It’s no secret I am in the midst of some serious deep-diving through the micronutrient evidence base & at a depth of about 30 metres I struck Boron! Don’t yawn! I saw that. Thinking, ‘boring’, when we hear, ‘Boron’, is almost as bankable as watching everyone reach for their water bottles when you mention anything hydration-related 🤣 But I am here to restore your positive regard for this mineral and remediate its bad (& boring) rep! In preparation for the Nutrient Prescriber’s Program we started each nutrient review with the seminal contemporary nutritional texts and then launched ourselves headlong into the latest & greatest research. By the end of all the Boron bits in all my trusty texts the yawn was not gorn! But the moment I started reading the research I was like, ‘Are we even talking about the same thing?!’Turns out we’re not 😵🤦♀️
You see Boron has been a longstanding victim of identity theft. What we’ve been lead to believe is Boron is weed-killer and ant-poison and look it does give us some of the benefits of Boron but not all. And it possess a pharmacokinetic & toxicity profile that naturally occurring Boron simply does not.
Who decided that the Boron that is ubiquitous in our environment but almost exclusively consumed by us only after biotransformation by plants – could just skip that last bit and still be safe and optimally beneficial?! Probably the same guy that came up with folic acid, may I suggest? Anyway, enough is enough. We all need to relearn Boron – naturally occurring Boron – in the form of Sugar Borate Esters (SBE)- the evidence of benefits for which will blow all of our little minds! Well it certainly blew mine! Looks like this natural form of Boron is going to hit the Australian market in the not-too-distant-future 🐦 can’t wait to see which supplier is sufficiently progressive and research-aware that they bring this to market, having been available as a high grade supplement, employed in numerous RCTS OS for some time. But this little Update in Under 30 is not waiting around for that release date – there is much to be gained from SBEs right now – so make some noise as the real Boron at last takes the stage!🎤
Boron has been the victim of longstanding identity theft and we unknowingly have been interacting with its imposter. Contrary to everything you’ve ever been told about this mineral, naturally occurring Boron is full to overflowing with benefits for our gut, our bones, our brain, our management of other minerals and is safe in large quantities. That ‘bad guy Boron’ you were introduced to and is still present in many of your supplements is a form we never consume in food…and therein lies a world of difference! Come meet the real Boron so you and your patients can get the real benefits!
You can purchase The Boron Deception: How We’ve Been Fooledhere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
Still. And yes – like you – I don’t see any slowing down any time soon in this extraordinary paradigm shift occurring in medicine and health. Which for us humans involves one humbling discovery after another.
Here we were thinking we made our dietary choices from a place of free will & individual preferences 🤣🦠
Thinking those microscopic mates, were making those B vitamins, and SCFAs and and and…for us & our benefit 🤣🤣🦠🦠
And while there’s a lotta love going on between our microbes and our micronutrients – in both directions – Pat Benatar said it best, “Love is a battlefield”
(sorry but I feel compelled to insert a link here for the youngsters – you’re welcome 😉)
The tussle over who gets to access those nutrients that are actually essential to both of us (the hostage and the microbiota) is an absolute turf war, peeps, and this battleground has seen some bloodshed! The new new question being raised is how the prescribing of nutrients, especially at the higher doses we tend to use, trickles down to influence and impact those microorganisms who reside in the bowel. Directly – as a selection pressure we have, likely unintentionally unknowingly, introduced. Which species do well when exposed to levels of a vitamin or a macro or trace mineral that are simply unobtainable in the diet? Yes – research answering these questions has begun in earnest revealing some positive ‘prebiotic-like actions’ of some but not of course for all nor in all scenarios. Want to learn more about this latest aspect we need to consider when formulating our nutrition prescriptions? You can either jump in and join us in the Nutrient Prescribers Program which kicks off next week to get across absolutely everything new in nutritional medicine or just dip your toe in here with our latest Update In Under 30: The Micronutrient Microbiota Universe
The world of health science went microbiota-mad a few turns back and there’s no sign of an end. Research continues to reveal the breadth of the GIT microbiota’s positive & negative reach, in particular, & with discovery upon discovery we’ve come to understand how often the microbiota are ‘managing us’. Both in terms of being integral to the success of our digestive, immunological, metabolic etc processes but also in a self-serving way, for example, directing our dietary preferences to satisfy their own needs. This has understandably prompted the question about the impact micronutrient supplementation is unintentionally having as a selection pressure on our gut microbes. Which bugs like which B vitamins when taken in excess of the amounts achievable in the diet? And which microbes flourish and which falter when we radically change their mineral exposure?
You can purchase The Micronutrient Microbiota Universehere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
I’m such a sucker for marketing!…ZoomZoom is from an old Australian car ad – an earworm clearly conveying ‘ the speed of something’, and let me tell you, totally fitting for this little Zinc tale I’m about to tell! Many years ago, I wrote a thesis on Zinc that necessitated me reading every research paper ever written (that’s how it felt anyway!🤪) on this trace mineral. Like everything in nutritional medicine, especially in the area of our burgeoning understanding of micronutrients, this is a highly dynamic space, so regular reviews of what’s new is essential and, since my thesis, part of my regular practice. Well, I just did my latest deep dive, and HELLOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO radical paradigm shift(s)…yep plural!
Zinc supplements should ideally be: Organic amino acid chelates Taken daily – due to the lack of Zinc stores in the body Taken fasting Taken in doses in excess of the RDI to compensate for the smaller % absorbed
Yep – nope. Or in true-blue Aussie: Yeah, nah. Can’t believe what you’re reading right now? Neither could I when I undertook this recent review but the studies are increasingly sophisticated and the resultant paradigm shifts are being echoed, reiterated & reinforced. And these have, in turn, challenged all those old ‘norms’ about how best to administer zinc for those patients with a shortfall. If you’d like to take this little journey for yourself…I suggest you start here! I immediately changed how I take it myself and now my mission is to both spread the word and get us all reflecting and reviewing our prescribing principles around Zinc…and tbh, around all micronutrients! After spending my ‘summer’ doing sufficient reading for a second thesis on everything new in micronutrients…I am armed and dangerously prepared for our upcoming *NEW* program: The Nutrient Prescriber’s Program which kicks off in late Feb for 5 months.
I truly believe that based on all this new information, we can now get so much more out of our medicines.
Nutrition represents such an extraordinary set of tools for us to work with, but it’s time to sharpen those tools in terms of how we apply them!
The Changing Zeitgeist Of Zinc Prescribing
Zinc research is a highly dynamic field and given its relative recency of discovery as being essential to humans, we’re still in the early days of truly getting to know this mineral. In just the last few years, enormous gaps have been filled-in regarding its regulation and roles that look to radically change our prescribing practices. Tune in to this essential update for some serious food for thought about doses and dosing frequency.
You can purchase The Changing Zeitgeist Of Zinc Prescribinghere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
Recently I asked practitioners to tell me where the ‘therapeutic reference range’ many of us were taught for nutrients comes from & no one has been able to answer that.🙄 If you’ve heard me refer to my original naturopathic education before you’ll know I generally hold it in high regard. And I’m forever mindful that there are always things that can be made better. What’s been playing on my mind lately is the recognition that I originally learned nutrition from one (exceptional) individual, and then went on to become the lecturer years later at that same and other institutions. Additionally, I am aware of some of my past students also going on to become the next generation of nutrition lecturers at those same places – and often in fact inheriting their lecturer’s notes, slides, overheads [showing my age!!] with the job. Can anyone else see a problem here? What’s brought this into sharp focus lately are many of the questions I’m endeavouring to answer as part of our much-anticipated Nutrient Prescriber’s Program. How much? How often? When? Which form when? & For how long? Which are the key questions we have to answer with every single nutritional prescription.
