Still. And yes – like you – I don’t see any slowing down any time soon in this extraordinary paradigm shift occurring in medicine and health. Which for us humans involves one humbling discovery after another.
Here we were thinking we made our dietary choices from a place of free will & individual preferences 🤣🦠
Thinking those microscopic mates, were making those B vitamins, and SCFAs and and and…for us & our benefit 🤣🤣🦠🦠
And while there’s a lotta love going on between our microbes and our micronutrients – in both directions – Pat Benatar said it best, “Love is a battlefield”
(sorry but I feel compelled to insert a link here for the youngsters – you’re welcome 😉)
The tussle over who gets to access those nutrients that are actually essential to both of us (the hostage and the microbiota) is an absolute turf war, peeps, and this battleground has seen some bloodshed! The new new question being raised is how the prescribing of nutrients, especially at the higher doses we tend to use, trickles down to influence and impact those microorganisms who reside in the bowel. Directly – as a selection pressure we have, likely unintentionally unknowingly, introduced. Which species do well when exposed to levels of a vitamin or a macro or trace mineral that are simply unobtainable in the diet? Yes – research answering these questions has begun in earnest revealing some positive ‘prebiotic-like actions’ of some but not of course for all nor in all scenarios. Want to learn more about this latest aspect we need to consider when formulating our nutrition prescriptions? You can either jump in and join us in the Nutrient Prescribers Program which kicks off next week to get across absolutely everything new in nutritional medicine or just dip your toe in here with our latest Update In Under 30: The Micronutrient Microbiota Universe
The world of health science went microbiota-mad a few turns back and there’s no sign of an end. Research continues to reveal the breadth of the GIT microbiota’s positive & negative reach, in particular, & with discovery upon discovery we’ve come to understand how often the microbiota are ‘managing us’. Both in terms of being integral to the success of our digestive, immunological, metabolic etc processes but also in a self-serving way, for example, directing our dietary preferences to satisfy their own needs. This has understandably prompted the question about the impact micronutrient supplementation is unintentionally having as a selection pressure on our gut microbes. Which bugs like which B vitamins when taken in excess of the amounts achievable in the diet? And which microbes flourish and which falter when we radically change their mineral exposure?
You can purchase The Micronutrient Microbiota Universehere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
Any steps towards inclusivity in societal & cultural terms are cause for celebration but in medicine, that can come in the form of a ‘diagnosis of inclusion’, the opposite, of course, of a ‘diagnosis of exclusion’ and potentially as slippery and loose as it sounds. That’s the somewhat precarious position we find ourselves presently in with perimenopause and menopause. With greater recognition of just how long health effects can kick in before there are any cycle changes [2-12 years for those of you playing along at home] and the widening lens now taking in the diversity of such health effects, women’s health has had a win. But, I would argue, this is not without a double edge. After all, aren’t we, as a result, more at risk, as women, of having everything attributed to “just ‘the change’, love”, and, in turn, going to be offered sex hormones more often as the solution?
The builder responsible for my reno arrived one day with a frown. When I asked him what was wrong – he said he’d just had his second high PSA result and now the doctor wants him to see a specialist. It was apparent that he felt this was a real cause for concern. Talk about raising a red flag to a bull 🚩🐂 Yes, of course you know what followed. I insisted on reviewing the results myself only to find the reference range provided on his report was not specific to his age – and if we adjusted up for this (as the science supports) his result is just 0.5 ng/mL above the expected value!
Now, remember he is a builder so, ‘0.5’ in his mind might well be on par with 5mm which apparently is a big deal…or so he keeps telling me every time I try asking for some weird unconventional thing for my roof, windows, walls, whatever!! So I still had to provide a little bit more detail for him to get perspective and to understand the true meaning (and lack of scary meaning) of his results.
This however is just a micro-illustration of a big problem in pathology – we all risk a lack of perspective but if we can get it back, aids us to see that seemingly ‘normal’ results are sometimes a concern, and so-called ‘concerning’ ones, non-significant. The incredible patient insights that can be gained from being able to measure & monitor actual quantities of things in our patients; nutrients to novel disease markers, precursors to end-products, all comes down to understanding how their values compare with…with what? With someone of a different sex and age? With ‘all adults 18-108!’? With any other pre-menopausal woman regardless of reproductive or cycle stage? With ‘the average’ adult given that this current definition is overweight & unwell? Who are we comparing ourselves and our patients to?
When I undertook my undergraduate training many moons ago – there was no education in blood test interpretation. But as soon as I got out into practice I found my patients had all these bits of paper filled with magic numbers that I felt certain might offer me insights and a deeper understanding of their whole health – and how to best help them.
I desperately wanted to decipher this foreign language and made it my mission to do so. I was lucky enough to meet and be paired with a kindred spirit, Dr Tini Gruner, who happened to be my supervisor when I returned to undertake my honours thesis. Together we pooled our knowledge, sought out & shared with each other yet more and found that, together with comprehensive case taking, it provided excellent scaffolding to our work-up of patient cases. Better than that, it created this baseline for patients, identified clear treatment objectives and we could measure the success of our interventions based on how their results did (or didn’t) respond to our interventions. It was (and still is) a totally thrilling way to practice.
We talk about there being both an art & science to medicine generally and certainly an integrative approach. Without the benefit of pathology interpretation, I felt too at sea at times, without quite enough of the science to check the accuracy of the ‘art’ and my speculation.
Being able to understand what each individual result represents and reflects, to know how to form meaningful comparisons – with external reference ranges that speak to healthy individuals of the same sex & life stage, derived from rigorous research – and also form a comparison with the patient themselves, to pick up on the most subtle and significant early alerts to an emerging pathophysiological or healing process – is the skill, I believe, we all need in health to complete the toolkit. That’s why I made it my mission to learn the language of labs, from a conventional & integrative interpretative perspective, and then to share this learning with everyone wanting and willing to take this baton from me (& Tini) and run with it 🏃♀️🏃
MasterCourse I: Comprehensive Diagnostics. Click here to read more and here to purchase it.
*Please note that this is the place to start for everyone wanting to add preventive diagnostics to their tool kit. It is also the pre-requisite for MasterCourse II, so make sure you have completed this before continuing with MasterCourse II: Thyroid and Adrenal Diagnostics.
MasterCourse II: Thyroid & Adrenal Diagnostics. Clickhereto read more and here to purchase it and sign up for the Free Watch Party commencing tomorrow, 3rd August 2023 with is included with each purchase of the MasterCourse II.
Rachel: And sometimes emails from practitioners provide me with both the question and their own answer to their question even!
Cameron Barker’s (Ex-student long-term learner & mentee)email arrives titled:Unexpected Source of Iodine in Placenta Caps?!
A 32 yo female with a 12-week-old daughter came to me as she was not feeling well, in particular, she reports fatigue, racing heartbeat, anxiety and loss of appetite. Previously, 2 years ago, I had helped her with her Hashimoto’s. I did not hear from her for a year or so and she fell pregnant and was recommended to take a well-known iodine-containing pregnancy multi.
Just as optimal integration of lab results into our patient work-ups makes ‘the invisible visible’ we thought we might make visible some of the everyday Q & A that we engage in with wonderful practitioners who are fast becoming Diagnostic Divas & Divos.
