Do you realise we’re often giving our patients Crabs? Stay with me 🙄 We’re all BIG fans of polyphenols right, but did you know that one of the key ways they qualify as antioxidants is that they chelate metals?
Chemically speaking that means that polyphenols (flavonoids, isoflavones, tannins, stilbenes etc) have a structure that looks and works like two ‘crab claws’ 🦀 the ends of each claw attracting and binding metal ions, following which, the claws kind of ‘close’ around the metals and trap them within. 🦀
Now sometimes the closing of those claws results in a clear ‘stop & block’ effect – the metal will remain trapped and be lost from the gut or other parts of the body along with the polyphenol but not always…other polyphenols can be favourable chelators just temporarily binding a metal but ultimately making it bioacccessible to us and increasing its bioavailability & bioefficacy. So polyphenol prescriptions, aka ‘crab medicine’, need to be precise. Every different class of chelator or ‘binder’ e.g. MCP, zeolites etc will have different metal affinities. Our beloved polyphenols have a predilection for one metal above all…and that happens to be iron!
As clinicians, we can harness their polyphenol power to either enhance iron uptake or block it.
🦀 Both actions, of course, well indicated in different patients & presentations 🦀
In the latest Update in Under 30 we write a polyphenol program for those individuals ‘on the road to iron overload’, who simply ‘can’t close the door to more’! Knowing how to perfect this prescription and still allow for personalisation & preferences etc is the key to sustainable essential everyday iron mitigation between blood removals and to minimise the need for these. And if your bigger challenge is the issue of iron deficient patients who are refractory to your well-reasoned remedies then take a listen and a look at the accompanying resource and ensure they are doing the exact opposite! I am being completely serious. I don’t think many people realise the power of the polyphenols & how pervasive they are in our herbal & dietary recommendations 🤓😲🤯
For those individuals with HFE mutations on the road to iron overload, whether they ultimately reach that destination of absolute hyperferritinaemia or not, excess iron mitigation ‘every day & in every way’ is key to better outcomes. While avoidance of dietary haem iron and, where indicated, therapeutic phlebotomy, are cornerstone treatments, patients are increasingly being offered add-ons such as PPIs and pharmaceutical chelators. However our polyphenol prescriptions (both food form and nutritional & herbal supplements) offer additional novel actions to address excess iron mitigation, while also providing patients with improved cardiovascular protection, immune system support etc. This recording comes with an incredible resource for both you and your patients. Packed with evidence-based options they can choose from at each meal & across the day, it offers them their own tailored treatment plan by identifying options as (un) favourable, & therapeutic in each category of food, beverage, even cooking methods.
You can purchaseThe Power of Polyphenols In Iron Excesshere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
Still. And yes – like you – I don’t see any slowing down any time soon in this extraordinary paradigm shift occurring in medicine and health. Which for us humans involves one humbling discovery after another.
Here we were thinking we made our dietary choices from a place of free will & individual preferences 🤣🦠
Thinking those microscopic mates, were making those B vitamins, and SCFAs and and and…for us & our benefit 🤣🤣🦠🦠
And while there’s a lotta love going on between our microbes and our micronutrients – in both directions – Pat Benatar said it best, “Love is a battlefield”
(sorry but I feel compelled to insert a link here for the youngsters – you’re welcome 😉)
The tussle over who gets to access those nutrients that are actually essential to both of us (the hostage and the microbiota) is an absolute turf war, peeps, and this battleground has seen some bloodshed! The new new question being raised is how the prescribing of nutrients, especially at the higher doses we tend to use, trickles down to influence and impact those microorganisms who reside in the bowel. Directly – as a selection pressure we have, likely unintentionally unknowingly, introduced. Which species do well when exposed to levels of a vitamin or a macro or trace mineral that are simply unobtainable in the diet? Yes – research answering these questions has begun in earnest revealing some positive ‘prebiotic-like actions’ of some but not of course for all nor in all scenarios. Want to learn more about this latest aspect we need to consider when formulating our nutrition prescriptions? You can either jump in and join us in the Nutrient Prescribers Program which kicks off next week to get across absolutely everything new in nutritional medicine or just dip your toe in here with our latest Update In Under 30: The Micronutrient Microbiota Universe
The world of health science went microbiota-mad a few turns back and there’s no sign of an end. Research continues to reveal the breadth of the GIT microbiota’s positive & negative reach, in particular, & with discovery upon discovery we’ve come to understand how often the microbiota are ‘managing us’. Both in terms of being integral to the success of our digestive, immunological, metabolic etc processes but also in a self-serving way, for example, directing our dietary preferences to satisfy their own needs. This has understandably prompted the question about the impact micronutrient supplementation is unintentionally having as a selection pressure on our gut microbes. Which bugs like which B vitamins when taken in excess of the amounts achievable in the diet? And which microbes flourish and which falter when we radically change their mineral exposure?
You can purchase The Micronutrient Microbiota Universehere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
I’m such a sucker for marketing!…ZoomZoom is from an old Australian car ad – an earworm clearly conveying ‘ the speed of something’, and let me tell you, totally fitting for this little Zinc tale I’m about to tell! Many years ago, I wrote a thesis on Zinc that necessitated me reading every research paper ever written (that’s how it felt anyway!🤪) on this trace mineral. Like everything in nutritional medicine, especially in the area of our burgeoning understanding of micronutrients, this is a highly dynamic space, so regular reviews of what’s new is essential and, since my thesis, part of my regular practice. Well, I just did my latest deep dive, and HELLOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO radical paradigm shift(s)…yep plural!
Zinc supplements should ideally be: Organic amino acid chelates Taken daily – due to the lack of Zinc stores in the body Taken fasting Taken in doses in excess of the RDI to compensate for the smaller % absorbed
Yep – nope. Or in true-blue Aussie: Yeah, nah. Can’t believe what you’re reading right now? Neither could I when I undertook this recent review but the studies are increasingly sophisticated and the resultant paradigm shifts are being echoed, reiterated & reinforced. And these have, in turn, challenged all those old ‘norms’ about how best to administer zinc for those patients with a shortfall. If you’d like to take this little journey for yourself…I suggest you start here! I immediately changed how I take it myself and now my mission is to both spread the word and get us all reflecting and reviewing our prescribing principles around Zinc…and tbh, around all micronutrients! After spending my ‘summer’ doing sufficient reading for a second thesis on everything new in micronutrients…I am armed and dangerously prepared for our upcoming *NEW* program: The Nutrient Prescriber’s Program which kicks off in late Feb for 5 months.
I truly believe that based on all this new information, we can now get so much more out of our medicines.
Nutrition represents such an extraordinary set of tools for us to work with, but it’s time to sharpen those tools in terms of how we apply them!
The Changing Zeitgeist Of Zinc Prescribing
Zinc research is a highly dynamic field and given its relative recency of discovery as being essential to humans, we’re still in the early days of truly getting to know this mineral. In just the last few years, enormous gaps have been filled-in regarding its regulation and roles that look to radically change our prescribing practices. Tune in to this essential update for some serious food for thought about doses and dosing frequency.