To not only source the most rigorous scientific answers to these core critical questions but to also develop a framework that we can all use to answer them for ourselves at the point of any future prescription creation, I have had to go to great lengths.
But as I research & write, I also keep asking myself, ‘How would ‘old-me’ have answered this?’ How did I up until now either consciously or unconsciously answer these sufficiently to make such decisions?
So it’s an ongoing little (& sometimes BIG🧠) internal debate that is raging as I write. And when I ask current praccies these questions they reflect back similar ‘old-me answers’, the vast majority of which were handed to us by our lecturers with plenty of top-up ideas from industry. These answers include things like:
How much? Somewhere within the therapeutic dose range? How often? Depends on lots of things but generally aiming for daily of course!
When? Minerals before food, fat soluble vitamins with or after, magnesium at night etc
Which form when? Now it gets tricky – because there are all these new forms that we weren’t even taught – but maybe ‘active’ – active is always better, right? Or is that natural? The most bioavailable?
& For how long?Ummmmm how long is a piece of string?! Until the signs and symptoms resolve?
Now all of these as general statements are partly correct. And with respect to the level of understanding we need to have when crafting a nutritional prescription for a specific patient, with a specific presentation and for a specific purpose (correction of deficiency Vs supranutritional Vs therapeutic antagonism etc)…well they are plain wrong in the majority of instances. Don’t freak-out in freefall!🪂 The prescribing of nutrients is a wonderful and typically, a wonderfully safe, modality that offers us the potential for extraordinary patient outcomes. When used well. We could all benefit, I believe, from just sharpening our tools so we bring out the very best in our medicines & in ourselves, as prescribers & clinicians. I am neck-deep in writing the 10 modules that can start us all on that journey. Want to join me?
And to be clear, about the educational echo chamber,
In the past I was part of the problem and ever since I have tried to be part of the solution.
With over a decade of mentoring practitioners, Rachel has recognised a need for an educational program that provides practitioners with more structure, more science, and therefore more certainty in navigating each individual prescription. This monthly meet-up is delivered in 5 live sessions and runs from February to June (10 modules). All sessions, encompassing both theoretical and applied learning will run for approximately 2 hrs each.
Let’s play a word association game of minerals & their major roles
I say, ‘Potassium’. Maybe you say, ‘Sodium Potassium Pump’ I say, ‘Magnesium’. You say, ‘Muscles?’ I say, ‘Calcium’. You say, “Bones’….
But I say, Second Messenger. And arguably the most pervasive & potent one, at that. Remind you about second messengers? Well, sure. They are the ones who get sh*t done. Not like a boss (i.e. hormone or neurotransmitter) who shout directives from above but never step foot inside the dirty guts of the engine room itself. It’s the second messengers who run these messages from the outside of the cell to the inside and the engine room, to ensure that the directive is actually actioned! Amazing huh! And free calcium in the blood is, as I said, really a superhero even among the second messengers – with its regular responsibilities including: Insulin, TSH, Adrenaline, Oxytocin, Serotonin receptor activation etc etc
Does, it have a dark side? Well, sure. Don’t most superheroes?
If the available Calcium in blood and the extracellular environment is too high then basically bad sh*t gets done. Including vasoconstriction, clotting, deposition of calcium in the wrong place like arteries and joints and etc etc. That’s why the amount of Calcium in our blood is the MOST tightly regulated of all electrolytes and, in turn, has the NARROWEST of reference ranges. But will a Serum Calcium level always tell you when there is a problem with Calcium regulation? No. You’d need to have measured the major regulator itself, Parathyroid Hormone (PTH). Wait, am I seriously trying to tell you, that Serum Calcium alone can look completely normal in spite of really damaging Calcium dysregulation underway – leading to accelerated BMD loss, increased cardiovascular and renal risks etc.? I most certainly am.
So do you know which of your patients’ really need PTH assessment and why 1 dominant group amongst those, is any woman leading up to and following menopause?
No? Well you better pull up a pew and have a listen and a watch then! Yes this latest Update in Under 30 episode even comes with a little video tutorial!🤓🤯
Parathyroid hormone is a career criminal. In addition to buoying dropping blood calcium levels via legitimate means, it illegitimately achieves this by stealing it from our bones. But you wouldn’t know it – because like all career criminals this occurs completely under the radar. Elevated PTH, however, constitutes the most modifiable risk factor for bone mineral density loss & fracture risk and offers the biggest BMD gains secondary to its normalisation. In addition to this, even within range but ‘high-normal’ PTH correlates with a range of other cardiovascular and urinary presentations & if combined with elevated serum calcium can become a multi-systemic presentation (GIT, Mental health etc) frequently mistaken for other aetiologies. So how can we be alert to this ‘bone thief’? Which of our patients will benefit the most from PTH measurement and monitoring? This recording, resource & video tutorial on how to use a Ca PTH Nomogram answers all!
You can purchase Unmasking Hyperparathyroidism – Menopause & Morehere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account. You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
Heck yeah. It’s going to take a lot more than 1 push-back post to turn this ship around! Likewise, I was only getting started with my recent Update in Under 30 episode, ‘What’s Hiding Behind Histamine’ 🤓😂 & part 2 has just been released where we unpack the case of a 41yo female with chronic diarrhoea, multiple food reactions, very high stress and very high oestrogen. Sounds like she’s a walking Histamine Headline – except she isn’t.
Right now we really do need to keep this conversation going such that a healthy discourse can help us deconstruct the histamine dogma.
I know I’m showing my age here, but anyone remember when Candida was having a ‘moment in the 90s? Ok, so that ‘moment’ stretched to over a decade of a ‘Candida-contagion’. No one could eat melons or mushrooms, eat ferments or feel joy. It was a bleak time that did our profession some reputational damage. Not only because seeing an ‘alternative practitioner’ became synonymous with being put on an unbearable, unattainable restrictive diet and positioned practitioners as peddlers of punishment but also because it took some time for science, in the form of accessible (& always improving) assessment methods, to come along and save us from the folly of the 1-diagnosis-for-all mentality.
Let me ask you, how many times do you actually see Candida overgrowth on reports from stool testing performed using best practice modern methods?
In my experience – never – not as a stand-alone issue. Occasionally, as part of the overgrowth of a suite of opportunistic organisms where the real-take home is the need to ‘remove the opportunity’ via the promotion of more good guys. So not only was the diagnosis incorrect, the proposed treatment for it was a complete misdirection as well.
Can’t help thinking in the current climate of Histamine Hysteria that history is repeating itself.
How will we all individually, and as a profession, respond this time?
In this follow-up episode we observe how the 3 key elements often hiding behind a histamine intolerance diagnosis: Misunderstandings, Missed Messages & the potential for Mistaken Identity, have played out in the case of a 41yo female who presents with chronic diarrhoea, a long list of problem foods including now a suspicion of ‘histamine foods’. Rachel offers up new ways to approach the patient work-up that cut through the ‘noise’ and enable us to better identify what is hiding behind histamine in similar cases of marked gut dysfunction.
