It’s no secret I am in the midst of some serious deep-diving through the micronutrient evidence base & at a depth of about 30 metres I struck Boron! Don’t yawn! I saw that. Thinking, ‘boring’, when we hear, ‘Boron’, is almost as bankable as watching everyone reach for their water bottles when you mention anything hydration-related 🤣 But I am here to restore your positive regard for this mineral and remediate its bad (& boring) rep! In preparation for the Nutrient Prescriber’s Program we started each nutrient review with the seminal contemporary nutritional texts and then launched ourselves headlong into the latest & greatest research. By the end of all the Boron bits in all my trusty texts the yawn was not gorn! But the moment I started reading the research I was like, ‘Are we even talking about the same thing?!’Turns out we’re not 😵🤦♀️
You see Boron has been a longstanding victim of identity theft. What we’ve been lead to believe is Boron is weed-killer and ant-poison and look it does give us some of the benefits of Boron but not all. And it possess a pharmacokinetic & toxicity profile that naturally occurring Boron simply does not.
Who decided that the Boron that is ubiquitous in our environment but almost exclusively consumed by us only after biotransformation by plants – could just skip that last bit and still be safe and optimally beneficial?! Probably the same guy that came up with folic acid, may I suggest? Anyway, enough is enough. We all need to relearn Boron – naturally occurring Boron – in the form of Sugar Borate Esters (SBE)- the evidence of benefits for which will blow all of our little minds! Well it certainly blew mine! Looks like this natural form of Boron is going to hit the Australian market in the not-too-distant-future 🐦 can’t wait to see which supplier is sufficiently progressive and research-aware that they bring this to market, having been available as a high grade supplement, employed in numerous RCTS OS for some time. But this little Update in Under 30 is not waiting around for that release date – there is much to be gained from SBEs right now – so make some noise as the real Boron at last takes the stage!🎤
Boron has been the victim of longstanding identity theft and we unknowingly have been interacting with its imposter. Contrary to everything you’ve ever been told about this mineral, naturally occurring Boron is full to overflowing with benefits for our gut, our bones, our brain, our management of other minerals and is safe in large quantities. That ‘bad guy Boron’ you were introduced to and is still present in many of your supplements is a form we never consume in food…and therein lies a world of difference! Come meet the real Boron so you and your patients can get the real benefits!
You can purchase The Boron Deception: How We’ve Been Fooledhere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
The debasing of BMI as a stand-alone assessment of weight is long overdue given its significant limitations and lack of meaningfulness with respect to overall health. This coincides with a bigger societal and cultural shift towards inclusivity which involves redressing bias against people with diverse body sizes and compositions.
And how do we, as integrative health professionals, continue to uphold our principles of prevention and treating the cause when excess adiposity may be a very real contributor? While ensuring we ‘see’ and treat each individual in front of us, not our assumptions about adiposity, not our body size bias nor blind spots?
One part of the answer: read and be led by their lab results – because pathology is nothing if not personalised.(more…)
Heck yeah. It’s going to take a lot more than 1 push-back post to turn this ship around! Likewise, I was only getting started with my recent Update in Under 30 episode, ‘What’s Hiding Behind Histamine’ 🤓😂 & part 2 has just been released where we unpack the case of a 41yo female with chronic diarrhoea, multiple food reactions, very high stress and very high oestrogen. Sounds like she’s a walking Histamine Headline – except she isn’t.
Right now we really do need to keep this conversation going such that a healthy discourse can help us deconstruct the histamine dogma.
I know I’m showing my age here, but anyone remember when Candida was having a ‘moment in the 90s? Ok, so that ‘moment’ stretched to over a decade of a ‘Candida-contagion’. No one could eat melons or mushrooms, eat ferments or feel joy. It was a bleak time that did our profession some reputational damage. Not only because seeing an ‘alternative practitioner’ became synonymous with being put on an unbearable, unattainable restrictive diet and positioned practitioners as peddlers of punishment but also because it took some time for science, in the form of accessible (& always improving) assessment methods, to come along and save us from the folly of the 1-diagnosis-for-all mentality.
Let me ask you, how many times do you actually see Candida overgrowth on reports from stool testing performed using best practice modern methods?
In my experience – never – not as a stand-alone issue. Occasionally, as part of the overgrowth of a suite of opportunistic organisms where the real-take home is the need to ‘remove the opportunity’ via the promotion of more good guys. So not only was the diagnosis incorrect, the proposed treatment for it was a complete misdirection as well.
Can’t help thinking in the current climate of Histamine Hysteria that history is repeating itself.
How will we all individually, and as a profession, respond this time?
In this follow-up episode we observe how the 3 key elements often hiding behind a histamine intolerance diagnosis: Misunderstandings, Missed Messages & the potential for Mistaken Identity, have played out in the case of a 41yo female who presents with chronic diarrhoea, a long list of problem foods including now a suspicion of ‘histamine foods’. Rachel offers up new ways to approach the patient work-up that cut through the ‘noise’ and enable us to better identify what is hiding behind histamine in similar cases of marked gut dysfunction.
You can purchase What’s Hiding Behind Histamine? – Part 2here. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account. You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
You’re invited to attend acnem’s 2023 Annual Conference ‘Long COVID, Navigating the Complexity, A Clinician’s Roadmap’.
Saturday 29th & Sunday 30th July 2023, Melbourne. Both face-to-face and online.
To get 25% off acnem Annual Conference USE CODE: acnem25
Over the years I’ve observed an increase in the incidence of practitioner paralysis. This occurs typically & understandably in the face of fearmongering. A good example is in the area of so-called ‘methylation medicine’ where we’ve been lead to believe that writing ‘the right’ nutritional prescription for patients requires a) their full gene profile, b) a knowledge of biochemistry that no one outside of a legit biochemist should have (!) and c) a bordering on perverse interest in in vitro research looking at how these pathways interact with different nutrients. And if we, as mere mortals (and naturopaths, nutritionists, herbalists or integrative pharmacists or GPs at that), are lacking in any of these WE WILL STUFF THIS UP GLOBALLY and put them on THE WRONG THING THAT WILL BE CATASROPH*C! Note: fearmongering always uses caps 😉
This stems from the misguided belief that ‘biochemistry alone maketh the man’ and ‘SNPs should write the ‘script!’
And the source of these falsisms are, what I refer to as, ‘Wallys with wall charts’. As impressed as we might be by individuals with brains for biochemistry or genetics, we should not let this overshadow the knowledge that health and disease are much more than 1 or 2 facets of your gene profile and how this may predict the pace of a few out of a million chemical reactions. Right? I mean I doubt any of us working in integrative health would intend to be so reductionistic and yet here we are with practitioners forgoing clinical (and RCT) evidence over that derived from in vitro with respect to supplements like SAMe and N-acetyl cystine, or worse still, taking as gospel, ideas that have come from pure hypotheses, based on 1 SNP out of an individual’s whole gene profile! This has infiltrated many areas of naturopathic and integrative medicine and certainly gotten the best of me at times too. But I am pushing back. Enough is enough. We humans are not our gene profile and holistic practitioners like us – know the manifold influences upon our health and wellbeing better than just about anyone else. And if you feel a bit lambasted by my little tirade – know that I have to give myself this very same talking- to every now and then – when I fall under the spell of Wallys and their wall charts!
In part one, we discovered the pro-drug nature of SAMe, revealing why evidence obtained from in vitro evidence can not be used to support either favourable claims or warnings. In the 2nd instalment we examined up close the misunderstandings about SAMe use in conjunction with antidepressants and clarified the real causes for concern in mental health clients. In this 3rd and final part we dissect claims and ideas about the success or safety of SAMe as a supplement with respect to methylation genetics and stages of pregnancy. All up this is indeed one BIG SAMe rethink that we reshape and re-inspire you about its prescription.
