It’s no secret I am in the midst of some serious deep-diving through the micronutrient evidence base & at a depth of about 30 metres I struck Boron! Don’t yawn! I saw that. Thinking, ‘boring’, when we hear, ‘Boron’, is almost as bankable as watching everyone reach for their water bottles when you mention anything hydration-related 🤣 But I am here to restore your positive regard for this mineral and remediate its bad (& boring) rep! In preparation for the Nutrient Prescriber’s Program we started each nutrient review with the seminal contemporary nutritional texts and then launched ourselves headlong into the latest & greatest research. By the end of all the Boron bits in all my trusty texts the yawn was not gorn! But the moment I started reading the research I was like, ‘Are we even talking about the same thing?!’Turns out we’re not 😵🤦♀️
You see Boron has been a longstanding victim of identity theft. What we’ve been lead to believe is Boron is weed-killer and ant-poison and look it does give us some of the benefits of Boron but not all. And it possess a pharmacokinetic & toxicity profile that naturally occurring Boron simply does not.
Who decided that the Boron that is ubiquitous in our environment but almost exclusively consumed by us only after biotransformation by plants – could just skip that last bit and still be safe and optimally beneficial?! Probably the same guy that came up with folic acid, may I suggest? Anyway, enough is enough. We all need to relearn Boron – naturally occurring Boron – in the form of Sugar Borate Esters (SBE)- the evidence of benefits for which will blow all of our little minds! Well it certainly blew mine! Looks like this natural form of Boron is going to hit the Australian market in the not-too-distant-future 🐦 can’t wait to see which supplier is sufficiently progressive and research-aware that they bring this to market, having been available as a high grade supplement, employed in numerous RCTS OS for some time. But this little Update in Under 30 is not waiting around for that release date – there is much to be gained from SBEs right now – so make some noise as the real Boron at last takes the stage!🎤
Boron has been the victim of longstanding identity theft and we unknowingly have been interacting with its imposter. Contrary to everything you’ve ever been told about this mineral, naturally occurring Boron is full to overflowing with benefits for our gut, our bones, our brain, our management of other minerals and is safe in large quantities. That ‘bad guy Boron’ you were introduced to and is still present in many of your supplements is a form we never consume in food…and therein lies a world of difference! Come meet the real Boron so you and your patients can get the real benefits!
You can purchase The Boron Deception: How We’ve Been Fooledhere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
Still. And yes – like you – I don’t see any slowing down any time soon in this extraordinary paradigm shift occurring in medicine and health. Which for us humans involves one humbling discovery after another.
Here we were thinking we made our dietary choices from a place of free will & individual preferences 🤣🦠
Thinking those microscopic mates, were making those B vitamins, and SCFAs and and and…for us & our benefit 🤣🤣🦠🦠
And while there’s a lotta love going on between our microbes and our micronutrients – in both directions – Pat Benatar said it best, “Love is a battlefield”
(sorry but I feel compelled to insert a link here for the youngsters – you’re welcome 😉)
The tussle over who gets to access those nutrients that are actually essential to both of us (the hostage and the microbiota) is an absolute turf war, peeps, and this battleground has seen some bloodshed! The new new question being raised is how the prescribing of nutrients, especially at the higher doses we tend to use, trickles down to influence and impact those microorganisms who reside in the bowel. Directly – as a selection pressure we have, likely unintentionally unknowingly, introduced. Which species do well when exposed to levels of a vitamin or a macro or trace mineral that are simply unobtainable in the diet? Yes – research answering these questions has begun in earnest revealing some positive ‘prebiotic-like actions’ of some but not of course for all nor in all scenarios. Want to learn more about this latest aspect we need to consider when formulating our nutrition prescriptions? You can either jump in and join us in the Nutrient Prescribers Program which kicks off next week to get across absolutely everything new in nutritional medicine or just dip your toe in here with our latest Update In Under 30: The Micronutrient Microbiota Universe
The world of health science went microbiota-mad a few turns back and there’s no sign of an end. Research continues to reveal the breadth of the GIT microbiota’s positive & negative reach, in particular, & with discovery upon discovery we’ve come to understand how often the microbiota are ‘managing us’. Both in terms of being integral to the success of our digestive, immunological, metabolic etc processes but also in a self-serving way, for example, directing our dietary preferences to satisfy their own needs. This has understandably prompted the question about the impact micronutrient supplementation is unintentionally having as a selection pressure on our gut microbes. Which bugs like which B vitamins when taken in excess of the amounts achievable in the diet? And which microbes flourish and which falter when we radically change their mineral exposure?
You can purchase The Micronutrient Microbiota Universehere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
I’m such a sucker for marketing!…ZoomZoom is from an old Australian car ad – an earworm clearly conveying ‘ the speed of something’, and let me tell you, totally fitting for this little Zinc tale I’m about to tell! Many years ago, I wrote a thesis on Zinc that necessitated me reading every research paper ever written (that’s how it felt anyway!🤪) on this trace mineral. Like everything in nutritional medicine, especially in the area of our burgeoning understanding of micronutrients, this is a highly dynamic space, so regular reviews of what’s new is essential and, since my thesis, part of my regular practice. Well, I just did my latest deep dive, and HELLOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO radical paradigm shift(s)…yep plural!
Zinc supplements should ideally be: Organic amino acid chelates Taken daily – due to the lack of Zinc stores in the body Taken fasting Taken in doses in excess of the RDI to compensate for the smaller % absorbed
Yep – nope. Or in true-blue Aussie: Yeah, nah. Can’t believe what you’re reading right now? Neither could I when I undertook this recent review but the studies are increasingly sophisticated and the resultant paradigm shifts are being echoed, reiterated & reinforced. And these have, in turn, challenged all those old ‘norms’ about how best to administer zinc for those patients with a shortfall. If you’d like to take this little journey for yourself…I suggest you start here! I immediately changed how I take it myself and now my mission is to both spread the word and get us all reflecting and reviewing our prescribing principles around Zinc…and tbh, around all micronutrients! After spending my ‘summer’ doing sufficient reading for a second thesis on everything new in micronutrients…I am armed and dangerously prepared for our upcoming *NEW* program: The Nutrient Prescriber’s Program which kicks off in late Feb for 5 months.
I truly believe that based on all this new information, we can now get so much more out of our medicines.
Nutrition represents such an extraordinary set of tools for us to work with, but it’s time to sharpen those tools in terms of how we apply them!
The Changing Zeitgeist Of Zinc Prescribing
Zinc research is a highly dynamic field and given its relative recency of discovery as being essential to humans, we’re still in the early days of truly getting to know this mineral. In just the last few years, enormous gaps have been filled-in regarding its regulation and roles that look to radically change our prescribing practices. Tune in to this essential update for some serious food for thought about doses and dosing frequency.