Praccie email arrives with subject header ‘Graves Help’ (or is that ‘Graves…HELP!’🤔)
Practitioner: I have a Grave’s patient who required Propylthiouracil (PTU) for a few months from late 2022 until Jan 2023 which obviously took her thyroid in the opposite direction (see labs). Following a miscarriage last year, she has conceived and is around 6/40 and her current TSH result has come in at 3.3mIU/L, her TPO Abs > 1000 and she also has low-level Tg Abs (TRAbs not measured this time) and this is what she just said to me:
“I just had my specialist session this morning – and she has put me on thyroxine (50mcg) as my thyroid is quite low. I also asked her about the prenatal vitamin and she said it was safe for me to be on iodine at this time, as the Graves isn’t present and baby needs it for the development of its own thyroid.”
Oh gawd! Preg? Iodine? Graves? Antibodies? Antenatal or postnatal aggravation?!
Is there an UU30 I can listen to to help me understand this?… sorry for the panicked email…
I’ve been ruffling feathers over here while speaking at AIMA in Auckland. While I am pretty familiar and comfortable with that role (& responsibility?) – this topic ruffled my own, arguably the most. In fact, I kicked off the presentation with, ‘What I’m going to say might make some of you uncomfortable but you know what, it makes me uncomfortable and if it makes you think a little less of me, well, to be honest, contemplating these issues has already made me think less of me!”
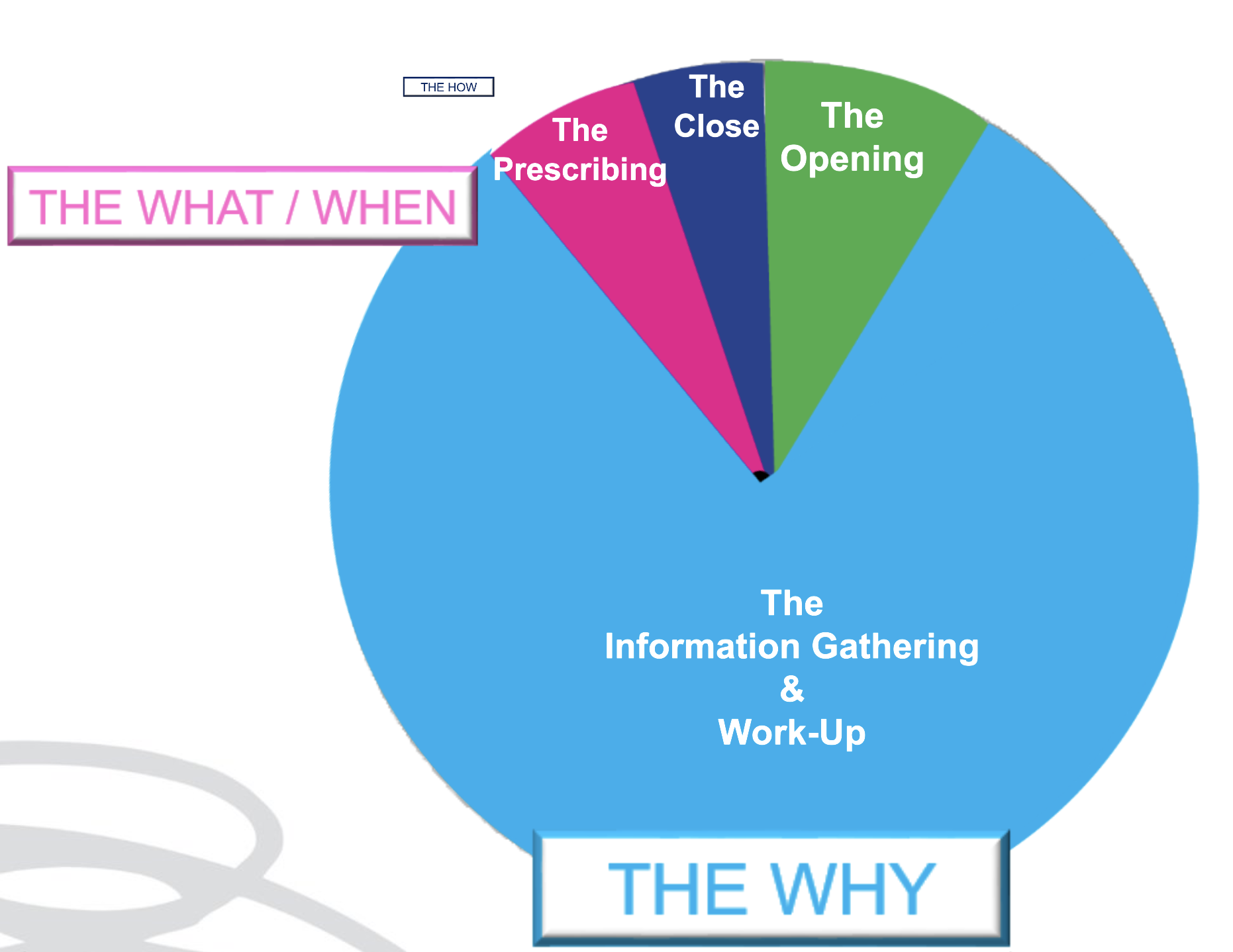
As an educator in integrative health, I have overwhelmingly been a peddler of knowledge and skills under the headings of: ‘WHY’ and‘WHAT’
Why – as in why does this patient present in this way, at this time. I am passionate about upskilling practitioners re our powerful contribution to the diagnostics & work-up of each individual. What – as in what changes (supps, herbs, diet etc) need to happen to correct for these very unique elements of imbalance in this patient to therefore aid resolution. We might label this, ‘personalised medicine’. But after so long in practice it’s patent that the best results don’t come from being the cleverest clinician nor the biggest biochemical brainiac. Knowing the ‘why’ and even the ‘what’, while enough for a minority of patients, fall short for the rest and can still fail to be truly about, & exclusively with, the most important person, in mind.
We’ve learned this before but it needs to be said again and again and again: much of any medicine is via the therapeutic relationship – and as part of this, our ability to PLACE the patient at the centre of their own SOLUTION. And therein lies the conversation we need to have in detail with them about the ‘HOW’ But how much time in your current consults is afforded to the ‘HOW’?
Being able to effectively negotiate with out patients the ‘HOW’ is an extension of Motivational Interviewing, Behaviour Change Theory & Patient Centred Care. It returns the humanity to our list of recommendations for each patient, pushing back against the autocracy that can tend to slip in with prescription writing. It powerfully reminds us that the prescription is only ever as good as the patient’s engagement & buy-in, and that’s only ever as good as our ability to write a prescription that is accessible & readily transplantable into their existing lives: to co-create with them Patient Centred Prescriptions. Someone in the audience had been my patient in the past – double awks right – because I absolutely know, I didn’t know this well enough back then. Back then when they were unable to do exactly as I had recommended – with their diet, their supps, their sleep, their work-life balance – they had, in turn, apologised for their ‘weakness’, ‘lack of willpower or diligence’ and me, being ever so gracious, accepted those apologies only to repeat the error of my ways and write yet more scripts that set them up to fail. 🤦♀️ I am committed to getting better at this and in this endeavour, giving both more attention & time in my appointments to the ‘HOW’ & yes I think we need to think creatively about how we use our appt time and between session touch points to achieve this – keen to hear about your perspective and experiences.
At the end of an information & insight heavy appointment, formulating a list of products and doses for our patients to take can feel like a bit of a ‘tada moment’, like a magician pulling a rabbit out of the hat. “Here is the solution – now off you go!” Research tells us, however, that treatment-plans that are a co-creation between you and your patient – evolving from a discussion that not only allows them a voice, but a major role in the decision making – are far more likely to succeed. While we are the authority on our medicines, our patients are the authority on what makes them tick & what’s likely to succeed, in terms of taste, texture, temperature & timing! This is called Patient Centred Prescribing and together with some other tips tricks and hacks I share with you in this episode, can really increase patient buy-in, compliance and therefore bring your treatment plan to fruition and fulfilment!