Recently a very experienced practitioner who uses SAMe frequently and successfully in her patients and also delivers education said to me, “I don’t know what I am doing wrong – practitioners still come back to me with cases where they’re throwing 8 different products at a patient to ‘lower histamine, improve mental health and support methylation’ instead of using just one – SAMe!” I laughed and said, whatever you’re doing WRONG in trying to teach people about SAMe I am doing WRONGER and for LONGER!! I’ve been trying to encourage and inspire confidence in prescribing SAMe for 2 decades now and still some of my most loyal listeners, are like, ‘I still haven’t prescribed it, I am too scared.’ 🤯
But I think the fear factor around SAMe occurs for several reasons: Misinformation – there is a LOT of misinformation about HOW SAMe works and WHAT kind of power it wields therapeutically Misunderstanding – this comes from a couple of key misunderstandings about drug interactions and SAMe pharmacokinetics & pharmacodynamics Mystery – even for me, SAMe has had an air of mystery about it, nagging, seemingly unanswerable questions that can undermine our confidence and certainty about its appropriate use and safety
I get it. And given the studies employing SAMe as a therapeutic agent date all the way back to the 1970s and continue to today – in psychiatry, hepatobiliary disease, cancer etc – there is a LOT of information that has been gathered overall and a LOT of old ideas/theories/speculation replaced by understanding thanks to better methods and models of scientific enquiry. So I decided it was time for me to confront this ‘man/molecule/medicine of mystery’ head on, conduct a completely updated literature review of SAMe and along the way – challenge many of my long held beliefs.
I thought about calling this latest episode, ’30 Things You Don’t Know About SAMe’ – and calling it like a horse race because in all honesty I learned THAT MUCH!
But I settled for: The Big SAMe Rethink – inspired by one of many pivotal papers which helped to revolutionise my understanding & approach to this nutraceutical which you can read yourself here. Misinformation, misunderstandings and mystery be gone (ok well most of it anyway!) – by filling in the gaps in our information that previously fuelled these – we can move forward with much greater confidence and clarity and we now know where the real safety concerns exist.
The Big SAMe Rethink Part1 Do you feel like you need to pick a SAMe side? Researchers and clinicians, alike, seem divided in their opinion about its therapeutic capacity and certainly its safety. One side are the ‘naysayers’: ‘SAMe can’t possibly be effective for both depression and in hepatobiliary conditions and and and’. Keeping them company are the ‘doomsayers’, preaching danger and destruction should we prescribe this ‘universal methyl donor’. But the other camp can seem just as fanatical and far-fetched at times: ‘it’s good for just about everything with zero safety concerns’. The divide and differences come down to origins of evidence and, once again, the truth lay somewhere in the middle. This new information on SAMe’s behaviour as a supplement will prompt you to rethink so much of what you thought you knew, whatever side you’re on!
I’ve been ruffling feathers over here while speaking at AIMA in Auckland. While I am pretty familiar and comfortable with that role (& responsibility?) – this topic ruffled my own, arguably the most. In fact, I kicked off the presentation with, ‘What I’m going to say might make some of you uncomfortable but you know what, it makes me uncomfortable and if it makes you think a little less of me, well, to be honest, contemplating these issues has already made me think less of me!”
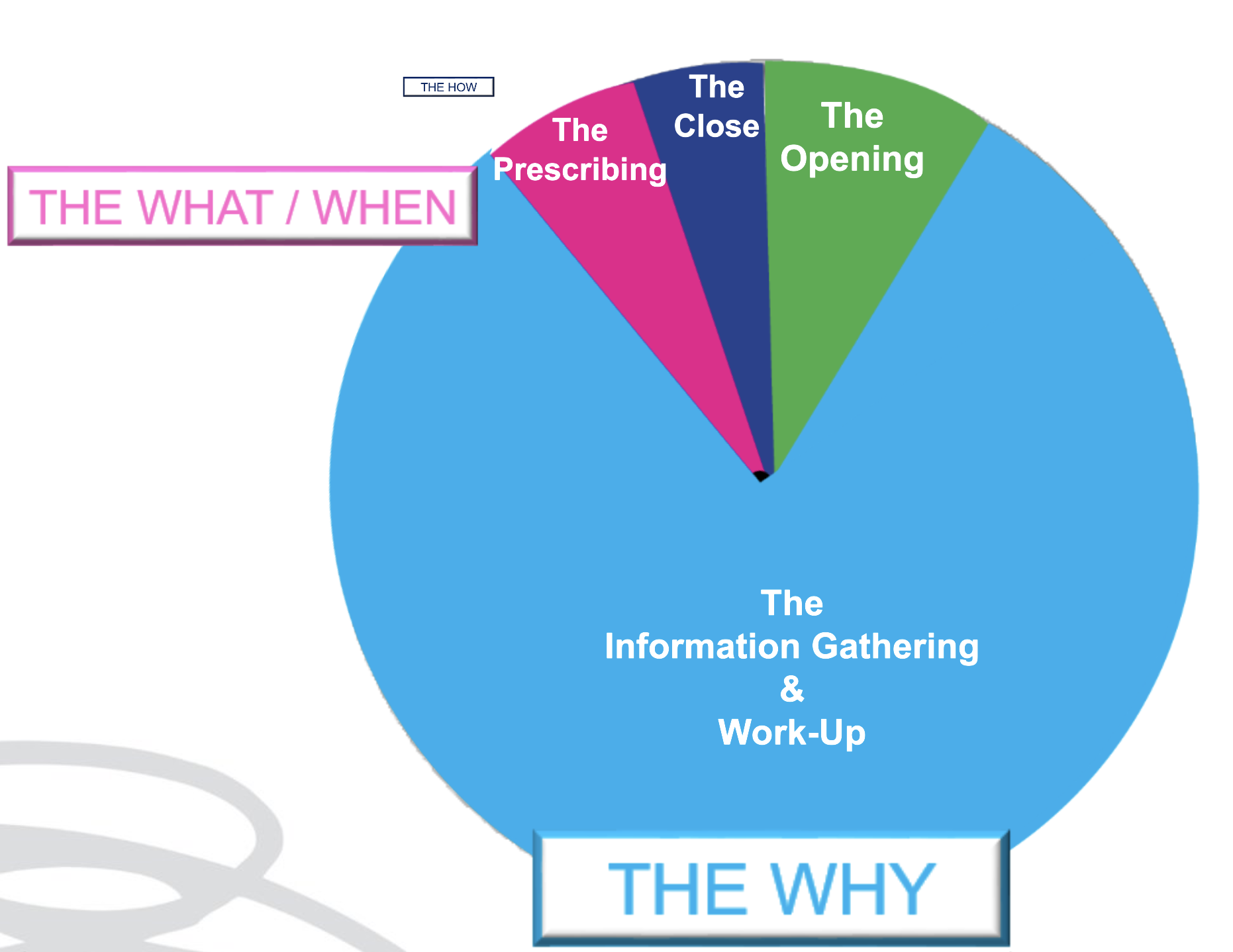
As an educator in integrative health, I have overwhelmingly been a peddler of knowledge and skills under the headings of: ‘WHY’ and‘WHAT’
Why – as in why does this patient present in this way, at this time. I am passionate about upskilling practitioners re our powerful contribution to the diagnostics & work-up of each individual. What – as in what changes (supps, herbs, diet etc) need to happen to correct for these very unique elements of imbalance in this patient to therefore aid resolution. We might label this, ‘personalised medicine’. But after so long in practice it’s patent that the best results don’t come from being the cleverest clinician nor the biggest biochemical brainiac. Knowing the ‘why’ and even the ‘what’, while enough for a minority of patients, fall short for the rest and can still fail to be truly about, & exclusively with, the most important person, in mind.