You can purchase What’s Hiding Behind Histamine? – Part 2here. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account. You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
You’re invited to attend acnem’s 2023 Annual Conference ‘Long COVID, Navigating the Complexity, A Clinician’s Roadmap’.
Saturday 29th & Sunday 30th July 2023, Melbourne. Both face-to-face and online.
To get 25% off acnem Annual Conference USE CODE: acnem25
I can barely bring myself to write the word given how overused it has been of late 🤐🙄😯😕🙃 But I gotta say something! If we have found ourselves currently in a place where every second (or indeed single!) patient has a ‘histamine issue’ then I am afraid that it is we, that have an issue. (more…)
What level of Serum Ferritin represents ’empty’? As in complete depletion of iron stores?
Is it any value below the minimum of the reference range? e.g. < 30 mcg/L Or does the bottom of the reference range allow for a buffer and ’empty’ is substantially lower than this? Could patients actually be ’empty’ but still have Serum Ferritin values within the normal range? Could the same Serum Ferritin value occur in one patient on ’empty’ but with adequate stores in another?
When it comes to the recognition of Nickel as the number one metal allergen worldwide, affecting up to 30% of adults and with a particular predilection for women, it seems like Australian health professionals really do come from the ‘land down under’, with many of us still somehow yet to read that memo.
I’ve been ruffling feathers over here while speaking at AIMA in Auckland. While I am pretty familiar and comfortable with that role (& responsibility?) – this topic ruffled my own, arguably the most. In fact, I kicked off the presentation with, ‘What I’m going to say might make some of you uncomfortable but you know what, it makes me uncomfortable and if it makes you think a little less of me, well, to be honest, contemplating these issues has already made me think less of me!”
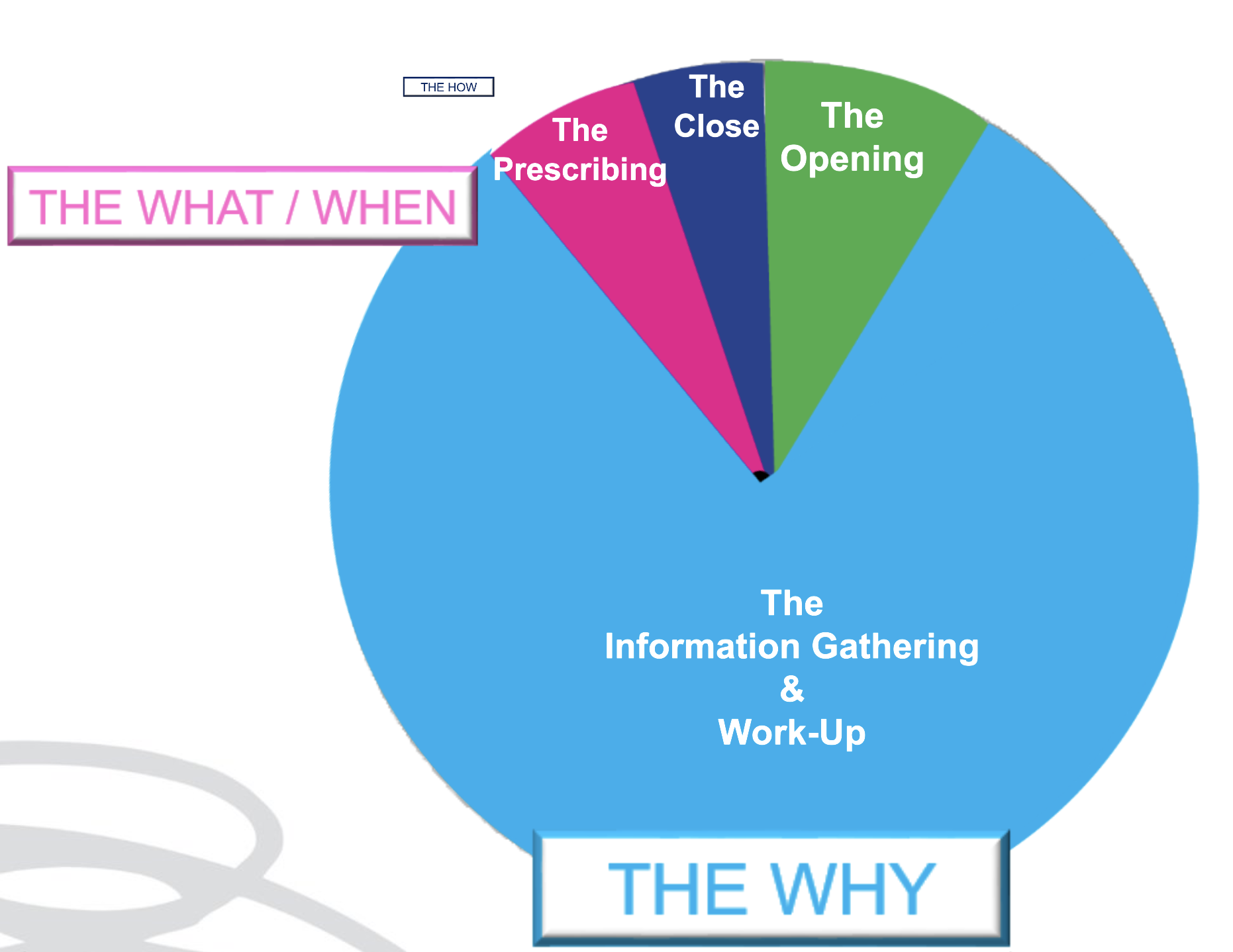
As an educator in integrative health, I have overwhelmingly been a peddler of knowledge and skills under the headings of: ‘WHY’ and‘WHAT’
Why – as in why does this patient present in this way, at this time. I am passionate about upskilling practitioners re our powerful contribution to the diagnostics & work-up of each individual. What – as in what changes (supps, herbs, diet etc) need to happen to correct for these very unique elements of imbalance in this patient to therefore aid resolution. We might label this, ‘personalised medicine’. But after so long in practice it’s patent that the best results don’t come from being the cleverest clinician nor the biggest biochemical brainiac. Knowing the ‘why’ and even the ‘what’, while enough for a minority of patients, fall short for the rest and can still fail to be truly about, & exclusively with, the most important person, in mind.
We’ve learned this before but it needs to be said again and again and again: much of any medicine is via the therapeutic relationship – and as part of this, our ability to PLACE the patient at the centre of their own SOLUTION. And therein lies the conversation we need to have in detail with them about the ‘HOW’ But how much time in your current consults is afforded to the ‘HOW’?
Being able to effectively negotiate with out patients the ‘HOW’ is an extension of Motivational Interviewing, Behaviour Change Theory & Patient Centred Care. It returns the humanity to our list of recommendations for each patient, pushing back against the autocracy that can tend to slip in with prescription writing. It powerfully reminds us that the prescription is only ever as good as the patient’s engagement & buy-in, and that’s only ever as good as our ability to write a prescription that is accessible & readily transplantable into their existing lives: to co-create with them Patient Centred Prescriptions. Someone in the audience had been my patient in the past – double awks right – because I absolutely know, I didn’t know this well enough back then. Back then when they were unable to do exactly as I had recommended – with their diet, their supps, their sleep, their work-life balance – they had, in turn, apologised for their ‘weakness’, ‘lack of willpower or diligence’ and me, being ever so gracious, accepted those apologies only to repeat the error of my ways and write yet more scripts that set them up to fail. 🤦♀️ I am committed to getting better at this and in this endeavour, giving both more attention & time in my appointments to the ‘HOW’ & yes I think we need to think creatively about how we use our appt time and between session touch points to achieve this – keen to hear about your perspective and experiences.
