As Britney so famously put it, ‘Oops, I did it again!’ I remember the actions on my to do list but not the intended recipients! D.O.H. I was talking with a practitioner the other day who lamented that she had never really learnt about stats nor how to assess the quality of research in her undergraduate and could I point her in the right direction towards a resource that simply explains this increasingly important basic skill-set…well I would if I could remember who you were!! Anyhoo, I followed through in my usually dogged way to the bottom of my actions list and with the help of a lovely past-intern, got directed to these free BMJ resources on how to read research…G.O.L.D.
Anyway…while I continue to ponder who this was actually intended for… it dawned on me how many people would just LOVE these & benefit from them immensely in the meantime. Couldn’t most of us do with a little more research literacy? So I thought I’d share. Don’t you love it when we work as a team. Now…who can help me find my keys?! 😉
It’s starting to feel a lot like…that Update in Under 30 time of the month!
Update in Under 30 are dynamic power-packed podcasts that will help you keep abreast of the latest must-knows in integrative medicine. Focused on one key issue at a time, Rachel details all the salient points so that you don’t have to trawl through all the primary evidence yourself. All topics are aimed at clinicians and cover a range of areas from patient assessment to management, from condition based issues to the latest nutritional research. Most importantly, each podcast represents unbiased education that can contribute to your CPE points, so if you haven’t subscribed yet…what are you waiting for??!! 🙂
Never say never, right. Back in my old uni teaching days, I scorned the very notion of treating someone with ‘actual melatonin’. Always in favour of upstream approaches over downstream, I was keen instead to give patients the ‘ingredients & cofactors’ so they could whip the right amount up themselves. Well fast forward another decade in clinical experience, and research too, and while I refuse to give in with many other ‘replacement remedies’, melatonin, has snuck well and truly into my list of treatment considerations for some very specific presentations such as silent reflux, treatment refractory GORD and Barrett’s oesophagus, buoyed by some amazing clinical successes. So much so…that in fact I’ve embraced this replacement approach, whose results in this setting especially, can’t be replicated by treating with ingredients and cofactors. Turns out of course I am not alone – melatonin has won a lot of fans over the last decade.
A recent Australian article from 6 minutesrevealed a significant increase in GPs prescribing melatonin for sleeping issues in children and then of course, there is its substantial use in cancer and typically at mega-doses that will make your toes curl.
But always in the back of my mind is the old me. Whispering things like, ‘ but melatonin isn’t a nutrient, nor a herb, so it’s not naturopathic’ – hence we can’t even prescribe it, needing to refer patients to others for access and yet more pressing, ‘what do we really know about the full implications of replacing such a potent and ubiquitous neurotransmitter?’ I know. This old me, she’s annoying, right.
But she’s also important.
So absolutely perfect timing then to hear about a homegrown (2 Aussie Naturopaths in fact) systematic review on the adverse effects & safety of melatonin which is full of important and surprising info and I think ….everyone…single…one…of…us needs to read it:
“While this review reveals a high degree of safety for melatonin with few adverse events that cannot be easily avoided or managed in most populations, it also reveals lack of clarity regarding melatonin’s relationship to endocrine processes, and its effect on hypertensive patients and potential drug interactions in this population.”
But the devil is in the detail.
So here’s a newsflash for you – 4 human studies found melatonin had negative effects on key aspects of reproduction, like sperm counts and ovulation and not at mega-doses my friends, no…at 2mg/d over several months. We shouldn’t be surprised, right, melatonin is critical to fertility cycles in all other animals…but how many health professionals know this, or not just know it…but make our recommendations with this in mind? Other studies reported fascinating impacts on insulin sensitivity (5mg) and amazingly, (or not being the king of all things circadian), opposing effects depending on the time of administration. Then there’s the drug interaction with anti-hypertensives…a negative one, I must add. No information still unfortunately about the impact of long-term replacement on our own endogenous production. Anyway…enough spoilers… READ THE ARTICLE. This hasn’t wiped melatonin off my list of potential recommendations all together but it has given me some serious food for thought and much greater clarity about in whom this suggestion should be off the menu.