We’ve learned this before but it needs to be said again and again and again: much of any medicine is via the therapeutic relationship – and as part of this, our ability to PLACE the patient at the centre of their own SOLUTION. And therein lies the conversation we need to have in detail with them about the ‘HOW’ But how much time in your current consults is afforded to the ‘HOW’?
Being able to effectively negotiate with out patients the ‘HOW’ is an extension of Motivational Interviewing, Behaviour Change Theory & Patient Centred Care. It returns the humanity to our list of recommendations for each patient, pushing back against the autocracy that can tend to slip in with prescription writing. It powerfully reminds us that the prescription is only ever as good as the patient’s engagement & buy-in, and that’s only ever as good as our ability to write a prescription that is accessible & readily transplantable into their existing lives: to co-create with them Patient Centred Prescriptions. Someone in the audience had been my patient in the past – double awks right – because I absolutely know, I didn’t know this well enough back then. Back then when they were unable to do exactly as I had recommended – with their diet, their supps, their sleep, their work-life balance – they had, in turn, apologised for their ‘weakness’, ‘lack of willpower or diligence’ and me, being ever so gracious, accepted those apologies only to repeat the error of my ways and write yet more scripts that set them up to fail. 🤦♀️ I am committed to getting better at this and in this endeavour, giving both more attention & time in my appointments to the ‘HOW’ & yes I think we need to think creatively about how we use our appt time and between session touch points to achieve this – keen to hear about your perspective and experiences.
At the end of an information & insight heavy appointment, formulating a list of products and doses for our patients to take can feel like a bit of a ‘tada moment’, like a magician pulling a rabbit out of the hat. “Here is the solution – now off you go!” Research tells us, however, that treatment-plans that are a co-creation between you and your patient – evolving from a discussion that not only allows them a voice, but a major role in the decision making – are far more likely to succeed. While we are the authority on our medicines, our patients are the authority on what makes them tick & what’s likely to succeed, in terms of taste, texture, temperature & timing! This is called Patient Centred Prescribing and together with some other tips tricks and hacks I share with you in this episode, can really increase patient buy-in, compliance and therefore bring your treatment plan to fruition and fulfilment!
This is not about body shaming nor body positivity. I understand the crudeness of the body mass index, as a measure of (un)healthy weight – let alone (un)healthy muscle mass, so I don’t use this as a stand-alone assessment of weight, nor rigidly adhere to the categories it allocates individuals. With only minor recognised racial adjustments for BMI, I also recognise our concept of ‘healthy weight’ is incredibly whitewashed with minimal regard and consideration for clear ethnic and racial differences in physique. Patient’s lab results tell the real story. It’s in their results that we can discover someone is thin-on-the-outside-fat-on-the-inside (TOFI) or FOTI. These are patients whose BMI, WC,WHR, Body fat% etc identify them as obese – yet there is not a whisper of what I call ‘Adiposity Patterns’: no subclinical inflammation, no reduced glucose tolerance or actual IR, no raised transaminases that we expect to correlate with girth and the corresponding fatty infiltration of their liver. In this, as in so many other aspects of clinical practice, we are reminded to see each individual, individually.
AND if we adhered to this always, listening unfiltered to the whole health story and letting the labs speak, we would not miss those patients in whom unhealthy weight really is the most important underpinning, & all impacting, issue. And we are not doing our job, when we don’t.
I mean – we all know the detrimental effects of excessive adiposity – that’s like Pathology Unit 1 topic 1, right? I know we know it. Yet there are so many reasons why we might down-play, step-around, or even ignore its enormous contribution in our patient work-up and certainly the discussion that follows with our patients. That too is a no-brainer. Who wants to say to someone whose come seeking your help, as an explanation for their complex health concerns, ‘There’s no zebras here just a horse – one really over-weight horse!’ Knowing too that unhealthy weight results from the most complex constellation of factors (biopsychosocial) unique to each individual and that change in this health determinant, is arguably the slowest and hardest to sustain. But how are we serving our patients if we don’t?.
A practitioner presented this case of a 48yo F seeking help with the work-up: Self-reported inability to lose weight after 1st pregnancy = ‘obesity’ ongoing – now BMI 33.1 –> 25yo Reflux & Hiatus hernia Tx Omeprazole initiated – ongoing –> 26yo Depression Tx Venlafaxine initiated – ongoing –> 30s Back and other musculoskeletal injuries Tx Surgery & Opiates – ongoing –> 40s Hypertension & elevated resting HR –> Last 12mo – changes in Mx cycles suggestive of perimenopause & substantial weight gain
This patient didn’t ‘have’ any lab results but I think I can make an educated guess about how they would look and in particular whether they show the characteristic ‘adiposity patterns’ I mentioned before. What was my first thought about the most impactful element of the case? Obesity. What was my second thought? Where is all the weight (diet & intervention) history that would help us to understand how she is where she is, right now? We didn’t have any. The practitioner informed me that the patient was ‘not very interested in talking about her weight’ – in fact, according to her, it didn’t seem like losing weight was one of her goals. Now this could be several things: the fear of judgement, even her own self-loathing, the paralysing awareness of the enormity of such a goal, the dashed hopes of the past, or it could just be that her weight, as the key negative determinant of the majority of her health concerns & quality of life, has just never been brought to her attention, nor the connections explained to her in simple accessible language. So over to us, right?
There were other health determinants at play in this patient but the centrality of the adiposity was undeniable & the practitioner said this was the greatest take-home. She’d been ready to don some jungle gear and go hunting some zebras – but there was a horse right here in front of her and that could not and should not, ever be ignored.
What else became apparent was the lack of knowledge & skills regarding how to take a comprehensive weight history & why this is crucial. Not only for this type of unhealthy weight, the underweight require exquisite attention, as do those with a more labile weight than expected as an adult. This brilliant article by Kushner et al from 2020 is a total gift in that regard and a must-read for every clinician. We feel uncomfortable asking about certain things when a) a patient feels uncomfortable which is usually because b) we are uncomfortable and this ultimately comes from not being clear about WHY this information is so important and HOW this will ultimately enable us to better help THEM.
This is the very latest, comprehensive review of the key aspects of thyroid assessment that will revolutionise your understanding of thyroid markers. Gain a clear understanding of how to provide the best, most individualised, thyroid management by learning to read the real story in each patient’s pathology patterns. Boost your knowledge and confidence looking at TFTs, rT3, thyroid antibodies & related nutrient patterns, as well as AITD, environmental EDCs, HPA driven HPT issues, thyroid nodules, the impact of dietary macro- & micro-nutrient imbalances and much more!
This 4 part series provides over 10 hours of the very latest research & findings, punctuated with real case studies, that will both contemporise and deepen your understanding of all things thyroid, with a bonus recording on Adrenal Assessment.
Gone are the days, thankfully, when we could all easily identify any individual taking an antipsychotic 1) because they were the marginalised ‘mad’ and 2) stigma and shame were rife. With the seismic shift that has occurred both in psychiatry & society we now know so many of the people we live or work with just might be taking ‘something’ & under any number of diagnostic labels. And increasingly the ‘anti-psychotics’ are not reserved for the psychotic nor the ‘mood stabilisers’ for the manic. Which can complicate things – especially when it comes to their thyroid.