You can purchase The Changing Zeitgeist Of Zinc Prescribinghere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
Recently I asked practitioners to tell me where the ‘therapeutic reference range’ many of us were taught for nutrients comes from & no one has been able to answer that.🙄 If you’ve heard me refer to my original naturopathic education before you’ll know I generally hold it in high regard. And I’m forever mindful that there are always things that can be made better. What’s been playing on my mind lately is the recognition that I originally learned nutrition from one (exceptional) individual, and then went on to become the lecturer years later at that same and other institutions. Additionally, I am aware of some of my past students also going on to become the next generation of nutrition lecturers at those same places – and often in fact inheriting their lecturer’s notes, slides, overheads [showing my age!!] with the job. Can anyone else see a problem here? What’s brought this into sharp focus lately are many of the questions I’m endeavouring to answer as part of our much-anticipated Nutrient Prescriber’s Program. How much? How often? When? Which form when? & For how long? Which are the key questions we have to answer with every single nutritional prescription.
To not only source the most rigorous scientific answers to these core critical questions but to also develop a framework that we can all use to answer them for ourselves at the point of any future prescription creation, I have had to go to great lengths.
But as I research & write, I also keep asking myself, ‘How would ‘old-me’ have answered this?’ How did I up until now either consciously or unconsciously answer these sufficiently to make such decisions?
So it’s an ongoing little (& sometimes BIG🧠) internal debate that is raging as I write. And when I ask current praccies these questions they reflect back similar ‘old-me answers’, the vast majority of which were handed to us by our lecturers with plenty of top-up ideas from industry. These answers include things like:
How much? Somewhere within the therapeutic dose range? How often? Depends on lots of things but generally aiming for daily of course!
When? Minerals before food, fat soluble vitamins with or after, magnesium at night etc
Which form when? Now it gets tricky – because there are all these new forms that we weren’t even taught – but maybe ‘active’ – active is always better, right? Or is that natural? The most bioavailable?
& For how long?Ummmmm how long is a piece of string?! Until the signs and symptoms resolve?
Now all of these as general statements are partly correct. And with respect to the level of understanding we need to have when crafting a nutritional prescription for a specific patient, with a specific presentation and for a specific purpose (correction of deficiency Vs supranutritional Vs therapeutic antagonism etc)…well they are plain wrong in the majority of instances. Don’t freak-out in freefall!🪂 The prescribing of nutrients is a wonderful and typically, a wonderfully safe, modality that offers us the potential for extraordinary patient outcomes. When used well. We could all benefit, I believe, from just sharpening our tools so we bring out the very best in our medicines & in ourselves, as prescribers & clinicians. I am neck-deep in writing the 10 modules that can start us all on that journey. Want to join me?
And to be clear, about the educational echo chamber,
In the past I was part of the problem and ever since I have tried to be part of the solution.
With over a decade of mentoring practitioners, Rachel has recognised a need for an educational program that provides practitioners with more structure, more science, and therefore more certainty in navigating each individual prescription. This monthly meet-up is delivered in 5 live sessions and runs from February to June (10 modules). All sessions, encompassing both theoretical and applied learning will run for approximately 2 hrs each.
Let’s play a word association game of minerals & their major roles
I say, ‘Potassium’. Maybe you say, ‘Sodium Potassium Pump’ I say, ‘Magnesium’. You say, ‘Muscles?’ I say, ‘Calcium’. You say, “Bones’….
But I say, Second Messenger. And arguably the most pervasive & potent one, at that. Remind you about second messengers? Well, sure. They are the ones who get sh*t done. Not like a boss (i.e. hormone or neurotransmitter) who shout directives from above but never step foot inside the dirty guts of the engine room itself. It’s the second messengers who run these messages from the outside of the cell to the inside and the engine room, to ensure that the directive is actually actioned! Amazing huh! And free calcium in the blood is, as I said, really a superhero even among the second messengers – with its regular responsibilities including: Insulin, TSH, Adrenaline, Oxytocin, Serotonin receptor activation etc etc
Does, it have a dark side? Well, sure. Don’t most superheroes?
If the available Calcium in blood and the extracellular environment is too high then basically bad sh*t gets done. Including vasoconstriction, clotting, deposition of calcium in the wrong place like arteries and joints and etc etc. That’s why the amount of Calcium in our blood is the MOST tightly regulated of all electrolytes and, in turn, has the NARROWEST of reference ranges. But will a Serum Calcium level always tell you when there is a problem with Calcium regulation? No. You’d need to have measured the major regulator itself, Parathyroid Hormone (PTH). Wait, am I seriously trying to tell you, that Serum Calcium alone can look completely normal in spite of really damaging Calcium dysregulation underway – leading to accelerated BMD loss, increased cardiovascular and renal risks etc.? I most certainly am.
So do you know which of your patients’ really need PTH assessment and why 1 dominant group amongst those, is any woman leading up to and following menopause?
No? Well you better pull up a pew and have a listen and a watch then! Yes this latest Update in Under 30 episode even comes with a little video tutorial!🤓🤯
Parathyroid hormone is a career criminal. In addition to buoying dropping blood calcium levels via legitimate means, it illegitimately achieves this by stealing it from our bones. But you wouldn’t know it – because like all career criminals this occurs completely under the radar. Elevated PTH, however, constitutes the most modifiable risk factor for bone mineral density loss & fracture risk and offers the biggest BMD gains secondary to its normalisation. In addition to this, even within range but ‘high-normal’ PTH correlates with a range of other cardiovascular and urinary presentations & if combined with elevated serum calcium can become a multi-systemic presentation (GIT, Mental health etc) frequently mistaken for other aetiologies. So how can we be alert to this ‘bone thief’? Which of our patients will benefit the most from PTH measurement and monitoring? This recording, resource & video tutorial on how to use a Ca PTH Nomogram answers all!
You can purchase Unmasking Hyperparathyroidism – Menopause & Morehere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account. You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
Ever feel like the universe has been preparing you just for this moment? Me neither really…but in this one weird way – yes!
So hear me out.
Thyroid disease as a result of a viral infection was first described in 1902 by Dr Fritz De Quervain and of course he and his ego called it De Quervain’s subacute thyroiditis. For some historical context, this predates the recognised role of iodine deficiency in thyroid disease! Skip ahead almost a century to deep in the 1990s and mini-me was sitting in a uni lecture room [front row & wearing fluro of course🤣] and over hundreds of hours (no scrap that zillions*^# of hours) of lecture content I was exposed to, the description of De Quervain’s Subacute Thyroiditis stood out and stayed stuck to me. I’ve brought it out for a twirl from time to time in the interim with some of my patients & in particular in correspondence with their docs.Skip ahead to the 2020s when we had this thing called. ‘a global pandemic’, and now everyone wants to talk viruses and their broader health implications & as a result, good ol’ Fritz, me and our buddy, De Quervain’s subacute thyroiditis, are all having a moment.
But just to recap – this is (clearly) not new.