At the end of an information & insight heavy appointment, formulating a list of products and doses for our patients to take can feel like a bit of a ‘tada moment’, like a magician pulling a rabbit out of the hat. “Here is the solution – now off you go!” Research tells us, however, that treatment-plans that are a co-creation between you and your patient – evolving from a discussion that not only allows them a voice, but a major role in the decision making – are far more likely to succeed. While we are the authority on our medicines, our patients are the authority on what makes them tick & what’s likely to succeed, in terms of taste, texture, temperature & timing! This is called Patient Centred Prescribing and together with some other tips tricks and hacks I share with you in this episode, can really increase patient buy-in, compliance and therefore bring your treatment plan to fruition and fulfilment!
This is not about body shaming nor body positivity. I understand the crudeness of the body mass index, as a measure of (un)healthy weight – let alone (un)healthy muscle mass, so I don’t use this as a stand-alone assessment of weight, nor rigidly adhere to the categories it allocates individuals. With only minor recognised racial adjustments for BMI, I also recognise our concept of ‘healthy weight’ is incredibly whitewashed with minimal regard and consideration for clear ethnic and racial differences in physique. Patient’s lab results tell the real story. It’s in their results that we can discover someone is thin-on-the-outside-fat-on-the-inside (TOFI) or FOTI. These are patients whose BMI, WC,WHR, Body fat% etc identify them as obese – yet there is not a whisper of what I call ‘Adiposity Patterns’: no subclinical inflammation, no reduced glucose tolerance or actual IR, no raised transaminases that we expect to correlate with girth and the corresponding fatty infiltration of their liver. In this, as in so many other aspects of clinical practice, we are reminded to see each individual, individually.
AND if we adhered to this always, listening unfiltered to the whole health story and letting the labs speak, we would not miss those patients in whom unhealthy weight really is the most important underpinning, & all impacting, issue. And we are not doing our job, when we don’t.
I mean – we all know the detrimental effects of excessive adiposity – that’s like Pathology Unit 1 topic 1, right? I know we know it. Yet there are so many reasons why we might down-play, step-around, or even ignore its enormous contribution in our patient work-up and certainly the discussion that follows with our patients. That too is a no-brainer. Who wants to say to someone whose come seeking your help, as an explanation for their complex health concerns, ‘There’s no zebras here just a horse – one really over-weight horse!’ Knowing too that unhealthy weight results from the most complex constellation of factors (biopsychosocial) unique to each individual and that change in this health determinant, is arguably the slowest and hardest to sustain. But how are we serving our patients if we don’t?.
A practitioner presented this case of a 48yo F seeking help with the work-up: Self-reported inability to lose weight after 1st pregnancy = ‘obesity’ ongoing – now BMI 33.1 –> 25yo Reflux & Hiatus hernia Tx Omeprazole initiated – ongoing –> 26yo Depression Tx Venlafaxine initiated – ongoing –> 30s Back and other musculoskeletal injuries Tx Surgery & Opiates – ongoing –> 40s Hypertension & elevated resting HR –> Last 12mo – changes in Mx cycles suggestive of perimenopause & substantial weight gain
This patient didn’t ‘have’ any lab results but I think I can make an educated guess about how they would look and in particular whether they show the characteristic ‘adiposity patterns’ I mentioned before. What was my first thought about the most impactful element of the case? Obesity. What was my second thought? Where is all the weight (diet & intervention) history that would help us to understand how she is where she is, right now? We didn’t have any. The practitioner informed me that the patient was ‘not very interested in talking about her weight’ – in fact, according to her, it didn’t seem like losing weight was one of her goals. Now this could be several things: the fear of judgement, even her own self-loathing, the paralysing awareness of the enormity of such a goal, the dashed hopes of the past, or it could just be that her weight, as the key negative determinant of the majority of her health concerns & quality of life, has just never been brought to her attention, nor the connections explained to her in simple accessible language. So over to us, right?
There were other health determinants at play in this patient but the centrality of the adiposity was undeniable & the practitioner said this was the greatest take-home. She’d been ready to don some jungle gear and go hunting some zebras – but there was a horse right here in front of her and that could not and should not, ever be ignored.
What else became apparent was the lack of knowledge & skills regarding how to take a comprehensive weight history & why this is crucial. Not only for this type of unhealthy weight, the underweight require exquisite attention, as do those with a more labile weight than expected as an adult. This brilliant article by Kushner et al from 2020 is a total gift in that regard and a must-read for every clinician. We feel uncomfortable asking about certain things when a) a patient feels uncomfortable which is usually because b) we are uncomfortable and this ultimately comes from not being clear about WHY this information is so important and HOW this will ultimately enable us to better help THEM.
This is the very latest, comprehensive review of the key aspects of thyroid assessment that will revolutionise your understanding of thyroid markers. Gain a clear understanding of how to provide the best, most individualised, thyroid management by learning to read the real story in each patient’s pathology patterns. Boost your knowledge and confidence looking at TFTs, rT3, thyroid antibodies & related nutrient patterns, as well as AITD, environmental EDCs, HPA driven HPT issues, thyroid nodules, the impact of dietary macro- & micro-nutrient imbalances and much more!
This 4 part series provides over 10 hours of the very latest research & findings, punctuated with real case studies, that will both contemporise and deepen your understanding of all things thyroid, with a bonus recording on Adrenal Assessment.
And for weeks now I’ve really been banging 🥁🥁 The 1st drum was me making us all salivate & suffer through my month-long Mediterranean feast The 2nd, my ongoing incurable fixation on the ‘Power of the Ps’ – Protein & Potassium, not just individually, in terms of meeting optimal requirements for each, but relationally, as in, the (im)balance between them & the clear goals that have come from research for best health outcomes.