‘Melatonin – Misunderstandings and Mistakes’ – this important 2017 clinical update about what we are getting right and wrong with Melatonin answers in particular, one of the most common sources of fascination & frustration for clinicians, the reasons behind the Melatonin non-responder. We’ve all encountered patients who have taken Melatonin for sleep problems and reported no benefit, or initially responded and then lost efficacy quickly, or even patients who experienced insomnia after taking. What does this tell you about your patient and what should you do to resolve this and better still, prevent it? This UU30 from 2017 reveals all!
While this ABC article is written for the public it’s a great checklist to have written up somewhere to prevent against placing your confidence in the wrong sources of info.
Just recently, I had a practitioner ask about the ‘risks’ of B12 dosing…& while B12 is considered to be free of a toxicity profile in just about any textbook or in-depth review paper you can find, a ‘methylation’ expert had made mention of there being demonstrated increased oxidative stress.
My response, ‘Have you checked their references?’ Their response,’No’
I get it, right, we’re all busy people and don’t have the time for a full literature review of every claim made by every educator, ‘expert’ or company… BUT sometimes a credibility check can be lightning fast!!!! As was the case in this instance.
I did check this expert’s reference (singular). I read the full article just out of interest but actually, I didn’t need to. I had my answer just by reading the title and abstract…the study was conducted in genetically altered rats made alcoholic and injected with B12 or something to that effect. Relevance?? Which is in stark contrast to the absolute consensus from 100s of human studies concluding that B12 toxicity is NOT a thing.
That also means this particular expert’s references probably need to be checked every time of course…until you can be more confident in the quality of their claims – tough but true. Below are the 7 top Qs to try and answer to determine the quality of any claim – and remember you rarely have to complete the list to get your answer…just start with reading the title of their key reference!!!
1. Who says? (….and what agenda/bias might they have) 2. Sample size ( a response rate of 20% might mean something in a sample of 10000 & nothing in a sample of 10!) 3. Lab-bench or real world 4. Correlation V causation 5. Statistically significant V clinically significant (…if something was shown to reduce people’s migraine pain by a rating of 0.5 – but most people rate their pain at 10/10…is it actually clinically meaningful?!) 6. Does the dose relate? (…watch out for animal studies where they are using doses at mg/kg body weight…that we could never match with oral dosing in humans because they would be eating buckets of the stuff!) 7. Got some time?…then dig a little deeper…if your article has passed all the above checkpoints and you’re still dubious (and this does happen!) check out who has cited this paper (easy via Google Scholar) and whether other researchers are in agreement or not with their findings. What’s been published in this area since then?
Oh and this article is also handy for the occasional misguided patient – who’s found some incredulous online info about something that contradicts your contrastingly well-sourced & quality-checked knowledge! 😉
Our new – New Graduate Mentoring Program kicks off in late January and offers an incredible opportunity for successful applicants to develop their core clinical competencies in record time during their transition into practice. Real world research cheat tips, is just one of the many practical competencies covered across the year’s curriculum. But if you’re interested in applying, jump onto it! Applications close on the 15th November
Finally a systematic review puts paid to the nonsense that ‘withdrawal from antidepressants’ is problematic only for a few, is ‘mild’ & ‘lasts only 1-2 weeks’ with no treatment necessary other than reassurance, which is still being perpetuated by current prescribing guidelines both here and overseas. In fact their review found that 56% of patients experienced problems with stopping antidepressants and the majority of these rated these as ‘severe’. Back in the good/bad old days when I worked for a pharmaceutical company who made psych meds the phenomenon of an ‘initiation phase’ during which time suicidal risk was heightened, was acknowledged and freely discussed…in-house at least. However, the concept of a ‘withdrawal syndrome’ was less clear. Anyone who has witnessed patients coming off ‘even the cleanest’ SSRIs will speak to a potential myriad of worrisome experiences including…
“Typical AD withdrawal reactions includeincreased anxiety, flu-like symptoms, insomnia, nausea, imbalance, sensory disturbances, and hyperarousal. Dizziness, electric shock-like sensations, brain zaps, diarrhoea, headaches, muscle spasms and tremors, agitation, hallucinations, confusion, malaise, sweatingand irritability are also reported (Warner, Bobo, Warner, Reid, & Rachal, 2006, Healy, 2012). Although the aforementioned symptoms are the most common physical symptoms, there is also evidence that AD withdrawal can induce mania and hypomania, (Goldstein et al., 1999; Naryan & Haddad, 2011) emotional blunting and an inability to cry, (Holguin-Lew & Bell, 2013) long-term or even permanent sexual dysfunction (Csoka & Shipko, 2006).”