What is new is the way this ‘virus of the moment’ has brought this Thyroid V Virus battle to the forefront. We are living an important chapter in history where all the textbook entries on De Quervain’s Subacute Thyroiditis are madly being rewritten to reflect the veracity of this viral attack on the gland and the wide-scale & varied damage that ensues over the months and years that follow. And so many of our patients are the walking embodiment of it – whether that be in the form of low or high thyroid hormones, nefarious changes to gland anatomy only evidenced on US. So what do we need to know? in short, that pathogens as goitrogens have never been more of an issue than right now for ourselves and our patients. And that compared with just our usual desire for comprehensive investigation of the HPT, taking a complete look ‘under the hood’, not only by way of a full TFT and Ab titres but also, wherever there is an additional suspicion – by way of a thyroid US – has become non-negotiable. But regardless of what you find there, once you look, do you know what to do next?
Biopsies and autopsies of diseased thyroid glands alike reveal the prevalence of many common viruses within, setting the scene perfectly for the Thyroid V Virus battle. So, what happens when a virus takes a specific liking to this gland? While there are several different possibilities, one brought to the forefront in recent years is viral thyroiditis wherein stage 1 is ‘spill’, stage 2 constitutes a gland that is now ’empty’ and while stage 3 is reported to be ‘recovery’, this is increasingly scarce – replaced with chronic or recurrent thyroiditis, relapses of previously remitted GD and a doubling of new AITD diagnoses – not to mention the wide variety of unfavourable anatomical changes being found on ultrasound. Comes with a great desktop reference with prescription examples.
You can purchase ThyVIRoidhere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account. You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
What level of Serum Ferritin represents ’empty’? As in complete depletion of iron stores?
Is it any value below the minimum of the reference range? e.g. < 30 mcg/L Or does the bottom of the reference range allow for a buffer and ’empty’ is substantially lower than this? Could patients actually be ’empty’ but still have Serum Ferritin values within the normal range? Could the same Serum Ferritin value occur in one patient on ’empty’ but with adequate stores in another?
Rachel: And sometimes emails from practitioners provide me with both the question and their own answer to their question even!
Cameron Barker’s (Ex-student long-term learner & mentee)email arrives titled:Unexpected Source of Iodine in Placenta Caps?!
A 32 yo female with a 12-week-old daughter came to me as she was not feeling well, in particular, she reports fatigue, racing heartbeat, anxiety and loss of appetite. Previously, 2 years ago, I had helped her with her Hashimoto’s. I did not hear from her for a year or so and she fell pregnant and was recommended to take a well-known iodine-containing pregnancy multi.
Over the years I’ve observed an increase in the incidence of practitioner paralysis. This occurs typically & understandably in the face of fearmongering. A good example is in the area of so-called ‘methylation medicine’ where we’ve been lead to believe that writing ‘the right’ nutritional prescription for patients requires a) their full gene profile, b) a knowledge of biochemistry that no one outside of a legit biochemist should have (!) and c) a bordering on perverse interest in in vitro research looking at how these pathways interact with different nutrients. And if we, as mere mortals (and naturopaths, nutritionists, herbalists or integrative pharmacists or GPs at that), are lacking in any of these WE WILL STUFF THIS UP GLOBALLY and put them on THE WRONG THING THAT WILL BE CATASROPH*C! Note: fearmongering always uses caps 😉
This stems from the misguided belief that ‘biochemistry alone maketh the man’ and ‘SNPs should write the ‘script!’
And the source of these falsisms are, what I refer to as, ‘Wallys with wall charts’. As impressed as we might be by individuals with brains for biochemistry or genetics, we should not let this overshadow the knowledge that health and disease are much more than 1 or 2 facets of your gene profile and how this may predict the pace of a few out of a million chemical reactions. Right? I mean I doubt any of us working in integrative health would intend to be so reductionistic and yet here we are with practitioners forgoing clinical (and RCT) evidence over that derived from in vitro with respect to supplements like SAMe and N-acetyl cystine, or worse still, taking as gospel, ideas that have come from pure hypotheses, based on 1 SNP out of an individual’s whole gene profile! This has infiltrated many areas of naturopathic and integrative medicine and certainly gotten the best of me at times too. But I am pushing back. Enough is enough. We humans are not our gene profile and holistic practitioners like us – know the manifold influences upon our health and wellbeing better than just about anyone else. And if you feel a bit lambasted by my little tirade – know that I have to give myself this very same talking- to every now and then – when I fall under the spell of Wallys and their wall charts!
In part one, we discovered the pro-drug nature of SAMe, revealing why evidence obtained from in vitro evidence can not be used to support either favourable claims or warnings. In the 2nd instalment we examined up close the misunderstandings about SAMe use in conjunction with antidepressants and clarified the real causes for concern in mental health clients. In this 3rd and final part we dissect claims and ideas about the success or safety of SAMe as a supplement with respect to methylation genetics and stages of pregnancy. All up this is indeed one BIG SAMe rethink that we reshape and re-inspire you about its prescription.
You know the saying, ‘If I had a dollar…’, well there’s so many ways I could finish that sentence, especially in relation to the most common questions I’m asked by praccies on a weeklybasis and ‘Can my patient on antidepressant ‘X’ take SAMe?’, would be in the top 10! While many of you might be mouths agape reading this, I bet the cause of that comical expression is not the same for everyone. Yes, like you, they’ve read the mandatory label warning: ‘individuals who are using prescription antidepressants or suffer from bipolar depression should not use this product unless under the supervision of a healthcare practitioner’ – but let me ask you, how do you interpret that? Turns out there are several interpretations and the most common is the most incorrect.
Yes you heard me. It’s time to remove that stain on SAMe’s reputation and take this nutraceutical, lauded amongst researchers and clinicians internationally for its excellent safety profile exactly in that scenario, in combination with antidepressants and other psych meds, out of the naughty corner – where it was mistakenly put in the first place! [No one puts SAMe in the corner 😂]
But I’m in no doubt many of you will take some convincing and while I am armed and dangerous ready with the answers, some will want to hear it from more than just me (and I 🙌 you ) Easy then – just read the research – take these for starters this one, that one, oh and this one – but there’s plenty more! Once you have, you’ll likely be scratching your head and asking yourself as I did, ‘How did we come to be so misinformed and come to a place where SAMe is so misunderstood?!’
I can answer that too 😉 And then for good measure I hope your brain pings you straight back to that warning on the SAMe label to follow up with – and what is the actual correct meaning and take-home of that label warning then?!🤔
In the previous Update in Under 30 episode we established where are lot of the misunderstanding originates with SAMe, in particular from lab based research that has little-no relevance on the effects of taking SAMe as a supplement, given what we understand now about its bioavailability and pharmacokinetics. While this helped us contextualise such ideas and get some serious perspective on the camp that exudes mild-moderate SAMe hysteria (arms flailing like the robot from Lost in Space, ‘Danger Will Robinson!”), supplemental SAMe is not right nor safe for all. And that is indeed something we need to sharpen our tools and our skills in recognising, monitoring and managing. Just a little somethin’ for your Christmas stocking & all those lazy hours on the beach you’re banking on over the break 😉
You’re welcome🤶
The Big SAMe Rethink Part 2
In part 1 we established where a lot of the misunderstanding originates with SAMe, in particular from lab-based research that has little-no relevance regarding the effects of taking SAMe as a supplement, given what we now understand about its behaviour in the body. In this instalment we go on to examine the evidence that led to the mistaken belief that SAMe was not safe in combination with pharmaceutical antidepressants and explore what the real safety concerns are with respect to its use in mental health patients. This audio comes with a great resource that helps you to both prescribe and supervise the taking of SAMe in your depressed patients, minimising risk and optimising outcomes.
