Name a B vitamin. Hey, Bingo! It’s on the list! What list? The complete one from all the review papers & references to possible links between individual nutrient deficiencies & Angular Cheilitis – inflammation & cracking at the corners of the mouth. So does that mean more Bs are the answer for people presenting with this painful, recurring issue?…Ahhhhhh No. Yes, you heard me correctly, these deficiencies rarely cause the breakdown of the integrity of this very specific area of skin in the patients we see. So now we have a double ouch, right?
We might send patients away with a B complex and some lip balm and over a week the cheilitis resolves – which one was the most therapeutic? …I hate to tell you 👀
What is the underpinning cause(s) & the important message we are missing with this presentation? Well, it could be one or more of a long LONG list of differentials, ranging from anatomical, habitual, immune related to iatrogenic. And while many nutrient deficiency pictures can include this feature and therefore make the ‘possible’ list, only one makes the ‘probable’ list. And that’s iron but only in severe deficiency, aka anaemia and only affecting 1 in 5.
Me???
…Telling anyone to push the nutritional issues further down the list of differentials for any condition? Well, that’s unexpected
…possibly unprecedented
And no, antifungals aren’t the answer either. Yep, that might be worth a listen….👂
Just an annoying, embarrassing, cosmetic condition or could it be the clue that helps you ‘crack the case’? There is a surprisingly long list of differentials for this condition but most of us only know a few, reflexively reaching for either B vitamins or anti-fungal creams. Does either make sense? Does either address the cause(s) which we now recognise to be a unique series of risk factors in each individual? Or are we at risk of shooting the messenger and missing the message of Cracking Corners altogether?
You can purchase Cracking in the Corners – Angular Cheilitishere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
Last week I had my say about acknowledging our elders & mentors, this week I want to speak to the power of the young peeps. Just like a younger sibling, nipping at your heels can act as a great motivator to move faster, or having children can inspire us to do more to improve the ‘world’ we’re welcoming them into, my interactions with naturopaths, nutritionists & herbalists of the younger generations generally effect both responses in me! The best of these come from cluey ‘youngsters’ (mature-age-second-career-new-nats included!!) who ask the most difficult questions & show dogged determination in getting answers to these either via me or in spite of!
This is exactly what’s been in play over the last few years (yes, you heard me…years) while I’ve been under the watchful gaze of Jostling Josh Weymouth! He’s a youngun’ – it’s all relative right – who has kept us both on the straight and narrow writing:The accuracy and interpretation of plasma selenium in our patients: a literature review,which hasjust been published in the the Australian Journal of Herbal & Naturopathic Medicine.
At the outset I was able to hand over a substantial selenium research hoard I had obsessively compiled, Josh was able to build on this, refine some fledgling theories I had and then completely redefine my appreciation & understanding of how chronic over-treatment (not toxicity…) is so deleterious to human health. Check this out:
When Selenium (Se) saturation point occurs in plasma, there is a potential reduction in health protection… Se will progressively pool within plasma non-specifically as SeMet in lieu of regular, sulphur containing methionine, in albumin and other proteins…inducing oxidative stress via a complex disruption of cell reactions/signalling This is likely to be how Selenium over-treatment increases the risk of both CVD and T2DM
Many of you may ‘Know Your Numbers’ when it comes to Serum Se targets in thyroid health or just generally know how to Stay Safe with Selenium Supplementation because I’ve spoken extensively about these in the past and you will be relieved to know neither my ‘numbers nor my message’ have changed BUT I encourage everyone to read this new article because Josh has added so much more, including the interplay between our microbiota and our individual selenium needs, handling and tolerance and and and….I could go on but…what I really want to say is, thanks Josh for your academic rigor, your firm determination & diligence and for nipping at my heels all this time. This important piece of work just wouldn’t have happened without it 🐶
If I could be granted 1 wish regarding all health professionals, it would be that we were all competent in reading Iron Studies. Think that’s overstating the issue? Or not a bodacious enough way to ‘spend’ my wish? I don’t. Especially when you consider the impact of GPs in this space.