You see it’s a mistake to think that only Lithium spells trouble for thyroid function
The latest piece of evidence from a study of over 25K BPAD patients in the US tells us this common misunderstanding makes us prone to not recognise all the other patients in whom their psych meds are disrupting and in fact driving thyroid (dys)function. Though Lithium carbonate remains the most noxious goitrogen due to its multiple disruptive mechanisms – the rest of a large group of Psych meds (yes even antidepressants!) are impacting to the point of effecting the thyroid function test results you are likely to see in patients taking these. And this is something we need to be alert to – these medications are essential, non-negotiable in most scenarios, but a secondary hypothyroidism is not their intended goal and can make matters worse.
Cue our growing understand of psychoneuroendocrinology, of course. Your HPT is influenced by your mood & vice versa
I told you I’ve rekindled my love and passion for thyroid pathology and this is one of the many elements I got to include in our latest updated training * Advanced Thyroid Assessment* and the upcoming MasterCourse. But I just had to hit record on this one aspect immediately – because if we don’t recognise the cause we are likely to be throwing all the wrong things at the thyroid – to no avail. This kind of subclinical or overt hypothyroidism is not due to nutrition per se, or due to some other kind of HPT re-setting influence like inflammation…it’s the meds & that necessitates different solutions & a much bigger conversation…so join me…
Many of us recognise the bidirectionality between thyroid function and psychiatry wherein ‘stress’ and mental illness can produce a predictable pattern and shift in TFTs and vice versa but regarding the question of psych meds as potential goitrogens, many of us are mistaken in thinking this issue begins and ends with the use of Lithium carbonate. As it turns out, an increasing number of these pharmaceuticals are recognised to disrupt thyroid health & activity via a variety of mechanisms both centrally and peripherally & as a result many patients may get stuck in a vicious loop of worsening thyroid function and mental wellbeing. – until someone calls it – someone like us.
Any pathology test is only of value if the result produced is ‘real’, or, representative of that individual, right? So the timing of the test is a major pivot point then: do I tell my patient to present for the test, or collect the sample themselves, on their ‘best’, their ‘worst’ or their ‘average’ day? 🤷♀️ Well, that all depends on the question you are trying to answer.
Whenever we reach or refer for a test, we have a question in mind we’re seeking an answer to. But the question always comes in two parts, at least.
Part 1: How much progesterone is she making? Part 2: …When she’s ovulated & her corpus luteum should be most productive?
A third might refine the question you’re answering further by adding another contextual clarification
Part 3,4,5: …When she’s eating her regular diet, not exercising excessively or under extreme stress
Without these other parts – the answer to the first one: How much progesterone is she making (full stop), is hard to correctly interpret, right? By refining and expanding on the full extent of our question, we can be clear about which elements of this patient’s life the result likely reflects. We might say that for her, this time-point, or set of collection conditions, is a ‘real reflection’ of her generally and therefore, representative. But what if she does occasionally undertake a 5 day fast, or train for & compete in marathons? If we were to specifically test during these times, we answer a different question, right? Likewise every time we instruct a patient to present for their blood tests (routine or fancy schmancy): Fasted, Rested, Hydrated and off their supplements – is this sound advice or a misdirection? Well it depends on the individual in front of you and the real question you want answered about them 🤓
Ahhhhh I love rules: both the making of them and the subsequent breaking of them 🦜🏴☠️
The collection conditions for any pathology test – can refine or ruin the question you were hoping to have answered about your patient but is it always appropriate to ask everyone to ensure their preparation for the test was ‘ideal’? What if their real life is far from ‘ideal’ and contrasts dramatically with these ‘conditions’ e.g. they forget to drink water but never alcohol! Or do they run 20km every weekday and 40 on weekends? And why would we tell some patients to stop their supplements prior to a blood-test and not others? If our goal is to ensure any pathology test answers the question we need answered we need to know how to respond to these and other scenarios. This new update is all about keeping results ‘real’ & representative.
You can purchase Fasted, Rested, Hydrated & Unsupplemented? Exceptions to the Rulehere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
Are we doing ourselves out of a job? I’ve been talking treatment plans with my New Grads recently. Given, only recently these were major assessment items in their clinic units, they have been trained to create ALL-ENCOMPASSING (biopsychosocial) prescriptions and recommendations of utterly EPIC PROPORTIONS – to simply prove they know it all. Problem is this doesn’t work in the real world.
Emailing your client multiple pages of advice that covers: a whole sizeable supplement schedule that only a military-training could nail (2 tablets 1 XTID 1 X BID, a liquid, a powder, some with food, some definitely not with food) plus dietary advice, plus hyperlinks to exercise advice, mindfulness exercises and a request for follow up investigations before the next appointment…is…a L*O*T!!
It is also ineffectual – because it completely disregards the human on the other end. Let me ask you this, how much change are you capable of between a first and second appointment, roughly a period of 2-3 weeks? Personally, I gotta say not that much. It took my dentist years to get me just embrace flossing & I don’t think I am an exception! With all the knowledge we possess its hard not to see people as (a long list of) problems (& problematic behaviours) that we translate into, and solve via, a prescription.
Effectively we are saying to patients with this practice model, ‘Go change & come back when you’re done & then I’ll probably ask you to change some more!’ That’s both a big ask and a huge missed opportunity.
I hear from reliable sources over the ditch, that GPs are increasingly referring their patients to, or teaming up with health coaches, rather than naturopaths. Given what I’m observing, I get it. Doctors on the whole only have time (and barely then) for a finger-pointing prescription – certainly not the time and touch-points required to actually support patients with the very difficult thing that is, behaviour change. Nor the skills to truly facilitate patients making the necessary and desired changes – so they outsource this role. But we shouldn’t.
After all – I want to be on my patients’ support bench & health care team always – not a flash in the pan, that blinded them with science or my ‘smarts’ and proved to them in one over-stretching prescription – that naturopathy is not for them, or at least, they’re not fit for the task.
At the end of an information & insight heavy appointment, formulating a list of products and doses for our patients to take can feel like a bit of a ‘tada moment’, like a magician pulling a rabbit out of the hat. “Here is the solution – now off you go!” Research tells us, however, that treatment-plans that are a co-creation between you and your patient – evolving from a discussion that not only allows them a voice, but a major role in the decision making – are far more likely to succeed. While we are the authority on our medicines, our patients are the authority on what makes them tick & what’s likely to succeed, in terms of taste, texture, temperature & timing! This is called Patient Centred Prescribing and together with some other tips tricks and hacks I share with you in this episode, can really increase patient buy-in, compliance and therefore bring your treatment plan to fruition and fulfilment!
Have you ever noticed that our products don’t work if our patients don’t take them?!🙄
The reasons for non-compliance, dis- or non-engagement, poor patient buy-in & follow through are many:
*My dog ate the instructions * My inbox swallowed the instructions *As soon as I left your clinic, your instructions left my brain
Reasons also include far more credible things such as non-patient centred prescribing. This is what most of us do when we’re full of good intentions but short on time at the end of a consult, so we just throw a bunch of products and a script with them out the door. Arguably many of us make this mistake also because our training perpetuated this relic of conventional medicine and paid insufficient attention to the therapeutic relationship. In contrast, patient centred prescribing recognises the patient as best-placed to find personalised solutions to their very individual challenges, including, decision making around dosing regimes. So while we continue to ensure & oversee that therapeutic doses are used and that best conditions for taking certain things are adhered to – your patient remains the expert in the room about how to actually achieve this – both in terms of when & where in their very real lives – with a little help from us – and what ‘works for them’, in terms of taste, texture & temperature.
That’s right, I said temperature…are you telling patients to take everything at room temperature??