Recently a very experienced practitioner who uses SAMe frequently and successfully in her patients and also delivers education said to me, “I don’t know what I am doing wrong – practitioners still come back to me with cases where they’re throwing 8 different products at a patient to ‘lower histamine, improve mental health and support methylation’ instead of using just one – SAMe!” I laughed and said, whatever you’re doing WRONG in trying to teach people about SAMe I am doing WRONGER and for LONGER!! I’ve been trying to encourage and inspire confidence in prescribing SAMe for 2 decades now and still some of my most loyal listeners, are like, ‘I still haven’t prescribed it, I am too scared.’ 🤯
But I think the fear factor around SAMe occurs for several reasons: Misinformation – there is a LOT of misinformation about HOW SAMe works and WHAT kind of power it wields therapeutically Misunderstanding – this comes from a couple of key misunderstandings about drug interactions and SAMe pharmacokinetics & pharmacodynamics Mystery – even for me, SAMe has had an air of mystery about it, nagging, seemingly unanswerable questions that can undermine our confidence and certainty about its appropriate use and safety
I get it. And given the studies employing SAMe as a therapeutic agent date all the way back to the 1970s and continue to today – in psychiatry, hepatobiliary disease, cancer etc – there is a LOT of information that has been gathered overall and a LOT of old ideas/theories/speculation replaced by understanding thanks to better methods and models of scientific enquiry. So I decided it was time for me to confront this ‘man/molecule/medicine of mystery’ head on, conduct a completely updated literature review of SAMe and along the way – challenge many of my long held beliefs.
I thought about calling this latest episode, ’30 Things You Don’t Know About SAMe’ – and calling it like a horse race because in all honesty I learned THAT MUCH!
But I settled for: The Big SAMe Rethink – inspired by one of many pivotal papers which helped to revolutionise my understanding & approach to this nutraceutical which you can read yourself here. Misinformation, misunderstandings and mystery be gone (ok well most of it anyway!) – by filling in the gaps in our information that previously fuelled these – we can move forward with much greater confidence and clarity and we now know where the real safety concerns exist.
The Big SAMe Rethink Part1 Do you feel like you need to pick a SAMe side? Researchers and clinicians, alike, seem divided in their opinion about its therapeutic capacity and certainly its safety. One side are the ‘naysayers’: ‘SAMe can’t possibly be effective for both depression and in hepatobiliary conditions and and and’. Keeping them company are the ‘doomsayers’, preaching danger and destruction should we prescribe this ‘universal methyl donor’. But the other camp can seem just as fanatical and far-fetched at times: ‘it’s good for just about everything with zero safety concerns’. The divide and differences come down to origins of evidence and, once again, the truth lay somewhere in the middle. This new information on SAMe’s behaviour as a supplement will prompt you to rethink so much of what you thought you knew, whatever side you’re on!
I’ve been ruffling feathers over here while speaking at AIMA in Auckland. While I am pretty familiar and comfortable with that role (& responsibility?) – this topic ruffled my own, arguably the most. In fact, I kicked off the presentation with, ‘What I’m going to say might make some of you uncomfortable but you know what, it makes me uncomfortable and if it makes you think a little less of me, well, to be honest, contemplating these issues has already made me think less of me!”
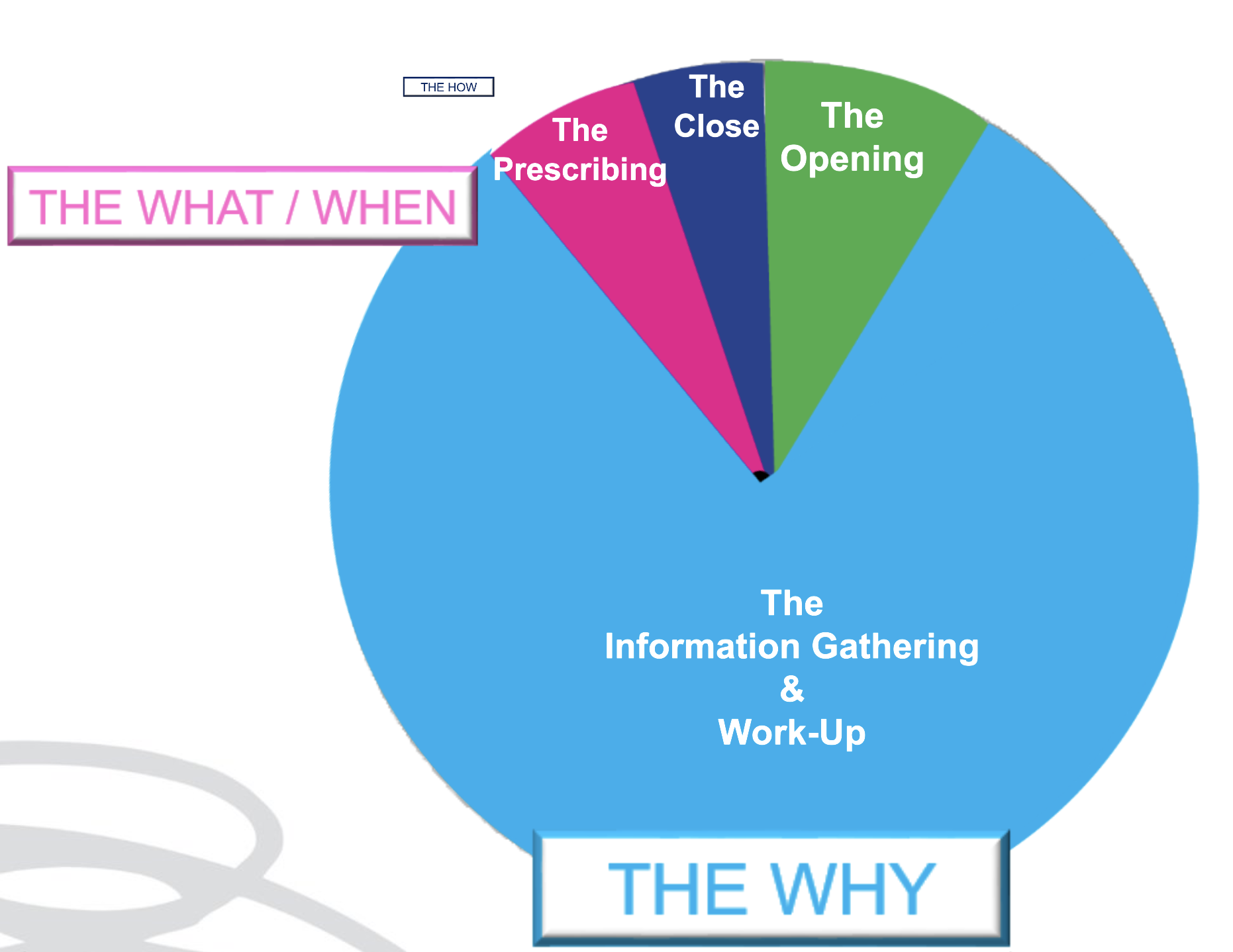
As an educator in integrative health, I have overwhelmingly been a peddler of knowledge and skills under the headings of: ‘WHY’ and‘WHAT’
Why – as in why does this patient present in this way, at this time. I am passionate about upskilling practitioners re our powerful contribution to the diagnostics & work-up of each individual. What – as in what changes (supps, herbs, diet etc) need to happen to correct for these very unique elements of imbalance in this patient to therefore aid resolution. We might label this, ‘personalised medicine’. But after so long in practice it’s patent that the best results don’t come from being the cleverest clinician nor the biggest biochemical brainiac. Knowing the ‘why’ and even the ‘what’, while enough for a minority of patients, fall short for the rest and can still fail to be truly about, & exclusively with, the most important person, in mind.