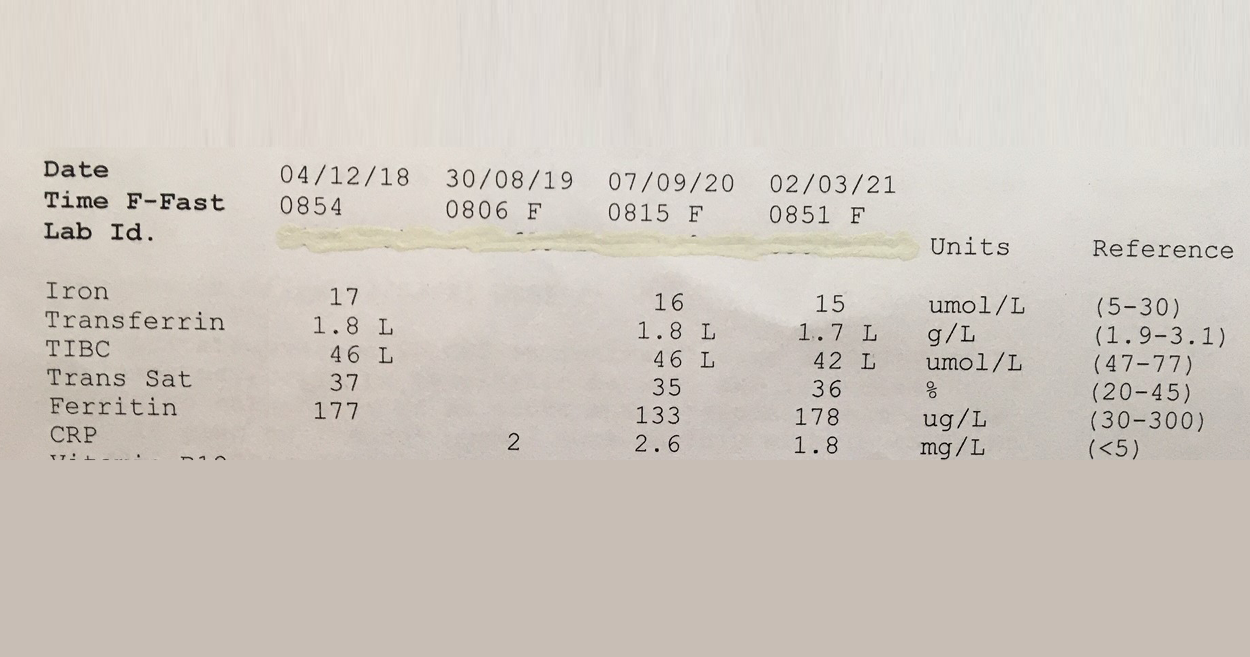
This 57Y male was asked to make a follow up appointment with his doctor, to discuss his ‘abnormal’ results which he was informed constitute Iron deficiency. Consequently he was was advised to start an iron supplement! #@!*
Your thoughts? Revoke this doctors medical licence? Insist on some very du jour ‘re-training’ at the very least? I mean, if you think this Iron pattern flags a deficiency or shortfall, then you’re as good as reading a map upside down and back to front…and written in a foreign language!! The ‘Ls’ in his latest labs flag he has suppressed transferrin, indicative of negative feedback inhibition of GIT uptake of this mineral, secondary to healthy stores or inflammation. And it’s not just that more iron is not indicated but that more iron in fact presents a patient like this with increased and unnecessary risk: to their microbiome, intestinal wall health, even according to the larger longer studies a potential correlation with colorectal cancer risk, if taken long term. Let alone the whole cardiovascular conundrum. Better still this same patient was told a few years back that he might have iron overload! Again the ‘map’ could only have been being read, upside down, back to front to reach such a conclusion!
So the one patient in just a few years by 2 different doctors has been diagnosed incorrectly with 2 different iron issues. Yep.