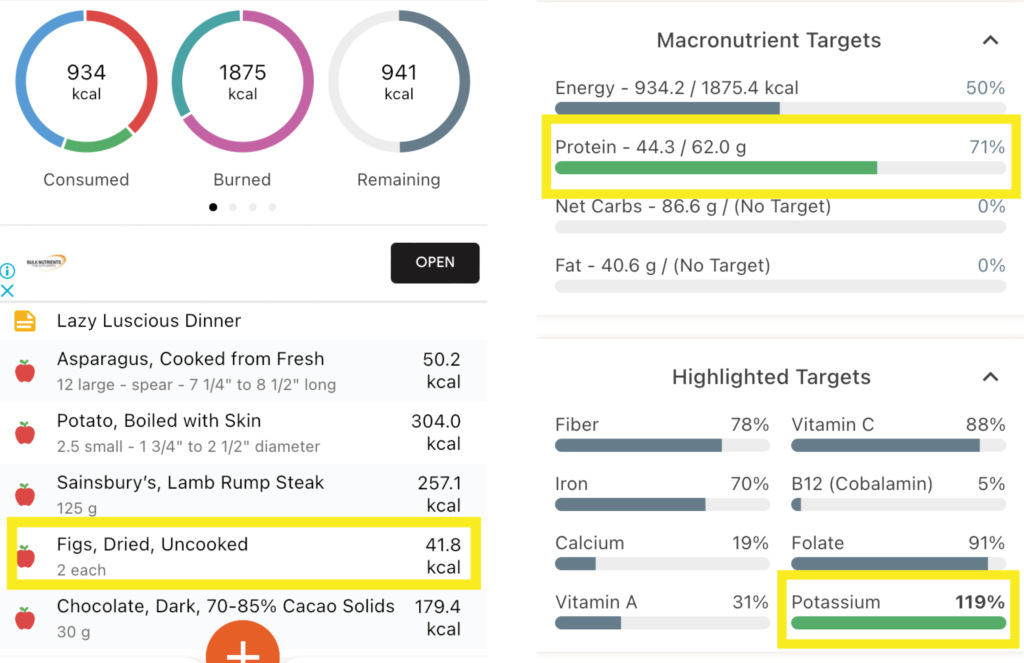
Maybe now you can hear the individual drumbeats merging to form some sort of chorus rather than a cacophony?! I can🎶 And largely that’s because I decided to put the Ps & Ps principles (Total Protein:Potassium < 1; Animal Protein:Potassium <0.6 etc) into practice, entering my own meals into software to see how often I kicked each goal and how often I missed (& [ouch] kicked myself). Personally, I think thirty years in the game can lead to some laziness around looking in depth at our own dietary habits. As in, I know the ‘rules’ right, back to front, so I’ve told the ref to have the rest of the season off! My meals are both mantra and memory foam. There’s a lot of eat and repeat. Like my heavy lunchtime reliance on my ‘protein power pack’: 2 XL soft boiled eggs on 1 piece of avocado paleo toast and a bunch of asparagus. My (in)famous buckwheat breakfasts loaded with nuts, yoghurt & fruit. My bulk-cooked plant protein heavy, animal protein light, stews, sauces and soups. Even, what I considered my laziest but luscious organic farmers market meal, pan fried lamb rump steak, steamed fresh new season potatoes & a bunch of asparagus. So which of these would you have put your money on for the most Ps& Ps goals kicked? 🤓🤯
The Lazy Luscious Steak & Veg Meal Wins with… Total Protein : Potassium of 0.56! Animal Protein : Potassium of 0.41 Btw that’s because of the Potassium-punch of Potatoes [>2200mg!] and the finale of Figs & dark chocolate [329mg]! Animal Protein : Vegetable Protein of 2 : 1 (ok so you can’t win everything!)
Now obviously I am just looking at each meal individually, but the Protein & Potassium goals are really daily ones, however, I, like most people, don’t lay out the totality of my ideal food intake for the day and then think, now how do I make this all edible?! I think in meals not metadata! So this little exercise was already incredibly rich in insights, checking my assumptions and snapping me out of some misguided mental calculations into the real world, placing a ref back on the pitch! I’m not ditching any of these favourites – just more mindful of what meal goes with others across the day, for better balance. Now all this analysis is time-consuming of course and while various software will do the macro and micro crunch, as far as I know, you still need to do all the Protein and Potassium calculations by hand, Ah yup. So, 1) I’m stopping now & 2) I’m thinking about creating a little spreadsheet that auto-calculates a lot of these targets once you’ve obtained that basic elemental data to input, for easier use in the future – would you use it?? [insert answer here 🙋♂️]
And then you can show me your kick arse protein/potassium combo! Because clearly even us ‘experts’ apparently need data to double-check our assumptions!
Now where’s the other 🥁 in all this, that Mediterranean one, I hear you ask? It’s in the figs! My lamb dinner actually just missed reaching the targets for protein and potassium balance…until my fig finale! And remember, what the Greeks say, ‘A few figs a day keep the chronic-mild-metabolic-acidosis at bay!’ 😂 Just jokes…
To prevent or minimise our slow but steady march towards sarcopenia, the need for dietary protein adequacy to fuel muscle maintenance is a no-brainer – but how does ageing affect this? We get less bang for our buck. We have to eat more, to get the same ‘amount’ but do you know why this is? Add to this, that also as we age, we experience a greater acid burden from a lower acid dietary load. And given that a higher acid load (PRAL), has been shown to have a negative effect on muscle and bone markers in the past, clearly to ensure optimal health of our bones and muscles as we age, we have a riddle, or two, we need to solve. How do we use Protein and Potassium intakes to benchmark our patient’s diet quality and musculoskeletal risks and can we modify their consumption of either, to drive therapeutic gains in terms of both BMD and muscle?
You can purchase The Protein & Potassium Riddle of Ageing – Muscles and Boneshere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
How much? How often? When is the best time & timing? do you know about friends, foes and frenemies? Which form, when? e.g. building blocks or bioactives? And for how long? aka are we there yet…?
These are the kind of questions that one would imagine nutritional prescribers can always answer – but can you? Yet this is the goal, right? So that with each and every unique individual who needs supplements – we have a clear, consistent go-to framework to guide & direct these prescriptions. One that makes scientific sense, offers optimal outcomes and removes the uncertainty.
From my interactions with thousands of practitioners, however, I know many of these key questions plague practitioners & they feel, at times, as if they’re flying without a net, or without a strong systematic approach, or at the very least without all the answers to these questions.
I’ve had so much good fortune & so many others to thank for providing me with this foundation. Fay Paxton – my nutrition lecturer in my under-grad who indoctrinated me with a systematic approach. Dr. Tini Gruner – my principal supervisor at SCU, who shared & further fuelled my passion for biochemistry and reading labs to extract insights into each individual. And thanks also to all the pharmacists I’ve delivered education to over the years, who, as a result of their grounding in the principles of pharmacokinetics, always ask the best questions – questions that if I don’t know the answer I know I need to know the answer! So I made it my mission to find out!
While we dip into these aspects of nutritional prescribing in our regular mentoring groups on an ‘as needs’ basis, I’ve decided the time has come to create a year-long program dedicated to sharing this information and building this skill-set in practitioners.
This monthly meet-up is delivered live (max 1.5hr) and runs from Feb to November with the following currently proposed format *subject to change dependent upon the needs of the group
Feb Factors Affecting: digestion, absorption (host, form, dose)
March What happens to what gets left behind? e.g. enhanced enterocyte micronutrient concentrations & their effects plus unabsorbed nutrients & their interactions with the colonic environment
April What happens to what’s absorbed e.g. distribution, hierarchy of needs, activation and deactivation
May The pharmacokinetics of prescribing
June Where do our ideas on dosing come from? e.g. Physiological Vs Pharmacological dosing & actions. The basis & believability of maximal intake boundaries?
July Bioefficacy V Bioequivalence. Beyond building block nutrients: Is ‘Bio’ (-active, -peptides, -materials) always better? e.g. GABA Vs Glycine, NAC Vs GSH, PLP Vs Pyridoxine, Niacin Vs Niacinamide riboside ——————————————————————Aug month off—————————————————————————
Sept How often & for how long? Are we there yet? And how would we know? Plus Fast Vs Slow Nutritional therapeutics
Oct Strategies for Supplement Success e.g. friends, foes and frenemies in nutrition underpinning principles with examples; compliance changers for clients
Nov Live attendance & opportunity to participate in a case-based mentoring session
This monthly ‘live’ meet up will be delivered as part of 2023 Group Mentoring as The Nutritional Prescribing Program Group Mentoring applications open 17 October 2022.
To join the waiting list and be notified when applications are open, email the team at [email protected]
Find out more about what groups are available for Group Mentoring in 2023 here.