We’ve learned this before but it needs to be said again and again and again: much of any medicine is via the therapeutic relationship – and as part of this, our ability to PLACE the patient at the centre of their own SOLUTION. And therein lies the conversation we need to have in detail with them about the ‘HOW’ But how much time in your current consults is afforded to the ‘HOW’?
Being able to effectively negotiate with out patients the ‘HOW’ is an extension of Motivational Interviewing, Behaviour Change Theory & Patient Centred Care. It returns the humanity to our list of recommendations for each patient, pushing back against the autocracy that can tend to slip in with prescription writing. It powerfully reminds us that the prescription is only ever as good as the patient’s engagement & buy-in, and that’s only ever as good as our ability to write a prescription that is accessible & readily transplantable into their existing lives: to co-create with them Patient Centred Prescriptions. Someone in the audience had been my patient in the past – double awks right – because I absolutely know, I didn’t know this well enough back then. Back then when they were unable to do exactly as I had recommended – with their diet, their supps, their sleep, their work-life balance – they had, in turn, apologised for their ‘weakness’, ‘lack of willpower or diligence’ and me, being ever so gracious, accepted those apologies only to repeat the error of my ways and write yet more scripts that set them up to fail. 🤦♀️ I am committed to getting better at this and in this endeavour, giving both more attention & time in my appointments to the ‘HOW’ & yes I think we need to think creatively about how we use our appt time and between session touch points to achieve this – keen to hear about your perspective and experiences.
At the end of an information & insight heavy appointment, formulating a list of products and doses for our patients to take can feel like a bit of a ‘tada moment’, like a magician pulling a rabbit out of the hat. “Here is the solution – now off you go!” Research tells us, however, that treatment-plans that are a co-creation between you and your patient – evolving from a discussion that not only allows them a voice, but a major role in the decision making – are far more likely to succeed. While we are the authority on our medicines, our patients are the authority on what makes them tick & what’s likely to succeed, in terms of taste, texture, temperature & timing! This is called Patient Centred Prescribing and together with some other tips tricks and hacks I share with you in this episode, can really increase patient buy-in, compliance and therefore bring your treatment plan to fruition and fulfilment!
How much? How often? When is the best time & timing? do you know about friends, foes and frenemies? Which form, when? e.g. building blocks or bioactives? And for how long? aka are we there yet…?
These are the kind of questions that one would imagine nutritional prescribers can always answer – but can you? Yet this is the goal, right? So that with each and every unique individual who needs supplements – we have a clear, consistent go-to framework to guide & direct these prescriptions. One that makes scientific sense, offers optimal outcomes and removes the uncertainty.
From my interactions with thousands of practitioners, however, I know many of these key questions plague practitioners & they feel, at times, as if they’re flying without a net, or without a strong systematic approach, or at the very least without all the answers to these questions.
I’ve had so much good fortune & so many others to thank for providing me with this foundation. Fay Paxton – my nutrition lecturer in my under-grad who indoctrinated me with a systematic approach. Dr. Tini Gruner – my principal supervisor at SCU, who shared & further fuelled my passion for biochemistry and reading labs to extract insights into each individual. And thanks also to all the pharmacists I’ve delivered education to over the years, who, as a result of their grounding in the principles of pharmacokinetics, always ask the best questions – questions that if I don’t know the answer I know I need to know the answer! So I made it my mission to find out!
While we dip into these aspects of nutritional prescribing in our regular mentoring groups on an ‘as needs’ basis, I’ve decided the time has come to create a year-long program dedicated to sharing this information and building this skill-set in practitioners.
This monthly meet-up is delivered live (max 1.5hr) and runs from Feb to November with the following currently proposed format *subject to change dependent upon the needs of the group
Feb Factors Affecting: digestion, absorption (host, form, dose)
March What happens to what gets left behind? e.g. enhanced enterocyte micronutrient concentrations & their effects plus unabsorbed nutrients & their interactions with the colonic environment
April What happens to what’s absorbed e.g. distribution, hierarchy of needs, activation and deactivation
May The pharmacokinetics of prescribing
June Where do our ideas on dosing come from? e.g. Physiological Vs Pharmacological dosing & actions. The basis & believability of maximal intake boundaries?
July Bioefficacy V Bioequivalence. Beyond building block nutrients: Is ‘Bio’ (-active, -peptides, -materials) always better? e.g. GABA Vs Glycine, NAC Vs GSH, PLP Vs Pyridoxine, Niacin Vs Niacinamide riboside ——————————————————————Aug month off—————————————————————————
Sept How often & for how long? Are we there yet? And how would we know? Plus Fast Vs Slow Nutritional therapeutics
Oct Strategies for Supplement Success e.g. friends, foes and frenemies in nutrition underpinning principles with examples; compliance changers for clients
Nov Live attendance & opportunity to participate in a case-based mentoring session
This monthly ‘live’ meet up will be delivered as part of 2023 Group Mentoring as The Nutritional Prescribing Program Group Mentoring applications open 17 October 2022.
To join the waiting list and be notified when applications are open, email the team at [email protected]
Find out more about what groups are available for Group Mentoring in 2023 here.
One of my dear friends told her husband several years ago that she had noticed he was now making, ‘old man noises’ upon standing up from couches & chairs. She told him that must simply stop. She pointed out that he was only 50 and that she neither could nor would listen to that for another 40 years!
He stopped!