And sadly I have sooooo many more cases of missed and mis-diagnoses with regard to this mineral. The latest RCPA Position Statement on the Use of Iron Studies, underscores that assessment of iron status and GPs competence in knowing when to do this and how to interpret, is an important part of core general practice. Given it “is the commonest nutritional deficiency state in Australia and is significantly under-diagnosed” This succinct document offers a quick crash course in Iron nutrition for doctors and it hits all the right marks with advice about not ordering ferritin as a stand-alone because “the interactive nature of the three components allows for more accurate interpretation”and this simple but sage advice:
“Transferrin, iron transport protein, tends to increase in ID… A better strategy (than being tricked by Serum Fe) is to report transferrin saturation. A low transferrin saturation in the setting of an equivocal ferritin level is suggestive of iron deficiency. An elevated transferrin saturation is the first manifestation of iron overload.“
I mean seriously, do doctors read these RAGCP resources & recommendations, or is it just me? 🤓😂
Need a rip-roaring review on how to really read iron studies? Or know another health professional who does?!! Consider this Easter Educational Gift Instead of Eggs!! So You Think You Know How To Read Iron Studies?
Overt Iron Deficiency Anaemia or Haemochromatosis aside…do you understand the critical insights markers like transferrin and its saturation reveal about your patients iron status? Most practitioners don’t and as a result give iron when they shouldn’t and fail to sometimes when they should. This audio complete with an amazing cheat sheet for interpreting your patients Iron Study results will sharpen your skills around iron assessment, enabling you to recognise the real story of your patients’ relationship with iron.
‘Hey Alexa, What’s that formula for correcting urinary iodine for hydration status?’ Oh yes, if only she could answer these kind of questions!
There’s no one here by that name but we get these kind of emails all the time [Oh and also for Freya who hasn’t worked here in like 5 years!!😂] But we love them because it means our blogs provide useful, sought after and (we like to think!) really really hard to get anywhere else answers . But hey try it, Ask Siri! We’re always forthcoming with references – not just citations but the full low down and dirty full texts (as long as we’ve managed to get our hands on it!!) and we know which topics particularly hit a spot across our professional group by not just the number of enquiries but how far the actual blog they’re referring to, dates back. So we’ve just received more comms regarding one that’s often on high rotation…a post I wrote on urinary Iodine Assessment & how and why we should adjust for hydration! That was 2014…what a vintage 🤩 Show’s though how topical and tricky this little test is.
The iodine landscape has undergone radical change recently. We’ve moved from recognising the resurfacing of a widespread deficiency, to large-scale food fortification that has failed to correct deficiency in most and produced excesses in a few. Parallel to this, we have the ever growing incidence of thyroid disorders and some radically contrasting ideas regarding iodine’s role in both aetiology and treatment. Micrograms V milligrams? Random urinary iodine or iodine loading test? Important new evidence and clinical experience helps us understand more about how to accurately assess patients’ need for iodine and know when & how to use it therapeutically & when not to!
That’s not a word you hear often spoken by people practising nutritional medicine. Which is odd. I mean outside of the whole, ‘I’m not good with sulphites so I just have to add these magic drops into my glass of red so I can knock back my share,” often overheard at our conferences… it’s like this essential macromineral, pivotal to human health for things like barrier function, antioxidant defence and our basic ability to create the white cells for immune defence (for that matter), detoxification, musculoskeletal tissue integrity etc has just not received its due attention from us. Not entirely surprising given 1) there’s no RDI and 2) there’s no lab test to assess an individual’s status and how about 3) because we were never taught about it!
But the biggest ‘call to action’ here is that, in spite of items 1, 2 & 3, we’re ‘prescribing’ Sulphur Strategies all the time!
Take one of my favourite examples;GAGs. Glycosaminoglycans like Glucosamine sulphate (not the crappy, found to be not as effective, other forms that we now see more commonly) hit the headlines back in the noughties as an effective arthritis remedy. This is one of the 100s of our body’s ‘end products’ of its endogenous Sulphur Stream. We naturally make this in adequate amounts to ensure the integrity of our joints (and many other tissues of course!) when we have enough Sulphur in the ‘top pool’ (organic Sulphur) to trickle down to the 2nd pool (Inorganic Sulphur), therefore creating a constant essential supply of something known as ‘the universal Sulphur donor’ – ‘PAPs’, to its friends 😉 Like a waterfall, it helps to have a good flow from the top to increase the likelihood we’ll have anything to ‘show’ at the bottom.
