Pathology Hub, for example: “I’ve done your MasterCourse in Diagnostics, does this cover something different?” or “LOVED😍 this new hub its *$@# incredible resources & extra training vids but I also wished it included your take on… [insert your pick from infinite list: thyroid, cortisol, zinc etc etc etc]
So here’s a Dummies Guide:
How to Find the Help you Need in Diagnostics
If you are just starting out on your path to pathology & true lab literacy & want an accelerated way to ensure you are starting this journey on solid ground and you have the most called-upon skills you’ll need in clinic today, then the RAN Student Pathology Hub is your perfect match. NOTE: this is not limited to actual students but anyone who considers themselves, like us, a life-long learner! This 12 part module includes some small core components of our MasterCourse, a few expanded episodes from our Update in Under 30, plus unique short training videos, covering tests and topics including: Iron studies, B12 assessment methods, Coeliac screening & much more
If you’re seeking the immersive experience – you want to maximise your competence and confidence & forge your path as a true Diagnostic Diva or Divo then look no further than our ‘mothership’, the MasterCourse in Comprehensive Diagnostics which now has a part payment option. This really is the most seminal training we offer, taking the time to dig deep into the science behind all the ‘signposts’ our patients’ results are pointing to. A big commitment for a big reward. It comprehensively covers all the routine labs you will see everyday: LFTs, Renal markers, Glucose and Lipids, FBE & WCCs & is loaded up with case illustrations for each key pathology pattern – that many practitioners say was an absolute highlight
Just have a specific question or need for upskilling in Cortisol assessment? Zinc or Zonulin? It’s probably in our vast Update in Under 30 library! Yes, with more than 100 episodes in there and my penchant for pathology…you’ll find something, if not in the UU30 episodes, then somewhere else on my website. You know how in pdfs ‘Control + F’ is a god! Ok on my site it is this fella 🔎 You can use this to search my whole site to find free information on the topic (blogs) or manifest the same magnifier🔎 magic once you have clicked ‘Catalogue’ on the top right of the tool bar on any page, to locate any specific educational offerings. Remember with the UU30, you can purchase single episodes or subscribe and get access to the whole shebang.
And for those of you primed praccies, patiently waiting for our MasterCourse II to land? Well about that…did we mention we got hit with a flood? Twice? And then got covid? Two of us? And have our beloved Nina about to depart to become a mumma!!! Yeah, so our plans to have this up and ready for May changed to Mayhem, real fast 🙄🤪 We will definitely keep you posted on any developments and new timeframes but for now we can only apologise for the delay and will do our best to get back on track with this, at the earliest opportunity. In the meantime maybe a little review of some of MasterCourse I is in order? I refer back and re-listen all the time, myself!!😂
Being a practitioner who is able to read labs will set you apart in practice. For your patients this flows from your ability to form a more sophisticated understanding of what’s happening for them, enabling you to better individualise treatment and deliver superior outcomes. Amongst other health professionals, it will attract positive regard and an increased willingness and enthusiasm for sharing the care of patients with you. Learning to be lab literate could take a lifetime…or you can enter the expressway from the very outset! We have curated the content to reflect the most essential elements, to help you hit the ground running in the shortest period of time. Spread across 12 modules which can be consumed as monthly instalments or, as an all-in-one experience for those wishing to waste no time. The teaching points, tips and tools make the complex simple, engaging, even fun!
Developed, designed and delivered with students of any health discipline in mind.
I’m ready to zip my lips 🤐 and ride off into the sunset of silly season. But first I wanted to tell you about the BIG PLANS we have ON THE BOIL! Noticed a bit of a thyroid theme of late? Last month I presented training in thyroid assessment for the 4th time for ACNEM but not a slide, possibly barely a dot-point remained from the original one I wrote back in 2009. That’s how much my ideas & understanding have changed.
Some of the assay techniques & technologies are new, there’s a river of research & a mountain of meta-analyses published in the time between & I have had the privilege of yet more clinical encounters in this space, to really nut out how all this translates into the real world.
