It’s no secret I am in the midst of some serious deep-diving through the micronutrient evidence base & at a depth of about 30 metres I struck Boron! Don’t yawn! I saw that. Thinking, ‘boring’, when we hear, ‘Boron’, is almost as bankable as watching everyone reach for their water bottles when you mention anything hydration-related 🤣 But I am here to restore your positive regard for this mineral and remediate its bad (& boring) rep! In preparation for the Nutrient Prescriber’s Program we started each nutrient review with the seminal contemporary nutritional texts and then launched ourselves headlong into the latest & greatest research. By the end of all the Boron bits in all my trusty texts the yawn was not gorn! But the moment I started reading the research I was like, ‘Are we even talking about the same thing?!’Turns out we’re not 😵🤦♀️
You see Boron has been a longstanding victim of identity theft. What we’ve been lead to believe is Boron is weed-killer and ant-poison and look it does give us some of the benefits of Boron but not all. And it possess a pharmacokinetic & toxicity profile that naturally occurring Boron simply does not.
Who decided that the Boron that is ubiquitous in our environment but almost exclusively consumed by us only after biotransformation by plants – could just skip that last bit and still be safe and optimally beneficial?! Probably the same guy that came up with folic acid, may I suggest? Anyway, enough is enough. We all need to relearn Boron – naturally occurring Boron – in the form of Sugar Borate Esters (SBE)- the evidence of benefits for which will blow all of our little minds! Well it certainly blew mine! Looks like this natural form of Boron is going to hit the Australian market in the not-too-distant-future 🐦 can’t wait to see which supplier is sufficiently progressive and research-aware that they bring this to market, having been available as a high grade supplement, employed in numerous RCTS OS for some time. But this little Update in Under 30 is not waiting around for that release date – there is much to be gained from SBEs right now – so make some noise as the real Boron at last takes the stage!🎤
Boron has been the victim of longstanding identity theft and we unknowingly have been interacting with its imposter. Contrary to everything you’ve ever been told about this mineral, naturally occurring Boron is full to overflowing with benefits for our gut, our bones, our brain, our management of other minerals and is safe in large quantities. That ‘bad guy Boron’ you were introduced to and is still present in many of your supplements is a form we never consume in food…and therein lies a world of difference! Come meet the real Boron so you and your patients can get the real benefits!
You can purchase The Boron Deception: How We’ve Been Fooledhere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
Still. And yes – like you – I don’t see any slowing down any time soon in this extraordinary paradigm shift occurring in medicine and health. Which for us humans involves one humbling discovery after another.
Here we were thinking we made our dietary choices from a place of free will & individual preferences 🤣🦠
Thinking those microscopic mates, were making those B vitamins, and SCFAs and and and…for us & our benefit 🤣🤣🦠🦠
And while there’s a lotta love going on between our microbes and our micronutrients – in both directions – Pat Benatar said it best, “Love is a battlefield”
(sorry but I feel compelled to insert a link here for the youngsters – you’re welcome 😉)
The tussle over who gets to access those nutrients that are actually essential to both of us (the hostage and the microbiota) is an absolute turf war, peeps, and this battleground has seen some bloodshed! The new new question being raised is how the prescribing of nutrients, especially at the higher doses we tend to use, trickles down to influence and impact those microorganisms who reside in the bowel. Directly – as a selection pressure we have, likely unintentionally unknowingly, introduced. Which species do well when exposed to levels of a vitamin or a macro or trace mineral that are simply unobtainable in the diet? Yes – research answering these questions has begun in earnest revealing some positive ‘prebiotic-like actions’ of some but not of course for all nor in all scenarios. Want to learn more about this latest aspect we need to consider when formulating our nutrition prescriptions? You can either jump in and join us in the Nutrient Prescribers Program which kicks off next week to get across absolutely everything new in nutritional medicine or just dip your toe in here with our latest Update In Under 30: The Micronutrient Microbiota Universe
The world of health science went microbiota-mad a few turns back and there’s no sign of an end. Research continues to reveal the breadth of the GIT microbiota’s positive & negative reach, in particular, & with discovery upon discovery we’ve come to understand how often the microbiota are ‘managing us’. Both in terms of being integral to the success of our digestive, immunological, metabolic etc processes but also in a self-serving way, for example, directing our dietary preferences to satisfy their own needs. This has understandably prompted the question about the impact micronutrient supplementation is unintentionally having as a selection pressure on our gut microbes. Which bugs like which B vitamins when taken in excess of the amounts achievable in the diet? And which microbes flourish and which falter when we radically change their mineral exposure?
You can purchase The Micronutrient Microbiota Universehere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
I’m such a sucker for marketing!…ZoomZoom is from an old Australian car ad – an earworm clearly conveying ‘ the speed of something’, and let me tell you, totally fitting for this little Zinc tale I’m about to tell! Many years ago, I wrote a thesis on Zinc that necessitated me reading every research paper ever written (that’s how it felt anyway!🤪) on this trace mineral. Like everything in nutritional medicine, especially in the area of our burgeoning understanding of micronutrients, this is a highly dynamic space, so regular reviews of what’s new is essential and, since my thesis, part of my regular practice. Well, I just did my latest deep dive, and HELLOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO radical paradigm shift(s)…yep plural!
Zinc supplements should ideally be: Organic amino acid chelates Taken daily – due to the lack of Zinc stores in the body Taken fasting Taken in doses in excess of the RDI to compensate for the smaller % absorbed
Yep – nope. Or in true-blue Aussie: Yeah, nah. Can’t believe what you’re reading right now? Neither could I when I undertook this recent review but the studies are increasingly sophisticated and the resultant paradigm shifts are being echoed, reiterated & reinforced. And these have, in turn, challenged all those old ‘norms’ about how best to administer zinc for those patients with a shortfall. If you’d like to take this little journey for yourself…I suggest you start here! I immediately changed how I take it myself and now my mission is to both spread the word and get us all reflecting and reviewing our prescribing principles around Zinc…and tbh, around all micronutrients! After spending my ‘summer’ doing sufficient reading for a second thesis on everything new in micronutrients…I am armed and dangerously prepared for our upcoming *NEW* program: The Nutrient Prescriber’s Program which kicks off in late Feb for 5 months.
I truly believe that based on all this new information, we can now get so much more out of our medicines.
Nutrition represents such an extraordinary set of tools for us to work with, but it’s time to sharpen those tools in terms of how we apply them!
The Changing Zeitgeist Of Zinc Prescribing
Zinc research is a highly dynamic field and given its relative recency of discovery as being essential to humans, we’re still in the early days of truly getting to know this mineral. In just the last few years, enormous gaps have been filled-in regarding its regulation and roles that look to radically change our prescribing practices. Tune in to this essential update for some serious food for thought about doses and dosing frequency.