So when we give a patient Glucosamine Sulphate it may well help. Or not. But did we ‘treat the cause’ of their Sulphur problem? Should we have treated higher up, increasing the size of either the organic or inorganic pool to have improved and widened the benefits for their health? Or, as is equally common, actually identified why someone might need more Sulphur than most – due to increased demand and losses?
Herein lies my reason for liking this particular Sulphur story somuch. The common medication that places the highest ‘demand’ on Sulphur (due to its need for detoxification) is paracetamol. There’s no debate regarding this – just absolute scientific consensus. NSAIDs and steroids also negatively affect the Sulphur status of individuals, as does Vitamin D deficiency and chronic mild metabolic acidosis. Now how commonly are these phenomena co-occurring in our patients afflicted with arthritis? And traditionally of course, what was the remedy for arthritis? Sulphur springs.
Unseen Sulphur – Time To Take A Look If you don’t have a clear picture of the gross daily requirements, determinants of altered individual needs, sources, regulation & associated deficiency picture of Sulphur, you’re not alone. Turns out this essential macromineral remains ‘unseen’ by most, even though you’re probably writing prescriptions every day that have Sulphur as their key component. From the simple: Taurine, N-acetyl cysteine, Protein powders, to the sublime: Brassica extracts & concentrates, N-acetyl Glucosamine, Alpha Lipoic acid etc. In order to use these Sulphur strategies successfully and safely, however, we need to fill in the missing detail on its metabolism, the difference between the ‘organic’ and ‘inorganic pools’, how regulation regularly goes wrong even in those seemingly consuming enough and how to balance the risks of this reactive medicine with its substantial therapeutic value. This recording comes with a great clinical tool to help you, at last, see the Sulphur strategy most indicated for your patient.
You can purchase Unseen Sulphur – Time to Take a Lookhere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
I say: Biotin, Broccoli Sprouts & Bone Broth You say….?
If you said: ‘Sulphur’, go directly to the top of the class, passing ‘Go’ & collecting $200 on your way!🤓 If you nervously said…”I don’t know, they all start with ‘B’ ?”, you are not alone. In fact, most integrative health professionals aren’t aware of the Sulphur Strategies they’re using, probably, everyday. But it’s time we all were.
How about this list? Glycosaminoglycans (GAGs for joint, gut etc tissue integrity), Cerebroside Sulphate (Myelin), Metallothionein, Glutathione, Hydrogen Sulphide (H2S), Co-Enzyme A, Lipoic acid, SAMe, are just some things Sulphur is essential for.
I could go on…and on and on. You see Sulphur, in spite of being an essential macromineral (adult dietary requirements > 1g per day) and critical to health, remains largely unseen. Often we don’t know when we’re writing patient prescriptions that actually we’re using a particular vehicle for Sulphur and therefore we’re also not able to discern which, of the very long list of options (dietary and supplements), makes the most sense in this patient at this time. We’re not to blame, not many ‘possess the power’ to see it, it seems. Por old essential, irreplaceable Sulphur doesn’t even have an RDI. But the time has come to take a good look. We need to know how patients are able to meet their needs, who needs more and how, very commonly, someone who is seemingly ‘consuming enough’ may still exhibit a functional Sulphur deficiency with poor musculoskeletal tissue integrity, low white cell replication capacity or higher oxidative stress load etc and in those who do have a shortfall, how to treat successfully & safely. Who needs a top down approach (more protein, methionine, cysteine, bone broth) and in whom would that be a risky path and using ‘downstream’ Sulphur products instead would be a better balance of pros and cons?
Because all Sulphur needs to be handled with care.
That’s right. Like other highly chemically reactive minerals, with reactivity comes risk – a great potency that requires careful consideration of both form and dose, so that we can harness this power for good not…well evil’s a bit strong…but how about, for not-good. I’m a bit of fan of Sulphur and using Sulphur strategies in my patients. I think it has interesting echoes with our past: the ‘healing’ waters of a Sulphur Spring and of course even further back the old ‘brimstone and treacle’ medicine of eons ago. This paper by Nimni in 2007: Are we getting enough sulfur in our diet? got me thinking about Sulphur again in a contemporary context, over a decade ago, I’ve done a lot more thinking, researching and prescribing since then but it seems that Sulphur still remains ‘unseen’ by most. But with the rise and rise and rise of popular Sulphur-based supplements (alpha lipoic acid, GSH, N-acetyl glucosamine, Brassica & Allium extracts and concentrates, N-acetyl-cysteine etc) I think it’s time to talk.