There’s a lot I need to catch you up on. And as I start creating our new MasterCourse II in Comprehensive Diagnostics…which will include 🥁…you guessed it…the humongously hardworking HPT, I’m just about bursting at the seams! And will those four little friends of every good practitioner, that sit superficially atop the ‘butterfly’, make it into our MCII?? I hope so because a) they should be our besties – being the director of Ca Mg D & P regulation and b) research tells us that where we find, ‘thyroid’ dx we should have another good hard look for ‘parathyroid’ dx and vide versa and c) over the last few years it has become increasingly apparent to me that this is one incredibly common source of ‘medical mysteries’ in our patients – remember the ‘Bones, Stones, Abdominal Groans & Psychic Moans’ catch-cry? Yep, that’s the patient who typically finds their way to us, with pervasive but hard to pinpoint gut issues (often misdiagnosed as SIBO, FGD, IBS -D or C), some significant stress perhaps even depression and insomnia and, if someone bothered to look, premature bone demineralisation. What other pathology panels and parameters will we be able to squeeze into our MasterCourse II?
Our current plans are to deliver the MCII live from May but just a reminder, because this next instalment assumes you have the exquisite foundational knowledge we laid down in the MCI – this is a pre-requisite for attending the MCII. So if you’ve been putting off your pathology apprenticeship now you have a hard deadline to work to!
And finally the last, last words. On topic because they came from someone who specialises in thyroid, did the original thyroid training with me, way back when, and last month was my fellow presenter & panellist on all things thyroid for ACNEM:
I’m sure I’m the 1 billionth person to reflect this back to you but I’ll do it anyway because I think we all need reminders sometimes – you have a truly special gift in critical thinking, discernment, and most importantly passing on complex knowledge in a very digestible way without making anyone feel silly for asking questions or not getting something the first (or fifth time…no, just me?). The endless analogies are a teaching tool you’ve well and truly nailed and boy am I grateful because it speaks to my way of learning very well.
So, a big thank you! Endless gratitude for your brain, passion and generosity with your time/knowledge/resources. Natalie Douglas
Here’s to another great year of learning, teaching, sharing & mentoring in 2022 – 1 billion and counting I hope 🌟🌈😂
We love hearing from our fellow fearless friends on the frontline – working with lab results & pathology providers – everyday. We recently received an SOS! from the Francesca Naish over yet another iodine assessment issue that you may need to also be alert to:
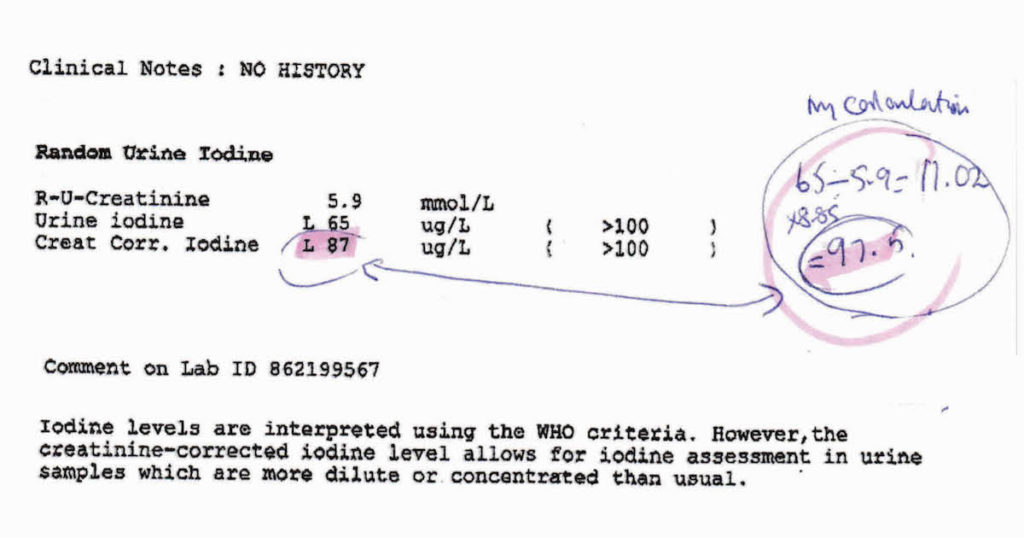
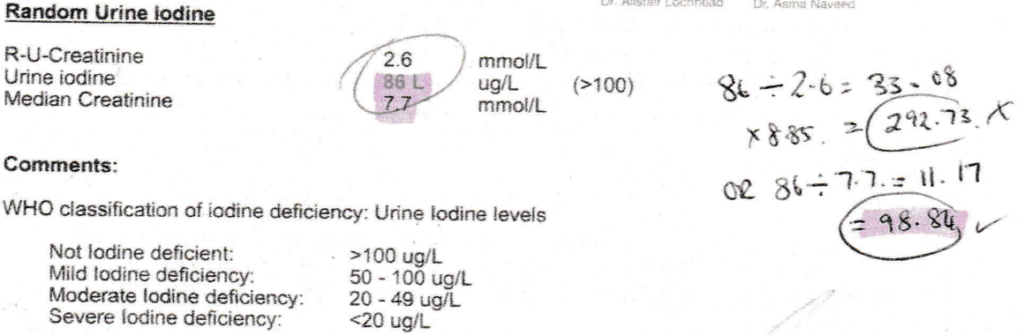
“Ever since you first drew our attention to the need to correct urinary iodine results, I have used your formula for all my patients’ results. Thank you for this. As most GPs don’t seem to be aware of the need to do this, I find it essential to warn my patients to wait for my interpretation before acting on their doctor’s advice! For a while now, Laverty have started giving the corrected result, which complies with the calculation you recommended. However, very recently Douglass Hanly Moir have started to give a corrected result on their result sheets, but it does not tally with the calculation I have been using (the one you recommended) and generally gives a lower figure.”