This is not about body shaming nor body positivity. I understand the crudeness of the body mass index, as a measure of (un)healthy weight – let alone (un)healthy muscle mass, so I don’t use this as a stand-alone assessment of weight, nor rigidly adhere to the categories it allocates individuals. With only minor recognised racial adjustments for BMI, I also recognise our concept of ‘healthy weight’ is incredibly whitewashed with minimal regard and consideration for clear ethnic and racial differences in physique. Patient’s lab results tell the real story. It’s in their results that we can discover someone is thin-on-the-outside-fat-on-the-inside (TOFI) or FOTI. These are patients whose BMI, WC,WHR, Body fat% etc identify them as obese – yet there is not a whisper of what I call ‘Adiposity Patterns’: no subclinical inflammation, no reduced glucose tolerance or actual IR, no raised transaminases that we expect to correlate with girth and the corresponding fatty infiltration of their liver. In this, as in so many other aspects of clinical practice, we are reminded to see each individual, individually.
AND if we adhered to this always, listening unfiltered to the whole health story and letting the labs speak, we would not miss those patients in whom unhealthy weight really is the most important underpinning, & all impacting, issue. And we are not doing our job, when we don’t.
I mean – we all know the detrimental effects of excessive adiposity – that’s like Pathology Unit 1 topic 1, right? I know we know it. Yet there are so many reasons why we might down-play, step-around, or even ignore its enormous contribution in our patient work-up and certainly the discussion that follows with our patients. That too is a no-brainer. Who wants to say to someone whose come seeking your help, as an explanation for their complex health concerns, ‘There’s no zebras here just a horse – one really over-weight horse!’ Knowing too that unhealthy weight results from the most complex constellation of factors (biopsychosocial) unique to each individual and that change in this health determinant, is arguably the slowest and hardest to sustain. But how are we serving our patients if we don’t?.
A practitioner presented this case of a 48yo F seeking help with the work-up: Self-reported inability to lose weight after 1st pregnancy = ‘obesity’ ongoing – now BMI 33.1 –> 25yo Reflux & Hiatus hernia Tx Omeprazole initiated – ongoing –> 26yo Depression Tx Venlafaxine initiated – ongoing –> 30s Back and other musculoskeletal injuries Tx Surgery & Opiates – ongoing –> 40s Hypertension & elevated resting HR –> Last 12mo – changes in Mx cycles suggestive of perimenopause & substantial weight gain
This patient didn’t ‘have’ any lab results but I think I can make an educated guess about how they would look and in particular whether they show the characteristic ‘adiposity patterns’ I mentioned before. What was my first thought about the most impactful element of the case? Obesity. What was my second thought? Where is all the weight (diet & intervention) history that would help us to understand how she is where she is, right now? We didn’t have any. The practitioner informed me that the patient was ‘not very interested in talking about her weight’ – in fact, according to her, it didn’t seem like losing weight was one of her goals. Now this could be several things: the fear of judgement, even her own self-loathing, the paralysing awareness of the enormity of such a goal, the dashed hopes of the past, or it could just be that her weight, as the key negative determinant of the majority of her health concerns & quality of life, has just never been brought to her attention, nor the connections explained to her in simple accessible language. So over to us, right?
There were other health determinants at play in this patient but the centrality of the adiposity was undeniable & the practitioner said this was the greatest take-home. She’d been ready to don some jungle gear and go hunting some zebras – but there was a horse right here in front of her and that could not and should not, ever be ignored.
What else became apparent was the lack of knowledge & skills regarding how to take a comprehensive weight history & why this is crucial. Not only for this type of unhealthy weight, the underweight require exquisite attention, as do those with a more labile weight than expected as an adult. This brilliant article by Kushner et al from 2020 is a total gift in that regard and a must-read for every clinician. We feel uncomfortable asking about certain things when a) a patient feels uncomfortable which is usually because b) we are uncomfortable and this ultimately comes from not being clear about WHY this information is so important and HOW this will ultimately enable us to better help THEM.
This is the very latest, comprehensive review of the key aspects of thyroid assessment that will revolutionise your understanding of thyroid markers. Gain a clear understanding of how to provide the best, most individualised, thyroid management by learning to read the real story in each patient’s pathology patterns. Boost your knowledge and confidence looking at TFTs, rT3, thyroid antibodies & related nutrient patterns, as well as AITD, environmental EDCs, HPA driven HPT issues, thyroid nodules, the impact of dietary macro- & micro-nutrient imbalances and much more!
This 4 part series provides over 10 hours of the very latest research & findings, punctuated with real case studies, that will both contemporise and deepen your understanding of all things thyroid, with a bonus recording on Adrenal Assessment.
How much? How often? When is the best time & timing? do you know about friends, foes and frenemies? Which form, when? e.g. building blocks or bioactives? And for how long? aka are we there yet…?
These are the kind of questions that one would imagine nutritional prescribers can always answer – but can you? Yet this is the goal, right? So that with each and every unique individual who needs supplements – we have a clear, consistent go-to framework to guide & direct these prescriptions. One that makes scientific sense, offers optimal outcomes and removes the uncertainty.
From my interactions with thousands of practitioners, however, I know many of these key questions plague practitioners & they feel, at times, as if they’re flying without a net, or without a strong systematic approach, or at the very least without all the answers to these questions.
I’ve had so much good fortune & so many others to thank for providing me with this foundation. Fay Paxton – my nutrition lecturer in my under-grad who indoctrinated me with a systematic approach. Dr. Tini Gruner – my principal supervisor at SCU, who shared & further fuelled my passion for biochemistry and reading labs to extract insights into each individual. And thanks also to all the pharmacists I’ve delivered education to over the years, who, as a result of their grounding in the principles of pharmacokinetics, always ask the best questions – questions that if I don’t know the answer I know I need to know the answer! So I made it my mission to find out!
While we dip into these aspects of nutritional prescribing in our regular mentoring groups on an ‘as needs’ basis, I’ve decided the time has come to create a year-long program dedicated to sharing this information and building this skill-set in practitioners.
This monthly meet-up is delivered live (max 1.5hr) and runs from Feb to November with the following currently proposed format *subject to change dependent upon the needs of the group
Feb Factors Affecting: digestion, absorption (host, form, dose)
March What happens to what gets left behind? e.g. enhanced enterocyte micronutrient concentrations & their effects plus unabsorbed nutrients & their interactions with the colonic environment
April What happens to what’s absorbed e.g. distribution, hierarchy of needs, activation and deactivation
May The pharmacokinetics of prescribing
June Where do our ideas on dosing come from? e.g. Physiological Vs Pharmacological dosing & actions. The basis & believability of maximal intake boundaries?
July Bioefficacy V Bioequivalence. Beyond building block nutrients: Is ‘Bio’ (-active, -peptides, -materials) always better? e.g. GABA Vs Glycine, NAC Vs GSH, PLP Vs Pyridoxine, Niacin Vs Niacinamide riboside ——————————————————————Aug month off—————————————————————————
Sept How often & for how long? Are we there yet? And how would we know? Plus Fast Vs Slow Nutritional therapeutics
Oct Strategies for Supplement Success e.g. friends, foes and frenemies in nutrition underpinning principles with examples; compliance changers for clients
Nov Live attendance & opportunity to participate in a case-based mentoring session
This monthly ‘live’ meet up will be delivered as part of 2023 Group Mentoring as The Nutritional Prescribing Program Group Mentoring applications open 17 October 2022.
