Sometimes I think I must be psychic..or is that psychotic? Don’t answer that, it’s a bad Byron Bay in-joke. I had literally just recorded my Update in Under 30 Copper in Kids and this excellent new study was published that same week, assessing and comparing trace minerals in age-matched ADHD and neurotypical kids. Snap! ✨ First, a moment of panic…because believe it or not, there are very few rigorous studies that have looked into this and so I had already read them all cover to cover and could confidently say, I had a grip on the literature. Gasp…’ will it have a different finding and challenge the much broader story about the excessive demonising of this mineral in kids health?’ Everyone take a big breath out…no.
But if you’re someone who thinks you’re seeing Copper toxicity in kids, you can keep taking a big breath in and while you’re at it a huge bit of new information:
Copper Excess is Normal in Children.
Every investigation of blood Copper levels in kids has reached the same conclusion and this latest one by a Russian group of researchers renowned for their work in Copper agrees. So the ideas that we have about optimal in terms of mineral balance for adults may stand, but can not and should not be applied to children. The elusive 1:1 relationship between Cu and Zn, for example, considered aspirational in optimising the mental health of big people, is absolutely not desirable or even healthy, in little ones. Why is it so? I hear you ask (…because you loved those old Cadbury chocolate ads with the crazy Professor as much as I did) Well, essentially because kids need more Copper than us, as a simple result of their increased growth requirements: blood vessels, bones, brains…Cu is a critical player in them all and more. And while we (and when I say ‘we’ I mean ‘I’) may be passionately passionate about Zinc’s importance, turns out, in paediatrics, it really does play second fiddle to Cu and should.
This new contribution to the Cu & Zn in ADHD kids debate did find that compared with neurotypical kids, their Cu:Zn was higher BUT – **and this is the really important bit **- as has been shown in a similar cohort before, the shift in relationship between the two was due in fact to lower Zinc levels NOT higher Copper.
So, I guess when you think about it…Zinc perhaps really does still deserve all our loving attention we give it 😂…we just need to rethink the whole negative attention we tend to mistakenly give Copper!
Copper, as a kingpin in angiogenesis, brain & bone building & iron regulation is a critical mineral during paediatric development. So much so, the kind of blood levels we see in a primary schooler might cause alarm if we saw them in an adult. So too their Zn:Cu. But higher blood Copper and more Copper than Zinc are not just healthy but perhaps necessary during certain paediatric periods. This recording redefines normal, low and high with a great clinical desktop tool to help you better interpret these labs, as well as reviewing the top causes and consequences of both types of Copper imbalance in kids.
The latest Update in Under 30 has landed. You can purchase January’s episode, Copper in Kids here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
-Your RAN Online Account has a NEW LOOK!!-
Next time your log in, you will experience a more user friendly way to search, view, listen and download your resources. Find out what’s new here.
While we may not all be pathology proficient, overwhelmingly we do take or record blood pressure, right? It’s such an easy but essential inroad to understand something more about patients’ cardiovascular system, and indeed their nervous system, when prone to the so-called ‘white-coat syndrome’. And it never fails to amaze me how the ‘numbers’ are so abstract and cryptic to the average patient. They’ll tell you things about previous BP readings like, ‘it’s normally fine I think, you know, like a 40 and maybe a 160, does that sound right? Ahhhhh…not quite. But of course these two numbers are not cryptic to us. And like all patient results, rather than our response being a simple, binary, GOOD/BAD one, we should be asking ourselves: What does this actually mean? What is it telling me?
Consequently, I’ve been interested in the blood pressure battle going on in America. Having traditionally placed the greater significance on a patient’s systolic pressure with comparatively little attention paid to the diastole, there have been lots of ruffled feathers following the redefined cut off for hypertension, which now flags any diastolic pressure over 80mmHg.
An unhealthy high systole of course is undeniably the most meaningful in terms of short term cardiovascular consequences and we are in no doubt that lowering this is critical for risk reduction BUT a new longitudinal study of over 13,000 UK citizens just published in the Journal of the American Heart Association, suggests that perhaps patients’ high or high-normal diastole in mid-life was in fact the earliest warning sign of poor cardiovascular health in the future. This comprehensive study followed participants for 8.5 years and essentially found that a rise in diastole in their mid-life (ahem, that’s our 40-50s 🙄) predicted the progression of arterial stiffness more strongly than any other measure. Additionally, while diastolic blood pressure tends to decrease as we move into our 6th decade and beyond, those individuals in mid-life with higher DBP –> more arterial stiffness were same people in whom their DBP drops the most significantly later in life. What a guise!! So, in a nutshell this substantial study teaches us:
“Prevention of arterial stiffening and the associated transition to a late-life hypertensive phenotype of falling diastolic BP is likely to depend on effective control of midlife diastolic BP in particular.”
Fortunately, the people we see are more in their mid- than late-life, which this new understanding speaks directly to, presenting the greatest window of opportunity for prevention in terms of modifiable risks for chronic disease, especially CVD, dementia and renal disease which arterial stiffness is such a major risk for. This extraordinary separate longitudinal study following individuals born in 1946 also suggests mid-life BP(both systole & diastole) is the major modifiable factor for later brain volume, integrity and function. Maybe we need to keep our eyes on that lower figure and our ears more closely peeled to hear what in fact it’s telling us 😊
Increasingly our patients are coming armed with lab results and this cumulative data helps us to clearly see their ‘norms’ (as opposed to textbook ones) and therefore be alert to any changes. However, results from different labs at different times, and even the same lab, are unlikely to be presented side by side for easy comparison. They certainly don’t come with all the important information about what was happening for that patient at each time point – important details pertaining to the blood collection itself (fasting, inflamed etc) which can profoundly alter results or the broader context: menstruating, breastfeeding, losing weight, on meds and supplements. The Patient Pathology Manager retains all the results for you, including the critical contextual elements, helping you to keep more accurate records to make the most correct interpretation. It also assists you to monitor changes related to various interventions.
Previously, this tool has only ever been available to clinicians who participate in Group Mentoring but due to frequent requests for access, we thought it was time to share this great tool for those wanting a foot up with some better systems in their practice.
Copper deficiency happens in kids, so does copper toxicity and both are serious concerns, but do we know when to accurately call either? First, we have to know ‘normal’. If we know what normal Serum Copper values look like in children, then we can easily spot those falling below or above this, right? That’s the first hurdle we tend to knock over and break a toe on! Being a mineral whose levels vary widely in soil from country to country, globally, the differences in reference ranges are breathtaking & absurd. Add to that, that copper is a key mineral in kids, driving huge demand for it during key periods of development, so the range for pre-schoolers isn’t the same as the primary or high schoolers – not that your lab is flagging that. Unhelpful? Yes. Dangerous, even? Potentially.
To diagnose ‘Copper Excess’ in a child is a big call to make.
One, because most practitioners are unaware just how much Copper a child really needs at each age & two, high copper is often a messenger for something else going on and then three, the primary objective based on this diagnosis becomes to lower their Copper but we could be either shooting the messenger or missing the mark all together…right?