Well, as always, cluey people ask cluey questions…and this did take some back & forth with DHM to solve. Increasingly, all the major pathology companies are coming around to the essentiality of urinary iodine correction, something I’ve been banging the drum 🥁 about now for….yikes…7 years..no wonder I’m going grey! This is a mathematical formula applied to any raw score for urinary iodine to account for the dilution/concentration of the given sample, because, as we all know, hydration status varies widely between individuals and even within an individual at different times – and this is something that can wildly lead you astray in your thoughts about their iodine status, if not accounted for. Some companies are now employing the formula we use: Iodine (mcg) ÷ Creatinine (mmol) X 8.85 = Corrected Iodine in mcg/gCr which is wonderful to see. But DHM have taken a different path, strangely enough, using this formula BUT rather than using the patient’s own reported urinary creatinine they instead use a ‘median creatinine’
Which…I am going to say it… MAKES NO SENSE!^%@* aka we WILL correct this iodine for hydration status – but we’ll correct it for someone else’s no yours! – Ms/Mr average…ok? Ahhhh no. Just look at the difference this makes in a patient with very dilute urine, in example number 2 above!!
So Francesca & all of you on the frontline, can be assured, if you’re using the formula above – it is correct – keep up the great work and know that it is often better to do something yourself than blindly trust a 3rd party when it comes to pathology…unless that 3rd party is our RAN Patient Pathology Manager template which calculates this perfectly of course!
Increasingly our patients are coming armed with lab results and this cumulative data helps us to clearly see their ‘norms’ (as opposed to textbook ones) and therefore be alert to any changes. However, results from different labs at different times, and even the same lab, are unlikely to be presented side by side for easy comparison. They certainly don’t come with all the important information about what was happening for that patient at each time point – important details pertaining to the blood collection itself (fasting, inflamed etc) which can profoundly alter results or the broader context: menstruating, breastfeeding, losing weight, on meds and supplements.
The Patient Pathology Manager retains all the results for you, including the critical contextual elements, helping you to keep more accurate records to make the most correct interpretation. It also assists you to monitor changes related to various interventions.
Previously, the RAN Patient Pathology Manager has only ever been available to clinicians who participate in Group Mentoring but due to frequent requests for access, we thought it was time to share this great tool for those wanting a foot up with some better systems in their practice.
This provides you with a template that can be used an infinite number of times plus a short training tutorial.
An ideal T4 is 15
An ‘anti-aging’ DHEAs must be >7
A ferritin of 100 is optimal for women…
I’ve heard it all, probably you have too, and far too often & too recently from practitioners who should have rationalised & researched their way beyond these functional falsehoods, by now. I bought into these ‘optimal wellness truths’ hook line & sinker early in my career and proceeded to even propagate a few but with (not much) more experience in clinic, I had to seriously question this pursuit of ‘perfection’ & ‘perfect pathology’…in favour of reality & scientific evidence! They didn’t add up. Not with my patients – even the healthiest ones, in fact some of the really unwell ones occasionally had these kind of high-normal results and they were part of the problem!. ‘But that’s because no one is truly healthy outside of those seeing a functional medicine practitioner & supercharged on supplements & hormone replacements!!’ came the counter-argument. Ahhh, really?