You can purchase The Changing Zeitgeist Of Zinc Prescribinghere. If you are an Update in Under 30 Subscriber, you will find it waiting for you in youronline account.You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audios and resources here.
When it comes to the recognition of Nickel as the number one metal allergen worldwide, affecting up to 30% of adults and with a particular predilection for women, it seems like Australian health professionals really do come from the ‘land down under’, with many of us still somehow yet to read that memo.
How much? How often? When is the best time & timing? do you know about friends, foes and frenemies? Which form, when? e.g. building blocks or bioactives? And for how long? aka are we there yet…?
These are the kind of questions that one would imagine nutritional prescribers can always answer – but can you? Yet this is the goal, right? So that with each and every unique individual who needs supplements – we have a clear, consistent go-to framework to guide & direct these prescriptions. One that makes scientific sense, offers optimal outcomes and removes the uncertainty.
From my interactions with thousands of practitioners, however, I know many of these key questions plague practitioners & they feel, at times, as if they’re flying without a net, or without a strong systematic approach, or at the very least without all the answers to these questions.
I’ve had so much good fortune & so many others to thank for providing me with this foundation. Fay Paxton – my nutrition lecturer in my under-grad who indoctrinated me with a systematic approach. Dr. Tini Gruner – my principal supervisor at SCU, who shared & further fuelled my passion for biochemistry and reading labs to extract insights into each individual. And thanks also to all the pharmacists I’ve delivered education to over the years, who, as a result of their grounding in the principles of pharmacokinetics, always ask the best questions – questions that if I don’t know the answer I know I need to know the answer! So I made it my mission to find out!
While we dip into these aspects of nutritional prescribing in our regular mentoring groups on an ‘as needs’ basis, I’ve decided the time has come to create a year-long program dedicated to sharing this information and building this skill-set in practitioners.
This monthly meet-up is delivered live (max 1.5hr) and runs from Feb to November with the following currently proposed format *subject to change dependent upon the needs of the group
Feb Factors Affecting: digestion, absorption (host, form, dose)
March What happens to what gets left behind? e.g. enhanced enterocyte micronutrient concentrations & their effects plus unabsorbed nutrients & their interactions with the colonic environment
April What happens to what’s absorbed e.g. distribution, hierarchy of needs, activation and deactivation
May The pharmacokinetics of prescribing
June Where do our ideas on dosing come from? e.g. Physiological Vs Pharmacological dosing & actions. The basis & believability of maximal intake boundaries?
July Bioefficacy V Bioequivalence. Beyond building block nutrients: Is ‘Bio’ (-active, -peptides, -materials) always better? e.g. GABA Vs Glycine, NAC Vs GSH, PLP Vs Pyridoxine, Niacin Vs Niacinamide riboside ——————————————————————Aug month off—————————————————————————
Sept How often & for how long? Are we there yet? And how would we know? Plus Fast Vs Slow Nutritional therapeutics
Oct Strategies for Supplement Success e.g. friends, foes and frenemies in nutrition underpinning principles with examples; compliance changers for clients
Nov Live attendance & opportunity to participate in a case-based mentoring session
This monthly ‘live’ meet up will be delivered as part of 2023 Group Mentoring as The Nutritional Prescribing Program Group Mentoring applications open 17 October 2022.
To join the waiting list and be notified when applications are open, email the team at [email protected]
Find out more about what groups are available for Group Mentoring in 2023 here.
Have you been told somewhere by someone that the ‘perfect’ TSH is 1.5 mIU/L? This is a wonderful, terrible & wonderfully terrible example of ‘magical numbers medicine’. As a push-back against the published reference ranges we’re given, that are so wide you could drive a truck through them, there has been an over-correction by some, leading to the myth of ‘magic numbers’. We can narrow the reference range substantially for many parameters with good rationale, make no mistake about that but once we start setting ‘aspirational goals’ that are explicitly rigid…well we’ve done 2 things 1) forgotten about the patient to whom this result belongs and 2) disregarded viewing each result as part of a ‘pattern’, that we must piece together and make sense of.
Back to TSH then… if my obese patient had a value of 1.5 mIU/L this in fact would be woefully inadequate – so too a child at any weight.
And we expect a higher value as well in our elderly clients too and this level there may be, in fact, increased mortality.
But the same result would be excessively & worringly high in my patient who’s undergone thyroidectomy.
Realising the full value of any test result in terms of what it reveals about the person sitting in front of you, requires these more thinking and more thoughtfulness. Unfortunately, a list of ‘magic numbers’ will often lead you astray. And building your scientific knowledge about labs will not only help you avoid the pitfalls of pathology but will strengthen your pathophysiology prowess in surprising ways, saving your patients a packet in terms of additional extraneous testing and help you truly personalise your prescriptions…because the ‘invisible (biochemical individuality, oxidative stress, genetic probabilities, subclinical states, imbalanced or burdened processes etc) just became visible’. I started requesting lab results early in my career and years later was lucky enough to be taken under the wing of Dr. Tini Gruner. I found some of our shared notes, from 10 years ago, scribbled all over patient results recently and I was struck by just how lucky I was to have her encouragement to really pursue my interest and how she was a guiding force about learning to recognise pathology patterns over single parameters. A decade on I can concede, much of my clinical and educative success has come off the back of this foundational skill-set and I know, this is true for so many I’ve taught too.
“The guidance I’ve received over the years from Rachel in relation to pathology interpretation has been one of the most valuable (and fascinating) investments I’ve made as a clinician. Her teachings have filled gaps in my knowledge base I never knew needed filling and have significantly enhanced my understanding of the inner workings of the body! Rachel has an incredible ability to make the numbers that patient’s so often present us with, both understandable and clinically meaningful. The knowledge I’ve gained by investing in this skillset has paid off in dividends and I’m certain will continue to do so into the future.”
Stacey Curcio – Cultivating Wellness
I hope you’ll join me for the most exciting up-skilling opportunity in learning labs yet. Oh…and all this talk about thyroid testing..this next MasterCourse series is focused on revolutionising your understanding of thyroid, adrenal, HPT & HPA markers based on the very latest research & findings & marry these together with everything you learned in MasterCourse I (ELFTs, FBE, Lipids & Glucose) to understand the ‘whole story’.
…an absolute treasure trove of free integrative health information about your patient!
DEEP DIVE INTO REAL CASE STUDIES TO DEMONSTRATE EACH PATHOLOGY PATTERN IN ACTION. ]\
There are limited places. To sign up for Rachel’s LIVE Series – MasterCourse II: Thyroid & Adrenal Diagnostics and for more information click here.
I’ve spent the best part of about 4 months recording my *NEW* Advanced Thyroid Assessment training. I told my team this would be easy and quick, given it was to be based on a great little 2-part, 2hr updated presentation I delivered just last year for ACNEM!! Sixteen weeks (like seriously…most of it) numerous rewrites and retakes later, our final product is 4 parts that goes for over 12hrs in total & has a bonus Adrenal recording! And yeah my team are impressed but unimpressed too if you know what I mean?!🙄🤪
Every time another, ‘Oh wow!’, or ‘No way!’, escaped my lips, it was a source of personal celebration, as another deeper layer of learning revealed itself.