You need to think again – this is something we can safely manipulate with many powdered & liquid remedies (some exceptions of course!) to match patient preferences & radically increase palatability, pleasure and ultimately patient compliance.
Are you like me? I have supplements scattered all over my house – in places that correlate with an action or moment in the day when I am most likely to take them. This is another important element of Patient Centred prescribing, so I work with my patients to identify these easy solutions too. After the gym? In the gym bag. After breakfast as you leave for work? In the key bowl. At work? On the desk beside the computer screen. Keeping taurine in the drinks cupboard in front of the alcohol is another nifty reminder and trick for those looking to ‘pre-load’ and cut down! Tips and tricks like these save our over-loaded memory. They remove or minimise barriers. They make compliance less effortful. And as a result, you know what? They might just get the results we would have expected!
Compliance Changers – Strategies for Success
At the end of an information & insight heavy appointment, formulating a list of products and doses for our patients to take can feel like a bit of a ‘tada moment’, like a magician pulling a rabbit out of the hat. “Here is the solution – now off you go!” Research tells us, however, that treatment-plans that are a co-creation between you and your patient – evolving from a discussion that not only allows them a voice, but a major role in the decision making – are far more likely to succeed. While we are the authority on our medicines, our patients are the authority on what makes them tick & what’s likely to succeed, in terms of taste, texture, temperature & timing! This is called Patient Centred Prescribing and together with some other tips tricks and hacks I share with you in this episode, can really increase patient buy-in, compliance and therefore bring your treatment plan to fruition and fulfilment!
You can purchase Compliance Changers – Strategies for Successhere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
Last week, yet another patient with refractory diarrhoea, up to 10 stools a day, Bristol type 5-7, for 3 decades following a diagnosis of Crohn’s at 16 years old. A range of specialists have thrown everything at ‘it’ – single & combination immunosuppressants, TNF alpha blockers, buckets of sulfasalazine and bathtubs of antibiotics – she’s been gluten and dairy free for years, trialled strict diets that are FODMAPs free, low histamine etc etc etc. She’s even had 50cm of her terminal ileum removed & the diarrhoea continues unabated – perhaps even worse than before…& therein lies a major clue.
1/2 patients with Crohn’s exhibit bile acid malabsorption –> diarrhoea but with terminal ileum resection this jumps to > 90%
This is Type I BAD (Bile Acid Diarrhoea) & is the easiest to spot, being the result of anatomical change. You remove the section of the small intestines responsible for 95% of the reabsorption of bile acids…a LOT of bile acids are going to be present in the colon where they act as potent osmotic laxatives, right? But there are 3 other types which are a little trickier to identify – including one that affects up to 50% of IBS-D patients.
Being a child of the 80s⚡🎹 (ok a teen of the 80s but who’s counting?!) and a personal fan of fat, I NEVER thought I would EVER be recommending a ‘low fat’ diet to ANYONE🤐
But hey, that’s another ‘absolute’ that needs challenging, right? I mean this is the primary, almost only, dietary change these patients need to make and as a stand-alone intervention, is highly effective for many. We’ve had several patient successes in the last year – a total game-changer for patients in similar situations where all kinds of ‘restriction’ had brought zero joy and reward for all their ‘good (dietary) behaviour’. While sequestrants (like cholestyramine) are recommended in BAD, and are certainly worth a trial at least, patients have very mixed results – for some, in combination with the low fat diet it’s a winner – for others these meds cause GIT upset all on their own and actually undo the good of the fat restriction. Being able to identify the true reason for their loose stools and stop them going down endless rabbit holes of ..is it? is it? is a great way to re-empower people who’ve been bossed and bullied by their bowel for far too long 🤓💪🧻
This is not a trick question. Up to 50% of all patients diagnosed with IBS-D actually have bile acid diarrhoea (BAD) underpinning their digestive complaints as well as some patients with non-resolving diarrhoea post-cholecystectomy and gastro. Knowing which ones do and how to manage this, which requires distinctly different approaches from our general management of IBS, is the key. As always, good lessons come from those we learn in the clinic and this story starts with a patient and how we came to recognise the BAD in her belly.
Did I say, ‘Our Brain’? 🙄 Maybe it really should be, ‘Their Brain…on Drugs: what recreational substances reveal’. While infinite self-analysis is an occupational hazard for health professionals, when we use our detective powers for good not evil, our patient work-up benefits. But of course, it is impossible (and not desirable) to avoid all self-reflection. Let me introduce myself: I am a high dopamine gal. How do I know? Because a valid accurate test of my neurotransmitters told so? Heck no – outside of lumbar puncture there isn’t one! Because my reactions to recreational drugs did.
A self-proclaimed ‘cheap date’, with amplified & protracted intoxication experiences from small amounts of any psychoactive & no, sadly, not always pleasant. I specialise in visual trails, a known trademark of dopamine surges, when under the influence of even just a few drinks – much to the bewilderment of my loved ones.
Some even famously once questioned whether I was, in fact, safe to ride a push-bike 500m on Lord Howe Island after 2 glasses of prosecco. Stop! I heard that murmur, this has nothing to do with my liver & its handling of such substances. [How rude!😆] I can cite ample other evidence in support of this. This is also not simply due to being a teetotaller and therefore having not (yet) developed tolerance. This high dopamine diva-stuff is echoed by my non-intoxicated ‘normal’: vivid dreaming, impulsivity, and bankable bad reactions to Vitex: ANGER (capitals intended). TMI? 🙄🤐
When you know the questions to ask, the answers to lean in further to, and then the way it can all come together, to create a neat little trail of breadcrumbs we can follow all the way to our their neurochemistry…you can find the gold.
The thing is – and I remain annoyed and frustrated by this to this day – our ‘schooling’ was not very ‘sex, drugs and rock’n’roll’. New grads tell me nothing has changed. In fact, these kind of topics were absolutely omitted, in spite of the claim we consider the ‘whole patient’, the whole health story! Interesting, hey? Nod to those working on the ‘sex’ bit in holistic health: Moira Bradfield-Strydom, Sage King, Monica Francia, Daniel Robson…love ya work! Now for the drugs! Do you know what recreational substances can reveal about your patients’ neurochemistry?
Finding out about your patient’s historical or current psychoactive appetites and adventures (and yes that could be as commonplace as alcohol), is not purely for the purpose of collecting yet more data on their ‘health behaviours’. Nor yet another cue for casting judgement! It is an opportunity to take a can-opener to their cranium, open that baby up & take a look inside. Without making a single incision!
But there’s a bunch of background knowledge you need to polish up on re psychoactive MoA and what each part of your patients’ experience (1st vs subsequent exposures, threshold for intoxication, the nature of the intoxication itself, & the possible aftermath) can reveal – as an inventory of their CNS materials and machinery. All the while having a process to follow to ensure your evidence is leading you to the right and reasonable conclusion. Come with me and let’s follow the trail of breadcrumbs your patients recreational substance experiences have laid out for you…🐓
Our Brain On Drugs – What Recreational Substances Reveal Part 1
Ever wondered why not everyone loves MDMA given it’s the ultimate love drug? Or why some of your clients are exquisitely sensitive to the aftermath of psychoactives and routinely, reliably experience ‘rebound’, in the following days while others ‘bounce’ seamlessly from a big night into the boardroom the very next morning? What do these things tell you about the state of play of their neurotransmitters & their neurochemistry? So much more than you expect and given the only validated accurate assessment of an individual’s neurotransmitters is via lumbar puncture…with far less pain and inconvenience. This is the first of a 2 part discussion.