If you don’t have a clear picture of the gross daily requirements, determinants of altered individual needs, sources, regulation & associated deficiency picture of Sulphur, you’re not alone. Turns out this essential macromineral remains ‘unseen’ by most, even though you’re probably writing prescriptions everyday that have Sulphur as their key component. From the simple: Taurine, N-acetyl cysteine, Protein powders, to the sublime: Brassica extracts & concentrates, N-acetyl Glucosamine, Alpha Lipoic acid etc. In order to use these Sulphur strategies successfully and safely, however, we need to fill in the missing detail on its metabolism, the difference between the ‘organic’ and ‘inorganic pools’, how regulation regularly goes wrong, even in those seemingly consuming enough, and how to balance the risks of this reactive medicine with its substantial therapeutic value. This recording comes with a great clinical tool to help you at last see the Sulphur strategy most indicated for your patient.
The latest Update in Under 30 has landed!!!
You can purchase Unseen Sulphur – Time to Take a Lookhere.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
Key texts tell us, 2nd trimester Serum Ferritin may be between: 2……………………………………………………………………………………….and……………………………………………………………………………………….230 mcg/L But a 2nd trimester Ferritin even > 40 mcg/L is remarkable – and not in a good way🙄 So, ummmm what should it be and why?
Given all the attention iron gets from me alone, you would think we would be a lot clearer and a little ‘clueier’ regarding the answers to core questions like this. But we’re not. Correction, they’re not. Who is this ‘they’ of which I speak, um well, just the dudes in the top level office who write the practice guidelines for GPs, Obs, Midwives etc. Big call I know, but answer these to get my drift:
What is the average Serum Ferritin in healthy women with healthy pregnancies in the 2nd trimester? After all the routine Iron treatment given across numerous countries, in line with the WHO recommendations, is there any evidence that values higher than this have irrefutable benefits for mother or baby? Is there evidence to the contrary, that it can be harmful?
And while we’re busy asking questions that shake the flimsy foundations of the practice guidelines regarding monitoring and managing iron levels in mid-pregnancy – how about we get up to speed with the evidence that shows 1st trimester Serum Ferritin is in fact the most meaningful as an iron marker both in the short and long-run for any woman’s pregnancy. I know, right…this is all sounding very different from the, inappropriately named, ‘normal’, which is to test women at wk28, in the midst of peak haemodilution, and therefore physiological anaemia, and to then send that patient home often with a new diagnosis of iron deficiency and a sense of urgency to ‘fix this fast for you and baby’. In some instances this is appropriate and important, especially women who weren’t comprehensively cared for & whose iron status wasn’t monitored & well-managed in the first trimester. But for so many women, who are just riding the Ferritin-Fun-Bus…they are right on track with looking their very worst!
Couldn’t resist finishing this year of Update and Under 30s with a serious BANG! 🧨🧨🧨
In this continuation of our discussion about better iron balance for mum and baby we now map what is happening in each trimester with regard to requirements and regulation, and accordingly, what ‘healthy looks like’ in terms of both serum ferritin and transferrin, at every time point. This also gives us a clear practice protocol around when and how exactly to treat iron deficiency in pregnant women. Additionally, we review the risks of both under and over-treatment.
The latest Update in Under 30 has landed!!!
You can purchase Pregnancy Iron Balance Part 2 here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
A few things really took up a disproportionate amount of our time & attention in 2020: Zoom, Mask Fashion & Gin based hand sanitiser.On a personal note I need to confess another: Iron. So while my one true (mineral) love remains zinc, iron answer hunting has infiltrated a lot of my days and some nights! There’s no hiding it…3 out of my 12 UU30 episodes this year have iron in the title 🙄 a sure sign its been on my and my mentees’ minds and sitting across the desk from a lot of health professionals in human form. And this affair I’ve been having, like most, started innocently… it started with a just a ‘quickie’, you know a quick question from a well meaning practitioner: “So, what’s expected in terms of ferritin levels across pregnancy?”