But aging and old (wo)man noises are coming for all of us, right? And by the time we’re making those noises or excusing ourselves from certain activities due to sore, dodgy or NQR [insert joint or body part], we’ve spent several decades unknowingly right on course to get here! We don’t generally pay any attention to our ECM (extracellular matrix) which suffers in silence, slowly but surely losing its structural & functional integrity from the age of 18 on, until we reach the tipping point: joint degeneration, repetitive soft tissue injuries etc, and a problem that will never be silent again! Cue your choice of anti-inflammatories it seems – til death do us part!
The Ageing Matrix is a thing.
And no I haven’t seen the movie – I don’t need to – I’m living it.
When I was pregnant I thought I wanted to specialise in pre-conception & pregnancy care. Then my babies arrived and I took a fancy to paediatrics. Sound familiar to anyone? Now, unsurprisingly, I have a real thirst for knowledge expressly aimed at bettering this whole ageing-thing! So in preparation for this Update in Under 30 episode, I’ve relished the opportunity to put the Ponds Institute & all similar cosmetic companies on notice! Scrutinising their claims that every woman on the planet would do better with more Collagen, more Elastin, more Hyaluronic Acid, just more of every key ECM component really. Ok, but in accordance with my bias and my business, my lit review pertained to oral supplements, not outrageously priced magical middle-life-crisis rubs and the therapeutic action I had in mind was the integrity of our ECM, and the roughly 2kg of collagen, we rely on, for functions a lot less frivolous than stopping sag. I have to say, I started out as non-believer but the research was quite the awakening…still there’s a lot to unpack here in order to repack our ECM and prevent against the erosion of its integrity and everything we build, and rely on, upon it – to live well!
Osteoarthritis (OA), like osteoporosis, is a diagnosis made after decades of disease. Underpinning it all, is our aging Extracellular Matrix (ECM) with its characteristic compositional change that leaves us vulnerable, from the ripe old age of 18! The ECM, like all other tissues, is made from basic building block nutrients but presented in their most fanciest of forms with triple helix structures, aggregates and other large molecular weight components, that each possess remarkable physico-chemical properties & convey extraordinary functionality to structures like joints. But is prevention against, and effective intervention for, OA as easy as consuming more of these ECM biomaterials?
You can purchase Supplementing Collagen & ECM Biomaterials – What’s the story?here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
Any pathology test is only of value if the result produced is ‘real’, or, representative of that individual, right? So the timing of the test is a major pivot point then: do I tell my patient to present for the test, or collect the sample themselves, on their ‘best’, their ‘worst’ or their ‘average’ day? 🤷♀️ Well, that all depends on the question you are trying to answer.
Whenever we reach or refer for a test, we have a question in mind we’re seeking an answer to. But the question always comes in two parts, at least.
Part 1: How much progesterone is she making? Part 2: …When she’s ovulated & her corpus luteum should be most productive?
A third might refine the question you’re answering further by adding another contextual clarification
Part 3,4,5: …When she’s eating her regular diet, not exercising excessively or under extreme stress
Without these other parts – the answer to the first one: How much progesterone is she making (full stop), is hard to correctly interpret, right? By refining and expanding on the full extent of our question, we can be clear about which elements of this patient’s life the result likely reflects. We might say that for her, this time-point, or set of collection conditions, is a ‘real reflection’ of her generally and therefore, representative. But what if she does occasionally undertake a 5 day fast, or train for & compete in marathons? If we were to specifically test during these times, we answer a different question, right? Likewise every time we instruct a patient to present for their blood tests (routine or fancy schmancy): Fasted, Rested, Hydrated and off their supplements – is this sound advice or a misdirection? Well it depends on the individual in front of you and the real question you want answered about them 🤓
Ahhhhh I love rules: both the making of them and the subsequent breaking of them 🦜🏴☠️
The collection conditions for any pathology test – can refine or ruin the question you were hoping to have answered about your patient but is it always appropriate to ask everyone to ensure their preparation for the test was ‘ideal’? What if their real life is far from ‘ideal’ and contrasts dramatically with these ‘conditions’ e.g. they forget to drink water but never alcohol! Or do they run 20km every weekday and 40 on weekends? And why would we tell some patients to stop their supplements prior to a blood-test and not others? If our goal is to ensure any pathology test answers the question we need answered we need to know how to respond to these and other scenarios. This new update is all about keeping results ‘real’ & representative.
You can purchase Fasted, Rested, Hydrated & Unsupplemented? Exceptions to the Rulehere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
Are we doing ourselves out of a job? I’ve been talking treatment plans with my New Grads recently. Given, only recently these were major assessment items in their clinic units, they have been trained to create ALL-ENCOMPASSING (biopsychosocial) prescriptions and recommendations of utterly EPIC PROPORTIONS – to simply prove they know it all. Problem is this doesn’t work in the real world.
Emailing your client multiple pages of advice that covers: a whole sizeable supplement schedule that only a military-training could nail (2 tablets 1 XTID 1 X BID, a liquid, a powder, some with food, some definitely not with food) plus dietary advice, plus hyperlinks to exercise advice, mindfulness exercises and a request for follow up investigations before the next appointment…is…a L*O*T!!
It is also ineffectual – because it completely disregards the human on the other end. Let me ask you this, how much change are you capable of between a first and second appointment, roughly a period of 2-3 weeks? Personally, I gotta say not that much. It took my dentist years to get me just embrace flossing & I don’t think I am an exception! With all the knowledge we possess its hard not to see people as (a long list of) problems (& problematic behaviours) that we translate into, and solve via, a prescription.
Effectively we are saying to patients with this practice model, ‘Go change & come back when you’re done & then I’ll probably ask you to change some more!’ That’s both a big ask and a huge missed opportunity.
I hear from reliable sources over the ditch, that GPs are increasingly referring their patients to, or teaming up with health coaches, rather than naturopaths. Given what I’m observing, I get it. Doctors on the whole only have time (and barely then) for a finger-pointing prescription – certainly not the time and touch-points required to actually support patients with the very difficult thing that is, behaviour change. Nor the skills to truly facilitate patients making the necessary and desired changes – so they outsource this role. But we shouldn’t.
After all – I want to be on my patients’ support bench & health care team always – not a flash in the pan, that blinded them with science or my ‘smarts’ and proved to them in one over-stretching prescription – that naturopathy is not for them, or at least, they’re not fit for the task.
At the end of an information & insight heavy appointment, formulating a list of products and doses for our patients to take can feel like a bit of a ‘tada moment’, like a magician pulling a rabbit out of the hat. “Here is the solution – now off you go!” Research tells us, however, that treatment-plans that are a co-creation between you and your patient – evolving from a discussion that not only allows them a voice, but a major role in the decision making – are far more likely to succeed. While we are the authority on our medicines, our patients are the authority on what makes them tick & what’s likely to succeed, in terms of taste, texture, temperature & timing! This is called Patient Centred Prescribing and together with some other tips tricks and hacks I share with you in this episode, can really increase patient buy-in, compliance and therefore bring your treatment plan to fruition and fulfilment!