Previously termed ‘discontinuation syndrome’ by expert panels – to distinguish these inconvenient effects from the more seriously viewed (read nasty) benzo-associated discontinuation problems – was an act of smoke and mirrors, according to this scathing and insightful review by Davies and Read, who argue strongly this is a clear cut withdrawal picture and it deserves as much consideration and concern. In particular they point out that of course, patients can experience these symptoms even without ‘discontinuation’ – but simply as a result of a delayed or skipped dose, an intentional dose reduction etc. And they provide the alarming context that one third of people in the U.K. (and likely similar developed countries) who take antidepressants for more than two years have no evidence-based clinical indications for continuing to take them. But wait..I’m just getting to the worst bit, this is the part that gets me personally…having been a peddler in the past of these meds and in certain patients still spruiking their benefits, I am in no disagreement about them being necessary, helpful & even life-savers in some patients…yes I have seen this too many times to ignore it…BUT…and now this is where I start raising my voice a tad….
Patients need to make informed choices, and having a clear understanding of what you are likely to experience on any given medication has been shown to improve outcomes but according to the 2 largest surveys conducted to date,< 2% of antidepressant users are being told any of this. Do you know why? Well, let’s start with the misleading guidelines… if the RACGP says it isn’t so…then can we expect their GP to know or say any differently?
Grrrrrrrr…. yes that’s me…not a wild animal in the room with you.
Because you know what happens in the absence of this?! And let me say I have also seen this too many times to ignore as well, people feel compelled to stay on them & this is truly heartbreaking to witness. The experience of a reduced dose or a period without is so terrifyingly disconcerting to that poor unsuspecting individual, and without explanation, is misinterpreted by them (and according to this review often by their doctor as well!!) as being either a sign of their inherent mental instability and need for ongoing medication, or misdiagnosed as a separate condition. Ok…apologies, this is over a decade of pent up frustration…resurfacing as a result of reading this incredibly important and disturbing review. I think I need a little lie down now 🙁
Helping patients off anti-depressants is a challenging and important function that must be initiated by the patient with the full support of the prescribing practitioner, however there’s a role for complementary medicine here too. Rachel walks you through a range of strategies and when you might consider each. Listen to thefree samplehere from the Update in Under 30 from 2013 – Leaving Anti-depressants Behind. Or perhaps you’re interested in all things Mental Health and should find out more about our specialist mentoring group running in 2019.
So we already know that thyroid problems can start in utero, right…but a recentMedscape review(the fountain of thyroid information that I frequently drinketh from 😉 ) on Hypothyroidism in childhood taught me a couple of big things I hadn’t known before!