To join the waiting list and be notified when applications are open, email the team at [email protected]
Find out more about what groups are available for Group Mentoring in 2023 here.
Have you been told somewhere by someone that the ‘perfect’ TSH is 1.5 mIU/L? This is a wonderful, terrible & wonderfully terrible example of ‘magical numbers medicine’. As a push-back against the published reference ranges we’re given, that are so wide you could drive a truck through them, there has been an over-correction by some, leading to the myth of ‘magic numbers’. We can narrow the reference range substantially for many parameters with good rationale, make no mistake about that but once we start setting ‘aspirational goals’ that are explicitly rigid…well we’ve done 2 things 1) forgotten about the patient to whom this result belongs and 2) disregarded viewing each result as part of a ‘pattern’, that we must piece together and make sense of.
Back to TSH then… if my obese patient had a value of 1.5 mIU/L this in fact would be woefully inadequate – so too a child at any weight.
And we expect a higher value as well in our elderly clients too and this level there may be, in fact, increased mortality.
But the same result would be excessively & worringly high in my patient who’s undergone thyroidectomy.
Realising the full value of any test result in terms of what it reveals about the person sitting in front of you, requires these more thinking and more thoughtfulness. Unfortunately, a list of ‘magic numbers’ will often lead you astray. And building your scientific knowledge about labs will not only help you avoid the pitfalls of pathology but will strengthen your pathophysiology prowess in surprising ways, saving your patients a packet in terms of additional extraneous testing and help you truly personalise your prescriptions…because the ‘invisible (biochemical individuality, oxidative stress, genetic probabilities, subclinical states, imbalanced or burdened processes etc) just became visible’. I started requesting lab results early in my career and years later was lucky enough to be taken under the wing of Dr. Tini Gruner. I found some of our shared notes, from 10 years ago, scribbled all over patient results recently and I was struck by just how lucky I was to have her encouragement to really pursue my interest and how she was a guiding force about learning to recognise pathology patterns over single parameters. A decade on I can concede, much of my clinical and educative success has come off the back of this foundational skill-set and I know, this is true for so many I’ve taught too.
“The guidance I’ve received over the years from Rachel in relation to pathology interpretation has been one of the most valuable (and fascinating) investments I’ve made as a clinician. Her teachings have filled gaps in my knowledge base I never knew needed filling and have significantly enhanced my understanding of the inner workings of the body! Rachel has an incredible ability to make the numbers that patient’s so often present us with, both understandable and clinically meaningful. The knowledge I’ve gained by investing in this skillset has paid off in dividends and I’m certain will continue to do so into the future.”
Stacey Curcio – Cultivating Wellness
I hope you’ll join me for the most exciting up-skilling opportunity in learning labs yet. Oh…and all this talk about thyroid testing..this next MasterCourse series is focused on revolutionising your understanding of thyroid, adrenal, HPT & HPA markers based on the very latest research & findings & marry these together with everything you learned in MasterCourse I (ELFTs, FBE, Lipids & Glucose) to understand the ‘whole story’.
…an absolute treasure trove of free integrative health information about your patient!
DEEP DIVE INTO REAL CASE STUDIES TO DEMONSTRATE EACH PATHOLOGY PATTERN IN ACTION. ]\
There are limited places. To sign up for Rachel’s LIVE Series – MasterCourse II: Thyroid & Adrenal Diagnostics and for more information click here.
13 years ago I was first asked to contribute to ACNEM’s thyroid training 8 years ago I put together a little Masterclass on Diagnostics & 6 years ago co-created another one on Thyroid 2 years ago I dived deep into new literature to update my ideas & my teaching for ACNEM again & reinspired by all I had discovered 1 year ago I promised a new MasterCourse, for all those eagerly awaiting the next instalment: Thyroid & Adrenals Now it is about to land!
Across this time I have fallen in and out of love with this topic. ‘In’, in the early heady days of learning some great tricks and tools, ratios and relationships between thyroid parameters (T4:T3, rT3:T3 etc) to aid interpretation but then ‘out’, when I discovered in my own patients and many others, that while this solved some thyroid patient puzzles, it left the curlier ones with questions remaining. I became unsatisfied with the simplistic stereotyping of the thyroid hormones (T3 important & always good, T4 not, rT3 never) and frustrated by the misapplication of ratios & lazy labelling of the thyroid as the ‘problem’. All of these things I intrinsically knew didn’t make good scientific sense and actually revealed a lack of depth in mine & our understanding. So I re-immersed myself in the very latest research and, wouldn’t you know it, in the time between there’s been a mini-revolution taking place in relation to our understanding of the HPT axis and the other endocrine circuits that manage it! Thank goodness for science!!
As a result, not a slide, possibly barely a dot-point remains from what I wrote back in 2009 and not a great deal more from 2015 even.
That’s how far the research has revolutionised my ideas & understanding.
Some of the assay techniques & technologies are new, there’s a river of research & a mountain of meta-analyses published in the time between & I have had the privilege of innumerable more clinical encounters in this space, to really nut out how all this translates into the real world. And most importantly I can confidently say that this training and teaching reflects the truly integrative nature of psychoneuroimmunoendocrinology…did I just make up a word?! Basically, if you think that the hypothalamus and/or pituitary is the boss of the thyroid – we need to talk! There’s a lot I need to catch you up on.
So like our first MasterCourse in Comprehensive Diagnostics earned us a reputation for, we are going to leave no stone unturned – no difficult question – unanswered, like…
Can you list the critical roles in health of T4 that are independent of its precursor potential?
How about rT3 – what are the important health implications for us if we don’t have enough?
When shouldn’t the T4:T3 in the plasma be approximately 3:1?
When and why would a drop in TPO & Tg antibodies signal progression not remission of AITD?
In the absence of imaging, can you still be confident that thyroid nodules are the most likely differential in your patient?
What is the one test result that differentiates between Euthyroid Sick Syndrome and Central Hypothyroidism?
Exactly how low in Selenium, Iron or Zinc do you need to have a measurable impact on thyroid hormones and function?
Who escapes from the Wolff-Chaikoff effect and how long after iodine dosing can we be certain?
So stay tuned… and watch this space! We thank you for your patience and know it will be worth the wait…
“Absolutely loved this course, I’ve listened to each of the recordings at least 3 times now taking furious notes and am still picking up new gems. Love that it’s helping me build up my knowledge and confidence in such a fundamental area of practice. The case studies are super valuable as they bring the labs to life, I’d be keen for more of these! Really appreciate all the extra PDFs / audios that have been added also. Eagerly awaiting MasterCourse II” – Naturopath | Australia
“Why wasn’t this content covered in medical school? As a psychiatrist, I have greatly benefited from attending this course which comprehensively covers the ins and outs of interpretation of pathology labs and how this applies to clinical cases – many of which have both physical and mental health considerations. I believe all doctors from general practitioners to specialists will gain from attending! ” – Psychiatrist | Australia
“Thank you so much for this course, it has been brilliant. It has ‘fuelled my practice’ and many people have benefited already – from such insights. It’s quite thrilling!!! I’ll definitely be signing up for the second course later next year” – Naturopath, Medical Herbalist | New Zealand
I’ve spent the best part of about 4 months recording my *NEW* Advanced Thyroid Assessment training. I told my team this would be easy and quick, given it was to be based on a great little 2-part, 2hr updated presentation I delivered just last year for ACNEM!! Sixteen weeks (like seriously…most of it) numerous rewrites and retakes later, our final product is 4 parts that goes for over 12hrs in total & has a bonus Adrenal recording! And yeah my team are impressed but unimpressed too if you know what I mean?!🙄🤪
Every time another, ‘Oh wow!’, or ‘No way!’, escaped my lips, it was a source of personal celebration, as another deeper layer of learning revealed itself.