You can purchase The Changing Zeitgeist Of Zinc Prescribinghere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
Recently I asked practitioners to tell me where the ‘therapeutic reference range’ many of us were taught for nutrients comes from & no one has been able to answer that.🙄 If you’ve heard me refer to my original naturopathic education before you’ll know I generally hold it in high regard. And I’m forever mindful that there are always things that can be made better. What’s been playing on my mind lately is the recognition that I originally learned nutrition from one (exceptional) individual, and then went on to become the lecturer years later at that same and other institutions. Additionally, I am aware of some of my past students also going on to become the next generation of nutrition lecturers at those same places – and often in fact inheriting their lecturer’s notes, slides, overheads [showing my age!!] with the job. Can anyone else see a problem here? What’s brought this into sharp focus lately are many of the questions I’m endeavouring to answer as part of our much-anticipated Nutrient Prescriber’s Program. How much? How often? When? Which form when? & For how long? Which are the key questions we have to answer with every single nutritional prescription.
To not only source the most rigorous scientific answers to these core critical questions but to also develop a framework that we can all use to answer them for ourselves at the point of any future prescription creation, I have had to go to great lengths.
But as I research & write, I also keep asking myself, ‘How would ‘old-me’ have answered this?’ How did I up until now either consciously or unconsciously answer these sufficiently to make such decisions?
So it’s an ongoing little (& sometimes BIG🧠) internal debate that is raging as I write. And when I ask current praccies these questions they reflect back similar ‘old-me answers’, the vast majority of which were handed to us by our lecturers with plenty of top-up ideas from industry. These answers include things like:
How much? Somewhere within the therapeutic dose range? How often? Depends on lots of things but generally aiming for daily of course!
When? Minerals before food, fat soluble vitamins with or after, magnesium at night etc
Which form when? Now it gets tricky – because there are all these new forms that we weren’t even taught – but maybe ‘active’ – active is always better, right? Or is that natural? The most bioavailable?
& For how long?Ummmmm how long is a piece of string?! Until the signs and symptoms resolve?
Now all of these as general statements are partly correct. And with respect to the level of understanding we need to have when crafting a nutritional prescription for a specific patient, with a specific presentation and for a specific purpose (correction of deficiency Vs supranutritional Vs therapeutic antagonism etc)…well they are plain wrong in the majority of instances. Don’t freak-out in freefall!🪂 The prescribing of nutrients is a wonderful and typically, a wonderfully safe, modality that offers us the potential for extraordinary patient outcomes. When used well. We could all benefit, I believe, from just sharpening our tools so we bring out the very best in our medicines & in ourselves, as prescribers & clinicians. I am neck-deep in writing the 10 modules that can start us all on that journey. Want to join me?
And to be clear, about the educational echo chamber,
In the past I was part of the problem and ever since I have tried to be part of the solution.
With over a decade of mentoring practitioners, Rachel has recognised a need for an educational program that provides practitioners with more structure, more science, and therefore more certainty in navigating each individual prescription. This monthly meet-up is delivered in 5 live sessions and runs from February to June (10 modules). All sessions, encompassing both theoretical and applied learning will run for approximately 2 hrs each.
The builder responsible for my reno arrived one day with a frown. When I asked him what was wrong – he said he’d just had his second high PSA result and now the doctor wants him to see a specialist. It was apparent that he felt this was a real cause for concern. Talk about raising a red flag to a bull 🚩🐂 Yes, of course you know what followed. I insisted on reviewing the results myself only to find the reference range provided on his report was not specific to his age – and if we adjusted up for this (as the science supports) his result is just 0.5 ng/mL above the expected value!
Now, remember he is a builder so, ‘0.5’ in his mind might well be on par with 5mm which apparently is a big deal…or so he keeps telling me every time I try asking for some weird unconventional thing for my roof, windows, walls, whatever!! So I still had to provide a little bit more detail for him to get perspective and to understand the true meaning (and lack of scary meaning) of his results.
This however is just a micro-illustration of a big problem in pathology – we all risk a lack of perspective but if we can get it back, aids us to see that seemingly ‘normal’ results are sometimes a concern, and so-called ‘concerning’ ones, non-significant. The incredible patient insights that can be gained from being able to measure & monitor actual quantities of things in our patients; nutrients to novel disease markers, precursors to end-products, all comes down to understanding how their values compare with…with what? With someone of a different sex and age? With ‘all adults 18-108!’? With any other pre-menopausal woman regardless of reproductive or cycle stage? With ‘the average’ adult given that this current definition is overweight & unwell? Who are we comparing ourselves and our patients to?
When I undertook my undergraduate training many moons ago – there was no education in blood test interpretation. But as soon as I got out into practice I found my patients had all these bits of paper filled with magic numbers that I felt certain might offer me insights and a deeper understanding of their whole health – and how to best help them.
I desperately wanted to decipher this foreign language and made it my mission to do so. I was lucky enough to meet and be paired with a kindred spirit, Dr Tini Gruner, who happened to be my supervisor when I returned to undertake my honours thesis. Together we pooled our knowledge, sought out & shared with each other yet more and found that, together with comprehensive case taking, it provided excellent scaffolding to our work-up of patient cases. Better than that, it created this baseline for patients, identified clear treatment objectives and we could measure the success of our interventions based on how their results did (or didn’t) respond to our interventions. It was (and still is) a totally thrilling way to practice.
We talk about there being both an art & science to medicine generally and certainly an integrative approach. Without the benefit of pathology interpretation, I felt too at sea at times, without quite enough of the science to check the accuracy of the ‘art’ and my speculation.
Being able to understand what each individual result represents and reflects, to know how to form meaningful comparisons – with external reference ranges that speak to healthy individuals of the same sex & life stage, derived from rigorous research – and also form a comparison with the patient themselves, to pick up on the most subtle and significant early alerts to an emerging pathophysiological or healing process – is the skill, I believe, we all need in health to complete the toolkit. That’s why I made it my mission to learn the language of labs, from a conventional & integrative interpretative perspective, and then to share this learning with everyone wanting and willing to take this baton from me (& Tini) and run with it 🏃♀️🏃
MasterCourse I: Comprehensive Diagnostics. Click here to read more and here to purchase it.
*Please note that this is the place to start for everyone wanting to add preventive diagnostics to their tool kit. It is also the pre-requisite for MasterCourse II, so make sure you have completed this before continuing with MasterCourse II: Thyroid and Adrenal Diagnostics.