&
Our Brain On Drugs – What Recreational Substances Reveal Part 1 Part 2
The 2nd part of this discussion goes into the detail of the MoA of each recreational drug class and what our patients’ encounters with these reveal about their neurochemistry. It also includes a resource we’ve developed to help you follow a process, in your review and rate the quality of evidence you have, to ensure your extrapolation and interpretation are well-founded. **WARNING OVERSIZE LOAD AHEAD** There is a bonus case discussion that puts into action everything outlined in both parts and the process of qualifying the evidence.
You can purchase individually Our Brain on Drugs – What Recreational Substances Reveal Part 1here and Part 2 here
or become an Update in Under 30 Subscriber to access both episodes plus the entire library (100+ episodes) of Update in Under 30 audio’s and resources here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
And health, no matter which side you sit on, seems to be particularly plagued by them. I (incorrectly) recall my 4 year degree as being a series of deep personal losses, some favourite food, then caffeine, then alcohol etc etc.😂 Likewise, I’m aware that naturopathy & integrative health’s ‘voice’ in the ‘conversation’, could arguably be perceived as mostly a negative one – as in, ‘No. Never. Not good. No, not even a little bit?!’ But I love both playing devil’s advocate & reading the research (ALL the research – even the stuff that doesn’t support my views and position GASP!~) so I am less in favour of absolutisms. This came up recently when I suggested alcohol may improve iron uptake 😬
Practitioners’ responses were 1 of 2 types: humorous dismissal (“steak & beer for breakfast – at last a naturopathic prescription I can support!”) or horror. But why are we so attached to the absolutes in spite of contradictory evidence?
Let me ask you this: is coffee bad? Full stop? Period? The end? Or is it the most concentrated source of antioxidants consumed in the average Western diet? Does it improve bile flow, peristalsis and at higher levels actually protect the liver against damage? Clearly, we need to read all the evidence, including, the favourable and make individual decisions about ‘what serves and what sabotages’, for each patient. But do we? Or do we imagine we only get membership to the ‘Ultimate Integrative Health-club’ when we adhere to blanket bans?
Similarly I, like many of you, see a LOT of iron deficient women – & a fair chunk of these have been incorrectly labelled, ‘refractory’ because theconventional correction strategies (high doses everyday) don’t actually make sense. But like you guys too, I’m always on the hunt for new ways to improve iron absorption in these women, so I can hit them & their gut with less. That’s why I shared the research regarding alternate day dosing, and taking a supplement within an hour of exercise and now, I dare to ask if a tipple could be helpful?
While we know that both ‘GOOD’ (exercise) & ‘BAD’ (alcohol) health behaviours increase gut permeability, which sounds ‘BAD’, right?
But could this be ‘GOOD’ for some?
This has certainly been demonstrated in relation to exercise & iron but most of the research investigating how alcohol intake effects iron uptake and status is based on alcohol abuse. The study below, however, based on a large sample of non, mild, moderate & heavy drinkers captured in NHANES data – is a very well written and reasoned article, such that it can exclude liver damage, inflammation and HFE mutations as other explanations for the better iron status, in drinkers. And it found:
I challenge you to read it for yourself and challenge your absolutes!🤓
Oh and just in case you’re thinking, “Have we all misdiagnosed iron deficiency and it’s actually a Copper deficiency underneath?”because last year the fashion was everyone was copper toxic and now this year someone’s making noise saying everyone is copper deficient !!! (Absolute? Anyone?!) Ah, no. Copper deficiency, as a cause of iron deficiency and anaemia, has been around for about as long as nutritional medicine itself. It is absolutely a thing. But in the absolute minority of people. And if you go back to some basic maths & compare and contrast Fe & Cu at each level: 1) requirements almost 20mg Vs < 2mg 2) average intake (inadequate Vs adequate) 3) bioavailability (Fe < 20% more typically < 10% in a modern low meat diet Vs Cu is typically >50% ) and do some basic sums I call, ‘Menstrual Maths’ – You’ll likely deduce that inadequate iron intake and uptake, given our losses, is in fact the common culprit and a ‘coldie’ may be more beneficial than copper in most! Can y’all stop asking me about that now – pretty please?
And then you don’t. The reality is we all struggle at times with correcting low ferritin or iron deficiency anaemia – so what have we got wrong? In spite of being the most common nutritional deficiency worldwide, the traditional treatment approaches to supplementation have been rudimentary, falling under the hit hard and heavy model e.g. 70mg TIDS, and are relatively unconvincing in terms of success. New research into iron homeostasis has revealed why these prescriptions are all wrong and what even us low-dosers need to do, to get it more right, more often!
Did you know you can subscribe to these? We deliver at the end of each month, just add a 12-month subscription to your cart and Rachel’s latest research is on it’s way to you!
“My 7yo daughter was frequently distressed, telling me she had that ‘throat feeling’.”
As you can imagine, mum offered up a smorgasbord of suggestions to help her try and describe it: Can you swallow ok? Does it burn or taste funny? Where is it? Is it hard, soft, moving, give me a rating out of ten….so many, but she just couldn’t. When it was really bad, her daughter said she also felt it in her sternum. The first doctor attributed it to ‘stress’ & mum understood why. Her 7yo is a bit of a worrier and while the ‘throat feeling’ was distressing, stress, itself, seemed to also perhaps bring this on. But by the time they made an appointment with their regular family GP, mum had noticed her daughter’s sx were worse with heavy, fatty, high meat meals & that she was burping excessively especially with the night time meal also. So, when their switched-on doctor heard these very careful observations, he referred her for a urea breath test (UBT) for H.pylori.
‘Miss 7’ blew 1200 on the UBT the decision limit is 200, to confirm the presence of the bacteria in significant amounts
As I’ve said previously, there are (sadly for ‘Miss 7’ & myself) no prizes for the highest score on this particular test. In fact, I spoke with a gastroenterologist last week who said, really it remains so debateable about the significance of the overall result (?size or virulence of colony) that results should probably be more considered like a pregnancy test: a simple yes or no! But this together with her sx was a clear yes. GP recommended triple antibiotic therapy which sadly produced vomiting in Ms 7 within a few days. GP contacted paediatric gastroenterologists to get some advice, which was: don’t treat unless symptomatic. Back to square 1.
“In the meantime, I had done Rachel’s two UU30 episodes on H.pylori, so I told him what ‘we’ would do (polyphenols plus cranberry juice plus Zn carnosine plus deal with the hypochlorhydria). GP says. “Ok, then let’s do it and then let’s breath test again in 3-6 months.
She has now breath tested at 200 and symptoms are non existent!”
Mum contacts me to relay the success story & give me the credit but mum is completely minimising her extraordinary actions that produced this outcome. Firstly, not resting with the ‘stress’ diagnosis. I have seen several children who present in very similar ways to Miss 7, YES! they are anxious, YES! parents might tell you they are the ‘worrying-type’ but when combined with these upper GIT sx I have found they test positive for H pylori more often than they don’t. And how clever is this mother’s medicine?
“I recognised it was worst after birthday parties where she has eaten too much and done cartwheels or run around (we now talk about recognising when she has a ‘full bucket’. We talk about the fact that her tummy takes a little bit more time to process food it means her bucket fills and she needs a bit of extra time to let it do it’s job before she adds more food to the bucket otherwise it spills over and she feels rubbish. She finds that analogy useful as she can feel her bucket getting full at birthday parties and when she gets the feeling, she knows why and doesn’t freak out.”