But to the wonderful, somewhat weary and definitely wary Sally, who does all my powerpoints, it was met with, ‘Oh boy!’, because it meant many multiple new slides to build full of visual metaphors, animation acrobatics, if not an entire new Part!*#@^
Her sage advice along the infinite research road I’ve been travelling was : ‘Stop. You’re going to have to stop.’
So I didbut now I am this meme. Everything I see currently through the lens of thyroid health, I talk in tongues TFTs and my brain is one giant neural network of integrative endocrinological circuits! I have fallen in love with this topic, this neuroendocrine axis and its ‘first responder’ role all over again! Hence our little thyroid character below – all ‘antennaed’ up – is one of the many tools we’ve developed for this training, to teach us that ‘bad thyroids’ per se are extremely rare – but bad scenarios are common (too much or too little of any macronutrient, key micronutrients, a change in the internal or external environment etc etc) and this little fellow and his board of directors (no – not the hypothalamus or pituitary!) – well it’s their job to ‘read the room’, right?!
In the absence of this key understanding we risk: A lot of lazy labelling in thyroid health – ‘You have a bad thyroid – that’s why you…[can’t lose weight, feel tired, have SIBO etc]’ Misdirected treatment & especially a tendency to overload the butterfly with ‘thyroid’ nutrients – which can do more harm than good
I’ve said many times, ‘perfect number pathology is a myth’ but it runs rife in practitioners’ beliefs about TFT results with complete disregard of the person those labs belong too! Did you know, for example, that your TFTs should all be higher if your BMI is? That your T4:T3 ratio should never be 3:1 if you are on replacement, have hot nodules, are pregnant or are acutely unwell etc etc etc? How about how low your Selenium or Iron levels need to be before this factor will influence the actual levels of thyroid hormones measurable – & what the impact of these deficiencies are well before then that is far more sinister and serious? Yep…you see here I am, pouring just some of the tiny take-homes of Advanced Thyroid Assessment ALL over you!
Watch this space my new Thyroid training is just around the corner!
An increasing number of our patients have thyroid concerns but unbeknown to many of us the most likely explanation of all is thyroid nodules, whose incidence is on the rise globally. The development of nodules has always been primarily viewed as a nutritional disease. Traditionally attributed to chronic iodine deficiency but recently novel nutritional causes have emerged. Benign nodules come in 2 flavours: hot and cold and while patients can present with a mixture, it is the presence or absence of a hot nodule that radically changes what complementary medicines you can and can’t use and what an effective treatment plan looks like. The pointers, as is often the case, are there for us in the patient’s presentation and pathology, so knowing the difference is no longer a guessing game. This UU30 comes with a great visual clinical resource and includes key papers on the nutritional management of nodules.
Are we doing ourselves out of a job? I’ve been talking treatment plans with my New Grads recently. Given, only recently these were major assessment items in their clinic units, they have been trained to create ALL-ENCOMPASSING (biopsychosocial) prescriptions and recommendations of utterly EPIC PROPORTIONS – to simply prove they know it all. Problem is this doesn’t work in the real world.
Emailing your client multiple pages of advice that covers: a whole sizeable supplement schedule that only a military-training could nail (2 tablets 1 XTID 1 X BID, a liquid, a powder, some with food, some definitely not with food) plus dietary advice, plus hyperlinks to exercise advice, mindfulness exercises and a request for follow up investigations before the next appointment…is…a L*O*T!!
It is also ineffectual – because it completely disregards the human on the other end. Let me ask you this, how much change are you capable of between a first and second appointment, roughly a period of 2-3 weeks? Personally, I gotta say not that much. It took my dentist years to get me just embrace flossing & I don’t think I am an exception! With all the knowledge we possess its hard not to see people as (a long list of) problems (& problematic behaviours) that we translate into, and solve via, a prescription.
Effectively we are saying to patients with this practice model, ‘Go change & come back when you’re done & then I’ll probably ask you to change some more!’ That’s both a big ask and a huge missed opportunity.
I hear from reliable sources over the ditch, that GPs are increasingly referring their patients to, or teaming up with health coaches, rather than naturopaths. Given what I’m observing, I get it. Doctors on the whole only have time (and barely then) for a finger-pointing prescription – certainly not the time and touch-points required to actually support patients with the very difficult thing that is, behaviour change. Nor the skills to truly facilitate patients making the necessary and desired changes – so they outsource this role. But we shouldn’t.
After all – I want to be on my patients’ support bench & health care team always – not a flash in the pan, that blinded them with science or my ‘smarts’ and proved to them in one over-stretching prescription – that naturopathy is not for them, or at least, they’re not fit for the task.
At the end of an information & insight heavy appointment, formulating a list of products and doses for our patients to take can feel like a bit of a ‘tada moment’, like a magician pulling a rabbit out of the hat. “Here is the solution – now off you go!” Research tells us, however, that treatment-plans that are a co-creation between you and your patient – evolving from a discussion that not only allows them a voice, but a major role in the decision making – are far more likely to succeed. While we are the authority on our medicines, our patients are the authority on what makes them tick & what’s likely to succeed, in terms of taste, texture, temperature & timing! This is called Patient Centred Prescribing and together with some other tips tricks and hacks I share with you in this episode, can really increase patient buy-in, compliance and therefore bring your treatment plan to fruition and fulfilment!
We all (inaudibly🤞) sigh when patients utter this & adopt the brace position for whatever mis- or dis-information may follow.
So how would you feel, if instead, these were the words of the health professional you’re seeing?
We could debate forever the pros and cons of FB and its forums – & indeed it offers both – but one thing we must never lose sight of is what it has in common with the ‘wild west’: unregulated, unvetted, and with plenty of cowboys – often sadly, masquerading as experts, or just ‘very “generous” very very active group members’, with hidden agendas. I don’t generally engage with the naturopathic forums but occasionally I catch sight of things that I can’t look away from, and I can’t not speak up. Recently, someone (with a not-so-hidden-at-least-to-me-agenda) was raving about the dangers of N-acetylcysteine as a supplement & the way it was spoken about made it seem like it would be *poison* at any dose. Wha? As you may have learned from me it is definitely potent and in turn, demands our respect as a powerful therapeutic agent – directing our decisions about timing and reminding us, yet again, that least dose is best dose. But what this individual was purporting were adverse effects I’d never heard of in relation to this nutraceutical. So I simply asked, ‘Can you please share your reference(s)?’