Copper excess does happen but not nearly as often as practitioners believe it does. And in kids, the fall-out from such misdiagnosis is bigger. And missing a Copper deficiency? (because we’re not as well-trained to recognise it and because Copper has been sadly demonised) Likely to have myriad negative impacts at this vulnerable age…almost none of which generate symptoms or a distinct clinical picture e.g. secondary iron deficiency, low neutrophils without necessarily compromised immunity. But what about the holy grail get-out of jail adjective: ‘relative’. You know, ‘this is at least a Copper excess relative to their Zinc?’
Well, to form this opinion you’re likely calculating the Zn:Cu ratio and applying an ideal adult value of 1:1 but show me the primary evidence that supports this for kids…anywhere? The Zn & Cu relationship shifts as we move through life-stages and in fact Copper is supposed to dominate through a lot of our childhood so…ummmmm…no.
HTMA Copper side-steps all of this?..double no.
I used to make the same mistake re Zn:Cu, I may have even taught you this?!🤦♀️ But as so often happens, a week spent in all the original scientific data and I’ve emerged a changed practitioner! Having been part of perpetuating this problematic premise in the past, I am determined to get the correct message out there to as many practitioners as possible. So help me spread the word on Copper in Kids – by telling others that this mineral is so critical to kids compared with adults, they will often have higher levels than ‘us’ and that until you’ve applied the right age-appropriate reference range and ruled out confounders you can’t possibly make a call on Copper. I mean, we kind of knew this all along, with healthy pregnancy Copper values being exponentially higher being a giant clue. Turns out kids’ ‘Copper Age’ extends way beyond the womb.
Copper, as a kingpin in angiogenesis, brain & bone building & iron regulation is a critical mineral during paediatric development. So much so, the kind of blood levels we see in a primary schooler might cause alarm if we saw them in an adult. So too their Zn:Cu. But higher blood Copper and more Copper than Zinc are not just healthy but perhaps necessary during certain paediatric periods. This recording redefines normal, low and high with a great clinical desktop tool to help you better interpret these labs, as well as reviewing the top causes and consequences of both types of Copper imbalance in kids.
The latest Update in Under 30 has landed. You can purchase January’s episode, Copper in Kids here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
-Your RAN Online Account has a NEW LOOK!!-
Next time your log in, you will experience a more user friendly way to search, view, listen and download your resources. Find out what’s new here.
When you start doing this with your patients’ pathology results, you know your client records are turning into a big hot mess and more importantly your ability to see the wood for the trees is seriously under threat! Private labs don’t play nicely with one another and if your patient has been to more than 1 pathology provider you lose an enormous amount of their potential value, blindsiding you to their patterns, & the most accurate interpretations. I have a saying when it comes to getting the most out of pathology in your practice: Cumulative Data is King & Context is Queen.
Increasingly we’re in in the fortunate position of patients taking responsibility for their health and coming armed with lab results – this cumulative data helps us to clearly see their ‘norms’ (as opposed to textbook ones) and therefore also any noteworthy variations.
But even in this luxurious position of multiple results across a variety of time points & stages of their life – our ability to derive the greatest understanding from these is greatly stunted if we don’t have the context.
For example: if he was ‘cross-fit-keto-crazy’ at the time, if she’d stopped being pregnant & started breastfeeding, if in light of a major shift in thyroid hormone results, they were on biotin, or iodine, or changed their dose of thyroxine or were drinking straight from the udder of a soybean (!) these all seem like fairly critical contextual details to be across, right? All of these factors: diet, acute health context, medications, reproductive state, even season… impact the lab results we expect to see and therefore should be captured and considered to form the most accurate interpretation. But how do we pull it all together in a systematic way that SAVES us time and SAVES your sanity and can keep growing alongside your ever-growing patient notes? Cue the: RAN Patient Pathology Manager!
Systems for sorting through huge amounts of patient information help us make sense of what we’re seeing…and help us spot the source & solutions.
Systematised patient timelines for a better overview of the chronology of any case, the RAN Patient Pathology Manager not only holds all the data for you, helping you keep more accurate records & make the most correct interpretation from these, but also maps and monitors changes related to various interventions. Lastly there’s my old BFF, Mindmaps and Timelines not ancient torture tools of clinical supervisors (!) but rather what distinguishes us as integrative, enabling us a to work up a case in a truly holistic fashion instead of: symptom–> solution, symptom –> solution. These are the 3 key clinic systems I really wished I’d had from the get-go…so, me and my team created them! We’ve re-crafted them with each year and this year our RANPatient Pathology Manager has undergone a significant evolutionary leap and it comes with a comprehensive video explaining how to easily get the most out of this resource for all your patients. We always share these tools with all our mentees but we’re frequently asked how others can access them so this year we thought those of you out there just wanting a foot up with some better systems might like to get your hands on them too! Maybe this is one very practical part of the ‘new year new you’?
Do you know this saying but the other way round? My dad said it often enough and always with such an exasperated tone that it’s got its own dedicated lobe in my brain. Almost. Lately, however, I’ve been reflecting on how much I learn from people younger than me, both patients and practitioners and think we need to flip it! I love the way that young people (oh lordy I just used the term, ‘young people’!!) can be incredibly solution-oriented, seemingly undaunted by the perceived barriers that tend to affect us older folk. A perfect example of this really is a young naturopath who previously worked for me, an absolute gun who seemed fearless in the face of any challenge who used to say, “my real super-power is forming the perfect Google search term” 😂 Of course this was totally under-selling her cleverness but I take the point that this is skill-set that us older peeps may be a little short on!
I really enjoy my consults with my Gen Y patients too for similar reasons. Check out this recent exchange with a 20 something female when I asked about her supplement compliance:
“Yeah, I use an app to remind me to take all the supplements and that gives me a weekly report so I know I’m usually about 80% compliant. I’ve dropped off a lot over the holidays but I’m getting back into it now. So I’ll wait til I’m back up to 80% to do these next bloods, right, because that would be pretty representative and show us the effect of what I am actually taking”
Are you hearing this?! How incredibly clever! One: she found an app (Medisafe) because she knows herself and she knows apps work for her! (and by the way, she said…yeah so the government probably now has this data as well but really, they had it anyway!) Two: she knows that it’s not human nature to be consistently consistent with compliance with anything, so more importantly she aims for doable, sustainable and therefore representative!! I myself even find myself delaying the pathology sometimes, erroneously thinking, oh I wasn’t at my absolute best this week!! 🤦♀️Dang, I wish I was that smart in my 20s. I may have saved a lot of sun-damaged skin, some serious $ and my dad many many headaches!
And my New Grad mentees, not all of them young by the way (!), but all new to the profession, when you check out their social sites, their business models and hear the life experience/past work they’re bringing together for exciting new hybrid offerings, it’s a quick reminder that wisdom isn’t a one-way street!
Want to know how else we can get smarter regarding your patient’s pathology?