H.pylori – Eradicate or Rehabilitate? For a bacteria identified just a few decades ago as being a cause of chronic gastritis, atrophic gastritis and gastric carcinoma, the escalation in the number of antibiotics used to eradicate it (4 at last count + PPI) has been nothing short of breath-taking. A management approach more consistent with both integrative medicine and with an improved understanding of the delicate microbiome focuses on changing the gastric environment to ‘remove the welcome mat’. What do we know about how to do this successfully? It turns out…quite a lot.
When was the last time you ‘got on the gear?’. Wait, am I showing my age?🙄 The afore mentioned ‘gear’ could be beers or GnTs, weed or hooch, eccies or pingers, ‘nose candy’ or blow. I could keep going! While, anything beyond alcohol, might be purely a historical tale for many of us – during a [ahem] ‘very different phase of our lives’, Australian research tells us that the patients who come to see naturopaths are just as likely to drink alcohol as those that don’t and are in fact about 40% more likely, to have used marijuana or other illicit drugs in the past 12mo. And this was the women in their 30s! You heard me.
Now, this is not a call to action, to dob in a dabbler.
This is instead a wake-up call for all of us, regarding the best insight into our patient’s neurochemistry, that is right there in the patient’s psychoactive substance encounters.
Because let’s get 1 thing clear, straight up – the ONLY valid, accurate, reliable pathology test for the measurement of neurotransmitters is a lumbar puncture. Correct. And anyway, if you’ve been following psychiatric research this millennium, you’ll know that the belief that neurotransmitter quantities are the whole story (or even main players) in neurochemistry, is fatally flawed. So, whether your patient’s ‘alcohol or other’ is purely in the past or in the present, this line of questioning and what it can reveal to you about their neurochemical nuances (high or low dopaminergic tone, shortfall in serotonin, high or low histamine etc) is gold.
Because no recreational substance BYO
Instead they raid your stocks and supplies, get your brain to develop ‘bigger ears’ for some signals over others. Their effects are purely a manipulation of the patient’s existing materials and machinery. And accordingly, here is the great reveal. So, a 30 something patient of mine reports dabbling in all sorts during her teens and twenties. She relays pretty ‘expected experiences’ with each substance – remember these psychoactives are known quantities, we know a lot about which buttons they push and I so I concur that her responses were anticipated & typical. Maybe if anything, she is able to recognise that she had a lower threshold for intoxication compared with other first time users. “But MDMA,” she says, “I don’t get it and boy I tried! Several times!” So, while everyone else felt the love in the room, danced all night to the fantazzmical beats and the orgasmic-optic light show…she felt like she’d taken nothing at all. Aha! This of course would prompt me to ask more questions to help clarify both her serotonergic tone & other instances where she might have encountered oxytocin. And the real insights about her neurochemical milieu (strengths, weaknesses, balance and imbalance) start to form, so too the best way to support her. Don’t miss the real reveal in your patient’s story – that offers to lift the lid on their cranium and let you take a look inside.
Our Brain on Drugs – What Recreational Substances Reveal Pt 1
Ever wondered why not everyone loves MDMA given it’s the ultimate love drug? Or why some of your clients are exquisitely sensitive to the aftermath of psychoactives and routinely, reliably experience ‘rebound’, in the following days while others ‘bounce’ seamlessly from a big night into the boardroom the very next morning? What do these things tell you about the state of play of their neurotransmitters & their neurochemistry? So much more than you expect and given the only validated accurate assessment of an individual’s neurotransmitters is via lumbar puncture…with far less pain and inconvenience. This is the first of a 2 part discussion.
You can purchase Our Brain on Drugs – What Recreational Substances Reveal Pt 1here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
There’s probably some poignant lines from a rap song everyone knows that I could insert here but, alas, Gold FM doesn’t play anything produced after 1999, so I’m none the wiser. What I’m trying to bring to mind, is the potential clash between our reality & our response: we’re not all gonna get instafamous, so the majority of us should probably curb the buy-now-pay-later spending and establish some contingency plans. And while it might seem like I’m just picking on the young folk, this can happen at any age and stage of life. These, in psycho-speak are called Positive Illusions, and are one of the concerns psychologists have about the potential impact of exclusively focussing on ‘the positives’, aka Positive Psychology (PP).
There’s a lot to like about this Gen Z offspring of psychology. And perhaps, as integrative health professionals, a ready-made romance, given both tribes (them & us) believe in health being something beyond the mere absence of disease. That and the fact they give due recognition to the role diet & exercise play in our mental wellbeing…how truly thrilling! Over the last 20 years PPIs (Positive Psychology Interventions not the other ones!) have become so pervasive: schools, workplaces, we’re in an age of the National Happiness Index, we’re overflowing with positivity, spilling over the lip of your coffee mug, emblazoned with ‘You’re Awesome!’ or ‘You’ve Got This!'(Just in case we forget momentarily) But we need to explore the science for and against, to better discern when these messages and tools are a help in clinic and in our patients, and when potentially a hindrance, worse still, a harm.
😁POSITIVITY😁
is extremely popular right now, but an obsession with it & rejection of all things negative (thoughts, feelings, experiences pasted over by something nicer and brighter!) is not necessarily a balanced recipe for mental wellbeing, according to the science.
PP has made a wonderful contribution to how we think and talk about our mental wellness as opposed to just our mental illness. However, there is a critical context in here that’s important for clinicians to understand, in order to use it well, and some thought-provoking criticisms and counter-balances that will help us all avoid becoming as (in)effective as a slogan on a coffee mug. Oh and guess what guys? Assessment first 🤓💪 this takes the guess work out of whether your patient is a good candidate for PPIs and we’ve included two in this latest Update in Under 30 – even a validated mental health screen that only uses positive language for those averse to those nasty negative thoughts and feelings!
UU30 Positive Psychology Its likability & limits
The ideas behind Positive Psychology may resonate deeply with integrative health professionals, for good reason. We have in common a belief that ‘the absence of disease’ does not constitute health & that prevention is better than cure. And PPIs have become so popularised they have permeated into schools, workplaces and most people’s therapeutic interactions, e.g. gratitude exercises, identifying our strengths via a strengths wheel, self-compassion. But do we know the limits of positive psychology? Do we know who it works for and what it means when it ‘doesn’t deliver’ mental wellness?
You can purchase Positive Psychology Its likability & limitshere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
And not in a good way, right. While we’ve known about the potential for peripheral neuropathy with excess B6 supplementation since the 1980s, currently there’s a seismic shift in our sense of safety even with previously regarded ‘safe’ levels. You may have heard individual whispers, or the chorus of voices coming together, both here and overseas, belonging to members of the public who report suffering sensory nerve impairment with as little as 2mg/d! Is this a mess of mis-diagnosis, false attribution & nocebo? Perhaps for some, but certainly not for all.
How could this be the case given the many RCTs employing hundreds of mgs per day over months, with no such events recorded? How could this be given, your (?), certainly my, high dose prescriptions, with only 1 case of quickly reversed, peripheral neuropathy in over 20 years, on my books? The pieces of this complex paradoxical pyridoxine puzzle are coming to light.
Is it the form?, the dose? the duration? individual differences in B6 metabolism & toxicity threshold? amplification of risk secondary to levels of other nutrients, or the use of certain medications? Yes. And we need to understand each element to better tailor every B6 prescription to the individual & mitigate risk. I have spent the best part of this month reading almost every paper on this from the 1970s to last month and I am now alarmed but more importantly, alert, to what prescription practice changes we can all make to lessen the risk, and control the power of B6. It’s been the most compelling deep-dive. Because in spite of a clear TGA warning issued last year that likely prompted the quiet removal of high dose products from market, it would seem none of the companies have the courage to have this difficult conversation with us 🙁 I invite you to ‘feel the fear & do it anyway’ & listen in to our latest Update in Under 30.