There are 2 answers to this. The first reflects the practice guidelines for GPs and obstetricians in most western countries: > 30 mcg/L regardless of trimester And then there’s another that is [ahem] evidence based, accounts for the essentiality of physiological anaemia in pregnancy &, naturally, trimester specific
There’s a big Fe-ar factor at play when it comes to answering the question, ‘Does this woman have enough iron for her and bub?’ Public health and practice guidelines appear to assume we are ‘guilty’ until proven innocent, patients are worried and health professionals are plagued with their own doubts about whether they’re ‘reading this right?!’ I’m sure we’ve all been in the situation where we feel our pregnant patient is doing well iron wise early in pregnancy, only for them to have that routine antenatal 28wk GP/Ob visit and discover a total panic has descended upon the patient and the rest of the health care team, with calls for ‘IV Iron STAT!’ But 28wks is the height of haemodilution right? You know, that time when ferritin, Hb and Hct should look at their lowest, right? There certainly is a limit to how low we want any pregnant woman to go – for her and her baby’s health but that limit is not the one routinely used and the truly evidenced based one is going to shock you. So what? What’s the issues if we are a little Fe-ar based about Fe, resulting in hypervigilance (calling a deficiency when there isn’t actually one) and giving them a ‘boost’ of more iron, surely this is good news ultimately for baby’s iron levels and for lactation and for…sorry what? No?
There’s a U shaped Curve for Iron supplementation & serum Ferritin levels in pregnant women?!!
It starts with a simple enough question: What should women’s ferritin levels be in pregnancy? But the answer will surprise many. There are in fact two. The first reflects the practice guidelines for GPs and obstetricians in most western countries regardless of trimester and then there’s another that is arguably more evidence based, accounts for the essentiality of physiological anaemia in pregnancy & is also, sensibly, trimester specific. To challenge the ‘noise’ and have the confidence that ‘normal’ is ‘enough’, we need to better understand the mother’s protective physiological adaptation of iron regulation and the intricate systems the foetus has to ensure its needs are met. This of course is not without limit, so we need to also be clear about the maternal serum ferritin threshold for negative impact on the foetus and newborn. Getting the balance or iron right in pregnancy for both mother and baby, is perhaps easier than we have been led to believe.
I talk so much about iron, I feel like I’m cheating on my life partner (Zinc)…but these two are arguably the main mineral deficiencies we encounter most consistently in our patients and, don’t tell Zn, but quite frankly, in terms of who’s more well recognised out there, Iron throws some serious shade! But the truth is they’re a ‘twofor’, as a result of their similar distribution in food, with both demonstrating significantly better bioavailability (read: virtually double) from flesh foods etc, ‘Watch out, she’s on the attack again!’ I can hear the V’s (vegetarians and vegans) say and yes I think you see this one coming…but I think it’s possible to be pro moderate meat, without being, antiV.
Ethical and environmental aspects aside (just momentarily) it is hard to argue against the nutritional benefits from moderate meat for most patients.
I tried, trust me. Put my own body on the line (and my babies) to be a vegetarian for over a decade. But as the wheels fell off for me, I noticed them falling off for so many others…and these were people who were educated, with a capital ‘E’ and putting serious ‘E for effort’ into substitution etc Not everyone of course – but a LOT of women and occasionally some men. There was no denying their ‘iron hunger’ (high serum transferrin), their movement towards microcytosis (however slight that ‘smallifying’ may be…we don’t wait for anaemia, right?), their poor zinc status and more importantly, the clinical chaos of impaired immunity, some cognitive or mood issues that presented, as a result. I went back to the mineral manual, back to all the science that helps us to understand these minerals especially in a modern dietary context.
Ah yes…meat has become marginalised in our diets compared to those of our yesteryear selves (ABS data) while our consumption of potential mineral inhibitors…you know, all the good, but bad, but good foods, like legumes and grains and green tea and and and…has risen…especially among the kind of clients who come to see us, right?