But to the wonderful, somewhat weary and definitely wary Sally, who does all my powerpoints, it was met with, ‘Oh boy!’, because it meant many multiple new slides to build full of visual metaphors, animation acrobatics, if not an entire new Part!*#@^
Her sage advice along the infinite research road I’ve been travelling was : ‘Stop. You’re going to have to stop.’
So I didbut now I am this meme. Everything I see currently through the lens of thyroid health, I talk in tongues TFTs and my brain is one giant neural network of integrative endocrinological circuits! I have fallen in love with this topic, this neuroendocrine axis and its ‘first responder’ role all over again! Hence our little thyroid character below – all ‘antennaed’ up – is one of the many tools we’ve developed for this training, to teach us that ‘bad thyroids’ per se are extremely rare – but bad scenarios are common (too much or too little of any macronutrient, key micronutrients, a change in the internal or external environment etc etc) and this little fellow and his board of directors (no – not the hypothalamus or pituitary!) – well it’s their job to ‘read the room’, right?!
In the absence of this key understanding we risk: A lot of lazy labelling in thyroid health – ‘You have a bad thyroid – that’s why you…[can’t lose weight, feel tired, have SIBO etc]’ Misdirected treatment & especially a tendency to overload the butterfly with ‘thyroid’ nutrients – which can do more harm than good
I’ve said many times, ‘perfect number pathology is a myth’ but it runs rife in practitioners’ beliefs about TFT results with complete disregard of the person those labs belong too! Did you know, for example, that your TFTs should all be higher if your BMI is? That your T4:T3 ratio should never be 3:1 if you are on replacement, have hot nodules, are pregnant or are acutely unwell etc etc etc? How about how low your Selenium or Iron levels need to be before this factor will influence the actual levels of thyroid hormones measurable – & what the impact of these deficiencies are well before then that is far more sinister and serious? Yep…you see here I am, pouring just some of the tiny take-homes of Advanced Thyroid Assessment ALL over you!
Watch this space my new Thyroid training is just around the corner!
An increasing number of our patients have thyroid concerns but unbeknown to many of us the most likely explanation of all is thyroid nodules, whose incidence is on the rise globally. The development of nodules has always been primarily viewed as a nutritional disease. Traditionally attributed to chronic iodine deficiency but recently novel nutritional causes have emerged. Benign nodules come in 2 flavours: hot and cold and while patients can present with a mixture, it is the presence or absence of a hot nodule that radically changes what complementary medicines you can and can’t use and what an effective treatment plan looks like. The pointers, as is often the case, are there for us in the patient’s presentation and pathology, so knowing the difference is no longer a guessing game. This UU30 comes with a great visual clinical resource and includes key papers on the nutritional management of nodules.
And health, no matter which side you sit on, seems to be particularly plagued by them. I (incorrectly) recall my 4 year degree as being a series of deep personal losses, some favourite food, then caffeine, then alcohol etc etc.😂 Likewise, I’m aware that naturopathy & integrative health’s ‘voice’ in the ‘conversation’, could arguably be perceived as mostly a negative one – as in, ‘No. Never. Not good. No, not even a little bit?!’ But I love both playing devil’s advocate & reading the research (ALL the research – even the stuff that doesn’t support my views and position GASP!~) so I am less in favour of absolutisms. This came up recently when I suggested alcohol may improve iron uptake 😬
Practitioners’ responses were 1 of 2 types: humorous dismissal (“steak & beer for breakfast – at last a naturopathic prescription I can support!”) or horror. But why are we so attached to the absolutes in spite of contradictory evidence?
Let me ask you this: is coffee bad? Full stop? Period? The end? Or is it the most concentrated source of antioxidants consumed in the average Western diet? Does it improve bile flow, peristalsis and at higher levels actually protect the liver against damage? Clearly, we need to read all the evidence, including, the favourable and make individual decisions about ‘what serves and what sabotages’, for each patient. But do we? Or do we imagine we only get membership to the ‘Ultimate Integrative Health-club’ when we adhere to blanket bans?
Similarly I, like many of you, see a LOT of iron deficient women – & a fair chunk of these have been incorrectly labelled, ‘refractory’ because theconventional correction strategies (high doses everyday) don’t actually make sense. But like you guys too, I’m always on the hunt for new ways to improve iron absorption in these women, so I can hit them & their gut with less. That’s why I shared the research regarding alternate day dosing, and taking a supplement within an hour of exercise and now, I dare to ask if a tipple could be helpful?
While we know that both ‘GOOD’ (exercise) & ‘BAD’ (alcohol) health behaviours increase gut permeability, which sounds ‘BAD’, right?
But could this be ‘GOOD’ for some?
This has certainly been demonstrated in relation to exercise & iron but most of the research investigating how alcohol intake effects iron uptake and status is based on alcohol abuse. The study below, however, based on a large sample of non, mild, moderate & heavy drinkers captured in NHANES data – is a very well written and reasoned article, such that it can exclude liver damage, inflammation and HFE mutations as other explanations for the better iron status, in drinkers. And it found:
I challenge you to read it for yourself and challenge your absolutes!🤓
Oh and just in case you’re thinking, “Have we all misdiagnosed iron deficiency and it’s actually a Copper deficiency underneath?”because last year the fashion was everyone was copper toxic and now this year someone’s making noise saying everyone is copper deficient !!! (Absolute? Anyone?!) Ah, no. Copper deficiency, as a cause of iron deficiency and anaemia, has been around for about as long as nutritional medicine itself. It is absolutely a thing. But in the absolute minority of people. And if you go back to some basic maths & compare and contrast Fe & Cu at each level: 1) requirements almost 20mg Vs < 2mg 2) average intake (inadequate Vs adequate) 3) bioavailability (Fe < 20% more typically < 10% in a modern low meat diet Vs Cu is typically >50% ) and do some basic sums I call, ‘Menstrual Maths’ – You’ll likely deduce that inadequate iron intake and uptake, given our losses, is in fact the common culprit and a ‘coldie’ may be more beneficial than copper in most! Can y’all stop asking me about that now – pretty please?
And then you don’t. The reality is we all struggle at times with correcting low ferritin or iron deficiency anaemia – so what have we got wrong? In spite of being the most common nutritional deficiency worldwide, the traditional treatment approaches to supplementation have been rudimentary, falling under the hit hard and heavy model e.g. 70mg TIDS, and are relatively unconvincing in terms of success. New research into iron homeostasis has revealed why these prescriptions are all wrong and what even us low-dosers need to do, to get it more right, more often!
Did you know you can subscribe to these? We deliver at the end of each month, just add a 12-month subscription to your cart and Rachel’s latest research is on it’s way to you!