The diagnostic criteria for subclinical hypothyroidism are raised TSH levels in combination with a normal concentration of free serum thyroxine (FT4) but because there are some differences between accepted ranges in TSH assays, high-risk groups should be screened, especially babies with malformations, whose mum received steroid treatment during pregnancy or in the neonatal period, or who had existing thyroid dysfunction, TFTs (or at the least TSH as part of what’s called the Neonatal Screening test) should be repeated 2 weeks later. But now comes the couple of big light-bulb moments: the incidence of eutopic thyroid in twin births is nearly double compared with singletons! As you know, I’m a mother of twins and I’m guessing at 18yrs old now (and multiple peachy TFTs 😉 ) the horse has well and truly bolted for my two but geez…I had no idea of the dramatic increase in risk. And it keeps going…monozygotic twins very commonly show a delayed TSH rise and those numbers are even more prominent in multiple births. The other not-so-fun-fact is the discovery that subclinical hypothyroidism in IVF babies is approx. 10% which is noteworthy considering none were observed in the control group.
This obviously left me thinking “W.H.Y?” And of course…the first place my head goes with the latter…is iodine.
The reasons behind our increasing rates of thyroid dysfunction across the life-stages are multifactorial (and don’t get me started on the very real contribution of EDCs!) and how, in spite of iodine adequacy being the first thing on the checklist for thyroid health, so many health professionals ignore this, at their patients’ peril… But now at least we know that patients with IVF babies, twins, and preterm bub, who are currently not included in the prioritised screening groups should be…and of course we should keep asking the questions, “what are the mechanisms behind this, why is it so?”
So if this has made you even more curious about the incredible butterflied-shaped gland and you’d like to go for a stroll on the vast plains of “thyroidisms” you can click on this link Thyroid Assessment in Kids and Teenagers and get completely “thyroided” up. There is always more research to come our way so keep your eyes and ears peeled.
A few months back I seriously ‘blew over’. Not on an RBT but on a UBT (Urea Breath Test). In spite of it being not the kind of test you want to score top marks for, my result was in the high 2000s, when all I needed was around 800 to confirm, and anything over 50 to be suspicious, that Helicobacter pylori had taken up residence in my stomach lining. I tell you, I knew it when I blew it! 😉 After ingesting the radioactive urea and waiting to blow up my sampling balloon, I felt like I could still fill a room full of balloons with all the gas being produced in my stomach and those balloons, I imagined, would all rise to the ceiling as if full of helium! Yep…I burped all the way home, which was representative of what I’d been experiencing daily for a month beforehand and what lead me to get the test done.
But initially, it wasn’t so clear.
The very first symptom I experienced was a sudden onset of severe tightness around my throat that lasted for minutes but started to happen multiple times in a day. Yep..no one panic. Together with a strange sensation of ‘extreme emptiness’ in my stomach on waking or delayed meals, and then mild nausea both with an empty and full stomach…only some days or weeks later the fabulously-unprecedented-&-socially-adorable-burping started, proper.
So a month or so later, I’ve solved my own mystery. Happy? Not in the least…where the heck have I picked up H.pylori from? Yes…that’s what I said because it had to come from somewhere people…right? I think there is much we have misunderstood about this bacteria with an incredibly long and interesting human history. Animals don’t and can’t carry this bacteria. The evidence suggests that it can’t survive for very long in the environment either (approx 4 days) but that is long enough to get into our food and water and maybe even onto shared chopsticks…just saying (listen in to hear the lowdown on all these and more!) Essentially hoomans are the traffickers, people! In fact one of the things that surprises people the most is the very high prevalence in young children and the clusters of positive tests & identical strains within families…but once you learn a little more about this bacteria…it won’t surprise you at all.(more…)
As an avid reader of medical news I face a barrage of headlines both domestic & international everyday. I feel this is important for many reasons – not just so that I know what’s being said about their medicine but what they’re saying about ours as well! Anyone see the jaw-dropping headline last week: Could Probiotics be bad for your gut? Yep.
Now how many of you didn’t make it past the headline? It’s hard isn’t it.