Which ultimately leads to a lower iron ‘income’ with the same outgoings, again especially for menstruating, pregnant & breastfeeding women.
The books don’t balance. (So then…IV Fe to the Rescue???)
Bite me…it’s just science. There have been some wonderfully thorough studies on this very issue and thoughtful discussions. This study in particular, by Reeves et al, of Australian women in their 20s followed for 6 years to 2009, argues that just a 1mg/d increase in heme iron from flesh foods could reduce susceptibility to the subsequent development of iron deficiency amongst omnivores. So while the median daily intake of fresh red meat in these women was just 39g/d, their analysis found that an additional 70g of lamb or 60g of beef…or about 140g of chicken and 250g of fish if you prefer white over red, appeared to be the positive tipping point for women and their ability to stay iron-replete. Well below ‘dietary guidelines’, nowhere near the scary cancer correlations (which of course may be more about fat or nitrates or ??). Moderate meat intake, right? Just saying. And don’t worry, I know. The only thing worse than an evangelical ex-smoker is a rambunctious reformed vegetarian 😂
Need A Manual on Minerals?
Minerals represent a critical tool in naturopathic nutrition and there has been an explosion of research in this area over the last 10 years. In order to optimise patient care, practitioners need to keep up with the constant stream of information, updating their previous beliefs and understanding in the process. This seminal 7hr seminar (!!)…yes…seriously..it’s THE MANUAL..is designed to facilitate and accelerate this process of review and re-evaluation via a fresh look at the key minerals iodine, selenium, iron, copper, zinc, calcium and magnesium.
I think I’m finally able to put my ‘late-90s-Creatine-frontline-trauma’ behind me. Back then, like many good nats in training, I was working the trenches of the health food stores and was faced on a daily basis with two types of men with two types of Creatine questions. The first type was scrawny and would ask, ‘will taking this help me build muscle?’, the second, built like the proverbial brick *&#@ house, asking, ‘will it help me build more muscle?’ Cue, eye roll. Come on… any of you current or ex apothecaries, pharmacy or retail assistants…you know exactly what I’m talking about!!! So deep was this trauma that I put Creatine as a supplement, into the ‘strictly sports folder’ in my brain (the bit in the deep dark back with other rarely accessed items) and never gave it much thought when I left retail and moved exclusively into private practice. Even back when I was a sub-editor for the Braun and Cohen 4th edition, it was apparently still too soon.
A great colleague of mine, Emily Bradley, had written the chapter on Creatine and, in doing so, presented compelling case to reconsider this supplement as offering great therapeutic potential well outside of the sports-field. That one was accidental 😂
I actually remember reading that chapter, especially the sections on Creatine supplementation for neurological & psychiatric conditions and thinking….WOW…who knew?! ??!! Well, clearly Emily for one 🙄 and also every author and researcher whose work she had read…so that made quite a lot of people actually! But another [ahem 😳] several years had to pass before the research into Creatine and the argument that this has been a grossly over-looked CAM option in mental health, beat down my door and finally got my full attention. Better late than never. And boy, do we all have some catching up to do!
Let’s start with 5 fun facts: 1. Creatine is critical for energy – like cellular currency it ‘tops’ back up our funds, after increased spending, everywhere, including the brain 2. The Brain consumes >20% of our resting energy expenditure & is fifth on the organ list in terms of highest concentration of this molecule 3. Creatine CNS depletion is a thing – and it happens in a wide variety of scenarios – from the seemingly benign (like chronic sleep deprivation) to the more sinister (neurodegeneration) 4. This then leads to higher Glutamate, Oxidative Stress & a spell of other sorts of ‘brain badness’ 5. Oral supplementation can cross the BBB and ‘refuel’ the brain and correct the Creatine deficit
Out of the thousand or so pages of research on this topic, I’ve just indulged in, there are several great reviews to pick from…it’s a tough call to make but perhaps this older one by Patricia Allen remains my favourite. This marks the beginning of a new era…I’m putting the trauma behind me & moving on & hope you’ll come along too!