How then do we reconcile this with the following: Individual genetics & biochemistry
Our biological resilience Healthy & appropriate senescence Large datasets of mixed race populations from other comparable first world countries…where these figures denote the statistical outliers?
I mean, if the 50th centile value for ferritin for actual living, breathing, bleeding, women in the US, Canada, Australia etc etc is 30-40 ng/mL and the 95th centile is 126 ng/mL and the WHO says that in fact, anyone menstruating with a ferritin > 150 ng/mL should attract suspicion for iron overload….but functional medicine men (mostly…sorry but it has to be said!) say 100 IS OPTIMAL FOR EVERY WOMAN #@^*…please tell me in which women, consuming what kind of diet, where in the world, & based on what improved or better health outcomes?
And while you’re there can someone please support this bold claim with a scrap of high quality evidence?? [Rant over🎤💧]
The falsehoods of functional medicine include the blanket belief, ‘more is better’ (ahhhhh not when it comes to many things, including iron where women’s lower levels have been found to be an evolutionary advantage…guys). But you know what, we’re better than that! We see each individual, recognising all the factors at play that make for their uniqueness, help to define what ‘healthy’ looks like for each person and don’t fall for one-size-fits-all claims without any evidence nor common sense even, to support them. What do you think?
Let’s make sense of the over-arching nutrition principles, that will profoundly change your understanding and application of this modality Truly understanding the ‘big’ concepts, so often overlooked, or incorrectly taught, ensures you get the critical ‘small’ detail in your nutritional prescriptions right. In this 4 hour recording, together with key clinical tools, we talk about the tough stuff: dose-response curves, active versus passive stores and excretory pathways and ooh lah lah…the myth of taking ‘activated vitamins’. Even those who feel satisfied with their original training – will find a lot in this critical review that is new, insightful and truly practise-changing!
I’m intrigued by the silence. Hair loss in women is frighteningly common, following pregnancy, menopause & with extreme stress (wait is that a tautology? 🙄) In fact it can strike at any age and for a multitude of reasons. When it happened to me a few years back I also initially responded with silence, terrified that if I said it out loud it would make it real, but when my daughter suddenly asked, ‘Mum are you losing your hair?’ with her trademark attention to detail & exquisite empathy, she gave me the words & a good kick into gear, simultaneously. Now I am fascinated by women’s silence around this generally, how little we share our stories & forewarn others, & as practitioners, the lack of adequate training we’ve had identifying the different types (hint: it involves donning gloves or if restricted to online consulting, knowing how to organise correctly positioned pics) & from there finding the right solutions.
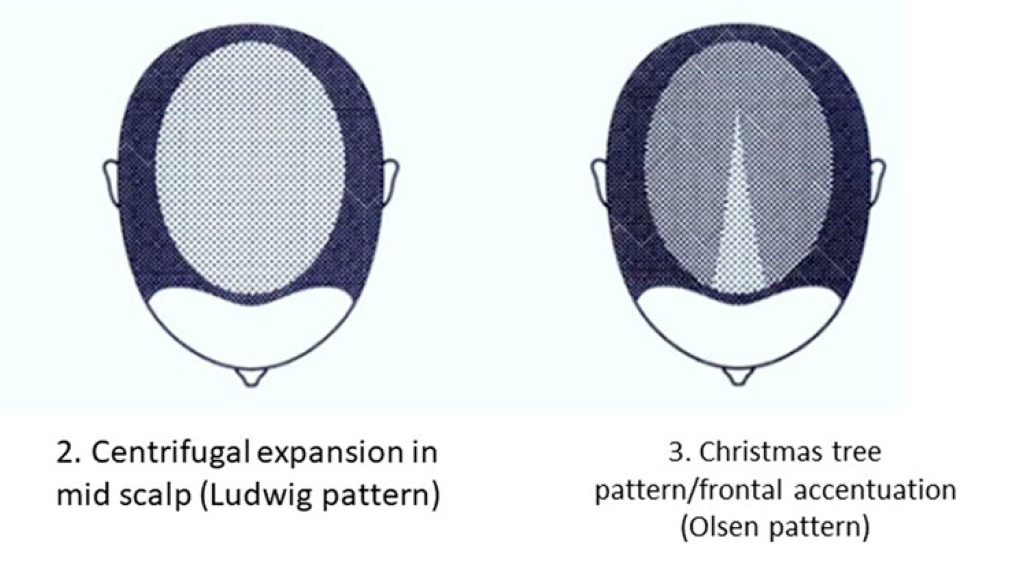
While Female Pattern Hair Loss (FPHL) is the dominant type in women – it only applies to the following pattern:
But alopecia due to stress, thyroid disorders, autoimmunity, contact dermatitis etc will affect different regions of the scalp and with a different onset & progression.