As my patient points out, we should never put off getting labs done, waiting for 100% compliance. It may never come and if it does…it’s likely only fleeting and therefore any results in this context will be too! What are you and your patients missing in relation to their blood tests – like when to have the blood tests done in relation to food, exercise, alcohol etc Beware of Bad Bloods! Occasionally, the fault of the pathology company but much more often the fault of the patient and the referring practitioner, who has not educated the patient correctly about what to do and not do prior to blood collection for certain tests. This recording clearly describes the 7 classic give-away patterns of ‘Bad Bloods’ which will enable you to spot them fast in the future. In addition to this. while we are unlikely to know the idiosyncrasies of very lab our patients will ever have done, knowing the ideal collection times and conditions for the most common ones assists you and your patients to avoid any in the future – handy clinic resource included.
You can hear all about it and download the resource when you purchase Beware of Bloodshere.
It’s that time of year when we tend to set our intentions both personally and professionally. For me, between the many meals, pressies and dunks in the river, I slip into some ‘silent work’. In particular, I find myself flagging a couple of key areas that I want to sharpen my knowledge in this year. I’ve already picked mine…have you identified yours?
For many practitioners if there is one topic in nutritional medicine that seems to be more generous than any other it would have to be iron: Iron gives us patients…loads of them! Patients who present with deficiency, with overload, with something in between but still noteworthy, or on iron and that’s causing them all sorts of problems.
But Iron’s generosity doesn’t end there.
It also tends to give a lot of practitioners a bit of a headache!
That’s because a) we were mistakenly taught about iron as if it were just another one of the mineral mob and accordingly allocated grossly inadequate time to do more than scratch the surface of what we need to know and b) what we need to know, thanks to it being the most researched mineral, has undergone a couple of major revelations and revolutions since then anyway! So we can benefit from Iron’s generosity most and leave its other unwanted pressies (the headaches, confusion, frustration & suboptimal management of patients) under the tree – we just need to give iron the real attention it deserves, filling in the gaps in ours and many people’s knowledge about this critical nutrient. And boy, do we (and I mean everyone!! including doctors, midwives, pharmacists…anyone who has ever called iron deficiency on a client!!) need to learn how to correctly read iron studies!!!
Because iron also gives us much needed insight into other micronutrients and just how exquisitely sophisticated their roles & regulation can be. Thanks to it being one of the ‘older minerals’ we know more about it than any other and in turn we have the most advanced assessment methods: Iron studies, a collection of 4 parameters, like 4 chapters in a book or 4 key characters in a play, that need to be viewed separately and then together to understand the whole story.
Yes it’s true the learning doesn’t ever end and as I’ve continued to learn about new iron research I’ve added to our one-stop-iron-resource-shop..the Iron Package. Our very latest edition? A new clinical cheat sheet with some other important numbers on there you want to have at your fingertips whenever you read iron studies. So if you’ve already purchased and have access to the Iron Package…SURPRISE! 🤩 Go back and look again and if not, there’s never been a time like now. Oh iron, you’re sooooo generous!! 😉
Listen to these audios and download the resources straight away in your online account.
If you’ve already purchased ‘Update in Under 30: How to Read Iron Studies’ or ‘Iron Package’ you will find this new clinical cheat sheet available with these audios when you log in to your account.
I know, timing, huh?! It’s almost like I’ve been sniffing around your recycling bins but I didn’t need to of course, at this time of year it’s a fairly safe bet you’re madly winding it back a tad from your most outrageous annual alcohol imbibing. And so are all our patients. To me, extracting accurate information succinctly from patients regarding their alcohol use can be one slippery little sucker. It’s one of the questions people tend to give you a very tidied up answer to, or in fact they’re in such denial they can’t be considered a reliable witness. Think about it. Being a non-habitual drinker myself, I can appear almost saintly when reporting my daily consumption, “None”…but that omits the ‘other me’ that might show up at a conference gala dinner or some live music event, with my volume controls adjusted significantly up…ergh…firsthand accounts anyone? And how often does that happen? Well anywhere between 4 times a week and once a month. See what I mean?
While I’m sure you’ve probably heard me say before, I ask every patient who does drink, what kind of drunk they are because it can hint at their underlying neurobiology, there is a new study that suggests, using a very short 4 item UCLA RRHDS survey, we can categorise patients alcohol use and misuse into 3 types:
Reward ReliefHabit
and in doing so, also be better able to identify the best way to manage them as well.
I’ve been interested in addiction neurobiology for a long time and very much resonate with the work of Koob, which in layman’s terms proposes that we seek intoxication initially for the ‘high’ and then with dependence, we continue to seek it to appease the terrible lows of withdrawal. It has long been known that alcohol use disorder is heterogeneous – there are different types and accordingly the kind of generalised treatment of these individuals proves extremely hit and miss. But articulating the different types and their distinct drivers and solutions has been fraught. Like what makes one alcoholic the functional type who in addition to their long-lunches is a CEO and the one who can’t keep their job? Is it just socioeconomic context or something more? Why are some types of alcoholism deemed also to run more in families and while others aren’t? There are clearly major difference in pathophysiology but what are they? More recently these 3 groups have emerged and this recent study confirms the value particularly in the distinction between those who drink driven by reward and those for relief + habit. It’s a great read but here are some key take-homes:
ReliefHabit
Relief/Habit: You predominantly drink to cope with, or resolve a negative physical and emotional experience (negative reinforcement). You have more depressive features and have more anxious traits than those ‘reward drinkers’.The key to managing this type of pattern is to target negative physical and psychological experiences with ‘downers’ (they calm down an overactive brain that’s on ‘alert’) such as sedatives, anxiolytics, and glutamatergic modulation. (Hint for practitioners: this is where Taurine & Glycine really shine)
Reward
These individuals drink to feel good so they are driven by positive reinforcement and therefore the approach to the helping them should be quite different, with lifestyle recommendations that offer other options for mood elevation such as exercise etc as well and herbal and nutritional approaches.( Hint hint…not the key group for Taurine, more like Tyrosine and Saffron etc)
So…back to my question…what kind of drunk are you & what drives you to drink? As a nation of over-consumers by nature, this is a question we need to ask all our patients
Rachel introduces you to new clinical tools that has been developing to help us all better master the maze of mental health. With so many possible biological drivers: from methylation to inflammation and from gonads to gut, these tools can help you quickly identify those most relevant to each patient and also outline the strategies necessary for redressing these. This presentation comes with an extensive library of resources including pdf of Assessments Tools and Case Study Notes.
Earlier this year at a Mental Health Training for IM doctors, 3 practitioners (myself, a doctor & a psychiatrist) walked into a bar…not really, but we did each present a case study of challenging patient & in whom we had some great outcomes. All 3 patients presented happened to have Gilbert’s Syndrome. Just in case you’re wondering if there was a secret Gilbert Syndrome Conference you didn’t get an invite to, no. Or that perhaps there was premeditation and intention on the organisers behalf for a bit of sub-theme and focus, no. While this was purely coincidental it does speak rather loudly to a couple of things though.
Patients with Gilbert’s syndrome are likely to be over-represented in our client base especially among those presenting with psychiatric and/or gut issues (and both presentations frustratingly for them, very hard to diagnose, define, pigeon hole etc) and secondly, even though their genes underpin their biological susceptibility to such health problems, great outcomes are really possible.