Prior to me inserting myself into the comments – there had been enormous engagement specifically with this individual’s claims- which mostly went like this: ‘Oh wow! I didn’t know this!!’ ‘Thank you – that’s so interesting!’ “Oh that explains why Tom doesn’t like it, and Dick won’t take it and Harry says it’s horrible!” 🤦♀️
FB forums – seeking out the support & opinions of our peers can be truly wonderful but it can totally derail our knowledge too if we don’t keep checking the quality of that information. A simple: Can you share your references, or, where did you learn this? Should be part of the respectful and expected scientific discourse in our profession. I’ve asked that before when I’ve found myself yet again in a forum thread and had a truly fabulous response – with the practitioner generously sharing a number of high quality published articles that would have taken me ages to find myself! 💪Not the case in this recent episode. The 3 distinct claims, which all centred on NAC being bad for high histamine individuals, were ‘substantiated’ by just 1 primary reference & that was a Poster Presentation: “Human placental tissue was minced and subjected to a fractionated ammonium sulphate precipitation (35% / 65%). A fraction high in DAO activity was purified using hydrophobic interaction chromatography (HIC), and incubated with the drugs in prescribed concentration” . The full research has never actually been published in its entirety and the brevity of detail on a poster means you know barely any of the important details regarding the methodology. I also looked for any other research that emulated these methods or findings or even cited this paper – nada. And if you lead with your best – this was appalling low level evidence that is really unlikely to be relevant. But hey – here’s the 1 provided reference – make your own mind up! (see how easy that is?!)
I asked for clarification and for papers to support the other 2 claims. Silence.
But actually before silence a bit of ‘How dare you ask!’
That’s when I got a different insight into this forum & arguably a culture that doesn’t foster curiosity & questioning, if that risks challenging the ‘poster’s’ position. And when several incredibly intelligent, kick-arse clinicians quietly contacted me on the side to say, ‘THANK YOU!~ This person posts comments like this all the time & it’s so misleading & someone needed to say something, but it probably had to be you.’ Well that really made me 😥 because it didn’t, you know – any one of us can ask, “Can you share the reference(s) for that?” and clearly we need to more often 🤓
Why are we afraid to question information or ask for references and why are people afraid of the question? This should not be a competition or hierarchy of who can ask or not ask questions. And if the forum that you’re a member of makes it seem that way – then ask yourself, if its doing you more harm than good.
Aren’t we on the same team here? We all have a professional duty of care to our patients to ensure that in looking for quick answers we don’t get incorrect ones that misinform us, our patients and our treatment decisions.
Over years of delivering independent education in integrative health I have spoken to some diverse audiences. This has included health professionals from very different backgrounds: from hospital-based psychiatrists & mental health nurses, to whom I presented on site in hospitals both in Australia & NZ, to a national sparkle-arkle speaking tour, in front of large groups of aesthetic practitioners. They’re the doctors & nurses for whom botox and fillers are their tools of trade, and yes I got to see actual demonstrations of their work performed live!!!😶 More recently, I’ve had several opportunities to deliver evidence-based independent education on nutrition to pharmacists en masse – which I always enjoy because they ask some of the best questions!
Underpinning each decision to accept an invitation from a 3rd party, be that a company an organisation or an institution, to speak, is: 1.The realisation of an opportunity for nutritional medicine to reach more people, a wider audience, & ultimately expand the circle of influence amongst health professionals, who interact with & advise the public at all different levels 2. An agreement and/or contract that ensures my independence, the correct use of my materials, image, brand and IP & removes any expectation to promote their products/services etc
And my ‘door’ is open to any invitation which meets these 2 criteria. So you might have seen my name, previously associated with some brands or organisations, in the last few years disappear off their speaker announcements, or no longer connected, and in turn you might see my name pop up in new places! Like….Metagenics Congress on Autoimmune Disease!! After many invitations from this company, that I wasn’t able to previously accept, I am pleased to be speaking at this face to face event on the Gold Coast in August. What a novelty, hey? Face to face?! My talk is about the 4 Mistakes not to Make in Hashimoto’s and as always, I’ve completed a full mini-literature review in order to speak to the very latest on diagnostics and nutritional management, in this condition. Yes, to quote a Costanza, “We’re back baby, we’re back!” And to see my full current smorgasbord of speaking commitments & all the people I am ‘spreading the (nutritional) word’ to – just click here.
This previous training will take your understanding of the interplay between food, nutrition, environment and the thyroid several steps further. With more supportive research and a greater focus on the mechanisms behind the relationships between these macro- & micro nutrient & environmental factors, this presentation is for the true thyroid die-hard.
I’m ready to zip my lips 🤐 and ride off into the sunset of silly season. But first I wanted to tell you about the BIG PLANS we have ON THE BOIL! Noticed a bit of a thyroid theme of late? Last month I presented training in thyroid assessment for the 4th time for ACNEM but not a slide, possibly barely a dot-point remained from the original one I wrote back in 2009. That’s how much my ideas & understanding have changed.
Some of the assay techniques & technologies are new, there’s a river of research & a mountain of meta-analyses published in the time between & I have had the privilege of yet more clinical encounters in this space, to really nut out how all this translates into the real world.
There’s a lot I need to catch you up on. And as I start creating our new MasterCourse II in Comprehensive Diagnostics…which will include 🥁…you guessed it…the humongously hardworking HPT, I’m just about bursting at the seams! And will those four little friends of every good practitioner, that sit superficially atop the ‘butterfly’, make it into our MCII?? I hope so because a) they should be our besties – being the director of Ca Mg D & P regulation and b) research tells us that where we find, ‘thyroid’ dx we should have another good hard look for ‘parathyroid’ dx and vide versa and c) over the last few years it has become increasingly apparent to me that this is one incredibly common source of ‘medical mysteries’ in our patients – remember the ‘Bones, Stones, Abdominal Groans & Psychic Moans’ catch-cry? Yep, that’s the patient who typically finds their way to us, with pervasive but hard to pinpoint gut issues (often misdiagnosed as SIBO, FGD, IBS -D or C), some significant stress perhaps even depression and insomnia and, if someone bothered to look, premature bone demineralisation. What other pathology panels and parameters will we be able to squeeze into our MasterCourse II?
Our current plans are to deliver the MCII live from May but just a reminder, because this next instalment assumes you have the exquisite foundational knowledge we laid down in the MCI – this is a pre-requisite for attending the MCII. So if you’ve been putting off your pathology apprenticeship now you have a hard deadline to work to!
And finally the last, last words. On topic because they came from someone who specialises in thyroid, did the original thyroid training with me, way back when, and last month was my fellow presenter & panellist on all things thyroid for ACNEM:
I’m sure I’m the 1 billionth person to reflect this back to you but I’ll do it anyway because I think we all need reminders sometimes – you have a truly special gift in critical thinking, discernment, and most importantly passing on complex knowledge in a very digestible way without making anyone feel silly for asking questions or not getting something the first (or fifth time…no, just me?). The endless analogies are a teaching tool you’ve well and truly nailed and boy am I grateful because it speaks to my way of learning very well.
So, a big thank you! Endless gratitude for your brain, passion and generosity with your time/knowledge/resources. Natalie Douglas
Here’s to another great year of learning, teaching, sharing & mentoring in 2022 – 1 billion and counting I hope 🌟🌈😂
Maybe it’s tax-time, just my wintery whinge or a tirade triggered by missing my twins’ 21st birthday due to border restrictions 😶 butI’m sorry for all the shouting of late…about interpreting iron studies, about the copper misinformed etc etc. and my gorgeous new grad mentees copped a full monologue, with links to articles, recordings & the Coeliac Society, when they asked me to expand on why we must exclude coeliac disease before removing gluten from anyone’s diet. I was so glad they asked though! I’m now using my inside voice.