Are we doing ourselves out of a job? I’ve been talking treatment plans with my New Grads recently. Given, only recently these were major assessment items in their clinic units, they have been trained to create ALL-ENCOMPASSING (biopsychosocial) prescriptions and recommendations of utterly EPIC PROPORTIONS – to simply prove they know it all. Problem is this doesn’t work in the real world.
Emailing your client multiple pages of advice that covers: a whole sizeable supplement schedule that only a military-training could nail (2 tablets 1 XTID 1 X BID, a liquid, a powder, some with food, some definitely not with food) plus dietary advice, plus hyperlinks to exercise advice, mindfulness exercises and a request for follow up investigations before the next appointment…is…a L*O*T!!
It is also ineffectual – because it completely disregards the human on the other end. Let me ask you this, how much change are you capable of between a first and second appointment, roughly a period of 2-3 weeks? Personally, I gotta say not that much. It took my dentist years to get me just embrace flossing & I don’t think I am an exception! With all the knowledge we possess its hard not to see people as (a long list of) problems (& problematic behaviours) that we translate into, and solve via, a prescription.
Effectively we are saying to patients with this practice model, ‘Go change & come back when you’re done & then I’ll probably ask you to change some more!’ That’s both a big ask and a huge missed opportunity.
I hear from reliable sources over the ditch, that GPs are increasingly referring their patients to, or teaming up with health coaches, rather than naturopaths. Given what I’m observing, I get it. Doctors on the whole only have time (and barely then) for a finger-pointing prescription – certainly not the time and touch-points required to actually support patients with the very difficult thing that is, behaviour change. Nor the skills to truly facilitate patients making the necessary and desired changes – so they outsource this role. But we shouldn’t.
After all – I want to be on my patients’ support bench & health care team always – not a flash in the pan, that blinded them with science or my ‘smarts’ and proved to them in one over-stretching prescription – that naturopathy is not for them, or at least, they’re not fit for the task.
At the end of an information & insight heavy appointment, formulating a list of products and doses for our patients to take can feel like a bit of a ‘tada moment’, like a magician pulling a rabbit out of the hat. “Here is the solution – now off you go!” Research tells us, however, that treatment-plans that are a co-creation between you and your patient – evolving from a discussion that not only allows them a voice, but a major role in the decision making – are far more likely to succeed. While we are the authority on our medicines, our patients are the authority on what makes them tick & what’s likely to succeed, in terms of taste, texture, temperature & timing! This is called Patient Centred Prescribing and together with some other tips tricks and hacks I share with you in this episode, can really increase patient buy-in, compliance and therefore bring your treatment plan to fruition and fulfilment!
Last week, yet another patient with refractory diarrhoea, up to 10 stools a day, Bristol type 5-7, for 3 decades following a diagnosis of Crohn’s at 16 years old. A range of specialists have thrown everything at ‘it’ – single & combination immunosuppressants, TNF alpha blockers, buckets of sulfasalazine and bathtubs of antibiotics – she’s been gluten and dairy free for years, trialled strict diets that are FODMAPs free, low histamine etc etc etc. She’s even had 50cm of her terminal ileum removed & the diarrhoea continues unabated – perhaps even worse than before…& therein lies a major clue.
1/2 patients with Crohn’s exhibit bile acid malabsorption –> diarrhoea but with terminal ileum resection this jumps to > 90%
This is Type I BAD (Bile Acid Diarrhoea) & is the easiest to spot, being the result of anatomical change. You remove the section of the small intestines responsible for 95% of the reabsorption of bile acids…a LOT of bile acids are going to be present in the colon where they act as potent osmotic laxatives, right? But there are 3 other types which are a little trickier to identify – including one that affects up to 50% of IBS-D patients.
Being a child of the 80s⚡🎹 (ok a teen of the 80s but who’s counting?!) and a personal fan of fat, I NEVER thought I would EVER be recommending a ‘low fat’ diet to ANYONE🤐
But hey, that’s another ‘absolute’ that needs challenging, right? I mean this is the primary, almost only, dietary change these patients need to make and as a stand-alone intervention, is highly effective for many. We’ve had several patient successes in the last year – a total game-changer for patients in similar situations where all kinds of ‘restriction’ had brought zero joy and reward for all their ‘good (dietary) behaviour’. While sequestrants (like cholestyramine) are recommended in BAD, and are certainly worth a trial at least, patients have very mixed results – for some, in combination with the low fat diet it’s a winner – for others these meds cause GIT upset all on their own and actually undo the good of the fat restriction. Being able to identify the true reason for their loose stools and stop them going down endless rabbit holes of ..is it? is it? is a great way to re-empower people who’ve been bossed and bullied by their bowel for far too long 🤓💪🧻
This is not a trick question. Up to 50% of all patients diagnosed with IBS-D actually have bile acid diarrhoea (BAD) underpinning their digestive complaints as well as some patients with non-resolving diarrhoea post-cholecystectomy and gastro. Knowing which ones do and how to manage this, which requires distinctly different approaches from our general management of IBS, is the key. As always, good lessons come from those we learn in the clinic and this story starts with a patient and how we came to recognise the BAD in her belly.
And health, no matter which side you sit on, seems to be particularly plagued by them. I (incorrectly) recall my 4 year degree as being a series of deep personal losses, some favourite food, then caffeine, then alcohol etc etc.😂 Likewise, I’m aware that naturopathy & integrative health’s ‘voice’ in the ‘conversation’, could arguably be perceived as mostly a negative one – as in, ‘No. Never. Not good. No, not even a little bit?!’ But I love both playing devil’s advocate & reading the research (ALL the research – even the stuff that doesn’t support my views and position GASP!~) so I am less in favour of absolutisms. This came up recently when I suggested alcohol may improve iron uptake 😬
Practitioners’ responses were 1 of 2 types: humorous dismissal (“steak & beer for breakfast – at last a naturopathic prescription I can support!”) or horror. But why are we so attached to the absolutes in spite of contradictory evidence?
Let me ask you this: is coffee bad? Full stop? Period? The end? Or is it the most concentrated source of antioxidants consumed in the average Western diet? Does it improve bile flow, peristalsis and at higher levels actually protect the liver against damage? Clearly, we need to read all the evidence, including, the favourable and make individual decisions about ‘what serves and what sabotages’, for each patient. But do we? Or do we imagine we only get membership to the ‘Ultimate Integrative Health-club’ when we adhere to blanket bans?
Similarly I, like many of you, see a LOT of iron deficient women – & a fair chunk of these have been incorrectly labelled, ‘refractory’ because theconventional correction strategies (high doses everyday) don’t actually make sense. But like you guys too, I’m always on the hunt for new ways to improve iron absorption in these women, so I can hit them & their gut with less. That’s why I shared the research regarding alternate day dosing, and taking a supplement within an hour of exercise and now, I dare to ask if a tipple could be helpful?
While we know that both ‘GOOD’ (exercise) & ‘BAD’ (alcohol) health behaviours increase gut permeability, which sounds ‘BAD’, right?
But could this be ‘GOOD’ for some?