One of the challenges comes from the medical dismissiveness of this genetic issue as simply ‘benign hyperbilirubinemia’. This has lead to a lack of diagnosis in patients affected and when it is incidentally picked up on routine bloods, a lack of follow up education about what having approx. 30% less phase 2 glucuronidation activity, in their gut and their liver, is really likely to mean, not to mention radically altered bile composition and digestion (!) and how they can make better choices in light of this. Similarly this year in our Mental Health Specialist Mentoring Group, the issue of reduced efficacy and tolerance of psychiatric medications, in those with Gilbert’s, raised its head over and over again. Given that so many drugs within the psychiatric class add at the very least to the ‘substrate load’ of the UGT system, if not frankly inhibit some members of this enzyme family, as this paper (check out Table 2…superb!) shared by my colleague, Kate Worsfold, points out, it actually shouldn’t come as a surprise.
But there is a change a’coming with an influx of research leading to improved understanding of this seemingly mercurial malady, resolving many riddles, identifying new key ways to help these patients and at last….some exceptionally good news for those with Gilbert’s.
For example, when I started this conversation back in 2013 with the Update in Under 30 Gilbert’s Girls, that was in response to seeing so many women at the time presenting with significant imbalances in both their sex hormones and their neurobiology as a result of their UGT impairment. But of course it was never meant to imply GS is just a girl thing! In fact there is a 3:1 dominance of men with this condition and some very good reasons as to why: more red blood cells and more testosterone…the former being the primary source of bilirubin and the later a terrifically powerful UGT inhibitor. The news from the research frontier is nothing short of thrilling, rewriting our thoughts on what medications and supplements (!!) are the most problematic, improved dietary management, how to track their progress more accurately and why completely normalising their bilirubin is not the goal…hey did someone say…longer telomeres?! 😉
The latest Update in Under 30 has landed: Gilbert’s – New Goals and Good News and my team has gone all out in producing a brilliant desktop reference to go with this recording that aids better understanding and clear treatment aims for your GS patients.
You can purchase Gilbert’s: New Goals & Good News here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
**But if you’re just joining us & this important conversation now,
ideally get the basics and backstory first and purchase all 3 key episodes in ‘A Guide to Gilbert’s Package’
-Your RAN Online Account has a NEW LOOK!!-
Next time your log in, you will experience a more user friendly way to search, view, listen and download your resources. Find out what’s new here.
When a teenage girl presents seeking her first oral contraceptive pill (OCP) script, what information is she privy to that enables her to make an informed decision? Read the insert inside the box? Please. Which 50 year old, let alone 15 year old does that? Forget it! What might her doctor tell her? Perhaps about clotting risk, as part of their determination of the suitability of this form of contraception for her but is there any discussion about the potential for adverse mood effects? A recent study of over 1,000 teenage girls followed over more than a decade adds to other evidence that suggests this should be flagged as a consideration prior to the prescription being written.
Most integrative health practitioners not only know about the potential negative impact on mood from OCP use in women but we’ve observed firsthand the havoc it has wreaked in some teenage girls’ and women’s lives.
A very experienced practitioner I know says, ‘if I am hearing mood instability and then I see a significantly elevated serum copper and or cortisol in these girls that’s when I just say to have to say to them, you know I don’t think this is the best contraception for you!’
This latest study did not find higher rates of depression across all OCP users in this group of 16-25 year olds but when they looked at this at different ages they found its use increased depression scores and was associated specifically with more crying, eating problems and hypersomnia. The discussion around the enhanced vulnerability at this younger age compared with older girls centres on the relative immaturity of their CNS. But wait, I hear you critical thinking clinicians ask, perhaps those teenage girls had more depressive features prior to starting the OCP. Good thinking 99! And the answer is…maybe…but the relationship goes both ways: from the related Medscape Continuing Medical Educational Activity
“For 16-year-old girls, the association was weakened after adjusting for depressive symptoms before use of OCPs, but the findings remained significant. This suggests that the relationship between OCP use and depressive symptoms could be bidirectional…For instance, 16-year-old OCP users were more sexually active and had more stressful events, as well as more menstruation-related pain and acne, than their counterparts in the nonuser group. Analyses showed that all these factors weakened the association, although none diminished it.”
The commentary surrounding this latest study is essentially 1) this is not the first study to find an association and others have been more able to demonstrate that COCP use predated the mood disorder in those affected and 2) those exhibiting higher depressive scores did not actually score strongly for anhedonia or sadness which are the most typical features in adult depression – so perhaps we are missing some of these negatively impacted young women. Awareness regarding reproductive psychology is rapidly growing and in Australia we are fortunate to have emerging hubs to seek help and specialist advice in this area, such as the important work of Professor Jayashri Kulkarni and colleagues out of the Women’s Mental Health Clinic. I’ve referred patients, both when a patient’s mental health appears to be caused or aggravated by use of hormonal agents but which they can’t not use for various reasons and for those small number of women in whom I feel hormonal management may in fact offer a psychiatric solution. So again I am asking, while we know & mainstream medicine increasingly knows about this association…who’s telling these young women?
How many of your clients are on a combination OCP? Do you know the full extent of the physiological impact as a result and are you able to identify to key pathology indicators of the size of that impact?
We’re all aware that in theory OCP use correlates with a range of elevated risks but in reality many females will make the decision that the pros, in terms of contraception or control of acne etc., outweigh the cons. What if we could provide more individualised advice by looking to their pathology results and identifying and quantifying specific danger signs for each individual? This approach enables us to better support patients who chose this form of contraception and to accurately identify those that should be be encouraged to find other safer options more biochemically suited to them. Learn more here.
Stop press. No, seriously. This new research warrants the attention of every practitioner working with children & teenagers. In the largest paediatric study of its kind to date, which included 2,480 children aged 10-18yrs diagnosed with hyperthyroidism (Grave’s or otherwise), Zader & colleagues found
Double the rate of ADHD diagnoses
5 times the rate of Bipolar diagnoses (almost 7 times in males)
5 times the rate of suicidality
That’s what I said: in 10-18 year olds
What is most alarming of course is that these mental health diagnoses were made in half of these children >3 months prior to the diagnosis of hyperthyroidism. What does this mean? It means we are missing this critical biological driver in this patient group. We all recognise the potential for some psychological presentations people affected with thyroid conditions, however, perhaps we are more alert to this in adults and letting it slip off our radar in kids? There’s been renewed talk about the over- and mis-diagnosing of ADHD lately and given that research has found up to 80% of hyperthyroid children meet ADHD diagnostic criteria this is one of the 1st place arguably to look! It also means, as these researchers discuss in detail, these kids are being medicated with psychiatric meds that in fact may, at the least mask their abnormal thyroid, lead to the incorrect diagnosis of hypothyroidism (lithium & even stimulants for example) or exacerbate their hyperthyroidism (quetiapine). But wait there’s more and it’s essential to understand.
Zadar & colleagues note that while we can not be 100% clear about the direction of the relationship…e.g. were these children already at risk psychologically and the hyperthyroidism just exacerbated that, they note that correction of the TFTs does not always equate to ‘cure’ of the mental health issues. This is not entirely surprising of course. What the problem emerges via a combination of biology and psychology & we resolve or remedy the biology…guess what you have left? PLUS the learned behaviours etc from suffering from anxiety, impaired cognition, suicidality they’ve been battling at the hands of excess T3 and a subsequent tsunami of reactive oxygen species.