But I don’t want my message to be misdirected and I fear it might be. It’s not you and it’s not me
‘We’ are doing our best. We are working in a field that demands us to be across soooooo many domains of knowledge and information, from the basic & not-so-basic medical sciences, to pathology interpretation, nutrition, herbal medicine and beyond. It’s a lot. None of us are across it all. I’m certainly not. And I’m aware, that the frustration I feel at others’ misunderstandings sometimes is unfair, because I’ve benefited from excellent early teachers all the way through to having a job now, that keeps my head in the research daily. And even still, without a doubt, the gaps & shortfalls I observe and criticise in others, I could have made of myself, earlier in my career. We don’t know what we don’t know, until we know better, right.
It’s them
Who is this ‘them’ of which I speak? Well, 25 years ago when I completed my under-graduate (and walked 10 miles to school in the rain, without shoes or breakfast 👵) I believe I received the training required to be the naturopath that I needed to be. Safe, effective, knowing my scope – which was basically coughs. colds, atopy and risk mitigation for future chronic disease. I never saw a lab test during my under-grad. I would have read a set of iron studies badly and something like ELFTs, like it was Latin. I wasn’t made aware by my lecturers of the critical part I could play in my patients’ lives, either by advocating and advancing correct diagnosis or by obscuring, confounding and delaying it (sorry, still thinking about the gluten debate!). But back then, I think this was appropriate for the time, the state of play of our collective medical knowledge and for the role naturopaths were playing in the health landscape. Not any more.
If you haven’t had a chance to read the extensive research about ‘us’ (Australian nats, nuts & herbalists) published of late, who we are, what we do, how we are viewed and what our patients expect, then you could be in for a surprise.
We’re perceived by many, if not most, of our patients to be a primary health care provider – either flying solo or co-piloting with the patient’s GP (& no auto-pilot function!!!) and as clinicians for chronic comorbid cases not the acute cold. My how times have changed and the question is – has the knowledge and level of competency of those in educational roles & the quality of what they deliver a good fit? Sorry, but if the majority of a large new graduate cohort have left their training with a mantra of ‘we must not diagnose’ and INTSEAD are likely to advocate a gluten free diet RATHER THAN Coeliac testing with the patients doctor first – then we’re falling at the first: Primum non nocere. Sorry,I forgot, inside voice 🙄🤐
This Update in Under 30 recording speaks to the seriousness and primacy of identifying Coeliac Disease in any patient reporting a suspected reaction to gluten and takes you through the latest evidence on the best screening protocol. With an increased understanding about the strengths and limitations of gene testing, serology and biopsy, we have a clear map to follow now. Along the way Rachel outlines 3 additional potential mechanisms for ‘gluten’ reactions amongst our patients, what to look for and how to tell the difference.
I stand on the shoulders of my elders. [I hope it’s not too painful for them, it’s been going on a long time now!!] And I regularly lean on my mentors – who are often my peers, practitioners specialising in areas different from mine. I recite their names often like a little mantra in our mentoring sessions: Kate Worsfold, Dawn Whitten, Tini Gruner, Michael Hayter, Jason Hawrelak and a few others that are on high rotation like ‘Rhiannon-repro’ Hardingham and I feel this is important to reaffirm that learning is lifelong for us all and to make clear the passing on and around of knowledge in our profession. There’s been a long history of honouring our history, so to speak, in naturopathy.
My training definitely acknowledged, paid homage to & revered elders past and present & while I’ve never been one to participate in the making of herbal preps by a full moon, at solstice, in a field somewhere, in the company of said herbal elders (you know who you are!!)…
I do try to continue & foster this important collegiate quality of our professional community by reciting the names of the saints source of clinical pearls I have been given so generously by others.
Lately, I’ve been wondering if we’re losing this tradition. I’m hearing practitioners present concepts as ‘theirs’, ‘develop’ & distribute teaching tools ‘adapted’ from others work, parrot identical ‘catch-cries’ even, with no mention of the origin, the source – even the inspiration. Now perhaps I am showing my age, reflecting a very different time in naturopathic training when we were so fortunate to be taught by some of these amazing (solstice honouring, field dwelling, herbal making) elders, but even by today’s standards and the dominant EBM model, surely every emerging clinician understands the need to cite their sources?
The green tea & lactulose intravaginal wash recipe I use and frequently share with mentees always comes with the prelude – “I got this from Gould’s” The tips on testing tools in mental health, I propagate like mad, has the epilogue – “All that I know, is because Kate taught me so!”
Of course I say more than I cite (otherwise the sessions would be impenetrable!) but I like the way it helps us all to see we are a part of something bigger.
I have! And just recently a stark contrast between the results from 2 different methods of cortisol capture in the same patient illustrated just how likely this is. How do we ‘capture’ something so ‘dynamic’ and interpret anything of substance from a ‘static’ assessment technique? But rather than throw up our hands and throw out the whole attempt to measure cortisol, we can improve the rigor, reliability and real-world meaningfulness of our patients’ results by refining our timing of tests, choosing the medium wisely & manipulating test conditions to answer specific questions about their HPA function. Great ready reference resource included!
If you’re already an Update in Under 30 Subscriber – go directly to your Active Content…it’s already there!
If you’re not and want to improve the accuracy of your Cortisol Capture in patients gohere!
Well, obviously(!)…this has been a year heavy on pathology interpretation for me and the huge number of practitioners who’ve just spent the last 6 months taking that learning journey with me. I celebrate and congratulate them all for their commitment to their own professional development and also their investment, in what is arguably, the most potent yet overlooked set of skills of any health professional… the ability to read bloods. Basic bloods. Mainstream labs. No…but to really read them. Backed by all the scientific understanding about what these parameters actually are, how they perform and what they (dis)prove e.g. subclinical inflammation and ramped up oxidative stress – not an informed guess but mappable…right there but where no one else can apparently see it! But I digress!
Actually what I wanted to discuss was the whole erroneous notion of ‘normal’.
No, I am not speaking from the heart about my personal quirks, sense of humour or dress sense but rather the incorrect assumption that a reference range defines ‘normal’ and that our answer for each patient and each result is, a Yes or a No!
In this brilliant article by Whyte & Kelly published in the BMJ they spell out this falsehood succinctly. They note that the term ‘normal range’ has slipped into medical language from the misunderstanding that all lab results follow a Gaussian (aka bell shaped curve & later referred to as ‘normal distribution’) pattern but many simply don’t. So for some parameters a result near the ‘middle of the reference interval’ constitutes aspirational whereas for others it spells danger. Add to this, that these reference intervals are mathematically determined to reflect the expected values of 95% of your patient population (mean +/- 2 SD either side) so…that means the chance of a YES…”Your patient’s results are ABNORMAL!”… is just 5%. And hey…who said all the values within the reference range are all equally “normal” or better yet, healthy?! Not these authors, nor I, nor the praccies who’ve just done our course. So while, in many regards, these goalposts are too wide, they are also too narrow – typically only representing a subset of adults age-wise and Caucasians, yes they are both ageist and racist (yep, I said it!). And if our practitioners have learnt anything it’s about keeping an ol’ eagle eye on the sneaky intra-individual shift! Only spotted, of course, if you know your patient’s normal (not theirs compared to anyone else…just theirs) and then spot a shift. [I can hear they’re shushing 🤫me…they’ve got it already, alright!!]