Have you ever noticed that our products don’t work if our patients don’t take them?!🙄
The reasons for non-compliance, dis- or non-engagement, poor patient buy-in & follow through are many:
*My dog ate the instructions * My inbox swallowed the instructions *As soon as I left your clinic, your instructions left my brain
Reasons also include far more credible things such as non-patient centred prescribing. This is what most of us do when we’re full of good intentions but short on time at the end of a consult, so we just throw a bunch of products and a script with them out the door. Arguably many of us make this mistake also because our training perpetuated this relic of conventional medicine and paid insufficient attention to the therapeutic relationship. In contrast, patient centred prescribing recognises the patient as best-placed to find personalised solutions to their very individual challenges, including, decision making around dosing regimes. So while we continue to ensure & oversee that therapeutic doses are used and that best conditions for taking certain things are adhered to – your patient remains the expert in the room about how to actually achieve this – both in terms of when & where in their very real lives – with a little help from us – and what ‘works for them’, in terms of taste, texture & temperature.
That’s right, I said temperature…are you telling patients to take everything at room temperature??
You need to think again – this is something we can safely manipulate with many powdered & liquid remedies (some exceptions of course!) to match patient preferences & radically increase palatability, pleasure and ultimately patient compliance.
Are you like me? I have supplements scattered all over my house – in places that correlate with an action or moment in the day when I am most likely to take them. This is another important element of Patient Centred prescribing, so I work with my patients to identify these easy solutions too. After the gym? In the gym bag. After breakfast as you leave for work? In the key bowl. At work? On the desk beside the computer screen. Keeping taurine in the drinks cupboard in front of the alcohol is another nifty reminder and trick for those looking to ‘pre-load’ and cut down! Tips and tricks like these save our over-loaded memory. They remove or minimise barriers. They make compliance less effortful. And as a result, you know what? They might just get the results we would have expected!
Compliance Changers – Strategies for Success
At the end of an information & insight heavy appointment, formulating a list of products and doses for our patients to take can feel like a bit of a ‘tada moment’, like a magician pulling a rabbit out of the hat. “Here is the solution – now off you go!” Research tells us, however, that treatment-plans that are a co-creation between you and your patient – evolving from a discussion that not only allows them a voice, but a major role in the decision making – are far more likely to succeed. While we are the authority on our medicines, our patients are the authority on what makes them tick & what’s likely to succeed, in terms of taste, texture, temperature & timing! This is called Patient Centred Prescribing and together with some other tips tricks and hacks I share with you in this episode, can really increase patient buy-in, compliance and therefore bring your treatment plan to fruition and fulfilment!
You can purchase Compliance Changers – Strategies for Successhere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
And health, no matter which side you sit on, seems to be particularly plagued by them. I (incorrectly) recall my 4 year degree as being a series of deep personal losses, some favourite food, then caffeine, then alcohol etc etc.😂 Likewise, I’m aware that naturopathy & integrative health’s ‘voice’ in the ‘conversation’, could arguably be perceived as mostly a negative one – as in, ‘No. Never. Not good. No, not even a little bit?!’ But I love both playing devil’s advocate & reading the research (ALL the research – even the stuff that doesn’t support my views and position GASP!~) so I am less in favour of absolutisms. This came up recently when I suggested alcohol may improve iron uptake 😬
Practitioners’ responses were 1 of 2 types: humorous dismissal (“steak & beer for breakfast – at last a naturopathic prescription I can support!”) or horror. But why are we so attached to the absolutes in spite of contradictory evidence?
Let me ask you this: is coffee bad? Full stop? Period? The end? Or is it the most concentrated source of antioxidants consumed in the average Western diet? Does it improve bile flow, peristalsis and at higher levels actually protect the liver against damage? Clearly, we need to read all the evidence, including, the favourable and make individual decisions about ‘what serves and what sabotages’, for each patient. But do we? Or do we imagine we only get membership to the ‘Ultimate Integrative Health-club’ when we adhere to blanket bans?
Similarly I, like many of you, see a LOT of iron deficient women – & a fair chunk of these have been incorrectly labelled, ‘refractory’ because theconventional correction strategies (high doses everyday) don’t actually make sense. But like you guys too, I’m always on the hunt for new ways to improve iron absorption in these women, so I can hit them & their gut with less. That’s why I shared the research regarding alternate day dosing, and taking a supplement within an hour of exercise and now, I dare to ask if a tipple could be helpful?
While we know that both ‘GOOD’ (exercise) & ‘BAD’ (alcohol) health behaviours increase gut permeability, which sounds ‘BAD’, right?
But could this be ‘GOOD’ for some?
This has certainly been demonstrated in relation to exercise & iron but most of the research investigating how alcohol intake effects iron uptake and status is based on alcohol abuse. The study below, however, based on a large sample of non, mild, moderate & heavy drinkers captured in NHANES data – is a very well written and reasoned article, such that it can exclude liver damage, inflammation and HFE mutations as other explanations for the better iron status, in drinkers. And it found:
I challenge you to read it for yourself and challenge your absolutes!🤓
Oh and just in case you’re thinking, “Have we all misdiagnosed iron deficiency and it’s actually a Copper deficiency underneath?”because last year the fashion was everyone was copper toxic and now this year someone’s making noise saying everyone is copper deficient !!! (Absolute? Anyone?!) Ah, no. Copper deficiency, as a cause of iron deficiency and anaemia, has been around for about as long as nutritional medicine itself. It is absolutely a thing. But in the absolute minority of people. And if you go back to some basic maths & compare and contrast Fe & Cu at each level: 1) requirements almost 20mg Vs < 2mg 2) average intake (inadequate Vs adequate) 3) bioavailability (Fe < 20% more typically < 10% in a modern low meat diet Vs Cu is typically >50% ) and do some basic sums I call, ‘Menstrual Maths’ – You’ll likely deduce that inadequate iron intake and uptake, given our losses, is in fact the common culprit and a ‘coldie’ may be more beneficial than copper in most! Can y’all stop asking me about that now – pretty please?
And then you don’t. The reality is we all struggle at times with correcting low ferritin or iron deficiency anaemia – so what have we got wrong? In spite of being the most common nutritional deficiency worldwide, the traditional treatment approaches to supplementation have been rudimentary, falling under the hit hard and heavy model e.g. 70mg TIDS, and are relatively unconvincing in terms of success. New research into iron homeostasis has revealed why these prescriptions are all wrong and what even us low-dosers need to do, to get it more right, more often!
Did you know you can subscribe to these? We deliver at the end of each month, just add a 12-month subscription to your cart and Rachel’s latest research is on it’s way to you!
“My 7yo daughter was frequently distressed, telling me she had that ‘throat feeling’.”