There’s almost a reflexive shutdown for many of us to dismiss such a proposition as simply ‘ridiculous’, surely on par with our response to an article from a climate skeptic…as we shake our heads with ‘you gotta be joking right?’… but unless we read on, we’ll never know. (more…)
Too many times we see thyroxine treated patients on the ‘set and forget’ setting. Often, they’re taking the same dose they started on a decade or so ago, in spite of weight changes, ageing of course and new comorbidities. They’ve undergone limited monitoring, with just an annual in-range TSH viewed as confirmation of efficacy. But is it? Many patients’ re-emerging hypothyroid signs and symptoms would suggest not.
A recent Medscape review article of a large study by Gullo et al 2017, identifies another shortcoming in the rudimentary way we ‘replace thyroid hormone’, in all patients but especially in those who’ve had their thyroid removed.(more…)
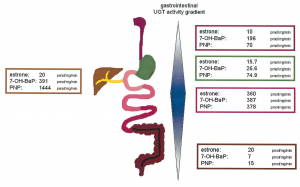
I’ve had my nose in all the research on Gilbert’s Syndrome again..watch this space…in the interim just thought I’d share this image and a couple of important details I may not have been able to convey when you last heard me talk (very fast!) about this important and common polymorphism:
While the incidence is approximately 10% of Caucasian population, rates are heavily influenced by ethnic background and the highest rates (up to 1/4) are seen in Middle Eastern populations
Gone are the days of thinking this condition only effects bilirubin levels and the enzyme responsible for its clearance – more recent research has shown over 3/4 of patients with Gilbert’s Syndrome have multiple SNPs that compromise clusters of enzymes within the glucuronidation pathway – with varying patterns – this goes a good chunk of the way to explaining the variability we see in bilirubin levels and symptom pictures across patients all deemed to have Gilbert’s Syndrome. This also explains why figures of reduced glucuronidation activity vary anywhere between 10% less to 90% less! It depends on your cluster..but the average reduction is around 50%
UGT enzymes, the ones affected in Gilbert’s, are also expressed all the way down the GIT and constitute important food and drug handling. These UGTs are most active in the small intestines,as you can see above, but may explain why Gilbert’s patients are ‘more sensitive’ to medications than just paracetamol!
And are you still thinking you need to run an $$$ gene test to confirm your Gilbert’s hunch in a client whose bilirubin sits consistently high normal or high? Think again… here’s a great little diagnostic short-cut that even theRoyal College of Pathologists Australasiacites as sufficient evidence to confirm the polymorphism:
In the face of elevated total bilirubin levels and in the absence of liver pathology or increased haemolysis to explain this..”If the diagnosis is uncertain the serum bilirubin fasting level can be measured and should exceed the non-fasting level by >50%.”
Nice. So that means you only need to demonstrate that the patient’s fasting total bilirubin levels go up by at least 50% compared with their fed levels and BINGO you have your diagnosis. Much easier. Oh and this image comes from an interesting paper from Tukey & Strassburg 2001 – but is probably not for the faint-hearted 😉
Stay tuned for more 🙂
Just new to this condition and need a soft place to land with understanding Gilbert’s Syndrome? This previous UU30 is just the thing! Affectionately called Gilbert’s Girls because in particular it details a set of twins with this condition, this short audio explains the basics about this common polymorphism and why we tend to see a lot of patients who have this…even if no one has pointed it out to them yet! You could be the first to provide them with this important understanding about how genetics is impacting their detox pathways, changing their sex hormone handling and perhaps setting them up for both mental health issues and some serious upset guts! Better still, what to do once we have that diagnosis.
With many of the mentoring sessions I run, I suspect there’s often a misperception that the learning is one way. Part of what thrills me about being a mentor is all the learning opportunities I am personally presented with.
Recently, I had an exceptional example. You see, I am privileged to have a colleague, Sonya Cacciotti, in one of my groups. She has worked for over a decade in tandem with an extraordinary doctor up here in Ballina, and they have had a particular long-standing interest in sleep quality, assessment and management. Consequently, her knowledge in this area is exceptional, particularly with regard to not just obstructive sleep apnoea (OSA) but the much more and often missed, upper airways resistance syndrome, that is especially common in women. She’s been in my ear on numerous occasions and during group sessions saying, ‘Watch out for this Rachel, it’s more common than we all realise and could be behind many people’s problems‘.