This is one of those papers we should all have to read top to toe and therefore ideally be able to access for free but alas 🙁 What you can read is the Medscape review of this, which is a reasonable summary but the full paper is worth it if you can. You know the other key take home here…the diagnosis of hyperthyroidism was only made with overt out of range TFTs… which begs the question what about all those subclinical hyperthyroid cases we know exist? Yes, no wonder this paper has RACHEL’ S FAVOURITE written all over it…paediatric thyroid assessment and missed biological drivers of mental health and the opportunity to get better at both…can my research reading get any better this week?!🤓
Currently in Australia there is limited use of age specific reference ranges for thyroid parameters in children & teenagers yet they are essential for correct interpretation and diagnosis. Even doctors & specialists seem to be at a loss with diagnosing thyroid problems in kids unless they are extreme presentations. Subclinical thyroid presentations, however, are increasing in both children and adults. Many practitioners competent in adult thyroid identification & management are less familiar and confident with knowing when why and how to test in this population. Make sure you’re not missing thyroid imbalance in your paediatric patients…early detection makes treatment easy.
Our knowledge is subject to constant change, and it is oh so necessary to stay up to date in our field for a bazillion reasons, give or take a few 😉 So sometimes we can feel like we need eight arms (for the visual amongst us) to manage and keep up with it all. However, if we ‘use the force’ together we are stronger, learn faster and can stop with the whole ‘recreating the wheel thingo’ that so many practitioners find themselves doing out there in solo practice. Like, like…well, how confident do you feel about putting pen to paper? How good are you at your inter-professional communicating?
Referrals and inter-professional communication are just lightly touched on in the current undergraduate degrees (if at all!). But it’s actually such an important way to grow your own professional reputation while simultaneously the credibility of our whole profession. One might even argue, a pillar that stabilises the castle of shared patient-centred care & the future of true integrative health. I hear from my “New Graduates” as well as seasoned mentees about the unease that starts to creep in at the thought of writing the dreaded referral letter. I’ve been writing referral letters for 20+ years and it’s given me a lot of time to think!And refine. And refine again! To make inter-professional care a positive experience for everyone, we need to correct some misperceptions and ensure that our patients are everyone’s priority. And to fulfil our duty of care, communicating with the other practitioners on your patient’s healthcare team is fundamental. Sometimes, as you’ll learn, it’s about modelling the best kind of shared care to boot and being the bigger person 😉
Better still, positive experiences of inter-professional communication will bring collaborators out of the woodwork. Medicos and other allied health professionals you may never have been aware of otherwise, with a desire and openness to shared care tend to rise to the surface.
To get you even more excited about referral letters (you didn’t think that was going to be possible, right?!) and unlearn that Pavlovian procrastination you may have developed, Rachel has completely redesigned an older presentation to ensure it’s truly reflective of the contemporary healthcare landscape (oh yes, RACGP position statement included!). Expect to roll up your sleeves and get seriously practical advice with loads of examples about how to medico-speak naturopathic concepts, explain your role in the patient’s care, provide rationale for consideration of investigations and present ‘red flags’ with punch but minus the sensationalism. And above all else, reveal yourself as the asset you really are to the rest of the healthcare team.
“Thank you so much for a wonderful presentation yesterday, Rachel. It gave me a new perspective on how it must feel as a GP to receive incessant demands from Naturopaths/Nutritionists to order pathology for their clients. I am in awe of your integrity, desire for patient empowerment, humility and respect for other professionals in the mainstream health arena. I felt that every single naturopath and nutritionist out in the big wide world ought to have listened to your insightful words of wisdom when it comes to shared care of our clients. We are blessed to have you as our teacher.” – Michelle Blum (Mentee 2019)
Kupfernickel. It’s the original German name for Nickel and it literally translates to ‘Copper Nickel’ which inferred it to be the ‘Copper Nickel’ aka ‘Devil’s Copper’…because each metal can masquerade and be mistaken for the other! There’s an interesting story behind this of course and lo and behold the explanation (as is often the case with minerals and metals) is revealed by looking at where Nickel sits in the periodic table. Haven’t heard me rave on before about how all the key nutritional relationships are illustrated in that cornerstone of chemistry?? Where have you been?! Nickel is a transition metal and that tells us many things – including that its key relationships and interactions are likely to be with Iron, Cobalt, Zinc and Copper. And guess what? It’s all true. Still, I’ve had another Nickel-centric chemistry lesson of late because I actually had not the slightest appreciation of how noxious this can make it for us humans.
It started with one patient then, as is always the way, I’ve had about 3 in the past few months: predominantly women, some with ‘known’ nickel allergies, in the form of jewellery-related dermatitis and sometimes not, many with significant gut disturbance (IBS like, non-infectious gastritis) and most with early or advanced autoimmunity.
And the vast amount of scientific literature on the prevalence of Ni allergy (conservative figures suggest 15% population with a very high female:male) and its capacity to go beyond the ‘cosmetic’ and trigger gross immunological aberrations in Th1 cells, well, the case for Noxious Nickel is one of those things that once you see it, you can’t ‘unsee’, ever. Think if you or your patients have never had an issue with wearing cheap jewellery we can rule this one out? Think again. While the jewellery reaction might be the helpful clue in some patients, there are also 3 other ways that the old Kupfernickel may be undermining your health. And yes! The fact that contact dermatitis to nickel-containing silver jewellery is such a common issue tells us straight up, that its absorbed via our skin, think: watches, mobile phones, e-cigarettes, hair clips, and…yes I am having another crack at these again…tattoos! We also inhale and consume it via a wide variety of food and drink we consume. Oh and did I mention dental interventions, yet? 👀 Sheesh….
So while we all accept humans have zero requirement for Nickel, it’s in us all the time and the question is (always) how each individual inner chemistry lab (!) is interacting with it and to what extent this may explain some pretty potent health problems, from GIT disturbance to Hashimotos and from skin conditions and alopecia to CFS & Fibromyalgia-like conditions.
My latest Update in Under 30: How Noxious is Nickel – highlights the fundamentals of Nickel in terms of our sources of exposure and who is most susceptible and just how this can play out as a driver of disease. Next month we move onto our testing options, drilling down into the myriad signs & symptoms and how to effectively manage the patient dancing with the Devil’s Copper. This one has been a real ‘sleeper’ for me, but it’s time to wake the beast for us all 👀
While nickel sits benignly among its mineral mates in the transition metals of the periodic table, it is a metal that humans are constantly exposed to yet have no need for. What could possibly go wrong? Well, a lot it seems. Nickel is the most prevalent metal allergen worldwide and beyond this there is strong evidence of its potential to trigger autoimmunity, major endocrine pathology and a raft of GIT problems that masquerade as other conditions like IBS & NCGS. This episode captures the dance we all do with the ‘Devil’s Copper’ and why some of our patients are likely to end up with a bigger dose and a much bigger disease picture as a result of noxious nickel.