An ideal T4 is 15
An ‘anti-aging’ DHEAs must be >7
A ferritin of 100 is optimal for women…
I’ve heard it all, probably you have too, and far too often & too recently from practitioners who should have rationalised & researched their way beyond these functional falsehoods, by now. I bought into these ‘optimal wellness truths’ hook line & sinker early in my career and proceeded to even propagate a few but with (not much) more experience in clinic, I had to seriously question this pursuit of ‘perfection’ & ‘perfect pathology’…in favour of reality & scientific evidence! They didn’t add up. Not with my patients – even the healthiest ones, in fact some of the really unwell ones occasionally had these kind of high-normal results and they were part of the problem!. ‘But that’s because no one is truly healthy outside of those seeing a functional medicine practitioner & supercharged on supplements & hormone replacements!!’ came the counter-argument. Ahhh, really?
How then do we reconcile this with the following: Individual genetics & biochemistry
Our biological resilience Healthy & appropriate senescence Large datasets of mixed race populations from other comparable first world countries…where these figures denote the statistical outliers?
I mean, if the 50th centile value for ferritin for actual living, breathing, bleeding, women in the US, Canada, Australia etc etc is 30-40 ng/mL and the 95th centile is 126 ng/mL and the WHO says that in fact, anyone menstruating with a ferritin > 150 ng/mL should attract suspicion for iron overload….but functional medicine men (mostly…sorry but it has to be said!) say 100 IS OPTIMAL FOR EVERY WOMAN #@^*…please tell me in which women, consuming what kind of diet, where in the world, & based on what improved or better health outcomes?
And while you’re there can someone please support this bold claim with a scrap of high quality evidence?? [Rant over🎤💧]
The falsehoods of functional medicine include the blanket belief, ‘more is better’ (ahhhhh not when it comes to many things, including iron where women’s lower levels have been found to be an evolutionary advantage…guys). But you know what, we’re better than that! We see each individual, recognising all the factors at play that make for their uniqueness, help to define what ‘healthy’ looks like for each person and don’t fall for one-size-fits-all claims without any evidence nor common sense even, to support them. What do you think?
Let’s make sense of the over-arching nutrition principles, that will profoundly change your understanding and application of this modality Truly understanding the ‘big’ concepts, so often overlooked, or incorrectly taught, ensures you get the critical ‘small’ detail in your nutritional prescriptions right. In this 4 hour recording, together with key clinical tools, we talk about the tough stuff: dose-response curves, active versus passive stores and excretory pathways and ooh lah lah…the myth of taking ‘activated vitamins’. Even those who feel satisfied with their original training – will find a lot in this critical review that is new, insightful and truly practise-changing!
I’m intrigued by the silence. Hair loss in women is frighteningly common, following pregnancy, menopause & with extreme stress (wait is that a tautology? 🙄) In fact it can strike at any age and for a multitude of reasons. When it happened to me a few years back I also initially responded with silence, terrified that if I said it out loud it would make it real, but when my daughter suddenly asked, ‘Mum are you losing your hair?’ with her trademark attention to detail & exquisite empathy, she gave me the words & a good kick into gear, simultaneously. Now I am fascinated by women’s silence around this generally, how little we share our stories & forewarn others, & as practitioners, the lack of adequate training we’ve had identifying the different types (hint: it involves donning gloves or if restricted to online consulting, knowing how to organise correctly positioned pics) & from there finding the right solutions.
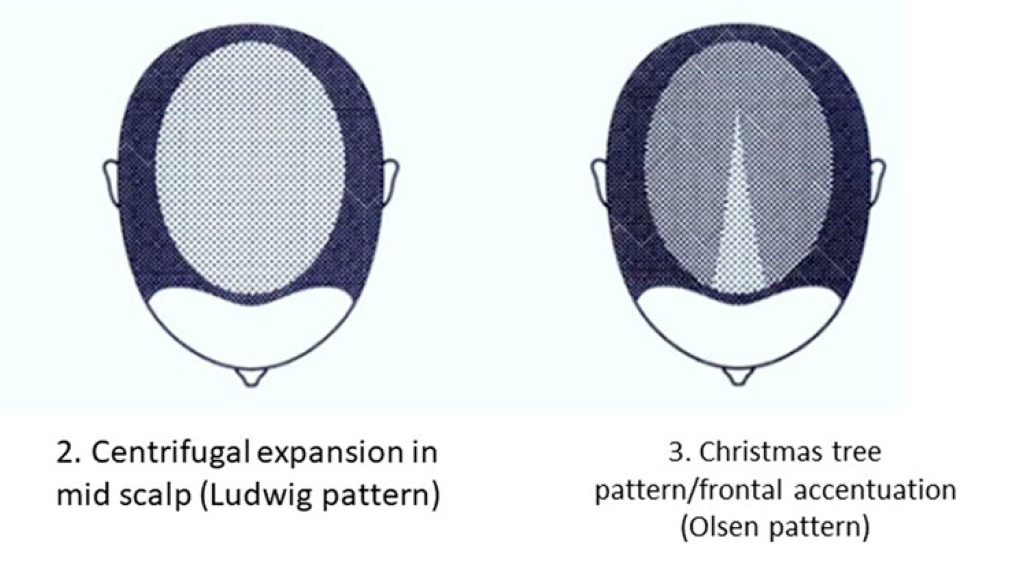
While Female Pattern Hair Loss (FPHL) is the dominant type in women – it only applies to the following pattern:
But alopecia due to stress, thyroid disorders, autoimmunity, contact dermatitis etc will affect different regions of the scalp and with a different onset & progression.
And remember, by the time YOU, the practitioner, can spot a patient is losing hair when they simply walk into the room, they have ALREADY LOST 50%😢 This is why I think we need to push back against the silence. The research is unflinching about the serious psychological impact this has on women – especially in cultures which place so much emphasis on looks generally, and hair, specifically as a commodity of very high value in women. The diagram above comes from a 2019 update on the phenomenon of FHPL and it’s a good articulation of the knowns and unknowns (pssst spoiler alert…it ain’t about androgens!) but let’s never forget the other causes and cures. So let’s make sure as the trusted practitioners women present to so often, we are sensitive enough to have this tricky conversation & skilled enough to help 💪
Stop Pulling Your Hair Out – The FPHL Answers You Need
Female Pattern Hair Loss (FPHL) is everywhere, perhaps you just haven’t been looking. As the leading cause of alopecia in women globally and with 1 in 5 women affected at any age, we’ve all got clients who have FPHL to different degrees. We need to be better able to recognise the early features of this condition which profoundly impairs quality of life and induces depression in its sufferers and that begins with validating patients’ concerns when they report “thinning” or “increased losses”. But what do we do from there? This recording talks you through the assessment, diagnosis and management of FPHL based on a combination of the most recent research and Rachel’s clinical experiences. Once you’ve ‘seen’ FPHL.., you won’t ever ‘unsee’ it and your patients will thank you.
While many of us have made it our business to ensure we are competent IN the business of understanding patients’ iron studies, it sadly seems, many even in teaching and training positions, still have not 🙁 I was sent 2 messages this week that had me lost for words (other than expletives). The first, an email from a final year nat in student clinic with the subject: Please tell me I’m not crazy!!
“Fasted male with high ferritin & high-normal transferrin saturation at two time points, with constantly raised Liver enzymes & neurological Sx. He is currently being treated for blasto in student clinic because they think the high ferritin comes from “blasto infection!!! He needs to be checked for an HFE mutation, right??”