As luck would have it, I have seen a series of cases now within quick succession that all look suspiciously like undiagnosed apnoea or airways resistance. I was listening all along but now Sonya’s wise words and these conditions have my full attention.(more…)
Not long ago, Kathryn Simpson and I were sharing a hotel room on yet another work trip to somewhere. The lights were out, it was way past our bedtime and we were just gasbagging incessantly like a couple of teens, when a thought pops into my head:
“Hey Kathryn, back when you were my student, did you ever imagine this scenario in the future – you know us being colleagues and friends and having slumber parties full of laughing?”, she replied, “Well no, but you know what I REALLY never could have imagined in my wildest dreams…the Australian Naturopathic Summit and you inviting me to be a co-founder of something that’s had such a big impact! That one I just didn’t see coming!”
Well to be honest, neither did I but sometimes I just have an idea that won’t leave me alone and is too important and too promising to ignore. Three years ago when I shared one of these, the vision of a national naturopathic conference by naturopaths for naturopaths, that would lift us all professionally, offer collaboration over competition and provide us the highest level of non-biased education, with Nirala Jacobi, turned out she’d been visited by the same thought bubble. Then I approached Kathryn, who was working for me at the time and pretty fresh out of uni but full of passion and drive about building a better ‘new’ naturopathic career path, one that supported rather than splintered those emerging out of great courses into a harsh, challenging professional space.
Time-travel forward to now, we are just 10 weeks(ish) out from erecting the chai tent, marquees and lanterns, for the second inception of this extraordinary thing called the Australian Naturopathic Summit24-26th August at Lennox Head.
This is the culmination of 3 years of work from us, one paid project manager and the exceptional generosity of over 25 of our naturopathic idols, thought leaders and torch bearers who are donating their time to present plenaries, workshops, case studies, panel discussions… because they believe so strongly in the cause and the need for such an event.
If you think I am running out of breath between all these words..I am. This thing…has taken on a shape and life much greater than even we had envisioned.
If you follow the work I do – you’ll know that I am passionate about collaboration over competition. I could never have come to this place in my career without the input of many (some who remain on speed dial even now!) and through my mentoring programs, the infamous RAN internship and hopefully times we’ve come across each other…I’ve encouraged you to do the same and by doing so, grow bigger together. So just imagine the value of collaborating face-to-face…over 3 days…at a festival in Lennox Heads… ? And not just for 1 hour, but for 3 full days with 100’s of other practitioners from all areas, specialities and locations. Oh and if you’re thinking you’ll just have to wait ’til the next one’…SPOILER…there is no guarantee of a next one! Being a passion project that we 3 donate our time to, for you, it requires your support to keep it going.
So with saying all that…..(cajon roll…that’s a drum for you non-hippies)….It is with great excitement and enthusiasm that today I can announce a special deal for RAN subscribers. Yes….that’s you! Just like myself you all see a need to grow and build skills, knowledge, competence and confidence in the practice of naturopathic medicine. Come join the very best of your profession and take up this special offer to attend the second independent Australian Naturopathic Summit held in Lennox Head on 24-26 August.
To get 15% off a full 3 day pass enter Festival at the checkout
This summit is unprecedented in Australia for the following reasons:
It is free from commercial bias
It is about professional development, improving our practices and career paths, not products
The primary objective is to support the Australian Naturopathic community, celebrating our diversity and creating a platform for our own Naturopathic torch-bearers in various areas (Practice, Research, Herbal Manufacture, Corporate Health, Entrepreneurship etc.) to help light the way for the broader professional community
This year our theme for ANS 2018 is ‘Coming Together On Common Ground’ Naturopathy has many different practices and paths, but we all work for the same purpose, guided by the same principles.