Hear all about it by listening to my latest Update in Under 30:
For all Update in Under 30 Subscribers, it’s now available in your online account and if you are not a subscriber you can purchase this individually here.
Tonic. Homeostatic modulator. These terms and concepts, which have a long tradition in herbal medicine (and let’s be clear, were considered yet another example of the wishy-washiness of the modality) are being appropriated by some areas of mainstream medicine right now. Cheer up ‘leaky gut’, you’re no longer alone! And arguably misappropriated by the public’s very ‘lay’ interpretation of the science on medicinal cannabis and its subsequent elevation to panacea, of late.
“So many of my patients are telling me they’re taking Cannabis now, just as a tonic”, says yet another practitioner to me recently, “No, not for pain, they’re young and fit but they take it because it’s a homeostatic regulator!!”
Oh lordy…
The capacity to maintain homeostasis, and particularly in the face of adversity or imbalance, is a sign of the vitality of the individual, according to what I remember from naturopathic philosophy (and have truly taken on and observed firsthand)…so just back up there a tad and explain to me how this one herb proposes to do this for everyone on a one-size-fits-all-fashion? As confessed in an earlier communication, I am a cannabis convert. But only in the sense of appreciating the niche areas where it is likely to offer true therapeutic benefits. I still have the words of warning from the brilliant Professor Michael Lintzeris, the Director of the Drug & Alcohol Services, South East Sydney Local Health District; Conjoint Professor, Division of Addiction Medicine etc., ringing in my ears, pleading with health practitioners to not ‘fall’ for cannabis in the way we have previously ‘fallen’ (so far and landed so badly) for the panaceas of the past: opiates and benzodiazepines. Most notable major omission for me, in an otherwise rigorous scientific debate of late, is any discussion about its potential for impacting fertility.
There is in fact evidence to suggest ‘sperm under the influence’…’lose their way’ and are less effective at finding and fertilising the egg. Sorry but the image always makes me chuckle…stoned sperm. ‘Hey, dude where’s my egg?!’ style. But it’s not funny when impaired fertility is a problem affecting so many these days, and we still are guilty of over-focusing on ‘her’ and under-assessing ‘him’…and lo and behold it could be his chronic cannabis use to blame. We had a case recently, years of unprotected sex, daily cannabis, no baby, no dots connected. We may think this is a handy incidental contraceptive for young men sitting on couches with cones (one mum recently said as much to me) but for the rest…?
As practitioners we should know as much about investigating and treating male hormone imbalances as we do female ones, yet this is often not the case. While we are increasingly aware of everyone’s exposure to lifestyle & environmental endocrine disruptors and the fragility of the HPO axis, we sometimes fail to recognise that the reproductive health of our male patients is equally under threat. This is clearly demonstrated by generally diminishing levels of testosterone amongst men and increasingly early onset of andropause. These issues then become barriers to achieving success in other health areas with your clients, mood, metabolism, fertility and beyond. Learn more here
I’d love to continue this conversation with you… so join me and be part of my ongoing dialog on this and my other blogs by following my Facebook page.
My current count is about 13. Lucky for some? Patient advocate, referral point, primary prescribing practitioner, behavioural change motivator, wise business counsel, good empathetic listener, fearless myth buster, researcher, head chef to a group of nats…that’s the toughest hat right there, right?! 🤣
While there is a concern in naturopathy and integrative health that we increase our own load due to our eclecticism – I see this as a strength & part of the appeal.
But it does warrant regular review.
I semi-regularly cry-out, “I just want a normal job, you know 9-5, clock on, clock off.” To which anyone who knows me tends to drop to the floor in a fit of uncontrollable laughter. They’re right of course, I do not have the temperament or the ability to be sufficiently single-minded to work at Coles. And the reality is I do feel privileged and satiated by wearing all my different hats bar just a couple…but this is par for the course and part of the important reflective process we should all continually undertake in our careers: Which hat no longer fits me? Which gives me a bit of headache? We can then re-orient our work and our businesses in a way that tries to reduce, or remove altogether, our time spent in these roles.
“I am completely over giving 101 dietary advice!” I wish I had a holiday for every time I’ve heard a nat with more than 10 yrs experience say that!
“Oh the never ending story of answering my inbox!!!!!!!!!!!!!!!!!!!!!!!”is another one on high rotation in our ranks.
These ‘lost loves’ and potential disproportionate time wasters should never be ignored & simply endured but should instead be met…head on. The more I hear about different practice models & observe my own business over 20+years, the more I can see that when a practitioner is losing too much time or job satisfaction, wearing some of these hats that no longer fit, the less financial growth and sustainability their practice model holds. I know…them’s fighting words! Anyway, I’ll be talking about this and the delicate balance of our mild super-powers V our soft underbelly at Vicherbs monthly meet-up Sept 26th if you live in Melbourne and want to come along the join in the conversation. I think it’s a good one that we need to keep having.
The Group Mentoring program provides integrative nutrition practitioners with monthly sessions of the most accelerated form of post-graduate education and clinically relevant skill development. Join this online 12 month program of like minded professionals and work with Rachel through real clinical cases and questions presented by each member in a collegiate setting. If you know you want in for next year already, get ahead of the queue and email us: [email protected]
“Rachel’s mentor program is something I look forward to each month and I feel very privileged to be one of her mentees (or mintees as she likes to call us). Each session is action packed with so much information shared that my brain gets a lot of dopamine hits! Rachel has a rare talent of teaching in a way that makes the most complicated information easy to understand, and even fun! The learning doesn’t stop after each mentor session. The group, including Rachel, will share research and continue to follow the cases shared. Amazing value for money. I know this is something I will want to do my whole career…there is always something more to be learned.”
Histamine, Oxalates & Nickel…any of which may be at fault when your patient reports they experience adverse reactions from eating them.The same can be said for legumes, with a few extra contenders thrown in like oligosaccharides for those farty on FODMAPs. Additionally, in either case, there could be a bona fide allergy (IgE) or an intolerance (IgG) at play. Tricky, right?
I hear from practitioners often, though, that their interpretation of food reactions like these are at risk of being 1 dimensional, like a food word association game: tomato = histamine; legumes = FODMAPS; gluten = NCGS.
The labyrinth of possible pathways for food reactions is just that, a labyrinth!! So, we have to always be on our toes and try and approach each case methodologically.
I outlined how to approach this in clinic in A Guide to Investigating Food Reactions, released earlier this year. We cover a lot in this 2hr recording, but let’s face it, it’s an area that needs yet more time and a field that we never stop learning in. Next week, as part of our UU30 series on Getting to the Guts of Joint Pain, we need to take a little scenic detour along Oxalate Boulevard! Keep your eyes open peeps, because our very own food prescriptions tend to be full of them!! Not naming any names….berries, green smoothies, sweet potato &…
Need to catch up on investigating adverse food reactions??
Elimination of suspected food culprits in most situations is only a short term reliever, not an appropriate long term solution, so to optimise results we need to know the real mechanism of action. The majority of these, of course, stem from the gut, but being able to elucidate exactly which of the many things that can go wrong there, is going wrong and therefore what foods are problematic until we address this, is the key. This 2hr mp4 is all about the bigger picture and helping you find method in the madness that can be the adverse food reactions landscape.