Ok so high ferritin because of ‘blasto’ is NOT A THING! And on the HFE front…Correct! I ask, “Have you mentioned this to the supervisor? What do they say?” Student’s reply, “They say HFE mutations are uncommon so, in a word, it’s not it. But THANK YOU!!!!!!!!!!!!!!!!!!!!! I feel sane again” So, what do I do? The student is studying at a leading institution, one that has sought advice and input from me in the past regarding their diagnostics curriculum, but it would seem, the clinicians they allow to supervise our precious next gen of nats are not expected to be even as competent as the students themselves. Danger Will Robinson! Danger! [old tv show reference…apologies, young folk!] I’ve [not] recovered from this when I get hit with the old 1-2! A naturopath messages me with a screenshot of a FB group exchange over a set of iron results: Ferritin over 400 but low serum iron and transferrin saturation values…which another health professional, who offers training to naturopaths, says is ‘Iron Deficiency’
Email says, “Please help me, I’ve worked so hard to understand iron studies and this has just CONFUSED THE #@*^ out of me!”
Again someone who would typically defer to the voice of authority here, fortunately knows enough to know to question this (mis)interpretation.
I tell you…you may have thought that when I previously wished for all health professionals to be competent in reading studies…but it’s actually a big ask, it would seem 🤔 Could we just, as a start, get anyone who professes to teach, train or mentor health professionals, to actually get up to speed on this themselves or…keep their mouths 🤐
Overt Iron Deficiency Anaemia or Haemochromatosis aside…do you understand the critical insights markers like transferrin and its saturation reveal about your patients iron status? Most practitioners don’t and as a result give iron when they shouldn’t and fail to sometimes when they should. This audio complete with an amazing cheat sheet for interpreting your patients Iron Study results will sharpen your skills around iron assessment, enabling you to recognise the real story of your patients’ relationship with iron.
Or better yet, go the whole hog, with our Iron Package
A few things really took up a disproportionate amount of our time & attention in 2020: Zoom, Mask Fashion & Gin based hand sanitiser.On a personal note I need to confess another: Iron. So while my one true (mineral) love remains zinc, iron answer hunting has infiltrated a lot of my days and some nights! There’s no hiding it…3 out of my 12 UU30 episodes this year have iron in the title 🙄 a sure sign its been on my and my mentees’ minds and sitting across the desk from a lot of health professionals in human form. And this affair I’ve been having, like most, started innocently… it started with a just a ‘quickie’, you know a quick question from a well meaning practitioner: “So, what’s expected in terms of ferritin levels across pregnancy?”
There are 2 answers to this. The first reflects the practice guidelines for GPs and obstetricians in most western countries: > 30 mcg/L regardless of trimester And then there’s another that is [ahem] evidence based, accounts for the essentiality of physiological anaemia in pregnancy &, naturally, trimester specific
There’s a big Fe-ar factor at play when it comes to answering the question, ‘Does this woman have enough iron for her and bub?’ Public health and practice guidelines appear to assume we are ‘guilty’ until proven innocent, patients are worried and health professionals are plagued with their own doubts about whether they’re ‘reading this right?!’ I’m sure we’ve all been in the situation where we feel our pregnant patient is doing well iron wise early in pregnancy, only for them to have that routine antenatal 28wk GP/Ob visit and discover a total panic has descended upon the patient and the rest of the health care team, with calls for ‘IV Iron STAT!’ But 28wks is the height of haemodilution right? You know, that time when ferritin, Hb and Hct should look at their lowest, right? There certainly is a limit to how low we want any pregnant woman to go – for her and her baby’s health but that limit is not the one routinely used and the truly evidenced based one is going to shock you. So what? What’s the issues if we are a little Fe-ar based about Fe, resulting in hypervigilance (calling a deficiency when there isn’t actually one) and giving them a ‘boost’ of more iron, surely this is good news ultimately for baby’s iron levels and for lactation and for…sorry what? No?
There’s a U shaped Curve for Iron supplementation & serum Ferritin levels in pregnant women?!!
It starts with a simple enough question: What should women’s ferritin levels be in pregnancy? But the answer will surprise many. There are in fact two. The first reflects the practice guidelines for GPs and obstetricians in most western countries regardless of trimester and then there’s another that is arguably more evidence based, accounts for the essentiality of physiological anaemia in pregnancy & is also, sensibly, trimester specific. To challenge the ‘noise’ and have the confidence that ‘normal’ is ‘enough’, we need to better understand the mother’s protective physiological adaptation of iron regulation and the intricate systems the foetus has to ensure its needs are met. This of course is not without limit, so we need to also be clear about the maternal serum ferritin threshold for negative impact on the foetus and newborn. Getting the balance or iron right in pregnancy for both mother and baby, is perhaps easier than we have been led to believe.
I talk so much about iron, I feel like I’m cheating on my life partner (Zinc)…but these two are arguably the main mineral deficiencies we encounter most consistently in our patients and, don’t tell Zn, but quite frankly, in terms of who’s more well recognised out there, Iron throws some serious shade! But the truth is they’re a ‘twofor’, as a result of their similar distribution in food, with both demonstrating significantly better bioavailability (read: virtually double) from flesh foods etc, ‘Watch out, she’s on the attack again!’ I can hear the V’s (vegetarians and vegans) say and yes I think you see this one coming…but I think it’s possible to be pro moderate meat, without being, antiV.
Ethical and environmental aspects aside (just momentarily) it is hard to argue against the nutritional benefits from moderate meat for most patients.
I tried, trust me. Put my own body on the line (and my babies) to be a vegetarian for over a decade. But as the wheels fell off for me, I noticed them falling off for so many others…and these were people who were educated, with a capital ‘E’ and putting serious ‘E for effort’ into substitution etc Not everyone of course – but a LOT of women and occasionally some men. There was no denying their ‘iron hunger’ (high serum transferrin), their movement towards microcytosis (however slight that ‘smallifying’ may be…we don’t wait for anaemia, right?), their poor zinc status and more importantly, the clinical chaos of impaired immunity, some cognitive or mood issues that presented, as a result. I went back to the mineral manual, back to all the science that helps us to understand these minerals especially in a modern dietary context.
Ah yes…meat has become marginalised in our diets compared to those of our yesteryear selves (ABS data) while our consumption of potential mineral inhibitors…you know, all the good, but bad, but good foods, like legumes and grains and green tea and and and…has risen…especially among the kind of clients who come to see us, right?
Which ultimately leads to a lower iron ‘income’ with the same outgoings, again especially for menstruating, pregnant & breastfeeding women.
The books don’t balance. (So then…IV Fe to the Rescue???)