This has certainly been demonstrated in relation to exercise & iron but most of the research investigating how alcohol intake effects iron uptake and status is based on alcohol abuse. The study below, however, based on a large sample of non, mild, moderate & heavy drinkers captured in NHANES data – is a very well written and reasoned article, such that it can exclude liver damage, inflammation and HFE mutations as other explanations for the better iron status, in drinkers. And it found:
I challenge you to read it for yourself and challenge your absolutes!🤓
Oh and just in case you’re thinking, “Have we all misdiagnosed iron deficiency and it’s actually a Copper deficiency underneath?”because last year the fashion was everyone was copper toxic and now this year someone’s making noise saying everyone is copper deficient !!! (Absolute? Anyone?!) Ah, no. Copper deficiency, as a cause of iron deficiency and anaemia, has been around for about as long as nutritional medicine itself. It is absolutely a thing. But in the absolute minority of people. And if you go back to some basic maths & compare and contrast Fe & Cu at each level: 1) requirements almost 20mg Vs < 2mg 2) average intake (inadequate Vs adequate) 3) bioavailability (Fe < 20% more typically < 10% in a modern low meat diet Vs Cu is typically >50% ) and do some basic sums I call, ‘Menstrual Maths’ – You’ll likely deduce that inadequate iron intake and uptake, given our losses, is in fact the common culprit and a ‘coldie’ may be more beneficial than copper in most! Can y’all stop asking me about that now – pretty please?
And then you don’t. The reality is we all struggle at times with correcting low ferritin or iron deficiency anaemia – so what have we got wrong? In spite of being the most common nutritional deficiency worldwide, the traditional treatment approaches to supplementation have been rudimentary, falling under the hit hard and heavy model e.g. 70mg TIDS, and are relatively unconvincing in terms of success. New research into iron homeostasis has revealed why these prescriptions are all wrong and what even us low-dosers need to do, to get it more right, more often!
Did you know you can subscribe to these? We deliver at the end of each month, just add a 12-month subscription to your cart and Rachel’s latest research is on it’s way to you!
Burning, tingling, crawling, buzzing, humming, zapping, pins & needles, numbness: our patients often tell us about strange sensations they have in various parts of their body. It’s typically not their major concern, but they mention it as an aside, a curiosity, ‘another weird thing I get’. While they may have trivialised this, relative to their ‘real issues’ [insert gut, hormonal, mental health] we should do the opposite and bring this concern to top of the list to correctly identify the cause.
If bilateral sensory nerves are mis-messaging it typically means 1 of 2 things: 1. Nerve damage is occurring – and if allowed to progress this can become irreversible or extend to motor and central deficits 2. Nerves are irritated or impaired – and this tells you something ‘systemic’ is out of whack and these sensations are often the only alarm bell
The top cause of paraesthesia, falls into the first category and is of course diabetes – and yes even now diabetics will walk into your clinic not knowing they have this (a good old HbA1c should be routine to rule this out). Second on the list is alcohol dependence. The third most likely explanation for the patient with paraesthesia is nutritional. And in contrast to what many of us might incorrectly think, there is a long list of nutritional imbalances that can be responsible for either, nerve damage or irritation, and B12 deficiency is not in fact the most likely.
That’s right all you nutritional ninjas🐱👤 – that makes the correct identification of the cause & the solution our bag, right? I mean who else is going to do this, accurately?
Asking the right questions about these sensations helps you to quickly confirm when a nutritional cause is likely. From there we need to know how each single micronutrient excess or deficiency or in the case of some, ‘sort of single’ nutrients (we all know people who sit in this category, right?! So why not nutrients 😂) are likely to present, via ‘easy-to-spot’ key characteristics that cover: pattern of distribution, speed of onset and progression, risk factors, accompanying features etc. In our final New Graduate mentoring session for 2021, a practitioner presented her patient who rated her concerns as 1) Fatigue 2) PMS 3) GIT issues & 4) Tingling & crawling sensations across limbs, face, lips and tongue…and I was like, whoa stop right there, you might just have given us the answer to all of the above~!~! Seriously. Here’s a clue: it wasn’t oral allergy syndrome and it wasn’t B12. Can you pick it?🤓
The Patient with Paraesthesia – Part 1 Patients often mention experiencing peculiar sensations: crawling, tingling, burning, as an aside, as a ‘oh and by the way’. But while it may not be their top priority – it should be ours. That’s because nutritional imbalances are the 3rd most common cause of these and timely treatment is essential to prevent progression to more serious issues. The list of potential nutrient deficiencies and excesses behind these, is long, but this recording, the first part of 2, will help you narrow the differentials, nail the diagnosis & the solution.
The Patient with Paraesthesia – Part 2 In this continuation of this topic, we discuss several less talked about nutrients whose deficiencies drive potent pathology for the nervous system & move onto a cluster group of minerals, whose imbalances create functional irritation rather than organic change. This episode includes a range of excellent resources from videos demonstrating in-house tests you can perform to aid diagnosis, as well as our own Ready Reference which assists correctly categorising the different paraesthesia patterns and the nutrient issues behind them
You can purchase The Patient with Paraesthesia Part 1here and Part 2here.
BUY PART 1 & PART 2 TOGETHER AND RECEIVE 10% DISCOUNT BY USING CODE BUNDLE12
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
Just like Kevin, ‘Niacin’ is profoundly misunderstood and consequently runs the risk of doing us harm. Unlike ‘Kevin’, we can’t watch the movie to see how this (our arguably excessive use of the wrong forms of B3 in supplements and fortified foods) is all going to play out, so that we can be suitably alarmed and start making some different choices. The risks that follow from our B3 ignorance are twofold:
One comes essentially from our gross under-estimation of this B vitamin – we’re stuck in the Pellagra Paradigm, believing that prevention of the 4 D’s is confirmation of adequacy.
The second, is our lack of discernment when it comes to the different forms or precursors of B3 & our unfamiliarity with their very specific physiological roles – good and bad.
In this regard we’re all likely to say, ‘Well back up there 1 second, we do know that Niacin (aka nicotinic acid) is different from the other forms!’ Producing flushing, yes. Used as a lipid lowering agent in pharmacological doses, yes. But can you tell me, which serious concerns and biochemical disruption is shared between both gram doses of niacin and everyday ‘routine’ mg doses of niacinamide? Yep, that one, the so-called ‘safe’ one. Better still, can we all list the various B3 forms in order from most to least potent, in regard to their capacity for NAD+ promotion in the human body?
Because this is now the definition of B3 ‘adequacy’ or ‘optimisation’ according to modern scientific understanding & it is a long long way from the absence of Diarrhoea, Dermatitis, Dementia and Death!
In fact, the boosting and optimisation of NAD+ pools in the human body is key to life – a long and healthy one according to the current research consensus – and its depletion is akin to ‘death’, or a faster one, anyway. From increased metabolic disorders, mitochondrial dysfunction, impaired gene stability (cancer, infertility etc) and higher rates of neurodegenerative disorders, just to start, these take up the lion’s share of our chronic health burden and battle that currently dominates the dis-ease landscape. And more niacinamide might just make that worse.
I didn’t mean to to alarm you. I am alarmed. Want to deep dive into this yourself? Start with this older but still brilliant review article by Bogan & Brenner. Want me to hold your hand while we jump off the high platform diving board together into this vastly different and powerful new understanding of B3? Let’s do it!
Most of us have been taught to ‘balance the Bs’ when supplementing, which discourages the use of single B vitamins in case this interferes with the regulation and roles of others. In reality, outside of a couple of dynamic duos like B12 and folate, there is little concrete information & evidence of this. In the case specifically of B3, however, we now know, the risk of an excess of the most common B3 forms found in supplements and fortified foods, results not only in disruption of other nutrients but imbalanced B3 biochemistry itself. Given B3, in its coenzyme form NAD+, is regarded as highly valued currency in the prevention of many diseases, as well as the key to our optimal health and longevity, it’s critical to understand the different forms and functions of the various B3 sources.