The ANS 2018 program has three distinct themes across the 3 days…
Friday 24 August: Custodians of the Vital Force
Saturday 25 August: Upskilling Your Clinical Practice
Sunday 26 August: The Business of Business Development
The morning of each day consists of plenary sessions followed by a lengthy lunch break that allows for networking, beach walking, guided outdoor meditation, perusing the vendor village, or simply enjoying the festival atmosphere in the beautiful outdoor location that our summit is surrounded by OR for those die-hards some amazing case studies presented by the likes of Jason Hawrelak, Dawn Whitten and Sandra Villella. Afternoon sessions are workshop-style, designed to be more interactive. There are plenty of workshops to choose from to keep you riveted and inspired.
We have created a jam-packed program to do just that. Download your copy of the fullprogram here! ANS 2018 – come join the very best of your profession.
Quite the month for it, I hear. My inbox has run hot with practitioners deeply concerned about some serious finger pointing that’s been going on.
The fingers in these instances have belonged to medical practitioners and the direction they’re all pointing, is seemingly at any complementary medicine their shared patient is taking.
Here’s a couple of good examples: “Your high blood pressure is the result of the combined mineral formula you’re taking!” These were the words of a GP to a 50 something female patient when he discovered she was taking a calcium, magnesium, potassium containing formula. The patient was hypertensive at the initial appointment, at which time the naturopath encouraged her to actually seek review, assessment and prescription of an anti-hypertensive, however the patient declined. The nutritional prescription was recommended in response to high acidity (raised anion gap) and prematurely low GFR (impaired renal function). Patient’s HBP continued to be problematic so the next doctor she sees, points the finger and says, it must be this product!
Would anyone like to explain that to me? In fact, that was my advice back to this very concerned and understandably rattled practitioner…just to cordially request the GP to outline the mechanism by which this might occur. (more…)
You know I’m not one to raise my voice and make scene.
Ok, I always raise my voice and make a scene, but only when I think something really warrants our attention and the issue of under-recognised, under-estimated and mismanaged chronic worms, demands our attention. I’ve been talking about this ever since the first patient stepped into my clinic, a young girl with severe mood issues who just happened to also have treatment-resistant chronic threadworm, and since then, as the volume of patients I see affected by this has grown, so too has the volume of my message. And there’s actually so much to say.
Chronic worm problems don’t always come with an itchy bottom calling card. In fact, many individuals don’t have any of the telltale signs you might be used to screening for. Recent research suggests adult men, in particular, are commonly asymptomatic when infected with them (Boga et al 2016)
So what alerts us as practitioners to the possibility of chronic worms – so many things…but here’s just some thought bubbles to get you started.
Are you treating patients with recurrent or treatment-resistant Dientamoeba fragilis?
Are you seeing women who have thrush-like symptoms, in spite of negative swabs and no benefit from antifungals?
Are you faced with families coming undone because of one child’s behaviour whether that’s aggression, defiance, emotional lability or just serious sleep problems?(more…)
“I always give some Glutamine to heal their leaky gut”
Cue pained expression on my face. No, I’m not a fan. I take that back, I have no problem with the amino acid itself and I’m still in awe of its incredible multifaceted role in the gut. What I do have a giant issue with is the mismatch between everything we are being told Glutamine is going to help our patients with, and the dosages that apparently will do that, and the reality. I know, I’m attacking the Holy Grail of Gut Health 101….right? But it’s time to set the record straight. Firstly, where’s the evidence at in terms of Glutamine interventions in GIT pathology, particularly in relation to reducing excessive intestinal permeability and improving lining integrity Well if you’re a rat – Good news! Rats’ GITs have a greater dependence on Glutamine than ours, a deficiency of this amino produces clear reproducible negative effects and supplementation fixes these brilliantly!