MasterCourse II: Thyroid & Adrenal Diagnostics. Clickhereto read more and here to purchase it and sign up for the Free Watch Party commencing tomorrow, 3rd August 2023 with is included with each purchase of the MasterCourse II.
Heck yeah. It’s going to take a lot more than 1 push-back post to turn this ship around! Likewise, I was only getting started with my recent Update in Under 30 episode, ‘What’s Hiding Behind Histamine’ 🤓😂 & part 2 has just been released where we unpack the case of a 41yo female with chronic diarrhoea, multiple food reactions, very high stress and very high oestrogen. Sounds like she’s a walking Histamine Headline – except she isn’t.
Right now we really do need to keep this conversation going such that a healthy discourse can help us deconstruct the histamine dogma.
I know I’m showing my age here, but anyone remember when Candida was having a ‘moment in the 90s? Ok, so that ‘moment’ stretched to over a decade of a ‘Candida-contagion’. No one could eat melons or mushrooms, eat ferments or feel joy. It was a bleak time that did our profession some reputational damage. Not only because seeing an ‘alternative practitioner’ became synonymous with being put on an unbearable, unattainable restrictive diet and positioned practitioners as peddlers of punishment but also because it took some time for science, in the form of accessible (& always improving) assessment methods, to come along and save us from the folly of the 1-diagnosis-for-all mentality.
Let me ask you, how many times do you actually see Candida overgrowth on reports from stool testing performed using best practice modern methods?
In my experience – never – not as a stand-alone issue. Occasionally, as part of the overgrowth of a suite of opportunistic organisms where the real-take home is the need to ‘remove the opportunity’ via the promotion of more good guys. So not only was the diagnosis incorrect, the proposed treatment for it was a complete misdirection as well.
Can’t help thinking in the current climate of Histamine Hysteria that history is repeating itself.
How will we all individually, and as a profession, respond this time?
In this follow-up episode we observe how the 3 key elements often hiding behind a histamine intolerance diagnosis: Misunderstandings, Missed Messages & the potential for Mistaken Identity, have played out in the case of a 41yo female who presents with chronic diarrhoea, a long list of problem foods including now a suspicion of ‘histamine foods’. Rachel offers up new ways to approach the patient work-up that cut through the ‘noise’ and enable us to better identify what is hiding behind histamine in similar cases of marked gut dysfunction.
You can purchase What’s Hiding Behind Histamine? – Part 2here. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account. You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
You’re invited to attend acnem’s 2023 Annual Conference ‘Long COVID, Navigating the Complexity, A Clinician’s Roadmap’.
Saturday 29th & Sunday 30th July 2023, Melbourne. Both face-to-face and online.
To get 25% off acnem Annual Conference USE CODE: acnem25
I can barely bring myself to write the word given how overused it has been of late 🤐🙄😯😕🙃 But I gotta say something! If we have found ourselves currently in a place where every second (or indeed single!) patient has a ‘histamine issue’ then I am afraid that it is we, that have an issue. (more…)
Just as optimal integration of lab results into our patient work-ups makes ‘the invisible visible’ we thought we might make visible some of the everyday Q & A that we engage in with wonderful practitioners who are fast becoming Diagnostic Divas & Divos.
Praccie email arrives with subject header ‘Graves Help’ (or is that ‘Graves…HELP!’🤔)
Practitioner: I have a Grave’s patient who required Propylthiouracil (PTU) for a few months from late 2022 until Jan 2023 which obviously took her thyroid in the opposite direction (see labs). Following a miscarriage last year, she has conceived and is around 6/40 and her current TSH result has come in at 3.3mIU/L, her TPO Abs > 1000 and she also has low-level Tg Abs (TRAbs not measured this time) and this is what she just said to me:
“I just had my specialist session this morning – and she has put me on thyroxine (50mcg) as my thyroid is quite low. I also asked her about the prenatal vitamin and she said it was safe for me to be on iodine at this time, as the Graves isn’t present and baby needs it for the development of its own thyroid.”
Oh gawd! Preg? Iodine? Graves? Antibodies? Antenatal or postnatal aggravation?!
Is there an UU30 I can listen to to help me understand this?… sorry for the panicked email…
When it comes to the recognition of Nickel as the number one metal allergen worldwide, affecting up to 30% of adults and with a particular predilection for women, it seems like Australian health professionals really do come from the ‘land down under’, with many of us still somehow yet to read that memo.
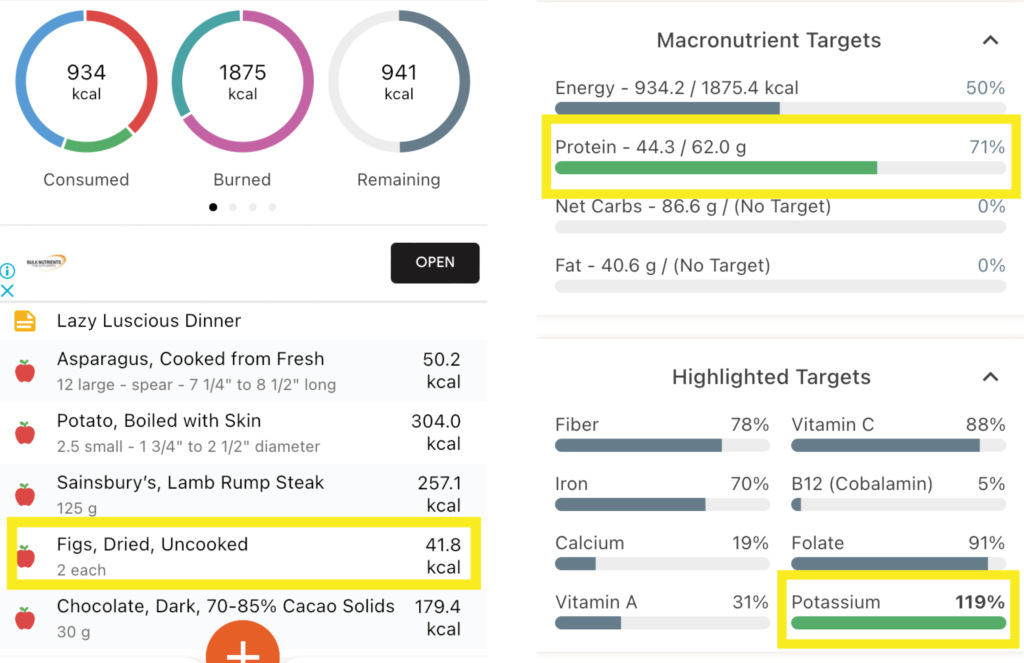
And for weeks now I’ve really been banging 🥁🥁 The 1st drum was me making us all salivate & suffer through my month-long Mediterranean feast The 2nd, my ongoing incurable fixation on the ‘Power of the Ps’ – Protein & Potassium, not just individually, in terms of meeting optimal requirements for each, but relationally, as in, the (im)balance between them & the clear goals that have come from research for best health outcomes.