Haven’t we always known that nutritional medicine is a potent prescription? Now thanks to more sophisticated research we have a much greater understanding of this and of both the intended and unintended effects of micronutrient supplements that have the potential to achieve supra-physiological levels. B6 metabolism is arguably the most complex of the Bs – involving 6 different forms, at least 2 of which are active – and exhibiting some of the most complicated regulatory control designed to both harness the power & limit the accompanying risks. Excess B6 supplementation, however, has long been known to present as peripheral neuropathy in some individuals and case reports of this are growing, at lower and lower doses. New information has come to light to help us understand the why, the how and better still how to mitigate risk to our patients.
You can purchase Dynamics and Dangers of B6 – Controlling the Powerhere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
I’m 100% confident that, as a professional group, among our highest values about healthy, preferable, food choices, would be characteristics like: ‘as close to nature as possible’, ‘unrefined’, ‘unprocessed’, ‘unadulterated’. Tell me I’m wrong.
So, when I keep hearing about NEW! “Never seen before” (read: never in nature) modified (read: more processed, adulterated) nutritional supplements: water soluble vitamin D, fat soluble C, bioflavonoids with unprecedented (read unnatural) bioavailability
I’m left wondering what these companies are missing about their customer group (because we are clear about our valuing of nature & what’s natural & have a desire to minimise exposures to things that are not, right?
or what are we missing here, in the clear conflict of our core values these constitute?
I think if we find ourselves forsaking this core value & prescribing highly modified, unnatural supps, it’s the result of both hype & fear. The hype is self-explanatory and I’ve written recently on how modifications exponentially increase profit margins for companies, all the while possibly reducing ours because patients are spending more on product and therefore there is less left over for the practitioner fees 🙁 [The ones spending hours with them face to face, not to mention years & thousands on our training] The fear is perhaps less apparent, more insidious. The fear is that we’re not using the best, being the most effective, and deeper still, inevitably that we will fail to action our patients return to health. This is a big one. I think it’s pervasive, if not omnipresent, and works as a motivator for many positive actions by practitioners – like engaging in further education, reading that latest journal edition on your lonesome laptop when you could be streaming some series on a shared sofa. But this same fear can also undermine us, overwhelm us and shake our tree of trust, that we believe to be so firmly rooted within us, of the healing power of nature.
So while my position sometimes makes me feel very ‘old school’, I’m not suggesting we return to nutritional prescriptions composed exclusively of bee pollen & brewer’s yeast and I absolutely recognise and respond to an individual who has very specific barriers to benefiting from nutrients in their natural normal forms. But let’s be clear, they are a minority.
Some of you will know naturopath Dawn Whitten & know that she is one of my mentors. I’ve had the benefit of speaking with her over the years about herbal prescriptions but also about the principles & philosophy behind our practice & in one of many conversations she told me that a key objective she has with her patients is to rebuild their trust in their body, their own biological resilience (I love this concept and that’s a talk for another time!) and ultimately in nature. Well jeepers Dawn – how did you get to be so wise so young? But isn’t that central to vis medicatrix naturae? Maybe that Naturopathic Nanna’s club isn’t so fuddy-duddy after all. Want to join us?
Speaking of using nutrients in their most natural state for the best health outcomes – the best B3 is probably not what you think!!…. The Balance of B3
Most of us have been taught to ‘balance the Bs’ when supplementing, which discourages the use of single B vitamins in case this interferes with the regulation and roles of others. In reality, outside of a couple of dynamic duos like B12 and folate, there is little concrete information & evidence of this. In the case specifically of B3, however, we now know, the risk of an excess of the most common B3 forms found in supplements and fortified foods, results not only in disruption of other nutrients but imbalanced B3 biochemistry itself. Given B3, in its coenzyme form NAD+, is regarded as highly valued currency in the prevention of many diseases, as well as the key to our optimal health and longevity, it’s critical to understand the different forms and functions of the various B3 sources.
I’m experiencing some serious POTTS exhaustion – how about you? No, not POTS, POTTS: Preposterous Over The Top Selling of supplements, which seems to be at an all time high even amongst our practitioner brands. I saw a product name recently that included the word, ‘supreme’!*^# Is the choice of nutritional supplements now on par with selecting our pizza toppings?
When I previously delivered university lectures on population nutrition & the role of the food industry – we acknowledged that all the processing, packaging, and promoting the food industry invests in, creates a market and a source of competition that essentially doesn’t exist for their primary whole-food ingredients.
Take apples. How can we increase the profit margin on a humble apple? Aside from organic V conventional farming, the price that any of us would pay is pretty narrow and fixed. But send that apple to the factory to make juice (and chuck in some added vitamins to boot so you can feature this on the label!!), puree and package it in the most non-biodegradable way for kiddies, dice and stew the stuff and put it in little plastic tubs for the slightly older or throw in a long list of nasties with ‘essence of apple’ to make sauce for idk and suddenly you have the capacity for mark-up, an exponentially expanded profit margin & ‘something to say and something to sell’. In supplement companies, it’s not as far from this as you might imagine. Because nutrition (**WHAT A SURPRISE**) is a lot like primary whole-food ingredients – how does vitamin C compete with vitamin C? Hey, make it liposomal!! And the nanoparticles that we’re fearful of in our sunscreens and cosmetics..let’s use the same technology for our ingestives!! YES!!! Ummm any one recall, our fears re folic acid? Just asking…
I propose that ‘practitioner only supplements’ come under the same plain packaging restrictions placed on tobacco in Australia [I am joking but only just]. Remove the bright shiny distracting graphics and hyperbolic descriptors and only state the full ingredients and excipients list plus source where relevant. Let’s bring it back to simple(?) science, basic quality ingredients and affordable effective products for our patients. Then let’s see if we can spot the difference 🧐
Rachel loves nothing better than breaking through marketing babble and spin to get to the truth about supplements – their real strengths, niches, weaknesses, contraindications, therapeutic doses and best forms & therefore there is a dedicated section of her website with resources and recordings that do just this,here. These include reviews onB3, B12, Folate, Selenium, Zinc & Iron (of course!),Calcium D Glucurate,Co Q10, Quercetin, high doseVitamin DandFish oilsfor Mental health. These are a mix of Update in Under 30 recordings and longer presentations and her library is ever expanding! So, if you have a supplement you think needs some serious sleuthing on – send us an email…we’re always sniffing around for more!!
 The debasing of BMI as a stand-alone assessment of weight is long overdue given its significant limitations and lack of meaningfulness with respect to overall health. This coincides with a bigger societal and cultural shift towards inclusivity which involves redressing bias against people with diverse body sizes and compositions.
The debasing of BMI as a stand-alone assessment of weight is long overdue given its significant limitations and lack of meaningfulness with respect to overall health. This coincides with a bigger societal and cultural shift towards inclusivity which involves redressing bias against people with diverse body sizes and compositions. 
 You can purchase
You can purchase 













 I’m experiencing some serious POTTS exhaustion – how about you? No, not POTS, POTTS: Preposterous Over The Top Selling of supplements, which seems to be at an all time high even amongst our practitioner brands. I saw a product name recently that included the word, ‘supreme’!*^# Is the choice of nutritional supplements now on par with selecting our pizza toppings?
I’m experiencing some serious POTTS exhaustion – how about you? No, not POTS, POTTS: Preposterous Over The Top Selling of supplements, which seems to be at an all time high even amongst our practitioner brands. I saw a product name recently that included the word, ‘supreme’!*^# Is the choice of nutritional supplements now on par with selecting our pizza toppings?