Bite me…it’s just science. There have been some wonderfully thorough studies on this very issue and thoughtful discussions. This study in particular, by Reeves et al, of Australian women in their 20s followed for 6 years to 2009, argues that just a 1mg/d increase in heme iron from flesh foods could reduce susceptibility to the subsequent development of iron deficiency amongst omnivores. So while the median daily intake of fresh red meat in these women was just 39g/d, their analysis found that an additional 70g of lamb or 60g of beef…or about 140g of chicken and 250g of fish if you prefer white over red, appeared to be the positive tipping point for women and their ability to stay iron-replete. Well below ‘dietary guidelines’, nowhere near the scary cancer correlations (which of course may be more about fat or nitrates or ??). Moderate meat intake, right? Just saying. And don’t worry, I know. The only thing worse than an evangelical ex-smoker is a rambunctious reformed vegetarian 😂
Need A Manual on Minerals?
Minerals represent a critical tool in naturopathic nutrition and there has been an explosion of research in this area over the last 10 years. In order to optimise patient care, practitioners need to keep up with the constant stream of information, updating their previous beliefs and understanding in the process. This seminal 7hr seminar (!!)…yes…seriously..it’s THE MANUAL..is designed to facilitate and accelerate this process of review and re-evaluation via a fresh look at the key minerals iodine, selenium, iron, copper, zinc, calcium and magnesium.
When I deliver foundational nutrition training to GPs I talk tough. It’s a tough field, right? Compared with the relative certainty of pharmaceuticals, their established pharmacokinetics, their sophisticated delivery systems to ensure high bioavailability…trying to fix micronutrient deficiencies in patients can feel a lot like you’re trying to perform minor miracles. Take iron for something different, its homeostasis pivots on its tight regulation at the gut wall – and this is a wall that is very tight!! At best you get about 10% of a supplement taken up, at worst you get none and the harder you push & the higher you go with your dose…the lower the fractional uptake. Tough stuff, right?!
It’s about at this point in my talk I read their collective minds and say, “I know, you’re thinking, oral supplementation is for suckers – what about we bypass that road block and use IV?!” [Ok, I definitely use nicer words than this]
And then I put up a list of pros and cons about IV micronutrient repletion: ‘100% bioavailable’ & ‘Bypasses the body’s regulatory systems’, go on both! You see, time & time again we discover, when we think we’re outsmarting the body, it still manages to outsmart us. There are some exceptions to this – some nutrients (Vitamin C) and some contexts (late pregnancy iron deficiency) but the broader promise of ‘rapid replenishment’ for everyone, in your lunch break, via an IV infusion..is not realistic, responsible nor without risk. Don’t get me wrong, I am an advocate of appropriate IV Fe use and have encouraged a small fraction of my patients to take this path. However, given the dramatic rise in prescriptions for this since 2013, I think it’s time to stop and seriously review each element: In reality what does it achieve and in whom is it a responsible recommendation; Was a risk benefit analysis performed for & communicated to each individual & was the remaining risk mitigated?
Think anaphylaxis is the major concern? It might be the most lethal but there are more serious concerns due to higher incidence with newer preparations.
So, how well do you know your different IV iron forms, and their predilection for potential problems? And have your answers ready to all the questions raised above? In order for all involved to make an informed choice (both practitioners and patients), we must.
You’re welcome 😉 and hey welcome back to tough talkin’ Tuesday…
While rates of iron deficiency and related anaemia continue to grow, the increase in prescriptions of IV Fe have expanded exponentially in western countries. What is behind this change in practice regarding how we treat iron deficiency and does it match with responsible prescribing? Do the benefits always outweigh the risks? And while we’re on the topic, who is most likely to benefit and what are all the risks? In light of a current class action in the US, relating to a lesser talked about adverse event associated with IV Fe and recent complaints here in Australia against GPs, allegedly due to inadequate information to enable informed patient consent…it’s time to answer these questions and more. When is IV Fe a means of rescue and when is it a risky repletion strategy with no evidence of advantage?
A 26 year old woman suffering years of fatigue from ‘persistent iron and B12 deficiency’ repetitively treated with both oral and IV, walks into a compounding chemist and finally meets her match 🐱🏍 A naturopath with years of experience working the frontline, used to dispensing iron galore (& to a lesser extent B12) to young women with similar stories. But this naturopath requests to see all her labs, she meticulously collates them and then she comes back to the client and deals the fatal blow: Has the iron or B12 ever made you feel any better? “No,” she replies.
“I didn’t think so,” says the Naturopath…”everyone’s been barking up the wrong tree all these years!” And she was right.
First glance at her blood results has all of us reflexively reaching for the same diagnosis everyone has made before – crikey that serum B12 is terrible! And then there’s the fuzzy family history of relations ‘needing’ B12 injections and some even with confirmed pernicious anaemia. But wait up…let’s keep our critical thinking hats on once you look over the rest of the lab you see there’s no evidence of functional B12 deficiency (no rise in Hcy, MCV even RDW) and then, the statement that seals the deal, ‘B12 injections have never made me feel any better’. This woman is not feeling the pinch of pernicious anaemia, not the crush of cobalamin clinical deficiency. In spite of being told that for almost a decade.
A low serum B12 value can of course flag a deficiency and we must never ignore it. But given the serum measures, in fact, predominantly Transcobalamin I (TCI), which is the carrier or taxi for B12 that almost ‘never drops its passengers off’, we are less concerned than when we see a low active B12 (TCII aka ‘the real deal’)
So what else could leave someone with less TCI, while not in fact creating a genuine functional deficit of B12? SNPs?🤧 Bless you!…Sorry that sounded like a sneeze and this retort, as we know is almost as common as the common cold! Sure…of course it could be sexy SNPs…but wait, what about something a little less ‘zebra’…a little more horse. The COCP…oh blooming heck..she’s spent the last decade on the COCP and guess what, its impact on B12 is thought to be principally a reduction in TCI! Oh and that iron story, that supposed ‘iron hunger’ we can see with her upregulation of transferrin? Well that’s an artefact of the COCP too, right? And BINGO was her name-O 🕵️♀️
B12 is a routinely under-rated and recognised micronutrient, which is in fact in high demand by many of our patients. As nutritional research pushes back against defining adequacy as simply the prevention of the deficiency-associated disease (macrocyctic anaemia, irreversible neurological damage) we enter a new landscape of more individualised approaches where we’re better able to recognise and treat those at risk of falling below ‘optimal’. But how do we accurately identify this and then choose the ‘best’ B12 (methyl- cyano- adenosyl- hyroxo-) supplement? Does it need to be this complex? Time to sort the B12 from the B*S#!! This recording comes with a bunch of great resources including a clever clinical tool.
Listen to me, I’m sounding all sporty 😂. I’m not though, just in case you suffer misguided visions of my virtues! But it’s not just the self-declared serious athletes that we need to have on our radar in relation to optimising their oxygen carrying capacity (aka window to winning). Our clinics are full of people, regularly running, doing triathlons for fun (!), riding vast distances clad in Lycra to drink coffee in other town’s cafes etc. etc. whose FBE might be feeling the pinch! That’s right! All these individuals, depending on the frequency and intensity of their exercise, could have the so-called, anaemia of an athlete.
Long gone is the idea that exercise-induced changes to your haemoglobin and red blood cells and perhaps even your iron, would only affect the ultra-marathon runners among us. It’s the swimmers, the cyclists, the Roller Derbyists, the CrossFitters, the basketballers, the Gym Junkies, the lawn bowlers..ok I may have gone too far now…they all are at increased risk.