Maybe now you can hear the individual drumbeats merging to form some sort of chorus rather than a cacophony?! I can🎶 And largely that’s because I decided to put the Ps & Ps principles (Total Protein:Potassium < 1; Animal Protein:Potassium <0.6 etc) into practice, entering my own meals into software to see how often I kicked each goal and how often I missed (& [ouch] kicked myself). Personally, I think thirty years in the game can lead to some laziness around looking in depth at our own dietary habits. As in, I know the ‘rules’ right, back to front, so I’ve told the ref to have the rest of the season off! My meals are both mantra and memory foam. There’s a lot of eat and repeat. Like my heavy lunchtime reliance on my ‘protein power pack’: 2 XL soft boiled eggs on 1 piece of avocado paleo toast and a bunch of asparagus. My (in)famous buckwheat breakfasts loaded with nuts, yoghurt & fruit. My bulk-cooked plant protein heavy, animal protein light, stews, sauces and soups. Even, what I considered my laziest but luscious organic farmers market meal, pan fried lamb rump steak, steamed fresh new season potatoes & a bunch of asparagus. So which of these would you have put your money on for the most Ps& Ps goals kicked? 🤓🤯
The Lazy Luscious Steak & Veg Meal Wins with… Total Protein : Potassium of 0.56! Animal Protein : Potassium of 0.41 Btw that’s because of the Potassium-punch of Potatoes [>2200mg!] and the finale of Figs & dark chocolate [329mg]! Animal Protein : Vegetable Protein of 2 : 1 (ok so you can’t win everything!)
Now obviously I am just looking at each meal individually, but the Protein & Potassium goals are really daily ones, however, I, like most people, don’t lay out the totality of my ideal food intake for the day and then think, now how do I make this all edible?! I think in meals not metadata! So this little exercise was already incredibly rich in insights, checking my assumptions and snapping me out of some misguided mental calculations into the real world, placing a ref back on the pitch! I’m not ditching any of these favourites – just more mindful of what meal goes with others across the day, for better balance. Now all this analysis is time-consuming of course and while various software will do the macro and micro crunch, as far as I know, you still need to do all the Protein and Potassium calculations by hand, Ah yup. So, 1) I’m stopping now & 2) I’m thinking about creating a little spreadsheet that auto-calculates a lot of these targets once you’ve obtained that basic elemental data to input, for easier use in the future – would you use it?? [insert answer here 🙋♂️]
And then you can show me your kick arse protein/potassium combo! Because clearly even us ‘experts’ apparently need data to double-check our assumptions!
Now where’s the other 🥁 in all this, that Mediterranean one, I hear you ask? It’s in the figs! My lamb dinner actually just missed reaching the targets for protein and potassium balance…until my fig finale! And remember, what the Greeks say, ‘A few figs a day keep the chronic-mild-metabolic-acidosis at bay!’ 😂 Just jokes…
To prevent or minimise our slow but steady march towards sarcopenia, the need for dietary protein adequacy to fuel muscle maintenance is a no-brainer – but how does ageing affect this? We get less bang for our buck. We have to eat more, to get the same ‘amount’ but do you know why this is? Add to this, that also as we age, we experience a greater acid burden from a lower acid dietary load. And given that a higher acid load (PRAL), has been shown to have a negative effect on muscle and bone markers in the past, clearly to ensure optimal health of our bones and muscles as we age, we have a riddle, or two, we need to solve. How do we use Protein and Potassium intakes to benchmark our patient’s diet quality and musculoskeletal risks and can we modify their consumption of either, to drive therapeutic gains in terms of both BMD and muscle?
You can purchase The Protein & Potassium Riddle of Ageing – Muscles and Boneshere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
How much? How often? When is the best time & timing? do you know about friends, foes and frenemies? Which form, when? e.g. building blocks or bioactives? And for how long? aka are we there yet…?
These are the kind of questions that one would imagine nutritional prescribers can always answer – but can you? Yet this is the goal, right? So that with each and every unique individual who needs supplements – we have a clear, consistent go-to framework to guide & direct these prescriptions. One that makes scientific sense, offers optimal outcomes and removes the uncertainty.
From my interactions with thousands of practitioners, however, I know many of these key questions plague practitioners & they feel, at times, as if they’re flying without a net, or without a strong systematic approach, or at the very least without all the answers to these questions.
I’ve had so much good fortune & so many others to thank for providing me with this foundation. Fay Paxton – my nutrition lecturer in my under-grad who indoctrinated me with a systematic approach. Dr. Tini Gruner – my principal supervisor at SCU, who shared & further fuelled my passion for biochemistry and reading labs to extract insights into each individual. And thanks also to all the pharmacists I’ve delivered education to over the years, who, as a result of their grounding in the principles of pharmacokinetics, always ask the best questions – questions that if I don’t know the answer I know I need to know the answer! So I made it my mission to find out!
While we dip into these aspects of nutritional prescribing in our regular mentoring groups on an ‘as needs’ basis, I’ve decided the time has come to create a year-long program dedicated to sharing this information and building this skill-set in practitioners.
This monthly meet-up is delivered live (max 1.5hr) and runs from Feb to November with the following currently proposed format *subject to change dependent upon the needs of the group
Feb Factors Affecting: digestion, absorption (host, form, dose)
March What happens to what gets left behind? e.g. enhanced enterocyte micronutrient concentrations & their effects plus unabsorbed nutrients & their interactions with the colonic environment
April What happens to what’s absorbed e.g. distribution, hierarchy of needs, activation and deactivation
May The pharmacokinetics of prescribing
June Where do our ideas on dosing come from? e.g. Physiological Vs Pharmacological dosing & actions. The basis & believability of maximal intake boundaries?
July Bioefficacy V Bioequivalence. Beyond building block nutrients: Is ‘Bio’ (-active, -peptides, -materials) always better? e.g. GABA Vs Glycine, NAC Vs GSH, PLP Vs Pyridoxine, Niacin Vs Niacinamide riboside ——————————————————————Aug month off—————————————————————————
Sept How often & for how long? Are we there yet? And how would we know? Plus Fast Vs Slow Nutritional therapeutics
Oct Strategies for Supplement Success e.g. friends, foes and frenemies in nutrition underpinning principles with examples; compliance changers for clients
Nov Live attendance & opportunity to participate in a case-based mentoring session
This monthly ‘live’ meet up will be delivered as part of 2023 Group Mentoring as The Nutritional Prescribing Program Group Mentoring applications open 17 October 2022.