But if you’re treating humans not rats – well – the evidence & the case for Glutamine for the Gut is not so straight forward or impressive.(more…)
They’ve just come from the immunologist, having presented with extensive vitiligo in dad and early stage vitiligo now in their primary school aged son. The immunologist, without running a single blood test, told them, ‘Bad news, you both have autoimmune issues and watch this space because the vitiligo is just the first presentation, there will be more to come’. Slightly unsatisfied with this dead-end conclusion and non-existent management plan, the family then presents at a long established naturopathic clinic to see Anna Sangster, a fabulously sleuth-like detective, who takes her patients’ health very seriously and has the knowledge and skills that make her one of the best at what she does. I can say that because I’ve been mentoring Anna for a long time & she is one of the clueiest practitioners I know.
For example, she knows about the substantial research demonstrating the overlap between thyroid autoimmunity and vitiligo and, in addition to comprehensive case taking, decides some blood tests may provide valuable insight that would help to understand the degree of self-attack from their immune systems, identify if there are in fact already concurrent autoimmune targets and perhaps even provide a clue as to underpinning drivers. Well, look what she found!(more…)
Just finished talking with the fearless fertility naturopathic specialist, Rhiannon Hardingham, who wanted to let me know that after listening to my Update in Under 30: Silent Reflux she’s had a lot of success treating both GORD and insomnia in her pregnant patients. That calls for double the celebration …YAY! YAY!
‘What’s the magic answer?’, I hear you ask…(more…)
That’s me…always questioning the ‘status quo’ and Iodine is the perfect example! The interview I did on this important subject with Andrew Whitfield-Cook from FxMedicine, covers a lot of key areas of confusion & underscores why it’s so critical all health practitioners get clarity on this topic. ‘It’s just a matter of geography’.
You know, I say to people, we can make vitamins ourselves, we can get all sorts of other organisms including animals, bacteria and plants to make vitamins for us, and then eat those…but minerals…our source of minerals…well it all comes down to the rocks and the soil our food itself is grown or fed on. And iodine is profoundly influenced by these factors.(more…)
No, I haven’t gone crazy for the ‘caped crusader’… but I thought that would get your attention…. oh look it did! 😉
I’m off to Melbourne for the ACNEM Conference May 5-6th and Batmania was one of the interim names of this very cool and happenin’ town before it became known as Melbourne in 1837! Things have certainly changed in nutrition and the environment since then and as practitioners we now need to address sometimes very complex dynamics between genes, gut, nutrition and environmental health. Which, luckily enough this conference is all about!
This year’s theme for ACNEM is Health for Life – Mastering the Integrated Approach.
I am fortunate to be included in the exceptional speaker line-up (thanks for lovely sentiments many of you have expressed so far about that 🙂 ) I am presenting on ageing..which many of you know that I am suddenly now very interested in…getting old and all.
“Researchers followed more than 500 women trying to conceive over about five years and found that, overall, those with moderate to severe iodine deficiency had 46% lower odds, per cycle, of becoming pregnant.”
All researchers dream of generating the kind of results that are ground-breaking but sometimes you read about the latest study’s findings and you think, ‘Really, you spent all your time & cleverness for years on this and that’s all you have to show for it!’ Like the study that finally confirmed dog’s can feel empathy (at last thank goodness …phew…cos I had my doubts until they crunched the numbers!)
So too a study published this month on the possibility that iodine deficiency is common in women trying to conceive in developed countries and may be connected to increasing fertility issues.
Stop press! I know…that made you spill your coffee!(more…)
Is this the way of the future for health practitioners interested in patients’ digestion…?
“The team developed an ingestible electronic capsule to monitor gas levels in the human gut. When it’s paired with a pocket-sized receiver and a mobile phone app, the pill reports tail-wind conditions in real time as it passes from the stomach to the colon…The authors are optimistic that the capsule’s gas readings can help clear the air over the inner workings of our intricate innards and the multitudes of microbes they contain. Such fume data could clarify the conditions of each section of the gut, what microbes are up to, and which foods may cause problems in the system. “(more…)