Integrative Psychiatry is an inspiring area to work in & its evidence base, acceptance and recognition of potency is rapidly growing & offering more patients, more. Going beyond the ‘neurotransmitter imbalance model’ for each presenting diagnosis helps us to see the unique mix of biological & psychological drivers in each individual who presents seeking our help. However sometimes I believe, we find ourselves falling into looking through the lens of just another short-list of alternate models:What kind of methylation imbalance does this person have? What sort of Zn, Cu issues?
While I am so grateful for having learned these tools and watched them be very successful in a portion of my mental health clients, they are simply not the answer for everyone. We need to keep our thinking and practices dynamic and up to date, to reflect the incredible increase in research in new areas of integrative psychiatry, such that more of our patients can benefit and that we can continue to think beyond the box…even if that box itself was originally so progressive!
What do you know, for example, about abnormal purine metabolism in mania and using serum urate as a BPAD prognostic marker in depressed patients? Think you can simply be guided by the reference range provided, think again. What could good old LFTs reveal about our patient’s mental health vulnerabilities and what have we potentially misunderstood about copper in this area, particularly in children?
I appreciate Zinc’s role in mental health as much as the next integrative practitioner. Okay, given my 20K word thesis manifesto, more. But increasingly I am seeing mental health patients who need treatment with different tools. This upcoming ACNEM Mental Health Module in Perth is on point: thinking outside of, outside the box!
While the above only speaks to what I’m presenting, I know Dr. Sanjeev Sharma will also be sharing his wealth of individualised management insights and he’s a big fan of addressing Chronic MIld Metabolic Acidosis as an early treatment objective. Maybe we all need to hear why? And I am so looking forward to getting a PTSD update from Christabelle and hear all about the research into therapeutic keto-diets in psychiatry from Cliff Harvey…haven’t read all those papers to know which conditions and when this approach shows merit? No, most of us haven’t. That’s the point of outsourcing our up-skilling to colleagues who we know are across these more than us and to boot have the clinical experience to ‘make real the research’. As I’ve said before, given the content of this upcoming ACNEM Mental Health program, I wish I wasn’t presenting really, so I could just kick back and take it all in, uninterrupted. But alas, I have some important new information on reading basic bloods through a mental health lens to share! I really hope to see you all there. Let’s get out of the rut of 3-4 nutritional approaches to mental health and make the most of the explosion of research and shared clinical experience.
ACNEM Face-to-Face Training Fremantle, 27-28 July 2019 at the Esplanade Hotel Fremantle by Rydges https://www.acnem.org/events/training
Oh and while you’re here…did you know the research into both beta-casomorphins and IgG casein reactions in relation to certain mental health diagnoses has taken some giant steps forward in the last couple of years? You should. Milk Madness is back and it’s via two distinct mechanisms – identifying which might be at play in your patients & correct management is now clearer than before. Want to get up to date in this area of mental health – check out our UU30 recordings: Milk Madness part 1 & part 2
Remember biochemical individuality folks? That great core underpinning principle of naturopathic & integrative nutrition. We should always keep this in front of mind, when something utterly fabulous for absolutely everyone pops its head up. Like every month or so, in the area of health, correct?
Fasting, in all its forms, is having a lot of time centre-stage right now. What a novel & truly prehistoric notion in this era of food 24/7! I get it and I agree, most of us would do much better by regularly moving out of the top paddock.
BUT…and there has to be a but…or we are no longer treating the individual…
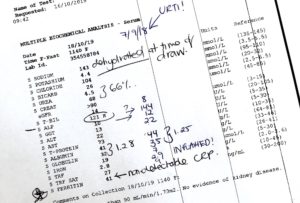
Some of whom, due to specific conditions or biochemical tendencies, do utterly horribly with any sort of prolonged periods between feeds. I already have a hit-list of conditions where fasting and food restriction is a no-no…then I saw a set of labs the other day from a patient who self-initiates regular, 4-6 day fasts during one of said fasts,whose alarming results jumped out in bold, italicized CAPITALS, illuminated itself in neon pink and reminded me to remind you! This patient’s (extended) fasting labs went a little like this… total bilirubin 48 (normally 15 umol/L), bicarbonate 18 (normally 26 mmol/L), corresponding anion gap 20 (normally 12), uric acid 0.62 (normally 0.4 mmol/L). Are you thinking what I am thinking B1?
So here’s my hit-list of ‘fasting = foe’ for – still subject to case by case assessment (of course!! because we treat the individual, right?!)…but
Any individual with a history of, or currently risk factors for, disordered eating, e.g. orthorexia, bulimia, binge eating disorder, anorexia
Gilbert’s Syndrome
Low T3 – thyroid ‘hibernation’
Hypocortisolemia
Anxiety and PTSD
Drug addiction
Children, pregnant women, the elderly…of course!
In short: any patient whose condition or biochemistry may be too negatively impacted even in the short term by any of the following: higher cortisol release, significant slowing of phase II detoxification, or radically elevated acidosis, should step away from the fast and towards the fridge! 🙂 🙂
Thyroid hibernation produces a low T3 value coupled with a ‘lowish’ TSH and typically a clinical picture of hypothyroidism. As the practitioner we are faced with the conundrum of how to effectively ‘wake up’ the pituitary which appears to be sleeping on the job. This audio connects up the dots between this type of thyroid dysfunction, dietary patterns, restrictive eating (including a history of eating disorders), carbohydrate intake and disturbed iodine nutrition of the thyroid gland. This pattern is increasingly seen in practice and this audio is a must for anyone working in the area.
Do you know that saying, ‘mind your Ps and Qs?’ It basically means mind your manners and I heard that a lot as a kid 😉 But what we really need to hear now, as practitioners and promoters of healthy eating and wellness is really, Mind your P’s and P’s because a lot of biggest health consequences of any diet are determined by the balance or imbalance of two major players; protein and potassium. We’re always looking for simpler ways to enable patients and ourselves to be able to both recognise the strengths and weaknesses of their diets and, better still, apply a simple method to making better choices moving forward. Eyeballing the protein and potassium rich sources in any diet speaks volumes about other essential dietary characteristics and the likely impact of diet on health – and getting the relationship between these two right should be a goal for us all.
“World Health Organization (WHO) Dietary Targets for Sodium and Potassium are Unrealistic”, reads the recent headline from yet another study finding that humans would rather challenge the solid science of human potassium requirements than acknowledge the urgent need to turn this ship of fools around!
This large study, conducted over 18 countries, involving over 100 thousand individuals, reported that 0.002% met these targets. That’s 1 person in 50,000. Now, the researchers’ response to this is that we should lower our dietary potassium expectations….such that the targets are more achievable and so that (frankly) we are less perpetually disappointed in ourselves and our terrible food choices. Wha????Back up there. The WHO guidelines, just like any other nutrition authority, derived these minimum amounts from a thorough review of the science that speaks to our physiological requirements and the level of nutrients that have been shown to be associated with health. Australia’s own fairly conservative NHMRC suggests even higher amounts for good health! Perhaps rather than revise the established dietary targets we should revise what we’re putting in our mouth!