As you can imagine, mum offered up a smorgasbord of suggestions to help her try and describe it: Can you swallow ok? Does it burn or taste funny? Where is it? Is it hard, soft, moving, give me a rating out of ten….so many, but she just couldn’t. When it was really bad, her daughter said she also felt it in her sternum. The first doctor attributed it to ‘stress’ & mum understood why. Her 7yo is a bit of a worrier and while the ‘throat feeling’ was distressing, stress, itself, seemed to also perhaps bring this on. But by the time they made an appointment with their regular family GP, mum had noticed her daughter’s sx were worse with heavy, fatty, high meat meals & that she was burping excessively especially with the night time meal also. So, when their switched-on doctor heard these very careful observations, he referred her for a urea breath test (UBT) for H.pylori.
‘Miss 7’ blew 1200 on the UBT the decision limit is 200, to confirm the presence of the bacteria in significant amounts
As I’ve said previously, there are (sadly for ‘Miss 7’ & myself) no prizes for the highest score on this particular test. In fact, I spoke with a gastroenterologist last week who said, really it remains so debateable about the significance of the overall result (?size or virulence of colony) that results should probably be more considered like a pregnancy test: a simple yes or no! But this together with her sx was a clear yes. GP recommended triple antibiotic therapy which sadly produced vomiting in Ms 7 within a few days. GP contacted paediatric gastroenterologists to get some advice, which was: don’t treat unless symptomatic. Back to square 1.
“In the meantime, I had done Rachel’s two UU30 episodes on H.pylori, so I told him what ‘we’ would do (polyphenols plus cranberry juice plus Zn carnosine plus deal with the hypochlorhydria). GP says. “Ok, then let’s do it and then let’s breath test again in 3-6 months.
She has now breath tested at 200 and symptoms are non existent!”
Mum contacts me to relay the success story & give me the credit but mum is completely minimising her extraordinary actions that produced this outcome. Firstly, not resting with the ‘stress’ diagnosis. I have seen several children who present in very similar ways to Miss 7, YES! they are anxious, YES! parents might tell you they are the ‘worrying-type’ but when combined with these upper GIT sx I have found they test positive for H pylori more often than they don’t. And how clever is this mother’s medicine?
“I recognised it was worst after birthday parties where she has eaten too much and done cartwheels or run around (we now talk about recognising when she has a ‘full bucket’. We talk about the fact that her tummy takes a little bit more time to process food it means her bucket fills and she needs a bit of extra time to let it do it’s job before she adds more food to the bucket otherwise it spills over and she feels rubbish. She finds that analogy useful as she can feel her bucket getting full at birthday parties and when she gets the feeling, she knows why and doesn’t freak out.”
H.pylori – Eradicate or Rehabilitate? For a bacteria identified just a few decades ago as being a cause of chronic gastritis, atrophic gastritis and gastric carcinoma, the escalation in the number of antibiotics used to eradicate it (4 at last count + PPI) has been nothing short of breath-taking. A management approach more consistent with both integrative medicine and with an improved understanding of the delicate microbiome focuses on changing the gastric environment to ‘remove the welcome mat’. What do we know about how to do this successfully? It turns out…quite a lot.
An ideal T4 is 15
An ‘anti-aging’ DHEAs must be >7
A ferritin of 100 is optimal for women…
I’ve heard it all, probably you have too, and far too often & too recently from practitioners who should have rationalised & researched their way beyond these functional falsehoods, by now. I bought into these ‘optimal wellness truths’ hook line & sinker early in my career and proceeded to even propagate a few but with (not much) more experience in clinic, I had to seriously question this pursuit of ‘perfection’ & ‘perfect pathology’…in favour of reality & scientific evidence! They didn’t add up. Not with my patients – even the healthiest ones, in fact some of the really unwell ones occasionally had these kind of high-normal results and they were part of the problem!. ‘But that’s because no one is truly healthy outside of those seeing a functional medicine practitioner & supercharged on supplements & hormone replacements!!’ came the counter-argument. Ahhh, really?
How then do we reconcile this with the following: Individual genetics & biochemistry
Our biological resilience Healthy & appropriate senescence Large datasets of mixed race populations from other comparable first world countries…where these figures denote the statistical outliers?
I mean, if the 50th centile value for ferritin for actual living, breathing, bleeding, women in the US, Canada, Australia etc etc is 30-40 ng/mL and the 95th centile is 126 ng/mL and the WHO says that in fact, anyone menstruating with a ferritin > 150 ng/mL should attract suspicion for iron overload….but functional medicine men (mostly…sorry but it has to be said!) say 100 IS OPTIMAL FOR EVERY WOMAN #@^*…please tell me in which women, consuming what kind of diet, where in the world, & based on what improved or better health outcomes?
And while you’re there can someone please support this bold claim with a scrap of high quality evidence?? [Rant over🎤💧]
The falsehoods of functional medicine include the blanket belief, ‘more is better’ (ahhhhh not when it comes to many things, including iron where women’s lower levels have been found to be an evolutionary advantage…guys). But you know what, we’re better than that! We see each individual, recognising all the factors at play that make for their uniqueness, help to define what ‘healthy’ looks like for each person and don’t fall for one-size-fits-all claims without any evidence nor common sense even, to support them. What do you think?
Let’s make sense of the over-arching nutrition principles, that will profoundly change your understanding and application of this modality Truly understanding the ‘big’ concepts, so often overlooked, or incorrectly taught, ensures you get the critical ‘small’ detail in your nutritional prescriptions right. In this 4 hour recording, together with key clinical tools, we talk about the tough stuff: dose-response curves, active versus passive stores and excretory pathways and ooh lah lah…the myth of taking ‘activated vitamins’. Even those who feel satisfied with their original training – will find a lot in this critical review that is new, insightful and truly practise-changing!



 You can purchase
You can purchase 
 You can purchase
You can purchase 


 You know the saying, ‘If I had a dollar…’, well there’s so many ways I could finish that sentence, especially in relation to the most common questions I’m asked by praccies on a weekly basis and ‘Can my patient on antidepressant ‘X’ take SAMe?’, would be in the top 10! While many of you might be mouths agape reading this, I bet the cause of that comical expression is not the same for everyone. Yes, like you, they’ve read the mandatory label warning: ‘individuals who are using prescription antidepressants or suffer from bipolar depression should not use this product unless under the supervision of a healthcare practitioner’ – but let me ask you, how do you interpret that? Turns out there are several interpretations and the most common is the most incorrect.
You know the saying, ‘If I had a dollar…’, well there’s so many ways I could finish that sentence, especially in relation to the most common questions I’m asked by praccies on a weekly basis and ‘Can my patient on antidepressant ‘X’ take SAMe?’, would be in the top 10! While many of you might be mouths agape reading this, I bet the cause of that comical expression is not the same for everyone. Yes, like you, they’ve read the mandatory label warning: ‘individuals who are using prescription antidepressants or suffer from bipolar depression should not use this product unless under the supervision of a healthcare practitioner’ – but let me ask you, how do you interpret that? Turns out there are several interpretations and the most common is the most incorrect.