And remember, by the time YOU, the practitioner, can spot a patient is losing hair when they simply walk into the room, they have ALREADY LOST 50%😢 This is why I think we need to push back against the silence. The research is unflinching about the serious psychological impact this has on women – especially in cultures which place so much emphasis on looks generally, and hair, specifically as a commodity of very high value in women. The diagram above comes from a 2019 update on the phenomenon of FHPL and it’s a good articulation of the knowns and unknowns (pssst spoiler alert…it ain’t about androgens!) but let’s never forget the other causes and cures. So let’s make sure as the trusted practitioners women present to so often, we are sensitive enough to have this tricky conversation & skilled enough to help 💪
Stop Pulling Your Hair Out – The FPHL Answers You Need
Female Pattern Hair Loss (FPHL) is everywhere, perhaps you just haven’t been looking. As the leading cause of alopecia in women globally and with 1 in 5 women affected at any age, we’ve all got clients who have FPHL to different degrees. We need to be better able to recognise the early features of this condition which profoundly impairs quality of life and induces depression in its sufferers and that begins with validating patients’ concerns when they report “thinning” or “increased losses”. But what do we do from there? This recording talks you through the assessment, diagnosis and management of FPHL based on a combination of the most recent research and Rachel’s clinical experiences. Once you’ve ‘seen’ FPHL.., you won’t ever ‘unsee’ it and your patients will thank you.
Well, this is different, now I’m watching you! 😆 In early 2021 we released our very popular MasterCourse I: Comprehensive Diagnostics, as a ‘self-paced’ online offering for the many who missed out on attending live in 2020. Many have grabbed this opportunity with both hands (& a headset and some hardcore Do Not Disturb! signs) but we know that for some, doing the entire course on your own, >24hrs of video presentations, can be a tad onerous & overwhelming. We want to remove these barriers and empower & upskill as many practitioners in pathology interpretation as are keen, and as a means to achieve this, we’re offering the MasterCourse I Watch Party. So bring your bhujia and a beverage and let’s do this!!
Practitioners who sign up for this will be able to watch each session’s video replay live with other practitioners and have the opportunity to ask Rachel questions & participate in case discussions at the end. Another key detail is that we will run the sessions weekly, so that the full course is covered in just 6wks, from July 8th to August 12th.
MasterCourse I: Comprehensive Diagnostics LIVE WATCH PARTY 24 hours of live Zoom sessions + Bonus sessions! 8, 15, 22, 29 July & 5, 12 August on Thursday at 3.30pm to 7.30pm AEST.
Each Thursday, the video presentation for that week will be played so we can watch it together. Then Rachel will open up her webcam and mic, inviting you to do the same, to participate in a Q&A as well as set case discussions. When you register, you get immediate access to watch our preliminary/preparatory sessions, prior to 8 July: Accurate Pathology Interpretation Starts Here and the RAN Patient Pathology Manager Tutorial.
Below is an overview of the Watch Party schedule.
Week 1 – 8 July | SESSION 1: Acid Base Balance & Electrolytes
Week 2 – 15 July | SESSION 2: Renal Markers Week 3 – 22 July | SESSION 3: Liver Enzymes
Week 4 – 29 July | SESSION 4: Lipids & Glucose
Week 5 – 5 August | SESSION 5: Immune Markers
Week 6 – 12 August | SESSION 6: Haematology
“I thought my pathology skills were pretty up there until I did Rachel’s Diagnostic Masterclass course! Nothing like being knocked off my perch by a literal avalanche of new information, especially when it comes from the most commonly tests that we all use so often. The course has been a fantastic learning opportunity for me, and has since helped me pick out many intricacies in cases that have previously been missed.