To join the waiting list and be notified when applications are open, email the team at [email protected]
Find out more about what groups are available for Group Mentoring in 2023 here.
One of my dear friends told her husband several years ago that she had noticed he was now making, ‘old man noises’ upon standing up from couches & chairs. She told him that must simply stop. She pointed out that he was only 50 and that she neither could nor would listen to that for another 40 years!
He stopped!
But aging and old (wo)man noises are coming for all of us, right? And by the time we’re making those noises or excusing ourselves from certain activities due to sore, dodgy or NQR [insert joint or body part], we’ve spent several decades unknowingly right on course to get here! We don’t generally pay any attention to our ECM (extracellular matrix) which suffers in silence, slowly but surely losing its structural & functional integrity from the age of 18 on, until we reach the tipping point: joint degeneration, repetitive soft tissue injuries etc, and a problem that will never be silent again! Cue your choice of anti-inflammatories it seems – til death do us part!
The Ageing Matrix is a thing.
And no I haven’t seen the movie – I don’t need to – I’m living it.
When I was pregnant I thought I wanted to specialise in pre-conception & pregnancy care. Then my babies arrived and I took a fancy to paediatrics. Sound familiar to anyone? Now, unsurprisingly, I have a real thirst for knowledge expressly aimed at bettering this whole ageing-thing! So in preparation for this Update in Under 30 episode, I’ve relished the opportunity to put the Ponds Institute & all similar cosmetic companies on notice! Scrutinising their claims that every woman on the planet would do better with more Collagen, more Elastin, more Hyaluronic Acid, just more of every key ECM component really. Ok, but in accordance with my bias and my business, my lit review pertained to oral supplements, not outrageously priced magical middle-life-crisis rubs and the therapeutic action I had in mind was the integrity of our ECM, and the roughly 2kg of collagen, we rely on, for functions a lot less frivolous than stopping sag. I have to say, I started out as non-believer but the research was quite the awakening…still there’s a lot to unpack here in order to repack our ECM and prevent against the erosion of its integrity and everything we build, and rely on, upon it – to live well!
Osteoarthritis (OA), like osteoporosis, is a diagnosis made after decades of disease. Underpinning it all, is our aging Extracellular Matrix (ECM) with its characteristic compositional change that leaves us vulnerable, from the ripe old age of 18! The ECM, like all other tissues, is made from basic building block nutrients but presented in their most fanciest of forms with triple helix structures, aggregates and other large molecular weight components, that each possess remarkable physico-chemical properties & convey extraordinary functionality to structures like joints. But is prevention against, and effective intervention for, OA as easy as consuming more of these ECM biomaterials?
You can purchase Supplementing Collagen & ECM Biomaterials – What’s the story?here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
Are we doing ourselves out of a job? I’ve been talking treatment plans with my New Grads recently. Given, only recently these were major assessment items in their clinic units, they have been trained to create ALL-ENCOMPASSING (biopsychosocial) prescriptions and recommendations of utterly EPIC PROPORTIONS – to simply prove they know it all. Problem is this doesn’t work in the real world.
Emailing your client multiple pages of advice that covers: a whole sizeable supplement schedule that only a military-training could nail (2 tablets 1 XTID 1 X BID, a liquid, a powder, some with food, some definitely not with food) plus dietary advice, plus hyperlinks to exercise advice, mindfulness exercises and a request for follow up investigations before the next appointment…is…a L*O*T!!
It is also ineffectual – because it completely disregards the human on the other end. Let me ask you this, how much change are you capable of between a first and second appointment, roughly a period of 2-3 weeks? Personally, I gotta say not that much. It took my dentist years to get me just embrace flossing & I don’t think I am an exception! With all the knowledge we possess its hard not to see people as (a long list of) problems (& problematic behaviours) that we translate into, and solve via, a prescription.
Effectively we are saying to patients with this practice model, ‘Go change & come back when you’re done & then I’ll probably ask you to change some more!’ That’s both a big ask and a huge missed opportunity.
I hear from reliable sources over the ditch, that GPs are increasingly referring their patients to, or teaming up with health coaches, rather than naturopaths. Given what I’m observing, I get it. Doctors on the whole only have time (and barely then) for a finger-pointing prescription – certainly not the time and touch-points required to actually support patients with the very difficult thing that is, behaviour change. Nor the skills to truly facilitate patients making the necessary and desired changes – so they outsource this role. But we shouldn’t.
After all – I want to be on my patients’ support bench & health care team always – not a flash in the pan, that blinded them with science or my ‘smarts’ and proved to them in one over-stretching prescription – that naturopathy is not for them, or at least, they’re not fit for the task.
At the end of an information & insight heavy appointment, formulating a list of products and doses for our patients to take can feel like a bit of a ‘tada moment’, like a magician pulling a rabbit out of the hat. “Here is the solution – now off you go!” Research tells us, however, that treatment-plans that are a co-creation between you and your patient – evolving from a discussion that not only allows them a voice, but a major role in the decision making – are far more likely to succeed. While we are the authority on our medicines, our patients are the authority on what makes them tick & what’s likely to succeed, in terms of taste, texture, temperature & timing! This is called Patient Centred Prescribing and together with some other tips tricks and hacks I share with you in this episode, can really increase patient buy-in, compliance and therefore bring your treatment plan to fruition and fulfilment!
Last week, yet another patient with refractory diarrhoea, up to 10 stools a day, Bristol type 5-7, for 3 decades following a diagnosis of Crohn’s at 16 years old. A range of specialists have thrown everything at ‘it’ – single & combination immunosuppressants, TNF alpha blockers, buckets of sulfasalazine and bathtubs of antibiotics – she’s been gluten and dairy free for years, trialled strict diets that are FODMAPs free, low histamine etc etc etc. She’s even had 50cm of her terminal ileum removed & the diarrhoea continues unabated – perhaps even worse than before…& therein lies a major clue.
1/2 patients with Crohn’s exhibit bile acid malabsorption –> diarrhoea but with terminal ileum resection this jumps to > 90%
This is Type I BAD (Bile Acid Diarrhoea) & is the easiest to spot, being the result of anatomical change. You remove the section of the small intestines responsible for 95% of the reabsorption of bile acids…a LOT of bile acids are going to be present in the colon where they act as potent osmotic laxatives, right? But there are 3 other types which are a little trickier to identify – including one that affects up to 50% of IBS-D patients.
Being a child of the 80s⚡🎹 (ok a teen of the 80s but who’s counting?!) and a personal fan of fat, I NEVER thought I would EVER be recommending a ‘low fat’ diet to ANYONE🤐
But hey, that’s another ‘absolute’ that needs challenging, right? I mean this is the primary, almost only, dietary change these patients need to make and as a stand-alone intervention, is highly effective for many. We’ve had several patient successes in the last year – a total game-changer for patients in similar situations where all kinds of ‘restriction’ had brought zero joy and reward for all their ‘good (dietary) behaviour’. While sequestrants (like cholestyramine) are recommended in BAD, and are certainly worth a trial at least, patients have very mixed results – for some, in combination with the low fat diet it’s a winner – for others these meds cause GIT upset all on their own and actually undo the good of the fat restriction. Being able to identify the true reason for their loose stools and stop them going down endless rabbit holes of ..is it? is it? is a great way to re-empower people who’ve been bossed and bullied by their bowel for far too long 🤓💪🧻
This is not a trick question. Up to 50% of all patients diagnosed with IBS-D actually have bile acid diarrhoea (BAD) underpinning their digestive complaints as well as some patients with non-resolving diarrhoea post-cholecystectomy and gastro. Knowing which ones do and how to manage this, which requires distinctly different approaches from our general management of IBS, is the key. As always, good lessons come from those we learn in the clinic and this story starts with a patient and how we came to recognise the BAD in her belly.
And health, no matter which side you sit on, seems to be particularly plagued by them. I (incorrectly) recall my 4 year degree as being a series of deep personal losses, some favourite food, then caffeine, then alcohol etc etc.😂 Likewise, I’m aware that naturopathy & integrative health’s ‘voice’ in the ‘conversation’, could arguably be perceived as mostly a negative one – as in, ‘No. Never. Not good. No, not even a little bit?!’ But I love both playing devil’s advocate & reading the research (ALL the research – even the stuff that doesn’t support my views and position GASP!~) so I am less in favour of absolutisms. This came up recently when I suggested alcohol may improve iron uptake 😬
Practitioners’ responses were 1 of 2 types: humorous dismissal (“steak & beer for breakfast – at last a naturopathic prescription I can support!”) or horror. But why are we so attached to the absolutes in spite of contradictory evidence?
Let me ask you this: is coffee bad? Full stop? Period? The end? Or is it the most concentrated source of antioxidants consumed in the average Western diet? Does it improve bile flow, peristalsis and at higher levels actually protect the liver against damage? Clearly, we need to read all the evidence, including, the favourable and make individual decisions about ‘what serves and what sabotages’, for each patient. But do we? Or do we imagine we only get membership to the ‘Ultimate Integrative Health-club’ when we adhere to blanket bans?
Similarly I, like many of you, see a LOT of iron deficient women – & a fair chunk of these have been incorrectly labelled, ‘refractory’ because theconventional correction strategies (high doses everyday) don’t actually make sense. But like you guys too, I’m always on the hunt for new ways to improve iron absorption in these women, so I can hit them & their gut with less. That’s why I shared the research regarding alternate day dosing, and taking a supplement within an hour of exercise and now, I dare to ask if a tipple could be helpful?
While we know that both ‘GOOD’ (exercise) & ‘BAD’ (alcohol) health behaviours increase gut permeability, which sounds ‘BAD’, right?
But could this be ‘GOOD’ for some?
This has certainly been demonstrated in relation to exercise & iron but most of the research investigating how alcohol intake effects iron uptake and status is based on alcohol abuse. The study below, however, based on a large sample of non, mild, moderate & heavy drinkers captured in NHANES data – is a very well written and reasoned article, such that it can exclude liver damage, inflammation and HFE mutations as other explanations for the better iron status, in drinkers. And it found:
I challenge you to read it for yourself and challenge your absolutes!🤓
Oh and just in case you’re thinking, “Have we all misdiagnosed iron deficiency and it’s actually a Copper deficiency underneath?”because last year the fashion was everyone was copper toxic and now this year someone’s making noise saying everyone is copper deficient !!! (Absolute? Anyone?!) Ah, no. Copper deficiency, as a cause of iron deficiency and anaemia, has been around for about as long as nutritional medicine itself. It is absolutely a thing. But in the absolute minority of people. And if you go back to some basic maths & compare and contrast Fe & Cu at each level: 1) requirements almost 20mg Vs < 2mg 2) average intake (inadequate Vs adequate) 3) bioavailability (Fe < 20% more typically < 10% in a modern low meat diet Vs Cu is typically >50% ) and do some basic sums I call, ‘Menstrual Maths’ – You’ll likely deduce that inadequate iron intake and uptake, given our losses, is in fact the common culprit and a ‘coldie’ may be more beneficial than copper in most! Can y’all stop asking me about that now – pretty please?
And then you don’t. The reality is we all struggle at times with correcting low ferritin or iron deficiency anaemia – so what have we got wrong? In spite of being the most common nutritional deficiency worldwide, the traditional treatment approaches to supplementation have been rudimentary, falling under the hit hard and heavy model e.g. 70mg TIDS, and are relatively unconvincing in terms of success. New research into iron homeostasis has revealed why these prescriptions are all wrong and what even us low-dosers need to do, to get it more right, more often!
Did you know you can subscribe to these? We deliver at the end of each month, just add a 12-month subscription to your cart and Rachel’s latest research is on it’s way to you!
There are some things we say so often to patients we could record them and just press <PLAY> Like this daily dogma: ‘When you’re under stress, your demand for Magnesium rises and then in turn that can make you more susceptible to further stress, so we’re going to give you some to support you’. But is this actually the whole story? You guessed it, no. (I know I am fairly predictable like that 😅)
Recently, a personal new record – a patient reported ongoing daily use of a very high dose Magnesium ‘practitioner only’ product 8 years after it was prescribed by her then naturopath – and guess what, the patient still hadn’t reached nirvana* not the band! – a transcendent state in which there is neither suffering, desire, nor sense of self
Jest as I may – I think this raises some serious questions. The pervasiveness of our prescriptions when patients are not given an end-date coupled with ongoing access. How (not) effective this intervention was if someone perceives ongoing undiminished dependency on it. And specifically with Magnesium – whether our prescriptions (form, dose, adjuvants, advice) are the problem? If stress is synonymous with a shortfall of this mineral then Magnesium is not a solution to stress itself but the amplified stress response and the stress still requires its own redress, right? But do our patients hear this as well when we press <PLAY>?
Likewise – the BIG doses per serve being recommended might make sense for the minority (seeking potential NMDA antagonism) but are a real mismatch with the majority, who are just stuck in the stress loop and weathering a perfect storm of Magnesium under-supply and increased demand.
I love my minerals as much as, ok more than, the next practitioner but I’m always keen to refine my repletion approaches and oh yes, by the way, there is good data, a meta-analysis in fact, examining how long it takes to achieve repletion using oral Magnesium – and guess what, it’s not 8 years! The latest Update in Under 30 goes into all this and much MuCh MUCH more…you’re welcome 😂
Practitioners working with nutrition appreciate that Magnesium is vulnerable to depletion by the stress response and that in turn, can make people more prone to stress & keep patients stuck in a so-called ‘stress loop’. But do we understand the intricacies of this and how we, as practitioners, can get stuck in another kind of loop – one of endless Magnesium prescribing without reaching repletion? We discuss ways to improve your Magnesium prescriptions – in particular, ‘doping Vs drip-feeding’ and other things to assess & address if the long road to repletion risks becoming an endless one!
You can purchase Magnesium – Stuck in the Stress Loophere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
And it will. It knocked again on a practitioner’s door last week. She in turn knocked on mine. It turned out to be a very familiar story:
Firstly:Patient presents distressed – recently a nurse applied the term ‘Chronic Kidney Disease’ to HER (note no one has ever mentioned this diagnosis) Secondly:She is in stage 3 of 5 Then: This practitioner is left to have ‘the conversation’ but wants to know where to start, ‘What do I say?’ Next up:And what else can I do for her – are we really able to make a difference?
Familiar to you too? So,1st & 2nd: Yes, this is not uncommon we would have to say and even with age-appropriate reference range adjustment, her GFR consistently in the 50s, flags premature decline. Then: What DO you say? Well this clearly is a delicate area, not only because of the level of patient distress and concern but because, at this stage the practitioner knows nothing more than what the patient tells her and her ELFTs over the last 2 years. This is not enough information, right? Chronic Kidney Disease is a heterogeneous condition, with many different causes, manifestations, comorbid conditions, and factors affecting prognosis (Levey et al., 2009) So while most individuals certainly progress from stage I to II and II to III the rate at which they do this differs dramatically.
Two years of data is not long enough for us to appreciate the trajectory of her CKD & means we are unable to provide the patient with any kind of perspective:
‘With no further decline in GFR or progression in stages over 5 years, you’re doing well, so keep doing what you’re doing!’ Vs ‘Ok, I can see what looks like a little period of accelerated decline – let’s review what’s been happening and how we can turn this around”
“Please sir can I have some more?’ Yes, back to her primary carers to request more information to fill in the gaps, and ideally more labs to calculate & observe the trajectory for yourself. Next Up: What do we have to offer the patient with CKD stage III? Soooooooooooooooooooooooooooooooooo much!! When is adequate hydration helpful? Always, except Stage V! (and these patients are not coming to see us) What are our treatment objectives & our evidence backed medicines to meet these? Hcy lowering (note often referred to as ‘folate refractory’ in renal dx), vitamin D adequacy, lowering the acid load, supporting the microbiome & in turn the Renal-GIT axis…hang on, got to go…someone’s knocking 😅 but hopefully we all can see, when they present to us, they are indeed knocking on the right door ✊
Nutritional or naturopathic support for the kidneys tends to have been over-looked in our training and yet research suggests there is much in our tool kit that can make an enormous difference to this system, in particular, slowing the progression of chronic kidney disease in patients. Rachel talks about what these key evidence based interventions are and also gives you the tools to identify the early pathology markers of renal impairment – the earlier the recognition, the earlier we can make a start on the remedy.
It seems almost farcical to question the merits of hydration for our renal health but is this actually the truism we have been lead to believe? Where does the recommendation of ‘8 glasses a day’ come from and what is the level of evidence to support it and in whom? Or should we in fact be setting our sights on output ie. 24 hr urinary volume, over input. Do all kidneys love water – or does this relationship change with the progressive impairment seen in CKD which affects up to 30% of our middle-aged population? When does hydration become harassment?
Most practitioners graduated with not much more than a few ‘kidney’ herbs and an under-appreciation of the contribution renal health makes to wellbeing. It’s not just about waste and water. In reality, the kidneys are pivotal in just about every major element: blood, bones, pH balance, methylation, control of oxidative stress, the GIT microbiome and more! And we are seeing the impact of this in our patients in all sorts of subtle and not so subtle presentations. This new instalment in diagnostics, brings the renal system into the spotlight so we can confidently identify and better manage its critical contribution. In addition to this, just like with other routine labs such as LFTs, we unpack how these so-called ‘renal markers’ can flag a plethora of other insights into your patients, from reflecting (un)healthy muscle mass, to calculating individual dietary protein adequacy, from key ‘danger and distress’ signals in response to disturbed metabolism, oxidative stress to certain types of GIT dysbiosis! We call this Explained, Expanded and Exploded because these routine labs can deliver XXX sized insights into your patients.
Last week I had my say about acknowledging our elders & mentors, this week I want to speak to the power of the young peeps. Just like a younger sibling, nipping at your heels can act as a great motivator to move faster, or having children can inspire us to do more to improve the ‘world’ we’re welcoming them into, my interactions with naturopaths, nutritionists & herbalists of the younger generations generally effect both responses in me! The best of these come from cluey ‘youngsters’ (mature-age-second-career-new-nats included!!) who ask the most difficult questions & show dogged determination in getting answers to these either via me or in spite of!
This is exactly what’s been in play over the last few years (yes, you heard me…years) while I’ve been under the watchful gaze of Jostling Josh Weymouth! He’s a youngun’ – it’s all relative right – who has kept us both on the straight and narrow writing:The accuracy and interpretation of plasma selenium in our patients: a literature review,which hasjust been published in the the Australian Journal of Herbal & Naturopathic Medicine.
At the outset I was able to hand over a substantial selenium research hoard I had obsessively compiled, Josh was able to build on this, refine some fledgling theories I had and then completely redefine my appreciation & understanding of how chronic over-treatment (not toxicity…) is so deleterious to human health. Check this out:
When Selenium (Se) saturation point occurs in plasma, there is a potential reduction in health protection… Se will progressively pool within plasma non-specifically as SeMet in lieu of regular, sulphur containing methionine, in albumin and other proteins…inducing oxidative stress via a complex disruption of cell reactions/signalling This is likely to be how Selenium over-treatment increases the risk of both CVD and T2DM
Many of you may ‘Know Your Numbers’ when it comes to Serum Se targets in thyroid health or just generally know how to Stay Safe with Selenium Supplementation because I’ve spoken extensively about these in the past and you will be relieved to know neither my ‘numbers nor my message’ have changed BUT I encourage everyone to read this new article because Josh has added so much more, including the interplay between our microbiota and our individual selenium needs, handling and tolerance and and and….I could go on but…what I really want to say is, thanks Josh for your academic rigor, your firm determination & diligence and for nipping at my heels all this time. This important piece of work just wouldn’t have happened without it 🐶
Is it just me or do you view everything with a trained eye? My son always laughed when I wrote him a shopping list: I would list items under each shop and I always wrote down our local supermarket the Independent Grocers Association, like this: IgA…you all see what I was doing, right?!! It’s actually known to everyone else as IGA…well truth be told, I didn’t until he pointed it out 😂 Then there’s this relic I regularly pass, as I walk through bushy parkland near my home, ‘Hmmmmmm, B12 hey?’, I’d muse. I’d be embarrassed to tell you exactly how long it was before I realised OMG it’s not a shrine to the vitamin but an old road sign telling you…Byron 12kms!!!
I preferred my take on it to be honest, because invariably once past this, the remainder of my walk was full of scintillating B12 banter. Just internally, people, no one panic, I don’t walk the streets of this town spouting out crazy random nutritional tidbits…although, let’s face it, I would be in good company in, the Byron Bay region!
I have a deep respect for B12 – weird but true. As a result of my clinical experiences helping patients who had a previously ‘unseen need’ for this nutrient and the significant improvements that come with its replenishment. Plus the deep dive I did into the science of the different forms and their actions last year. In particular, I now have 2 families where the TCNII SNP is evident in mum and all her children. No gene testing necessary, the pattern is self-evident once you know what to look for and the clear ‘call to action’ – more B12 please! And just this month, a fresh aspect has come to my attention in regard some brand spanking new research on B12 and IBD and the microbial (im)balance of this vitamin as a pivot point for the pathophysiology. Wowza! Early days, but I think we’re headed next level on this nutrient again! And I can’t say, I’m surprised. For while I don’t think the CHOICE of the supplemental form for B12 is complex at all (hence why we need to separate the B12 from the B*S#!) I recognise it is a complex character far beyond what regular dietetics has reduced it to.
B12 is a routinely under-rated and recognised micronutrient, which is in fact in high demand by many of our patients. As nutritional research pushes back against defining adequacy as simply the prevention of the deficiency-associated disease (macrocyctic anaemia, irreversible neurological damage) we enter a new landscape of more individualised approaches where we’re better able to recognise and treat those at risk of falling below ‘optimal’. But how do we accurately identify this and then choose the ‘best’ B12 (methyl- cyano- adenosyl- hyroxo-) supplement? Does it need to be this complex? Time to sort the B12 from the B*S#!! This recording comes with a bunch of great resources including a clever clinical tool.
I say: Biotin, Broccoli Sprouts & Bone Broth You say….?
If you said: ‘Sulphur’, go directly to the top of the class, passing ‘Go’ & collecting $200 on your way!🤓 If you nervously said…”I don’t know, they all start with ‘B’ ?”, you are not alone. In fact, most integrative health professionals aren’t aware of the Sulphur Strategies they’re using, probably, everyday. But it’s time we all were.
How about this list? Glycosaminoglycans (GAGs for joint, gut etc tissue integrity), Cerebroside Sulphate (Myelin), Metallothionein, Glutathione, Hydrogen Sulphide (H2S), Co-Enzyme A, Lipoic acid, SAMe, are just some things Sulphur is essential for.
I could go on…and on and on. You see Sulphur, in spite of being an essential macromineral (adult dietary requirements > 1g per day) and critical to health, remains largely unseen. Often we don’t know when we’re writing patient prescriptions that actually we’re using a particular vehicle for Sulphur and therefore we’re also not able to discern which, of the very long list of options (dietary and supplements), makes the most sense in this patient at this time. We’re not to blame, not many ‘possess the power’ to see it, it seems. Por old essential, irreplaceable Sulphur doesn’t even have an RDI. But the time has come to take a good look. We need to know how patients are able to meet their needs, who needs more and how, very commonly, someone who is seemingly ‘consuming enough’ may still exhibit a functional Sulphur deficiency with poor musculoskeletal tissue integrity, low white cell replication capacity or higher oxidative stress load etc and in those who do have a shortfall, how to treat successfully & safely. Who needs a top down approach (more protein, methionine, cysteine, bone broth) and in whom would that be a risky path and using ‘downstream’ Sulphur products instead would be a better balance of pros and cons?
Because all Sulphur needs to be handled with care.
That’s right. Like other highly chemically reactive minerals, with reactivity comes risk – a great potency that requires careful consideration of both form and dose, so that we can harness this power for good not…well evil’s a bit strong…but how about, for not-good. I’m a bit of fan of Sulphur and using Sulphur strategies in my patients. I think it has interesting echoes with our past: the ‘healing’ waters of a Sulphur Spring and of course even further back the old ‘brimstone and treacle’ medicine of eons ago. This paper by Nimni in 2007: Are we getting enough sulfur in our diet? got me thinking about Sulphur again in a contemporary context, over a decade ago, I’ve done a lot more thinking, researching and prescribing since then but it seems that Sulphur still remains ‘unseen’ by most. But with the rise and rise and rise of popular Sulphur-based supplements (alpha lipoic acid, GSH, N-acetyl glucosamine, Brassica & Allium extracts and concentrates, N-acetyl-cysteine etc) I think it’s time to talk.
If you don’t have a clear picture of the gross daily requirements, determinants of altered individual needs, sources, regulation & associated deficiency picture of Sulphur, you’re not alone. Turns out this essential macromineral remains ‘unseen’ by most, even though you’re probably writing prescriptions everyday that have Sulphur as their key component. From the simple: Taurine, N-acetyl cysteine, Protein powders, to the sublime: Brassica extracts & concentrates, N-acetyl Glucosamine, Alpha Lipoic acid etc. In order to use these Sulphur strategies successfully and safely, however, we need to fill in the missing detail on its metabolism, the difference between the ‘organic’ and ‘inorganic pools’, how regulation regularly goes wrong, even in those seemingly consuming enough, and how to balance the risks of this reactive medicine with its substantial therapeutic value. This recording comes with a great clinical tool to help you at last see the Sulphur strategy most indicated for your patient.
The latest Update in Under 30 has landed!!!
You can purchase Unseen Sulphur – Time to Take a Lookhere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.



 MasterCourse I: Comprehensive Diagnostics.
MasterCourse I: Comprehensive Diagnostics. 
 You can purchase
You can purchase