Why? Isn’t exercise good for you? You know I so want to say, ‘Surprise! It’s not!’ but alas. Of course it is good for us BUT there are some fascinating challenges regular exercise can throw at your dear old blood and its bestie, iron. These challenges are incredibly dynamic – having one effect during exercise, a different one immediately following, and yet another in the days of rest in between. And sometimes, in fact, often, our patients can end up on the wrong side of these seismic shifts. Here’s how the story usually goes
“Oh yeah..I’ve had anaemia for ages! You know and it doesn’t matter how much Iron I take or how I take it – it never budges. But I’ve been told to stay on the Ferrograd anyway”
Typically, being told it’s ‘Athlete’s Anaemia’ is the first, in a series, of many many errors to follow. Because in fact, there is no such thing. That’s right. Anaemia is a symptom not a disease and exercise induced anaemia comes in 4 common flavours: Dilutional, Heamolytic, Iron Deficient & Acute Anaemia of Exercise, and knowing the difference is critical to correct management. Only 1 of them will reliably improve with iron and it needs to be prescribed in a totally novel way. Others will get worse with more iron. Yep. And one is a complete illusion. So when we don’t make the right diagnosis, which of the 4 types your patient actually has, we fail to find the fix. And while all of our patients may not be overly obsessed with improving their performance or even winning, let’s face it, they all want to achieve their PB, that’s why they came to see you. So can you tell the difference?
WARNING: I got so enthused about this topic that I went over. The current ‘Update in Under 30’ is a ‘serving suggestion’ only! And you may need to speed up your playback to squeeze in another bonus 10 min, if you can only afford your usual 30 min car trip to listen!
Outrunning ‘Athlete’s’ Anaemia
Persistent ‘hard-to-resolve’ anaemia is a common presentation for anyone participating routinely in sport and that can be at any level, not just among the professionals. From our lovely ladies who take up running or CrossFit in their middle-age, to our MIL (men in Lycra) and ‘weekend warriors’, they may love it but their haemoglobin and their iron doesn’t! Anaemia equals reduced oxygen carrying capacity, a concern for anyone interested in optimising their performance but equally relevant to patients just trying to manage their energy throughout the day. In this important episode we identify 4 different types of anaemia seen in patients as a result of exercise, incorrectly lumped together as ‘Athlete’s Anaemia’. Each type is easy to recognise once you know how and effective treatment of each is remarkably different. This summary and the super handy clinical resource that accompanies it will help you and your patients absolutely outrun it, at last.
For all Update in Under 30 Subscribers, you will find it waiting for you in your online account and don’t forget the **EXTRA BONUS LIVE CALL WITH RACHEL.
**This live Zoom call with Rachel is for current Update in Under 30 Subscribers ONLY. A Q&A session for subscribers on the UU30 episodes released in 2020. Contact the RAN Team to reserve your spot!
It’s that time of year when we tend to set our intentions both personally and professionally. For me, between the many meals, pressies and dunks in the river, I slip into some ‘silent work’. In particular, I find myself flagging a couple of key areas that I want to sharpen my knowledge in this year. I’ve already picked mine…have you identified yours?
For many practitioners if there is one topic in nutritional medicine that seems to be more generous than any other it would have to be iron: Iron gives us patients…loads of them! Patients who present with deficiency, with overload, with something in between but still noteworthy, or on iron and that’s causing them all sorts of problems.
But Iron’s generosity doesn’t end there.
It also tends to give a lot of practitioners a bit of a headache!
That’s because a) we were mistakenly taught about iron as if it were just another one of the mineral mob and accordingly allocated grossly inadequate time to do more than scratch the surface of what we need to know and b) what we need to know, thanks to it being the most researched mineral, has undergone a couple of major revelations and revolutions since then anyway! So we can benefit from Iron’s generosity most and leave its other unwanted pressies (the headaches, confusion, frustration & suboptimal management of patients) under the tree – we just need to give iron the real attention it deserves, filling in the gaps in ours and many people’s knowledge about this critical nutrient. And boy, do we (and I mean everyone!! including doctors, midwives, pharmacists…anyone who has ever called iron deficiency on a client!!) need to learn how to correctly read iron studies!!!
Because iron also gives us much needed insight into other micronutrients and just how exquisitely sophisticated their roles & regulation can be. Thanks to it being one of the ‘older minerals’ we know more about it than any other and in turn we have the most advanced assessment methods: Iron studies, a collection of 4 parameters, like 4 chapters in a book or 4 key characters in a play, that need to be viewed separately and then together to understand the whole story.
Yes it’s true the learning doesn’t ever end and as I’ve continued to learn about new iron research I’ve added to our one-stop-iron-resource-shop..the Iron Package. Our very latest edition? A new clinical cheat sheet with some other important numbers on there you want to have at your fingertips whenever you read iron studies. So if you’ve already purchased and have access to the Iron Package…SURPRISE! 🤩 Go back and look again and if not, there’s never been a time like now. Oh iron, you’re sooooo generous!! 😉
Listen to these audios and download the resources straight away in your online account.
If you’ve already purchased ‘Update in Under 30: How to Read Iron Studies’ or ‘Iron Package’ you will find this new clinical cheat sheet available with these audios when you log in to your account.
Yet another super-helpful part of Iron-Land has been mapped!! Ever struggled to correct chronic iron deficiency in athletes or even just weekend warriors? Yep, me too. One of the key barriers being the 2-3 fold rise in hepcidin in response to exercise. Hepcidin whose day job is an inflammatory signal that two-times as an iron uptake blocking agent at the small intestine. In addition to other exercise-induced factors that either reduce Fe uptake or increase losses, it really is no surprise that these cases can be hard to treat. However, a recently published small Australian study has brought to light some constructive new information. Similar to the often talked about ‘anabolic window of opportunity’ whereby we encourage people to consume protein +/- CHOs within a short time-frame post-exercise to optimise exercise outcomes and negate negatives, these new findings imply the same might be true for optimal Iron uptake. But only in relation to exercise done in the morning!
The key finding was when individuals consumed iron after 90mins of exercise in the morning they exhibited higher uptake than both when they took the iron at the same time but didn’t exercise beforehand or took it after exercising at night.
This is a game-changer for potentially ALL our patients who struggle with iron absorption. With the key take-home being…not just take your iron preferably in the morning which we already know (when hepcidin is naturally lower as part of its diurnal rhythm) but before you pop that pill, pop on your sneakers and get busy sweating! How on earth might this be working? Well this study demonstrated that while hepcidin rises after exercise typically for up to 6hrs…it is not yet ‘up’ and blocking within the first hour – gotcha! But why would this mean an even greater uptake compared with the same iron at the same time in the same individual…but a resting version of themselves? Because exercise may in fact cause a transient leaky gut post exercise & enhanced nutrient uptake may be its silver lining! A small study that actually punches above its weight, this one is worth the read – via a great comprehensive summary on Medscape if you have it or you can check out the abstract.