So this is music 🎻to my ears, from Whyte & Kelly: “The intraindividual variation in laboratory values is usually much smaller than the interindividual variability (ie, the variation in the population). Variation in the concentration of an analyte, if significantly outside of a patient’s usual values (but still within the reference interval), could be a sign of early or latent disease”
So if you want to tap into the power of pathology…start with Whyte & Kelly, maybe even dip your pinky in the pool by checking out Accurate Pathology Results Interpretation Starts Here – an easy little 1.5hr kickstarter…or jump right in the deep end with the rest of us pathology reading polo players and sign up for the MasterCourse 1: Comprehensive Diagnostics for some DIY summer fun 🌊
ps I know your type and know that is EXACTLY the kind of weird nerdy thing you have planned for your break…you should see my summer fun list!!! 😅
MasterCourse 1: Comprehensive Diagnostics is a self-paced online program due for release in December. The course has pver 18 hours of video presentations plus 2 free bonus sessions 1) Accurate Pathology Interpretation Starts Here and 2) Patient Pathology Manager and access to resources and tools within, for your own use. This is a pre-requisite for MasterCourse II that will be delivered live in 2021.
This skillset has been found by many to be biggest ‘game-changer’ in Integrative Health You can view the full course outline here.
We are getting ready to launch our new look Group Mentoring for 2021! We are now counting down the weeks days (gULp!!) until we open up applications for Group Mentoring next year. We’re keeping everything our practitioners have told us they love, over the past 8 years, and simply improving the formula, with some great new bonuses for 2021!
So with 2 weeks to go, we’d thought we’d introduce what’s on offer.
Live sessions are starting in February for 2021. January is often a period when we’re recovering from ‘recovering’ e.g. Christmas holidays, so we thought it would be good to start a month later this time around, in February when everyone’s recharged and ready to get back in the swing. There will be 10 live sessions in 2021 starting Feb and ending November.
Fly on the wall options on offer! Want to present a case? Great! Not ready or have enough time to present one? Great! Having successfully launched the ‘fly on the wall’ (non-presenting participants) experience this year we’ve been left in no doubt that practitioners loved this & continued to learn just as much as those in the ‘hot-seat’. Hence, it’s back again!
BONUS: Update in Under 30 Subscription is now included for those in General Group Mentoring (GM1 or GM2), either of our Mental Health Groups (Primer & MH Applied) or to those in our MasterCourse Alumni (not included for New Graduates)You gain access to the ENTIRE back catalogue of Rachel’s UU30 recordings (30 min podcasts), with atotal value of over $1800, and receive a new podcast each month for 12 months. For those mentees who are already current subscribers, when your subscription expires in 2021, you’ll get to renew for free! This provides you with even more of an opportunity to drill down and dig deeper into certain areas that we routinely come across in our session cases and content. This gives you a much greater opportunity to seriously expand your learning in those areas most relevant to you.
We’ve broadened your 30% discount to ALL Rachel Arthur Nutrition products on our website for 2021.
Certificate for CPE Hour
Here’s what one of our mentees had to say this year…
“I’ve listened to the recording of the live mentoring sessions multiple times and sooo sooo much goodness in each session. I love how your mind works Rachel. This is also my second year in mentoring and I am so grateful for this safe space to continue to enlarge our thinking. I learn something new every single time. I am also loving the update in under 30 – that is also changing my practice with every single listen. Eg the ones regarding interpreting iron studies and prescribing. TOTAL GAME CHANGER. I was a novice in iron prescription kind of going with whatever my patients Dr’s were prescribing but then understood why they were getting such crappy results – both in actual improvements in their iron test results but also negative symptoms. Honestly, the combination of mentoring with the little individual nuggets in the updates is totally transforming my practice so I’m so grateful. Rachel please keep mentoring forever. I love it.” – Bek DiMauro, Functional Nutritionist, Adelaide
We have a great range of groups to choose from. Whether your a nervous newbie or have 15+ years experience…
General Group Mentoring – our regular case presentation groups, with one practitioner presenting a case each month, or just listen in.
New Graduate Groups – great opportunity for New Grads to build confidence as they leap from student to practitioner, or for practitioners wanting to refresh their core clinical skills such as MindMaps, Pathology, Case Taking etc
New Grad Next Level group – for graduates of the New Graduate 2021 group to continue to build on your skills and apply all the great learning from this year to real client cases.
Mental Health Primer – topic based tutes & interactive sessions to build on your knowledge in the role of naturopathic medicine in Mental Health – from screening tools to key management issues, specialist diagnostics and beyond.
Mental Health Applied – practitioners presenting their client cases with a focus on primarily Mental Health presentations.
MasterCourse Alumni Monthly – NEW for 2021 – Participants from this year’s MasterCourse In Comprehensive Diagnostics can continue to build on their knowledge and application of Pathology interpretation with this Live monthly session and online community.
For all those Mentoring Virgins 😇out there wanting a clearer understanding of what it’s really like to be part of my group mentoring, this video is a little snippet from a session with one of my groups. This year has flown by and I have thoroughly enjoyed working with each fabulous group of dedicated ‘life-long learners’.
And don’t forget some of the offerings our Group Mentoring already reliably provides – the high level of applied knowledge, our incredible Basecamp platform for communication and support between sessions and our ongoing sharing of pearls of knowledge from my 22+ years of experience and research together with the collective wisdom and know-how of each group.
Can you see yourself in this collective?
REGISTRATIONS OPEN 9 November!
Information on how to apply will be released soon, to find out more click here. Join the waiting list now so you won’t miss out by sending us an email on [email protected].
As a health practitioner, you are always actively building: your reputation, your practice and your knowledge.There’s theoretical …and then there’s applied. Some of the biggest leaps we take forward as practitioners come with being shown how (rather than told) & then being forced to ‘do the work’ ourselves, rather than being exposed to simply more information, be that about pathology, patient prescriptions or practice structure! The slogan ‘Just Do It!’, might have already been nabbed and TMed by a huge corporate beast, but this doesn’t undo the universal truth of it! Prefer your mantras to come from mystical philosophers rather than monster multinationals? How about this then?
I hear and I forget. I see and I remember. I do and I understand. Confucius
This mentoring community that I am a part of, we are about applied learning. We learn by doing. We learn, not just through each individual’s patient encounters but through the collective clinical experience. We make what can otherwise be an isolating experience of constantly, seemingly, reinventing the wheel, if not many wheels (!), into one of collegiality and ‘using the force’. If you haven’t experienced Group Mentoring with me previously and are thinking about next year being your year (see below to find out more about our 2021 offerings), we put together this fun little video here to get across that mentoring isn’t about a conversation between just two people.
With Group Mentoring you’ll be learning, through the application of core clinical skills, improved patient questioning, methodical information gathering, evidence based answer finding & getting access to resources that you can apply in real-time in your own practice.
“Having the group session each month, as well as having Basecamp to bounce ideas around in, is a reassuring connection to know is there if I need it. Having just started practice this year and working in an environment without other Nats around, I have noticed the occasional feeling of isolation. So having the monthly catch up keeps me feeling connected to other clinicians and gives me exposure to other cases and perspectives that I wouldn’t have otherwise had.” – Georgie
We have a range of groups on offer to suit all levels and most types of integrative health modalities. Go to our Group Mentoring page to discover the groups and bonus extras on offer for 2021.
Going by the landslide registrations for 2020, our ongoing excellent retention rate of practitioners from year to year & our already overflowing waitlist for 2021, the reputation of RAN Group Mentoring is highly regarded and a popular choice.
So, if being part of our community excites you and if the thought of learning and applying collective knowledge from expertise outside of our own, now’s the time to put your hat 🎩 in the ring, put your hand up ✋🏼 & join the conversation 📣 through Group Mentoring.


 MasterCourse I: Comprehensive Diagnostics.
MasterCourse I: Comprehensive Diagnostics.