I say: Biotin, Broccoli Sprouts & Bone Broth You say….?
If you said: ‘Sulphur’, go directly to the top of the class, passing ‘Go’ & collecting $200 on your way!🤓 If you nervously said…”I don’t know, they all start with ‘B’ ?”, you are not alone. In fact, most integrative health professionals aren’t aware of the Sulphur Strategies they’re using, probably, everyday. But it’s time we all were.
How about this list? Glycosaminoglycans (GAGs for joint, gut etc tissue integrity), Cerebroside Sulphate (Myelin), Metallothionein, Glutathione, Hydrogen Sulphide (H2S), Co-Enzyme A, Lipoic acid, SAMe, are just some things Sulphur is essential for.
I could go on…and on and on. You see Sulphur, in spite of being an essential macromineral (adult dietary requirements > 1g per day) and critical to health, remains largely unseen. Often we don’t know when we’re writing patient prescriptions that actually we’re using a particular vehicle for Sulphur and therefore we’re also not able to discern which, of the very long list of options (dietary and supplements), makes the most sense in this patient at this time. We’re not to blame, not many ‘possess the power’ to see it, it seems. Por old essential, irreplaceable Sulphur doesn’t even have an RDI. But the time has come to take a good look. We need to know how patients are able to meet their needs, who needs more and how, very commonly, someone who is seemingly ‘consuming enough’ may still exhibit a functional Sulphur deficiency with poor musculoskeletal tissue integrity, low white cell replication capacity or higher oxidative stress load etc and in those who do have a shortfall, how to treat successfully & safely. Who needs a top down approach (more protein, methionine, cysteine, bone broth) and in whom would that be a risky path and using ‘downstream’ Sulphur products instead would be a better balance of pros and cons?
Because all Sulphur needs to be handled with care.
That’s right. Like other highly chemically reactive minerals, with reactivity comes risk – a great potency that requires careful consideration of both form and dose, so that we can harness this power for good not…well evil’s a bit strong…but how about, for not-good. I’m a bit of fan of Sulphur and using Sulphur strategies in my patients. I think it has interesting echoes with our past: the ‘healing’ waters of a Sulphur Spring and of course even further back the old ‘brimstone and treacle’ medicine of eons ago. This paper by Nimni in 2007: Are we getting enough sulfur in our diet? got me thinking about Sulphur again in a contemporary context, over a decade ago, I’ve done a lot more thinking, researching and prescribing since then but it seems that Sulphur still remains ‘unseen’ by most. But with the rise and rise and rise of popular Sulphur-based supplements (alpha lipoic acid, GSH, N-acetyl glucosamine, Brassica & Allium extracts and concentrates, N-acetyl-cysteine etc) I think it’s time to talk.
If you don’t have a clear picture of the gross daily requirements, determinants of altered individual needs, sources, regulation & associated deficiency picture of Sulphur, you’re not alone. Turns out this essential macromineral remains ‘unseen’ by most, even though you’re probably writing prescriptions everyday that have Sulphur as their key component. From the simple: Taurine, N-acetyl cysteine, Protein powders, to the sublime: Brassica extracts & concentrates, N-acetyl Glucosamine, Alpha Lipoic acid etc. In order to use these Sulphur strategies successfully and safely, however, we need to fill in the missing detail on its metabolism, the difference between the ‘organic’ and ‘inorganic pools’, how regulation regularly goes wrong, even in those seemingly consuming enough, and how to balance the risks of this reactive medicine with its substantial therapeutic value. This recording comes with a great clinical tool to help you at last see the Sulphur strategy most indicated for your patient.
The latest Update in Under 30 has landed!!!
You can purchase Unseen Sulphur – Time to Take a Lookhere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
I talk so much about iron, I feel like I’m cheating on my life partner (Zinc)…but these two are arguably the main mineral deficiencies we encounter most consistently in our patients and, don’t tell Zn, but quite frankly, in terms of who’s more well recognised out there, Iron throws some serious shade! But the truth is they’re a ‘twofor’, as a result of their similar distribution in food, with both demonstrating significantly better bioavailability (read: virtually double) from flesh foods etc, ‘Watch out, she’s on the attack again!’ I can hear the V’s (vegetarians and vegans) say and yes I think you see this one coming…but I think it’s possible to be pro moderate meat, without being, antiV.
Ethical and environmental aspects aside (just momentarily) it is hard to argue against the nutritional benefits from moderate meat for most patients.
I tried, trust me. Put my own body on the line (and my babies) to be a vegetarian for over a decade. But as the wheels fell off for me, I noticed them falling off for so many others…and these were people who were educated, with a capital ‘E’ and putting serious ‘E for effort’ into substitution etc Not everyone of course – but a LOT of women and occasionally some men. There was no denying their ‘iron hunger’ (high serum transferrin), their movement towards microcytosis (however slight that ‘smallifying’ may be…we don’t wait for anaemia, right?), their poor zinc status and more importantly, the clinical chaos of impaired immunity, some cognitive or mood issues that presented, as a result. I went back to the mineral manual, back to all the science that helps us to understand these minerals especially in a modern dietary context.
Ah yes…meat has become marginalised in our diets compared to those of our yesteryear selves (ABS data) while our consumption of potential mineral inhibitors…you know, all the good, but bad, but good foods, like legumes and grains and green tea and and and…has risen…especially among the kind of clients who come to see us, right?
Which ultimately leads to a lower iron ‘income’ with the same outgoings, again especially for menstruating, pregnant & breastfeeding women.
The books don’t balance. (So then…IV Fe to the Rescue???)
Bite me…it’s just science. There have been some wonderfully thorough studies on this very issue and thoughtful discussions. This study in particular, by Reeves et al, of Australian women in their 20s followed for 6 years to 2009, argues that just a 1mg/d increase in heme iron from flesh foods could reduce susceptibility to the subsequent development of iron deficiency amongst omnivores. So while the median daily intake of fresh red meat in these women was just 39g/d, their analysis found that an additional 70g of lamb or 60g of beef…or about 140g of chicken and 250g of fish if you prefer white over red, appeared to be the positive tipping point for women and their ability to stay iron-replete. Well below ‘dietary guidelines’, nowhere near the scary cancer correlations (which of course may be more about fat or nitrates or ??). Moderate meat intake, right? Just saying. And don’t worry, I know. The only thing worse than an evangelical ex-smoker is a rambunctious reformed vegetarian 😂
Need A Manual on Minerals?
Minerals represent a critical tool in naturopathic nutrition and there has been an explosion of research in this area over the last 10 years. In order to optimise patient care, practitioners need to keep up with the constant stream of information, updating their previous beliefs and understanding in the process. This seminal 7hr seminar (!!)…yes…seriously..it’s THE MANUAL..is designed to facilitate and accelerate this process of review and re-evaluation via a fresh look at the key minerals iodine, selenium, iron, copper, zinc, calcium and magnesium.



 You can purchase
You can purchase 
 You can purchase
You can purchase 









 Burning, tingling, crawling, buzzing, humming, zapping, pins & needles, numbness:
Burning, tingling, crawling, buzzing, humming, zapping, pins & needles, numbness:

