Do you realise we’re often giving our patients Crabs? Stay with me 🙄 We’re all BIG fans of polyphenols right, but did you know that one of the key ways they qualify as antioxidants is that they chelate metals?
Chemically speaking that means that polyphenols (flavonoids, isoflavones, tannins, stilbenes etc) have a structure that looks and works like two ‘crab claws’ 🦀 the ends of each claw attracting and binding metal ions, following which, the claws kind of ‘close’ around the metals and trap them within. 🦀
Now sometimes the closing of those claws results in a clear ‘stop & block’ effect – the metal will remain trapped and be lost from the gut or other parts of the body along with the polyphenol but not always…other polyphenols can be favourable chelators just temporarily binding a metal but ultimately making it bioacccessible to us and increasing its bioavailability & bioefficacy. So polyphenol prescriptions, aka ‘crab medicine’, need to be precise. Every different class of chelator or ‘binder’ e.g. MCP, zeolites etc will have different metal affinities. Our beloved polyphenols have a predilection for one metal above all…and that happens to be iron!
As clinicians, we can harness their polyphenol power to either enhance iron uptake or block it.
🦀 Both actions, of course, well indicated in different patients & presentations 🦀
In the latest Update in Under 30 we write a polyphenol program for those individuals ‘on the road to iron overload’, who simply ‘can’t close the door to more’! Knowing how to perfect this prescription and still allow for personalisation & preferences etc is the key to sustainable essential everyday iron mitigation between blood removals and to minimise the need for these. And if your bigger challenge is the issue of iron deficient patients who are refractory to your well-reasoned remedies then take a listen and a look at the accompanying resource and ensure they are doing the exact opposite! I am being completely serious. I don’t think many people realise the power of the polyphenols & how pervasive they are in our herbal & dietary recommendations 🤓😲🤯
For those individuals with HFE mutations on the road to iron overload, whether they ultimately reach that destination of absolute hyperferritinaemia or not, excess iron mitigation ‘every day & in every way’ is key to better outcomes. While avoidance of dietary haem iron and, where indicated, therapeutic phlebotomy, are cornerstone treatments, patients are increasingly being offered add-ons such as PPIs and pharmaceutical chelators. However our polyphenol prescriptions (both food form and nutritional & herbal supplements) offer additional novel actions to address excess iron mitigation, while also providing patients with improved cardiovascular protection, immune system support etc. This recording comes with an incredible resource for both you and your patients. Packed with evidence-based options they can choose from at each meal & across the day, it offers them their own tailored treatment plan by identifying options as (un) favourable, & therapeutic in each category of food, beverage, even cooking methods.
You can purchaseThe Power of Polyphenols In Iron Excesshere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
It’s no secret I am in the midst of some serious deep-diving through the micronutrient evidence base & at a depth of about 30 metres I struck Boron! Don’t yawn! I saw that. Thinking, ‘boring’, when we hear, ‘Boron’, is almost as bankable as watching everyone reach for their water bottles when you mention anything hydration-related 🤣 But I am here to restore your positive regard for this mineral and remediate its bad (& boring) rep! In preparation for the Nutrient Prescriber’s Program we started each nutrient review with the seminal contemporary nutritional texts and then launched ourselves headlong into the latest & greatest research. By the end of all the Boron bits in all my trusty texts the yawn was not gorn! But the moment I started reading the research I was like, ‘Are we even talking about the same thing?!’Turns out we’re not 😵🤦♀️
You see Boron has been a longstanding victim of identity theft. What we’ve been lead to believe is Boron is weed-killer and ant-poison and look it does give us some of the benefits of Boron but not all. And it possess a pharmacokinetic & toxicity profile that naturally occurring Boron simply does not.
Who decided that the Boron that is ubiquitous in our environment but almost exclusively consumed by us only after biotransformation by plants – could just skip that last bit and still be safe and optimally beneficial?! Probably the same guy that came up with folic acid, may I suggest? Anyway, enough is enough. We all need to relearn Boron – naturally occurring Boron – in the form of Sugar Borate Esters (SBE)- the evidence of benefits for which will blow all of our little minds! Well it certainly blew mine! Looks like this natural form of Boron is going to hit the Australian market in the not-too-distant-future 🐦 can’t wait to see which supplier is sufficiently progressive and research-aware that they bring this to market, having been available as a high grade supplement, employed in numerous RCTS OS for some time. But this little Update in Under 30 is not waiting around for that release date – there is much to be gained from SBEs right now – so make some noise as the real Boron at last takes the stage!🎤
Boron has been the victim of longstanding identity theft and we unknowingly have been interacting with its imposter. Contrary to everything you’ve ever been told about this mineral, naturally occurring Boron is full to overflowing with benefits for our gut, our bones, our brain, our management of other minerals and is safe in large quantities. That ‘bad guy Boron’ you were introduced to and is still present in many of your supplements is a form we never consume in food…and therein lies a world of difference! Come meet the real Boron so you and your patients can get the real benefits!
You can purchase The Boron Deception: How We’ve Been Fooledhere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
Still. And yes – like you – I don’t see any slowing down any time soon in this extraordinary paradigm shift occurring in medicine and health. Which for us humans involves one humbling discovery after another.
Here we were thinking we made our dietary choices from a place of free will & individual preferences 🤣🦠
Thinking those microscopic mates, were making those B vitamins, and SCFAs and and and…for us & our benefit 🤣🤣🦠🦠
And while there’s a lotta love going on between our microbes and our micronutrients – in both directions – Pat Benatar said it best, “Love is a battlefield”
(sorry but I feel compelled to insert a link here for the youngsters – you’re welcome 😉)
The tussle over who gets to access those nutrients that are actually essential to both of us (the hostage and the microbiota) is an absolute turf war, peeps, and this battleground has seen some bloodshed! The new new question being raised is how the prescribing of nutrients, especially at the higher doses we tend to use, trickles down to influence and impact those microorganisms who reside in the bowel. Directly – as a selection pressure we have, likely unintentionally unknowingly, introduced. Which species do well when exposed to levels of a vitamin or a macro or trace mineral that are simply unobtainable in the diet? Yes – research answering these questions has begun in earnest revealing some positive ‘prebiotic-like actions’ of some but not of course for all nor in all scenarios. Want to learn more about this latest aspect we need to consider when formulating our nutrition prescriptions? You can either jump in and join us in the Nutrient Prescribers Program which kicks off next week to get across absolutely everything new in nutritional medicine or just dip your toe in here with our latest Update In Under 30: The Micronutrient Microbiota Universe
The world of health science went microbiota-mad a few turns back and there’s no sign of an end. Research continues to reveal the breadth of the GIT microbiota’s positive & negative reach, in particular, & with discovery upon discovery we’ve come to understand how often the microbiota are ‘managing us’. Both in terms of being integral to the success of our digestive, immunological, metabolic etc processes but also in a self-serving way, for example, directing our dietary preferences to satisfy their own needs. This has understandably prompted the question about the impact micronutrient supplementation is unintentionally having as a selection pressure on our gut microbes. Which bugs like which B vitamins when taken in excess of the amounts achievable in the diet? And which microbes flourish and which falter when we radically change their mineral exposure?
You can purchase The Micronutrient Microbiota Universehere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
I’m such a sucker for marketing!…ZoomZoom is from an old Australian car ad – an earworm clearly conveying ‘ the speed of something’, and let me tell you, totally fitting for this little Zinc tale I’m about to tell! Many years ago, I wrote a thesis on Zinc that necessitated me reading every research paper ever written (that’s how it felt anyway!🤪) on this trace mineral. Like everything in nutritional medicine, especially in the area of our burgeoning understanding of micronutrients, this is a highly dynamic space, so regular reviews of what’s new is essential and, since my thesis, part of my regular practice. Well, I just did my latest deep dive, and HELLOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO radical paradigm shift(s)…yep plural!
Zinc supplements should ideally be: Organic amino acid chelates Taken daily – due to the lack of Zinc stores in the body Taken fasting Taken in doses in excess of the RDI to compensate for the smaller % absorbed
Yep – nope. Or in true-blue Aussie: Yeah, nah. Can’t believe what you’re reading right now? Neither could I when I undertook this recent review but the studies are increasingly sophisticated and the resultant paradigm shifts are being echoed, reiterated & reinforced. And these have, in turn, challenged all those old ‘norms’ about how best to administer zinc for those patients with a shortfall. If you’d like to take this little journey for yourself…I suggest you start here! I immediately changed how I take it myself and now my mission is to both spread the word and get us all reflecting and reviewing our prescribing principles around Zinc…and tbh, around all micronutrients! After spending my ‘summer’ doing sufficient reading for a second thesis on everything new in micronutrients…I am armed and dangerously prepared for our upcoming *NEW* program: The Nutrient Prescriber’s Program which kicks off in late Feb for 5 months.
I truly believe that based on all this new information, we can now get so much more out of our medicines.
Nutrition represents such an extraordinary set of tools for us to work with, but it’s time to sharpen those tools in terms of how we apply them!
The Changing Zeitgeist Of Zinc Prescribing
Zinc research is a highly dynamic field and given its relative recency of discovery as being essential to humans, we’re still in the early days of truly getting to know this mineral. In just the last few years, enormous gaps have been filled-in regarding its regulation and roles that look to radically change our prescribing practices. Tune in to this essential update for some serious food for thought about doses and dosing frequency.
You can purchase The Changing Zeitgeist Of Zinc Prescribinghere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
Wow, menopause is really having a moment, isn’t it? Or is that just me (and my mates who are all somewhere on that perimenopausal path)?! But seriously, medical perception of this reproductive transition is undergoing a revolution right now—widening the lens to take in more diverse potential presentations and lengthening the period of impact recognised both ‘before, during, and after’ that last, last…no hang on…last period. But I fear we are at a crucial crossroads. Anything could be related to (peri)menopause, but not everything is or should be.
There are several other conditions whose onset tends to rise or peak at the same age and stage for women, and due to their shared features, they get missed & misdiagnosed, misattributed to that!(more…)
Any steps towards inclusivity in societal & cultural terms are cause for celebration but in medicine, that can come in the form of a ‘diagnosis of inclusion’, the opposite, of course, of a ‘diagnosis of exclusion’ and potentially as slippery and loose as it sounds. That’s the somewhat precarious position we find ourselves presently in with perimenopause and menopause. With greater recognition of just how long health effects can kick in before there are any cycle changes [2-12 years for those of you playing along at home] and the widening lens now taking in the diversity of such health effects, women’s health has had a win. But, I would argue, this is not without a double edge. After all, aren’t we, as a result, more at risk, as women, of having everything attributed to “just ‘the change’, love”, and, in turn, going to be offered sex hormones more often as the solution?
Recently I asked practitioners to tell me where the ‘therapeutic reference range’ many of us were taught for nutrients comes from & no one has been able to answer that.🙄 If you’ve heard me refer to my original naturopathic education before you’ll know I generally hold it in high regard. And I’m forever mindful that there are always things that can be made better. What’s been playing on my mind lately is the recognition that I originally learned nutrition from one (exceptional) individual, and then went on to become the lecturer years later at that same and other institutions. Additionally, I am aware of some of my past students also going on to become the next generation of nutrition lecturers at those same places – and often in fact inheriting their lecturer’s notes, slides, overheads [showing my age!!] with the job. Can anyone else see a problem here? What’s brought this into sharp focus lately are many of the questions I’m endeavouring to answer as part of our much-anticipated Nutrient Prescriber’s Program. How much? How often? When? Which form when? & For how long? Which are the key questions we have to answer with every single nutritional prescription.
To not only source the most rigorous scientific answers to these core critical questions but to also develop a framework that we can all use to answer them for ourselves at the point of any future prescription creation, I have had to go to great lengths.
But as I research & write, I also keep asking myself, ‘How would ‘old-me’ have answered this?’ How did I up until now either consciously or unconsciously answer these sufficiently to make such decisions?
So it’s an ongoing little (& sometimes BIG🧠) internal debate that is raging as I write. And when I ask current praccies these questions they reflect back similar ‘old-me answers’, the vast majority of which were handed to us by our lecturers with plenty of top-up ideas from industry. These answers include things like:
How much? Somewhere within the therapeutic dose range? How often? Depends on lots of things but generally aiming for daily of course!
When? Minerals before food, fat soluble vitamins with or after, magnesium at night etc
Which form when? Now it gets tricky – because there are all these new forms that we weren’t even taught – but maybe ‘active’ – active is always better, right? Or is that natural? The most bioavailable?
& For how long?Ummmmm how long is a piece of string?! Until the signs and symptoms resolve?
Now all of these as general statements are partly correct. And with respect to the level of understanding we need to have when crafting a nutritional prescription for a specific patient, with a specific presentation and for a specific purpose (correction of deficiency Vs supranutritional Vs therapeutic antagonism etc)…well they are plain wrong in the majority of instances. Don’t freak-out in freefall!🪂 The prescribing of nutrients is a wonderful and typically, a wonderfully safe, modality that offers us the potential for extraordinary patient outcomes. When used well. We could all benefit, I believe, from just sharpening our tools so we bring out the very best in our medicines & in ourselves, as prescribers & clinicians. I am neck-deep in writing the 10 modules that can start us all on that journey. Want to join me?
And to be clear, about the educational echo chamber,
In the past I was part of the problem and ever since I have tried to be part of the solution.
With over a decade of mentoring practitioners, Rachel has recognised a need for an educational program that provides practitioners with more structure, more science, and therefore more certainty in navigating each individual prescription. This monthly meet-up is delivered in 5 live sessions and runs from February to June (10 modules). All sessions, encompassing both theoretical and applied learning will run for approximately 2 hrs each.
Let’s play a word association game of minerals & their major roles
I say, ‘Potassium’. Maybe you say, ‘Sodium Potassium Pump’ I say, ‘Magnesium’. You say, ‘Muscles?’ I say, ‘Calcium’. You say, “Bones’….
But I say, Second Messenger. And arguably the most pervasive & potent one, at that. Remind you about second messengers? Well, sure. They are the ones who get sh*t done. Not like a boss (i.e. hormone or neurotransmitter) who shout directives from above but never step foot inside the dirty guts of the engine room itself. It’s the second messengers who run these messages from the outside of the cell to the inside and the engine room, to ensure that the directive is actually actioned! Amazing huh! And free calcium in the blood is, as I said, really a superhero even among the second messengers – with its regular responsibilities including: Insulin, TSH, Adrenaline, Oxytocin, Serotonin receptor activation etc etc
Does, it have a dark side? Well, sure. Don’t most superheroes?
If the available Calcium in blood and the extracellular environment is too high then basically bad sh*t gets done. Including vasoconstriction, clotting, deposition of calcium in the wrong place like arteries and joints and etc etc. That’s why the amount of Calcium in our blood is the MOST tightly regulated of all electrolytes and, in turn, has the NARROWEST of reference ranges. But will a Serum Calcium level always tell you when there is a problem with Calcium regulation? No. You’d need to have measured the major regulator itself, Parathyroid Hormone (PTH). Wait, am I seriously trying to tell you, that Serum Calcium alone can look completely normal in spite of really damaging Calcium dysregulation underway – leading to accelerated BMD loss, increased cardiovascular and renal risks etc.? I most certainly am.
So do you know which of your patients’ really need PTH assessment and why 1 dominant group amongst those, is any woman leading up to and following menopause?
No? Well you better pull up a pew and have a listen and a watch then! Yes this latest Update in Under 30 episode even comes with a little video tutorial!🤓🤯
Parathyroid hormone is a career criminal. In addition to buoying dropping blood calcium levels via legitimate means, it illegitimately achieves this by stealing it from our bones. But you wouldn’t know it – because like all career criminals this occurs completely under the radar. Elevated PTH, however, constitutes the most modifiable risk factor for bone mineral density loss & fracture risk and offers the biggest BMD gains secondary to its normalisation. In addition to this, even within range but ‘high-normal’ PTH correlates with a range of other cardiovascular and urinary presentations & if combined with elevated serum calcium can become a multi-systemic presentation (GIT, Mental health etc) frequently mistaken for other aetiologies. So how can we be alert to this ‘bone thief’? Which of our patients will benefit the most from PTH measurement and monitoring? This recording, resource & video tutorial on how to use a Ca PTH Nomogram answers all!
You can purchase Unmasking Hyperparathyroidism – Menopause & Morehere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account. You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
I shared this recently on socials but for those of us that don’t hang around that ‘hood I am sharing again here because it is just too important. While we’re busy updating our knowledge regarding reproductive health for women (soooo many huge headlines of late!)…ahhhhh…this might be something we all want to read!🤓
This thought-provoking reviewchallenges the long held assumption that oestrogen is at the root of much breast cancer causation. Instead it creates the case for PROGESTERONE as the actual source of oncogenesisand relegates oestrogen to merely (but monstrously) fanning the flames.
Now before anyone panics (?too late ) you need to read the article in its entirety – esp this not being about demonstrable differences in measurable P4 levels – and keep in mind that this hypothesis, though well argued and supported by evidence also from trans-gender individuals, is not currently a consensus. BUT what I think it does really well is SHAKE THE TREE🌴🥥 and prompt us to challenge our own biases and blind-spots. For far too long in IM Oestrogen has been made out to be the baddy. I too am guilty of having done that. And Progesterone everyone’s saviour! Of course there are a lot of PMDD sufferers who have good grounds to punch us for even suggesting this.
But of late – many of my peers have helped remediate oestrogen’s reputation and put us back on a more balanced path – I am thinking of @Sandra Villella especially here.
Who straight away responded to my post regarding this on socials, “I just got back from the Australasian menopause Congress in Queenstown, and the different types of exogenous progestogens are certainly implicated in breast cancer.” And then generously shared some of the hot off the press slides and stats from the Australasian Menopause Society.
In a nutshell she says, “Breast cancer increases with age and with increased time of use and those increases are greater when Progesterone is included in the MHT prescription”
And whoah…maybe we all need to rethink all the pro-progesterone prescribing…dare I say?!
Btw – the article implies that having anovulatory cycles might actually be protective too!!
Not my normal space and speciality area but I keep finding these gems in women’s hormonal & repro health and I feel a duty of care to share!
Update and Under 30 Podcast episodes are streamed monthly audios and resources to keep you up to date with the latest ‘must-knows’ in integrative medicine, covering a wide variety of topics from diagnostics to diet, all through the lens of an integrative health model. Every month each new episode will provide you with a quick scientific review with ‘clinic-ready’ practice tips, in under 30 minutes. In addition, the subscription gives you access to the ENTIRE back catalogue of UU30 audios that have been released…that’s over 120 episodes! You can become an Update in Under 30 Subscriber to access the entire library of Update in Under 30 audios and resources here.
The debasing of BMI as a stand-alone assessment of weight is long overdue given its significant limitations and lack of meaningfulness with respect to overall health. This coincides with a bigger societal and cultural shift towards inclusivity which involves redressing bias against people with diverse body sizes and compositions.
And how do we, as integrative health professionals, continue to uphold our principles of prevention and treating the cause when excess adiposity may be a very real contributor? While ensuring we ‘see’ and treat each individual in front of us, not our assumptions about adiposity, not our body size bias nor blind spots?
One part of the answer: read and be led by their lab results – because pathology is nothing if not personalised.(more…)
I can barely bring myself to write the word given how overused it has been of late 🤐🙄😯😕🙃 But I gotta say something! If we have found ourselves currently in a place where every second (or indeed single!) patient has a ‘histamine issue’ then I am afraid that it is we, that have an issue. (more…)
Rachel: And sometimes emails from practitioners provide me with both the question and their own answer to their question even!
Cameron Barker’s (Ex-student long-term learner & mentee)email arrives titled:Unexpected Source of Iodine in Placenta Caps?!
A 32 yo female with a 12-week-old daughter came to me as she was not feeling well, in particular, she reports fatigue, racing heartbeat, anxiety and loss of appetite. Previously, 2 years ago, I had helped her with her Hashimoto’s. I did not hear from her for a year or so and she fell pregnant and was recommended to take a well-known iodine-containing pregnancy multi.
Over the years I’ve observed an increase in the incidence of practitioner paralysis. This occurs typically & understandably in the face of fearmongering. A good example is in the area of so-called ‘methylation medicine’ where we’ve been lead to believe that writing ‘the right’ nutritional prescription for patients requires a) their full gene profile, b) a knowledge of biochemistry that no one outside of a legit biochemist should have (!) and c) a bordering on perverse interest in in vitro research looking at how these pathways interact with different nutrients. And if we, as mere mortals (and naturopaths, nutritionists, herbalists or integrative pharmacists or GPs at that), are lacking in any of these WE WILL STUFF THIS UP GLOBALLY and put them on THE WRONG THING THAT WILL BE CATASROPH*C! Note: fearmongering always uses caps 😉
This stems from the misguided belief that ‘biochemistry alone maketh the man’ and ‘SNPs should write the ‘script!’
And the source of these falsisms are, what I refer to as, ‘Wallys with wall charts’. As impressed as we might be by individuals with brains for biochemistry or genetics, we should not let this overshadow the knowledge that health and disease are much more than 1 or 2 facets of your gene profile and how this may predict the pace of a few out of a million chemical reactions. Right? I mean I doubt any of us working in integrative health would intend to be so reductionistic and yet here we are with practitioners forgoing clinical (and RCT) evidence over that derived from in vitro with respect to supplements like SAMe and N-acetyl cystine, or worse still, taking as gospel, ideas that have come from pure hypotheses, based on 1 SNP out of an individual’s whole gene profile! This has infiltrated many areas of naturopathic and integrative medicine and certainly gotten the best of me at times too. But I am pushing back. Enough is enough. We humans are not our gene profile and holistic practitioners like us – know the manifold influences upon our health and wellbeing better than just about anyone else. And if you feel a bit lambasted by my little tirade – know that I have to give myself this very same talking- to every now and then – when I fall under the spell of Wallys and their wall charts!
In part one, we discovered the pro-drug nature of SAMe, revealing why evidence obtained from in vitro evidence can not be used to support either favourable claims or warnings. In the 2nd instalment we examined up close the misunderstandings about SAMe use in conjunction with antidepressants and clarified the real causes for concern in mental health clients. In this 3rd and final part we dissect claims and ideas about the success or safety of SAMe as a supplement with respect to methylation genetics and stages of pregnancy. All up this is indeed one BIG SAMe rethink that we reshape and re-inspire you about its prescription.
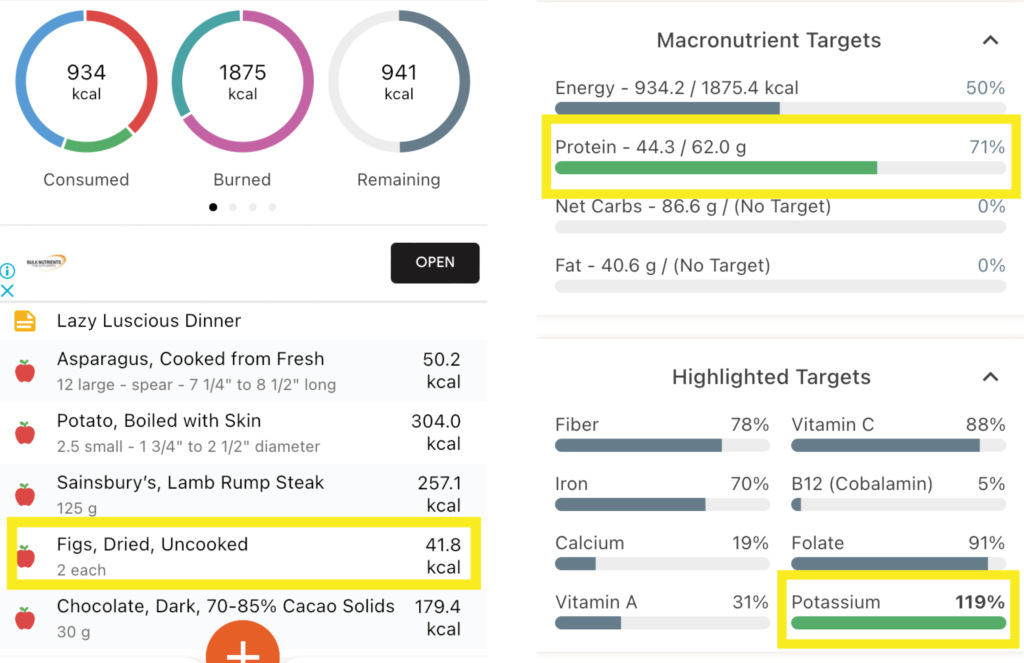
And for weeks now I’ve really been banging 🥁🥁 The 1st drum was me making us all salivate & suffer through my month-long Mediterranean feast The 2nd, my ongoing incurable fixation on the ‘Power of the Ps’ – Protein & Potassium, not just individually, in terms of meeting optimal requirements for each, but relationally, as in, the (im)balance between them & the clear goals that have come from research for best health outcomes.
Maybe now you can hear the individual drumbeats merging to form some sort of chorus rather than a cacophony?! I can🎶 And largely that’s because I decided to put the Ps & Ps principles (Total Protein:Potassium < 1; Animal Protein:Potassium <0.6 etc) into practice, entering my own meals into software to see how often I kicked each goal and how often I missed (& [ouch] kicked myself). Personally, I think thirty years in the game can lead to some laziness around looking in depth at our own dietary habits. As in, I know the ‘rules’ right, back to front, so I’ve told the ref to have the rest of the season off! My meals are both mantra and memory foam. There’s a lot of eat and repeat. Like my heavy lunchtime reliance on my ‘protein power pack’: 2 XL soft boiled eggs on 1 piece of avocado paleo toast and a bunch of asparagus. My (in)famous buckwheat breakfasts loaded with nuts, yoghurt & fruit. My bulk-cooked plant protein heavy, animal protein light, stews, sauces and soups. Even, what I considered my laziest but luscious organic farmers market meal, pan fried lamb rump steak, steamed fresh new season potatoes & a bunch of asparagus. So which of these would you have put your money on for the most Ps& Ps goals kicked? 🤓🤯
The Lazy Luscious Steak & Veg Meal Wins with… Total Protein : Potassium of 0.56! Animal Protein : Potassium of 0.41 Btw that’s because of the Potassium-punch of Potatoes [>2200mg!] and the finale of Figs & dark chocolate [329mg]! Animal Protein : Vegetable Protein of 2 : 1 (ok so you can’t win everything!)
Now obviously I am just looking at each meal individually, but the Protein & Potassium goals are really daily ones, however, I, like most people, don’t lay out the totality of my ideal food intake for the day and then think, now how do I make this all edible?! I think in meals not metadata! So this little exercise was already incredibly rich in insights, checking my assumptions and snapping me out of some misguided mental calculations into the real world, placing a ref back on the pitch! I’m not ditching any of these favourites – just more mindful of what meal goes with others across the day, for better balance. Now all this analysis is time-consuming of course and while various software will do the macro and micro crunch, as far as I know, you still need to do all the Protein and Potassium calculations by hand, Ah yup. So, 1) I’m stopping now & 2) I’m thinking about creating a little spreadsheet that auto-calculates a lot of these targets once you’ve obtained that basic elemental data to input, for easier use in the future – would you use it?? [insert answer here 🙋♂️]
And then you can show me your kick arse protein/potassium combo! Because clearly even us ‘experts’ apparently need data to double-check our assumptions!
Now where’s the other 🥁 in all this, that Mediterranean one, I hear you ask? It’s in the figs! My lamb dinner actually just missed reaching the targets for protein and potassium balance…until my fig finale! And remember, what the Greeks say, ‘A few figs a day keep the chronic-mild-metabolic-acidosis at bay!’ 😂 Just jokes…
To prevent or minimise our slow but steady march towards sarcopenia, the need for dietary protein adequacy to fuel muscle maintenance is a no-brainer – but how does ageing affect this? We get less bang for our buck. We have to eat more, to get the same ‘amount’ but do you know why this is? Add to this, that also as we age, we experience a greater acid burden from a lower acid dietary load. And given that a higher acid load (PRAL), has been shown to have a negative effect on muscle and bone markers in the past, clearly to ensure optimal health of our bones and muscles as we age, we have a riddle, or two, we need to solve. How do we use Protein and Potassium intakes to benchmark our patient’s diet quality and musculoskeletal risks and can we modify their consumption of either, to drive therapeutic gains in terms of both BMD and muscle?
You can purchase The Protein & Potassium Riddle of Ageing – Muscles and Boneshere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
How much? How often? When is the best time & timing? do you know about friends, foes and frenemies? Which form, when? e.g. building blocks or bioactives? And for how long? aka are we there yet…?
These are the kind of questions that one would imagine nutritional prescribers can always answer – but can you? Yet this is the goal, right? So that with each and every unique individual who needs supplements – we have a clear, consistent go-to framework to guide & direct these prescriptions. One that makes scientific sense, offers optimal outcomes and removes the uncertainty.
From my interactions with thousands of practitioners, however, I know many of these key questions plague practitioners & they feel, at times, as if they’re flying without a net, or without a strong systematic approach, or at the very least without all the answers to these questions.
I’ve had so much good fortune & so many others to thank for providing me with this foundation. Fay Paxton – my nutrition lecturer in my under-grad who indoctrinated me with a systematic approach. Dr. Tini Gruner – my principal supervisor at SCU, who shared & further fuelled my passion for biochemistry and reading labs to extract insights into each individual. And thanks also to all the pharmacists I’ve delivered education to over the years, who, as a result of their grounding in the principles of pharmacokinetics, always ask the best questions – questions that if I don’t know the answer I know I need to know the answer! So I made it my mission to find out!
While we dip into these aspects of nutritional prescribing in our regular mentoring groups on an ‘as needs’ basis, I’ve decided the time has come to create a year-long program dedicated to sharing this information and building this skill-set in practitioners.
This monthly meet-up is delivered live (max 1.5hr) and runs from Feb to November with the following currently proposed format *subject to change dependent upon the needs of the group
Feb Factors Affecting: digestion, absorption (host, form, dose)
March What happens to what gets left behind? e.g. enhanced enterocyte micronutrient concentrations & their effects plus unabsorbed nutrients & their interactions with the colonic environment
April What happens to what’s absorbed e.g. distribution, hierarchy of needs, activation and deactivation
May The pharmacokinetics of prescribing
June Where do our ideas on dosing come from? e.g. Physiological Vs Pharmacological dosing & actions. The basis & believability of maximal intake boundaries?
July Bioefficacy V Bioequivalence. Beyond building block nutrients: Is ‘Bio’ (-active, -peptides, -materials) always better? e.g. GABA Vs Glycine, NAC Vs GSH, PLP Vs Pyridoxine, Niacin Vs Niacinamide riboside ——————————————————————Aug month off—————————————————————————
Sept How often & for how long? Are we there yet? And how would we know? Plus Fast Vs Slow Nutritional therapeutics
Oct Strategies for Supplement Success e.g. friends, foes and frenemies in nutrition underpinning principles with examples; compliance changers for clients
Nov Live attendance & opportunity to participate in a case-based mentoring session
This monthly ‘live’ meet up will be delivered as part of 2023 Group Mentoring as The Nutritional Prescribing Program Group Mentoring applications open 17 October 2022.
To join the waiting list and be notified when applications are open, email the team at [email protected]
Find out more about what groups are available for Group Mentoring in 2023 here.
Have you been told somewhere by someone that the ‘perfect’ TSH is 1.5 mIU/L? This is a wonderful, terrible & wonderfully terrible example of ‘magical numbers medicine’. As a push-back against the published reference ranges we’re given, that are so wide you could drive a truck through them, there has been an over-correction by some, leading to the myth of ‘magic numbers’. We can narrow the reference range substantially for many parameters with good rationale, make no mistake about that but once we start setting ‘aspirational goals’ that are explicitly rigid…well we’ve done 2 things 1) forgotten about the patient to whom this result belongs and 2) disregarded viewing each result as part of a ‘pattern’, that we must piece together and make sense of.
Back to TSH then… if my obese patient had a value of 1.5 mIU/L this in fact would be woefully inadequate – so too a child at any weight.
And we expect a higher value as well in our elderly clients too and this level there may be, in fact, increased mortality.
But the same result would be excessively & worringly high in my patient who’s undergone thyroidectomy.
Realising the full value of any test result in terms of what it reveals about the person sitting in front of you, requires these more thinking and more thoughtfulness. Unfortunately, a list of ‘magic numbers’ will often lead you astray. And building your scientific knowledge about labs will not only help you avoid the pitfalls of pathology but will strengthen your pathophysiology prowess in surprising ways, saving your patients a packet in terms of additional extraneous testing and help you truly personalise your prescriptions…because the ‘invisible (biochemical individuality, oxidative stress, genetic probabilities, subclinical states, imbalanced or burdened processes etc) just became visible’. I started requesting lab results early in my career and years later was lucky enough to be taken under the wing of Dr. Tini Gruner. I found some of our shared notes, from 10 years ago, scribbled all over patient results recently and I was struck by just how lucky I was to have her encouragement to really pursue my interest and how she was a guiding force about learning to recognise pathology patterns over single parameters. A decade on I can concede, much of my clinical and educative success has come off the back of this foundational skill-set and I know, this is true for so many I’ve taught too.
“The guidance I’ve received over the years from Rachel in relation to pathology interpretation has been one of the most valuable (and fascinating) investments I’ve made as a clinician. Her teachings have filled gaps in my knowledge base I never knew needed filling and have significantly enhanced my understanding of the inner workings of the body! Rachel has an incredible ability to make the numbers that patient’s so often present us with, both understandable and clinically meaningful. The knowledge I’ve gained by investing in this skillset has paid off in dividends and I’m certain will continue to do so into the future.”
Stacey Curcio – Cultivating Wellness
I hope you’ll join me for the most exciting up-skilling opportunity in learning labs yet. Oh…and all this talk about thyroid testing..this next MasterCourse series is focused on revolutionising your understanding of thyroid, adrenal, HPT & HPA markers based on the very latest research & findings & marry these together with everything you learned in MasterCourse I (ELFTs, FBE, Lipids & Glucose) to understand the ‘whole story’.
…an absolute treasure trove of free integrative health information about your patient!
DEEP DIVE INTO REAL CASE STUDIES TO DEMONSTRATE EACH PATHOLOGY PATTERN IN ACTION. ]\
There are limited places. To sign up for Rachel’s LIVE Series – MasterCourse II: Thyroid & Adrenal Diagnostics and for more information click here.
One of my dear friends told her husband several years ago that she had noticed he was now making, ‘old man noises’ upon standing up from couches & chairs. She told him that must simply stop. She pointed out that he was only 50 and that she neither could nor would listen to that for another 40 years!
He stopped!
But aging and old (wo)man noises are coming for all of us, right? And by the time we’re making those noises or excusing ourselves from certain activities due to sore, dodgy or NQR [insert joint or body part], we’ve spent several decades unknowingly right on course to get here! We don’t generally pay any attention to our ECM (extracellular matrix) which suffers in silence, slowly but surely losing its structural & functional integrity from the age of 18 on, until we reach the tipping point: joint degeneration, repetitive soft tissue injuries etc, and a problem that will never be silent again! Cue your choice of anti-inflammatories it seems – til death do us part!
The Ageing Matrix is a thing.
And no I haven’t seen the movie – I don’t need to – I’m living it.
When I was pregnant I thought I wanted to specialise in pre-conception & pregnancy care. Then my babies arrived and I took a fancy to paediatrics. Sound familiar to anyone? Now, unsurprisingly, I have a real thirst for knowledge expressly aimed at bettering this whole ageing-thing! So in preparation for this Update in Under 30 episode, I’ve relished the opportunity to put the Ponds Institute & all similar cosmetic companies on notice! Scrutinising their claims that every woman on the planet would do better with more Collagen, more Elastin, more Hyaluronic Acid, just more of every key ECM component really. Ok, but in accordance with my bias and my business, my lit review pertained to oral supplements, not outrageously priced magical middle-life-crisis rubs and the therapeutic action I had in mind was the integrity of our ECM, and the roughly 2kg of collagen, we rely on, for functions a lot less frivolous than stopping sag. I have to say, I started out as non-believer but the research was quite the awakening…still there’s a lot to unpack here in order to repack our ECM and prevent against the erosion of its integrity and everything we build, and rely on, upon it – to live well!
Osteoarthritis (OA), like osteoporosis, is a diagnosis made after decades of disease. Underpinning it all, is our aging Extracellular Matrix (ECM) with its characteristic compositional change that leaves us vulnerable, from the ripe old age of 18! The ECM, like all other tissues, is made from basic building block nutrients but presented in their most fanciest of forms with triple helix structures, aggregates and other large molecular weight components, that each possess remarkable physico-chemical properties & convey extraordinary functionality to structures like joints. But is prevention against, and effective intervention for, OA as easy as consuming more of these ECM biomaterials?
You can purchase Supplementing Collagen & ECM Biomaterials – What’s the story?here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
I’ve spent the best part of about 4 months recording my *NEW* Advanced Thyroid Assessment training. I told my team this would be easy and quick, given it was to be based on a great little 2-part, 2hr updated presentation I delivered just last year for ACNEM!! Sixteen weeks (like seriously…most of it) numerous rewrites and retakes later, our final product is 4 parts that goes for over 12hrs in total & has a bonus Adrenal recording! And yeah my team are impressed but unimpressed too if you know what I mean?!🙄🤪
Every time another, ‘Oh wow!’, or ‘No way!’, escaped my lips, it was a source of personal celebration, as another deeper layer of learning revealed itself.
But to the wonderful, somewhat weary and definitely wary Sally, who does all my powerpoints, it was met with, ‘Oh boy!’, because it meant many multiple new slides to build full of visual metaphors, animation acrobatics, if not an entire new Part!*#@^
Her sage advice along the infinite research road I’ve been travelling was : ‘Stop. You’re going to have to stop.’
So I didbut now I am this meme. Everything I see currently through the lens of thyroid health, I talk in tongues TFTs and my brain is one giant neural network of integrative endocrinological circuits! I have fallen in love with this topic, this neuroendocrine axis and its ‘first responder’ role all over again! Hence our little thyroid character below – all ‘antennaed’ up – is one of the many tools we’ve developed for this training, to teach us that ‘bad thyroids’ per se are extremely rare – but bad scenarios are common (too much or too little of any macronutrient, key micronutrients, a change in the internal or external environment etc etc) and this little fellow and his board of directors (no – not the hypothalamus or pituitary!) – well it’s their job to ‘read the room’, right?!
In the absence of this key understanding we risk: A lot of lazy labelling in thyroid health – ‘You have a bad thyroid – that’s why you…[can’t lose weight, feel tired, have SIBO etc]’ Misdirected treatment & especially a tendency to overload the butterfly with ‘thyroid’ nutrients – which can do more harm than good
I’ve said many times, ‘perfect number pathology is a myth’ but it runs rife in practitioners’ beliefs about TFT results with complete disregard of the person those labs belong too! Did you know, for example, that your TFTs should all be higher if your BMI is? That your T4:T3 ratio should never be 3:1 if you are on replacement, have hot nodules, are pregnant or are acutely unwell etc etc etc? How about how low your Selenium or Iron levels need to be before this factor will influence the actual levels of thyroid hormones measurable – & what the impact of these deficiencies are well before then that is far more sinister and serious? Yep…you see here I am, pouring just some of the tiny take-homes of Advanced Thyroid Assessment ALL over you!
Watch this space my new Thyroid training is just around the corner!
An increasing number of our patients have thyroid concerns but unbeknown to many of us the most likely explanation of all is thyroid nodules, whose incidence is on the rise globally. The development of nodules has always been primarily viewed as a nutritional disease. Traditionally attributed to chronic iodine deficiency but recently novel nutritional causes have emerged. Benign nodules come in 2 flavours: hot and cold and while patients can present with a mixture, it is the presence or absence of a hot nodule that radically changes what complementary medicines you can and can’t use and what an effective treatment plan looks like. The pointers, as is often the case, are there for us in the patient’s presentation and pathology, so knowing the difference is no longer a guessing game. This UU30 comes with a great visual clinical resource and includes key papers on the nutritional management of nodules.
We all (inaudibly🤞) sigh when patients utter this & adopt the brace position for whatever mis- or dis-information may follow.
So how would you feel, if instead, these were the words of the health professional you’re seeing?
We could debate forever the pros and cons of FB and its forums – & indeed it offers both – but one thing we must never lose sight of is what it has in common with the ‘wild west’: unregulated, unvetted, and with plenty of cowboys – often sadly, masquerading as experts, or just ‘very “generous” very very active group members’, with hidden agendas. I don’t generally engage with the naturopathic forums but occasionally I catch sight of things that I can’t look away from, and I can’t not speak up. Recently, someone (with a not-so-hidden-at-least-to-me-agenda) was raving about the dangers of N-acetylcysteine as a supplement & the way it was spoken about made it seem like it would be *poison* at any dose. Wha? As you may have learned from me it is definitely potent and in turn, demands our respect as a powerful therapeutic agent – directing our decisions about timing and reminding us, yet again, that least dose is best dose. But what this individual was purporting were adverse effects I’d never heard of in relation to this nutraceutical. So I simply asked, ‘Can you please share your reference(s)?’
Prior to me inserting myself into the comments – there had been enormous engagement specifically with this individual’s claims- which mostly went like this: ‘Oh wow! I didn’t know this!!’ ‘Thank you – that’s so interesting!’ “Oh that explains why Tom doesn’t like it, and Dick won’t take it and Harry says it’s horrible!” 🤦♀️
FB forums – seeking out the support & opinions of our peers can be truly wonderful but it can totally derail our knowledge too if we don’t keep checking the quality of that information. A simple: Can you share your references, or, where did you learn this? Should be part of the respectful and expected scientific discourse in our profession. I’ve asked that before when I’ve found myself yet again in a forum thread and had a truly fabulous response – with the practitioner generously sharing a number of high quality published articles that would have taken me ages to find myself! 💪Not the case in this recent episode. The 3 distinct claims, which all centred on NAC being bad for high histamine individuals, were ‘substantiated’ by just 1 primary reference & that was a Poster Presentation: “Human placental tissue was minced and subjected to a fractionated ammonium sulphate precipitation (35% / 65%). A fraction high in DAO activity was purified using hydrophobic interaction chromatography (HIC), and incubated with the drugs in prescribed concentration” . The full research has never actually been published in its entirety and the brevity of detail on a poster means you know barely any of the important details regarding the methodology. I also looked for any other research that emulated these methods or findings or even cited this paper – nada. And if you lead with your best – this was appalling low level evidence that is really unlikely to be relevant. But hey – here’s the 1 provided reference – make your own mind up! (see how easy that is?!)
I asked for clarification and for papers to support the other 2 claims. Silence.
But actually before silence a bit of ‘How dare you ask!’
That’s when I got a different insight into this forum & arguably a culture that doesn’t foster curiosity & questioning, if that risks challenging the ‘poster’s’ position. And when several incredibly intelligent, kick-arse clinicians quietly contacted me on the side to say, ‘THANK YOU!~ This person posts comments like this all the time & it’s so misleading & someone needed to say something, but it probably had to be you.’ Well that really made me 😥 because it didn’t, you know – any one of us can ask, “Can you share the reference(s) for that?” and clearly we need to more often 🤓
Why are we afraid to question information or ask for references and why are people afraid of the question? This should not be a competition or hierarchy of who can ask or not ask questions. And if the forum that you’re a member of makes it seem that way – then ask yourself, if its doing you more harm than good.
Aren’t we on the same team here? We all have a professional duty of care to our patients to ensure that in looking for quick answers we don’t get incorrect ones that misinform us, our patients and our treatment decisions.
Over years of delivering independent education in integrative health I have spoken to some diverse audiences. This has included health professionals from very different backgrounds: from hospital-based psychiatrists & mental health nurses, to whom I presented on site in hospitals both in Australia & NZ, to a national sparkle-arkle speaking tour, in front of large groups of aesthetic practitioners. They’re the doctors & nurses for whom botox and fillers are their tools of trade, and yes I got to see actual demonstrations of their work performed live!!!😶 More recently, I’ve had several opportunities to deliver evidence-based independent education on nutrition to pharmacists en masse – which I always enjoy because they ask some of the best questions!
Underpinning each decision to accept an invitation from a 3rd party, be that a company an organisation or an institution, to speak, is: 1.The realisation of an opportunity for nutritional medicine to reach more people, a wider audience, & ultimately expand the circle of influence amongst health professionals, who interact with & advise the public at all different levels 2. An agreement and/or contract that ensures my independence, the correct use of my materials, image, brand and IP & removes any expectation to promote their products/services etc
And my ‘door’ is open to any invitation which meets these 2 criteria. So you might have seen my name, previously associated with some brands or organisations, in the last few years disappear off their speaker announcements, or no longer connected, and in turn you might see my name pop up in new places! Like….Metagenics Congress on Autoimmune Disease!! After many invitations from this company, that I wasn’t able to previously accept, I am pleased to be speaking at this face to face event on the Gold Coast in August. What a novelty, hey? Face to face?! My talk is about the 4 Mistakes not to Make in Hashimoto’s and as always, I’ve completed a full mini-literature review in order to speak to the very latest on diagnostics and nutritional management, in this condition. Yes, to quote a Costanza, “We’re back baby, we’re back!” And to see my full current smorgasbord of speaking commitments & all the people I am ‘spreading the (nutritional) word’ to – just click here.
This previous training will take your understanding of the interplay between food, nutrition, environment and the thyroid several steps further. With more supportive research and a greater focus on the mechanisms behind the relationships between these macro- & micro nutrient & environmental factors, this presentation is for the true thyroid die-hard.
 Do you realise we’re often giving our patients Crabs? Stay with me 🙄 We’re all BIG fans of polyphenols right, but did you know that one of the key ways they qualify as antioxidants is that they chelate metals?
Do you realise we’re often giving our patients Crabs? Stay with me 🙄 We’re all BIG fans of polyphenols right, but did you know that one of the key ways they qualify as antioxidants is that they chelate metals? 

 Wow, menopause is really having a moment, isn’t it? Or is that just me (and my mates who are all somewhere on that perimenopausal path)?! But seriously, medical perception of this reproductive transition is undergoing a revolution right now—widening the lens to take in more diverse potential presentations and lengthening the period of impact recognised both ‘before, during, and after’ that last, last…no hang on…last period. But I fear we are at a crucial crossroads. Anything could be related to (peri)menopause, but not everything is or should be.
Wow, menopause is really having a moment, isn’t it? Or is that just me (and my mates who are all somewhere on that perimenopausal path)?! But seriously, medical perception of this reproductive transition is undergoing a revolution right now—widening the lens to take in more diverse potential presentations and lengthening the period of impact recognised both ‘before, during, and after’ that last, last…no hang on…last period. But I fear we are at a crucial crossroads. Anything could be related to (peri)menopause, but not everything is or should be.


 You can purchase
You can purchase 


 The debasing of BMI as a stand-alone assessment of weight is long overdue given its significant limitations and lack of meaningfulness with respect to overall health. This coincides with a bigger societal and cultural shift towards inclusivity which involves redressing bias against people with diverse body sizes and compositions.
The debasing of BMI as a stand-alone assessment of weight is long overdue given its significant limitations and lack of meaningfulness with respect to overall health. This coincides with a bigger societal and cultural shift towards inclusivity which involves redressing bias against people with diverse body sizes and compositions.