Our ever-expanding Iron knowledge gives us great hope for the improved understanding we are likely to reach with all nutrients in the future. Let’s not forget Iron has about a 70 year head-start on other microminerals such as Zinc and almost a century on Selenium, which was identified to be essential in just 1979!
And the contrast is apparent anywhere you care to compare and contrast the ‘older’ with the ‘younger’ nutrients. Just look at iron studies. A personalised detailed account of each individual’s iron story: how much you’re consuming, how effective you are at absorbing what you’ve been offered, how hungry that makes you for more and what good stores mean to you (not some fictitious average male or female)! All told through 4 distinct but inter-related markers: serum iron, transferrin, transferrin saturation and ferritin. What can we glean from our current routine assessment of Selenium in contrast? Their short-term Se intake…yep. Looking forward to the multi-parameter markers of each individual nutrient we just might have at our fingertips in the future, thanks to iron nutrition which continues to teach us how sophisticated nutritional physiology really is 🙂
We know the most about iron and yet we know there is always more to learn. And who better to teach us this than our clients with iron deficiency or iron excess? Need some help getting across the most important aspects of recognising and correcting each iron issue in clinic? We released an Iron Package earlier this year for this very reason. It covers how to really read iron studies (with a great cheat sheet), how not to fall for a fake (deficiency) and what the best supplements and dosing regimes look like and how that differs in pregnancy, athletes, those with marked gut issues and other key groups. It’s your 1 stop iron shop.
We’re not deaf…we heard that stampede of Iron-Inundated Practitioners!
Our recordings and clinical resources for improving your skill-set in all things iron including, your accuracy of diagnosing deficiencies, pseudo-deficiencies & excesses, plus radically rethinking the best treatment approaches for each scenario…have been some of our most popular. Because nailing iron (pardon the pun) is harder than we were all lead to believe and at least 1 ‘iron maiden’ or ‘iron man’ walks into our practice every day, right? So we’ve brought together 5 extremely popular UU30’s on Iron into one bundle for the price of 4! So if you’re more than ready to graduate from ‘iron school’, now’s your best chance!
1. So You Think You Know How to Read Iron Studies? (≤30 min audio + Cheat Sheet)
Overt Iron Deficiency Anaemia or Haemochromatosis aside…do you understand the critical insights markers like transferrin and its saturation reveal about your patients iron status? Most practitioners don’t and as a result give iron when they shouldn’t and fail to sometimes when they should. This audio complete with an amazing cheat sheet for interpreting your patients Iron Study results will sharpen your skills around iron assessment, enabling you to recognise the real story of your patients’ relationship with iron.
2. Pseudo Iron Deficiency (≤30 minute audio)
The most common mistake made in the interpretation of Iron Studies is this one: confusing inflammation driven iron ‘hiding’ with a genuine iron deficiency. Worse still, following through and giving such a patient oral iron – when in fact it is at its most ‘toxic’ to them.
This audio together with some key patient pathology examples will prevent you ever falling for this one! Learn how to recognise a ‘Pseudo Iron Deficiency’ in a heartbeat!
3. Iron Overload… But not as you know it (≤30 minute audio)
We’re increasingly seeing high ferritin levels in our patients and getting more comfortable referring those patients for gene testing of the haemochromatosis mutations; but, do you know how to distinguish between high ferritin levels that are likely to be genetic and those that are not? This can save you and your patient time and money and there are some strong road signs you need to know. In addition to this, what could cause ferritin results in the hundreds if it’s not genetic nor inflammation? This Update in Under 30 summary will help you streamline your investigations and add a whole new dimension to understanding iron overload…but not as you know it!
4. So You Think You Know How To Treat Iron Deficiency? (≤30 min audio)
And then you don’t. The reality is we all struggle at times with correcting low ferritin or iron deficiency anaemia – so what have we got wrong? In spite of being the most common nutritional deficiency worldwide, the traditional treatment approaches to supplementation have been rudimentary, falling under the hit hard and heavy model e.g. 70mg TIDS, and are relatively unconvincing in terms of success. New research into iron homeostasis has revealed why these prescriptions are all wrong and what even us low-dosers need to do to get it more right, more often!
5. So You Think You Know the Best Iron Supplement, Right?! (≤30 min audio + Iron Supplement Guide)
Iron supplementation, regardless of brand, presents us with some major challenges: low efficacy, poor tolerability & high toxicity – in terms of oxidative stress, inflammation (local and systemic) and detrimental effects on patients’ microbiome. What should we look for to minimise these issues & enhance our patients’ chance of success. Which nutritional adjuvants are likely to turn a non-responder into a success story and how do we tailor the approach for each patient? It’s not what you’ve been taught nor is it what you think! This comes with a bonus clinical tool, a fabulous easy reference guide – to help you individualise your approach to iron deficiency and increase your likelihood of success.
You’ll never look at iron studies or your iron-challenged patients the same way.
Listen to these audios straight away in your online account.
And then you don’t, right? Because if my experience is anything to go by, there are some patients that just don’t respond to the usual iron repletion strategies. Depending on how low their ferritin is, this can then precipitate ‘practitioner panic’ (we’ve all had it right?!) where we’re inclined to go higher & higher with the dose and number of doses per day. Typically, this also fails. I hear about this from other practitioners all the time and I see the ‘normal’ doses of iron sneaking up and up. Remember the days when we couldn’t get a non-pharmacy supplement with over 5mg elemental iron in it and now we have > 20mg? But still, I hear you say, this fades into insignificance when you think about the standard medical model for iron correction which provides 100-200mg/day and you’re right.
Gee… after hundreds of years of knowing about this deficiency and being the most common deficiency word-wide, you’d think we had our supplemental regime nailed.
 Do you realise we’re often giving our patients Crabs? Stay with me 🙄 We’re all BIG fans of polyphenols right, but did you know that one of the key ways they qualify as antioxidants is that they chelate metals?
Do you realise we’re often giving our patients Crabs? Stay with me 🙄 We’re all BIG fans of polyphenols right, but did you know that one of the key ways they qualify as antioxidants is that they chelate metals? 











 A 26 year old woman suffering years of fatigue from ‘persistent iron and B12 deficiency’ repetitively treated with both oral and IV, walks into a compounding chemist and finally meets her match 🐱🏍 A naturopath with years of experience working the frontline, used to dispensing iron galore (& to a lesser extent B12) to young women with similar stories. But this naturopath requests to see all her labs, she meticulously collates them and then she comes back to the client and deals the fatal blow: Has the iron or B12 ever made you feel any better? “No,” she replies.
A 26 year old woman suffering years of fatigue from ‘persistent iron and B12 deficiency’ repetitively treated with both oral and IV, walks into a compounding chemist and finally meets her match 🐱🏍 A naturopath with years of experience working the frontline, used to dispensing iron galore (& to a lesser extent B12) to young women with similar stories. But this naturopath requests to see all her labs, she meticulously collates them and then she comes back to the client and deals the fatal blow: Has the iron or B12 ever made you feel any better? “No,” she replies.