The course structure was great, the level of detail was right up my alley, and the case studies were entertaining (in true RA fashion). Once again Rachel has increased my knowledge base, and help me provide way better service to my patients.” – Rohan Smith, Naturopath
Join Rachel on MasterCourse I: Comprehensive Diagnostics Watch Party and register here.
MasterCourse I is a pre-requisite to join MasterCourse II which will be delivered live in 2022.
I love a little temporal lobe tap. Especially the kind patients provide. This week mine came from a mentee’s patient who, while presenting with concerns about possible perimenopause, was found to have radical shifts in her thyroid hormones, largely thanks to a dramatic increase in TPO Abs (>1000). The patient’s other presenting complaint was ongoing gastritis (confirmed via scope) and reflux…and that’s when I started to deep-dive into the archaeological archives of my brain…with the…’didn’t I have somewhere in here, in some dark dusty deep recess…a connection between the two?!’
Aha! With the help of a torch [read Google Scholar] the temporal tap bore fruit. 1 in 4 patients with AITD (Hashimoto’s or Graves, you choose!) test positive to Parietal Cell Antibodies
I’ve created (clearly, not-so)SmartArt graphics on powerpoint slides on this exact topic, waxed lyrical about it in my thyroid training packages…but in fact needed a temporal tap to be reminded! And in turn thought, well gosh if this has slipped from my mind, it might just have slipped from yours too! ‘Thyrogastric autoimmunity’ as it’s called, refers to a patient group that exhibit antibodies to both and remember, the antibodies precede the condition in both disorders, so you can have a patient with established AITD, who has zero gastric symptoms but tests positive for the antibody…an important heads-up, as it speaks to significant risk of the subsequent development of gastritis in the following years. This excellent prospective study of AITD patients by Tozzoli and colleagues mapped exactly that! Jump forward just another day or so and…
I’m preparing for our final FiNAl FINAL Q & A on Haematology for our MasterCourse in Comprehensive Diagnostics and I’m wrestling with all the conflicting ‘facts’ about the anaemia that may present alongside hypothyroidism – it has been documented and described as being macrocytic, normocytic and even microcytic… how can it possibly be so diverse I wonder and then 💡 I’m guessing the presence or absence of these parietal cell Abs likely has something to do with it!!
Anyway, it’s getting towards the end of a VeRy loooooooooooooooooooooooooooooong year…thought we could all do with a temporal tap 😉
My how the time just flies when you’re chasing answers from private pathology companies! As Brisbane based naturopath, Sandi Cooper, can attest to having recently been down the seemingly eternal email trail with a pathology company trying to ascertain if their urinary iodine result accounts for the concentration of the urine sample (via the iodine:creatinine) or doesn’t….because of course it can make the world 🌎 of difference. Like clarifying that someone who appears to have very little iodine in their urine, actually has a lot or vice versa! I wrote about this back when I was a mere ‘babe blogger’, more than 5 years ago. After recently reading this historical document, Sandi has been practising due diligence and checking with her providers whether they have already corrected for creatinine..or whether she needs to herself and she shared that multi-departmental epic email endurance event thread with me. The short answer? They used to and now they don’t. Why? Oh…formatting issues or something 🙄
But just in case you do want the ‘short answer’ regarding your particular pathology provider…without emailing enigmas…the answer is, in fact, in front of you & it’s Super Short!
mcg/g Vsmcg/L
If your patient’s urinary iodine result (random or 24hr) is reported using the units on the left, sometimes actually written mcg/grCR, then BiNGo! The pathology provider has done the creatinine correction for you. If they only report the urinary iodine results using the units on the right…it’s time for some maths to avoid misinterpretation. No one panic, the formula is easy: Iodine (mcg) ÷ Creatinine (mmol) X 8.85 = Corrected Iodine. So don’t lose time sending endless emails like poor Sandy or placing countless calls, like poor Nina on my team…who has to pursue pathology providers on an almost daily basis for answers to our zillions of sensible questions!! Just check the units! You’re welcome everyone 😉 oh thank you Sandi for chasing this again and sorry about needing to chase this again! 😳
And if all of this is nEWs to yOU, you might want to review what you thought you knew, about Comprehensive Thyroid Assessment too!