So where does protein come into this? Well one of the most important and central nutrient dynamics is the balance or imbalance of our intake of both. And in this regard, yet again, we have a surprising lot in common with plants! Whether you’re trying to understand optimal nutrition conditions for growth (nitrogen alone won’t get a plant there, nor protein alone in a human) or the intricacies and nuances of finely tuning our physiological processes such as cardiovascular function, renal health, blood glucose management etc. the answer lies in a happy marriage between these two.
In this area of nutrition, we should be listening most closely in fact to renal specialists/researchers. These ‘undercover’ protein and potassium experts have been talking about this for a long time and in particular, in my humble opinion, Lynda Frassetto has lead that charge for decades. If you haven’t read much on this issue and want somewhere to start at least, jump into her pivotal paper from 2001 which eloquently explains why the human design can not shoulder a potassium shortfall…well not without causing real health problems…like the ones we’re seeing in record numbers currently and why the protein potassium balance of any diet is a major health determinant. That’s why giving ourselves and our patients the knowledge and the tools (yes lovely shiny meaningful infographics included!!), to quickly determine their protein potassium balance, are so necessary and important.
Thanks to Frassetto and many other researchers’ work, looking at food through this protein potassium lens has sharpened my focus and I think it’s about time we all took a good look 🙂
Check out the latest UU30 to hear the latest information…
The health consequences of any diet are largely determined by the balance or imbalance of two major players & proxy markers; protein and potassium. When it comes to this area of nutrition, we should be listening more closely to renal specialists whose research shows why the human design cannot support a potassium shortfall and the health consequences of this. Whether you’re trying to understand optimal nutrition conditions for growth (nitrogen alone won’t get a plant there, nor protein alone in a human) or the intricacies and nuances of finely tuning our physiological processes such as cardiovascular function, renal health, blood glucose management etc. the answer lies in a truly happy marriage between our intake of these two. These recording comes with a clinical resource tool to help you quickly identify the dietary protein:potassium balance for your clients.
Hear all about it by listening to my latest Update in Under 30: Mind Your P’s and P’s For all Update in Under 30 Subscribers, it’s now available in your online account and if you are not a subscriber you can purchase this individually here.
How often were we told this in our training? And how often have we found this to be true in practice? And now suddenly, it seems, the medical researchers (at last!) are rapidly coming around to this core concept?? Our microbiome is suddenly the hottest property on the body block, and it seems every interested party is shouting, ‘Buy!Buy!Buy!’ As integrative health practitioners, of course, we had a major head-start, not just by appreciating the gut’s central positioning in the whole health story (iridology beliefs, maps & teasers aside!!) but also a heads-up about the damage the western diet, our medication exposures and lifestyle tend to wreak upon it. A favourite quote of Jason Hawrelak’s by Justin Sonnenburg, “The western diet starves your microbial self”, underscores the significance of just one element of this impact. And…are we all clear that the increasing number of patients reporting adverse food reactions, once again, overwhelmingly are a response to aberrant processes in the GIT?
Sounds silly it’s so obvious right, but it’s easy to get distracted & misattribute blame…for example, it’s the food that’s the problem. Well yes in a minority of situations interactions between someone’s genes, immune system and a particular food turns something otherwise healthy into something pathological, but for the majority, the food itself & in others is healthy, & could be beneficial to this individual, if only we could resolve their GIT issues…like FODMAPs for example.
Not the problem, just the messenger.
So if the ‘problem food’ is just the messenger, what’s the actual message we need to understand? Is it that this patient has medication, disease or otherwise induced hypochlorhydria, impairing ‘chopping up’ of potential antigens implicated in immune mediated food reactions? Or is that this person’s got fat maldigestion &/or malabsorption so that in addition to not tolerating fats, they may experience dietary oxalate intolerance to boot? Or are the food reactions the result of altered microflora changing what we can and can’t digest (via their critical contribution) & absorb?
So what message does the presence of IgG antibodies to consumed foods send us about the state of someone’s gut? It’s telling us 2 things: this individual exhibits abnormal intestinal permeability & currently in the context of this leaky gut, these foods may constitute a barrier to resolving this & other symptoms as well.
We’ve recently released the mp4 (that’s audio plus the movie version of the slideshow so grab your popcorn…that’s if you don’t have a corn issue!) of A Guide to Investigating Adverse Food Reactions – What’s IgG got to do with it? which details the science behind IgG, including debunking, the incorrect debunking of IgG food antibody testing!! But more than this, it overviews the whole maze of adverse food reactions, articulates a logical investigative path for practitioners through this maze, and helps us to really understand that finding the food(s) responsible for a patient’s symptoms is not the final destination..and can be in fact a distraction, if we don’t cut to the chase and find out the why…and funnily enough…my dear old iridology teachers and colleagues...it almost always comes back to the gut 😉
Confronted with the possibility of adverse food reactions in an increasing number of our patients can be an overwhelming prospect, in terms of accurately identifying and understanding the faulty mechanism underpinning these aberrant responses to healthy foods. Elimination of culprits in most situations is only a short term reliever, not an appropriate long term solution, so to optimise results we need to know the real mechanism of action. The majority of these, of course, stem from the gut, but being able to elucidate exactly which of the many things that can go wrong there, is going wrong and therefore what foods are problematic until we address this, is the key. This 2hr mp4 is all about the bigger picture and helping you find method in the madness that can be the AFR landscape. Along the way, we detail the science of where IgG reactions fit into this and it’s a fascinating story that just might be the missing puzzle in your leaky gut patients.
How long? How long must we sing this song? I’m feeling a bit 80s anthemic and righteous. It turns out that patients’ bowel movements could be improved by using a foot stool?!! Who said that??
Only every naturopath, ever. Right?
But now medical researchers are singing the praises of the Stool Stool too…sorry, I mean the ‘defaecation postural modification device’…because lo and behold a new study of over 1000 bowel movements revealed using a stool to elevate your feet while on the toilet improved the speed and ease, improved full emptying, reduced the strain etc of laxation, >70% of the time, even in ‘healthy, non-constipated patients’. There’s a quick video you can watch to get across this groundbreaking research, or you can read the full article here. I’ve been educating patients about this for about 20 years and it never fails to revolutionise their world!
It would seem that elevating your feet results in straightening “the unnatural bend in the rectum that occurs when sitting on the toilet by placing the body in the squatting position nature intended”…hang on a second…who’s calling what unnatural???…I think the highfalutin anti-anatomical bathroom contraption, we westerners call a toilet, wins the ‘unnatural’ crown!
Next thing you know there’ll be a study that tells us squatting to have babies makes more sense that lying on your back…right?! 🙂
Love talking all-things Stool?
Fabulous Farty Fibre is a previous UU30 recording. Rachel at her warmest and funniest reminds us that fibre is a critical component to good nutrition and is often overlooked, partly due to the popularity of paleolithic and no grain diets. This UU30 details the important functions of different types of fibre and therefore the importance and therapeutic applications for fibre diversity.