We can never rest when it comes to learning more about the individual nuances of our patients thyroid pictures! In this 90min recording, Rachel covers the key thyroid parameters both functional & autoimmune (TSH, T4, T3, rT3, TPO, TgAbs, TRAB). As well as the most accurate methods of assessing relevant thyroid nutrients: iodine & selenium & a genuinely game-changing insight on interpretation of these . Finally she pulls all the individual parameters together to illustrate common patterns of thyroid imbalance – making it almost as easy 1-2-3! Well, hey..it’s the thyroid…a fickle fellow.
No doubt you’ve heard me refer to the thyroid Abs by their nicknames, TRAb is one I mention often, or Thyroid Receptor Antibody, as its mum calls it, when it’s in trouble. And it’s always in trouble! But TRAb is actually the collective name for several flavours of trouble. What these auto-antibodies share in common is the ability to bind the TSH receptors throughout the body. They differ however, in terms of whether, once engaged, they stimulate this receptor (mimicking the action of the real-deal TSH) or they block it, so that the real-deal can’t in fact dock and do its job. The contrasting consequence is clear: stimulating ones drive up thyroid hormone production, while the blocking variety contribute to low thyroid hormone levels – and what was meaningful was each patients (im)balance of the two to produce a net effect. Because yes…a proportion of patients make both.
In Australia, and many other countries, we previously measured TRAb as a sum total and then specified what fraction was each ‘flavour’ but then the ‘flavours went out of favour’!
So for a long time now, TRAb has been measured, undifferentiated, and the assumption is, they’re stimulating…because this is in fact a) more common and b) the most common reason this test would be referred for…a set of TFTs that look suspiciously on the high-side aka Grave’s disease.
But a new era has dawned, with many mainstream laboratories now opting for the more specific assay: Thyroid Stimulating Immunoglobulins (TSI)* over the old TRAb. Fancy schmanzy, I know. Considered more accurate in the detection of autoimmune hyperthyroidism and in this regard, we’re told we’ve made a diagnostic step forward and nothing has been lost. Except the much less common type of antibodies that bind the TSH receptor only to fill it full of gum so it won’t work. That apparently, due to its low incidence and reduced clinical impact is no longer something worth testing. So consider the TSI results for your patients, the new version of your old (drab) TRAb, with similar cut-offs etc. And remember detectable levels of this may be seen in toxic nodules, and acute toxic Hashimoto’s, as well as prodromal and active Grave’s disease.
AND DON’T FORGET
(and yes, I am screaming because it is so easy to forget!!)
Biotin!! Patients on biotin at the time of the test (even as little as 1mg as part of a formula) can produce False Positives for the TSI!!! And give you and your patient the ‘fright of your life’ with a pseudo hyperthyroid set of labs to match!
Need to read more on this because you’re left thinking WTF about the TSI?!@#%^ Check out Mayo Medical Labs (always a good go-to for info on pathology) or this recent review paper 🙂
*Note TSI does not stand for Turbo fuel stratified injection in this scenario!!
Want to learn all the thyroid antibody alphabet??!! Start Here!
Learn the ropes of Thyroid Dysfunction Assessment & Identification, including all the related thyro-nutrition! Rachel covers the key thyroid parameters both functional & autoimmune (TSH, T4, T3, rT3, TPO, TgAbs, TRAB). As well as the most accurate methods of assessing relevant thyroid nutrients: iodine & selenium & a genuinely game-changing insight on interpretation of these . Finally she pulls all the individual parameters together to illustrate common patterns of thyroid imbalance – making it as easy 1-2-3!…almost!


 You can purchase
You can purchase 
 You can purchase
You can purchase  The debasing of BMI as a stand-alone assessment of weight is long overdue given its significant limitations and lack of meaningfulness with respect to overall health. This coincides with a bigger societal and cultural shift towards inclusivity which involves redressing bias against people with diverse body sizes and compositions.
The debasing of BMI as a stand-alone assessment of weight is long overdue given its significant limitations and lack of meaningfulness with respect to overall health. This coincides with a bigger societal and cultural shift towards inclusivity which involves redressing bias against people with diverse body sizes and compositions. 
 MasterCourse I: Comprehensive Diagnostics.
MasterCourse I: Comprehensive Diagnostics.