When we recap the contemporary science of shared pathophysiology in mental health, we have: oxidative stress, impaired neurogenesis, monoamine deficits, glutamate excess, hypometabolism & mitochondrial dysfunction. When we ask researchers which of these supplemental Creatine might be able to assist with, we get hits at each and every point. Turns out, Creatine’s capacity for enhancing performance is not limited to athletes but can be capitalised on for anyone vulnerable to a CNS shortfall. Ignored for far too long, this economic and impactful brain nutrient is coming to the fore for psychiatric and neurological disorders.
The latest Update in Under 30 has landed!!!
You can purchase Creatine – The Brain Builder Part 1here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
Did I mention my mentees ask the meanest (!) & most meaningful questions? Especially those early career practitioners engaged in our New Grads program! And it’s been almost a whole month minute since I’ve talked about iron, so I wanted to share this gem from Katherine Geary:
“Why are so many women seriously low in iron? Periods aren’t a modern invention and it seems a bit of a design fault to have half the population dragging themselves around with iron deficiency anaemia! So why is it so common, even in women who seem to have reasonable dietary intake and low/average menstrual blood loss?”
Well I am so glad you asked! And not because I or anyone has the definitive answer. But there are some excellent voices joining in this conversation about how iron nutriture has seemingly become the collective female Achilles and how, in fact, this might be, as opposed to a ‘design fault’…wait for it…an evolutionary advantage! Particularly hard to believe I bet for those of us ‘dragging ourselves around with iron deficiency anaemia’…to contemplate that this makes you, in fact, some kind of Superhero! But let’s back up there a bit. Firstly, in light of iron being the 4th most common element on earth and concurrently the number one micronutrient globally we struggle to stay replete in…the contradiction is striking. Add to this the fact that while women and children of developing countries experience higher rates of deficiency & IDA, those of us living the ‘good life’ in the top pastures of the developed ones, are still affected at strikingly high rates. Katherine’s right of course, periods are not new…so have the rates of iron deficiency always been so high, or if not, what’s changed?Well, a few things.
As so often seems to be the case 🙄 most of the finger-pointing is at the problem child period: the Agricultural Revolution. This radical shift in diet, away from meat towards cereals, is a clear contributor.
And then came the infections. Both the GIT ones, with bacteria (not naming any names, H.pylori!) parasites & helminths etc getting cosy and cohabiting inside no-longer nomadic humans (stealing even more of our precious iron) and then following on as well, the rise of infectious illnesses, flu, smallpox, malaria, TB, etc. [Ok this is the bit where you can don your cape!] If you have one of the latter, then having one of the former can be really handy! Let’s say this another way. Iron deficiency is considered protective against the infections that can kill.
That’s why we see that characteristic sequestering of iron during any significant inflammation in our patients – ferritin rises because in fact as much iron as possible has been removed from the blood…because our infectious foes are fans of ferrous (not Ferris..😳)
Authors like Denic and colleagues contend therefore that “humans may have ‘failed to adapt’, genetically and culturally, to continuous deficiency of iron because relative iron deficiency was protective against many infectious diseases”. So next time you find yourself cursing the ‘dragging feet deficiency’, perhaps rather than our Stone-Age genes we can blame the blinkin’ Agrarian ones! It’s food for thought. Add to that, other major changes in the lives of women over time, like more time menstruating, both with a tendency to earlier menarche and significantly less cumulative time pregnant over our lifetime but I am sure there are many other theories out there. Have you got one?
Love Getting Answers to the Iron Questions That Bug Us All? Us Too!
Hence, The Iron Package
That’s why we’re often adding new tools and resources to our Iron Package for that very reason! Already, this package provides you with an opportunity to take a significant step up with regard to identifying, lows, highs and everything in between of iron status, and how best to manage deficiencies..our number one bug bear (as per above)! So if you’re not already a proud (iron) package practitioner, maybe there’s no time like….now?
I love a good iron question. It makes me emit a sound like Jack Sparrow might, when faced with something pleasingly piratey 🏴☠️ Lucky because I am asked SO MANY GOOD ONES, SO OFTEN!! Being one of the earliest minerals discovered to be essential…we know so much more about it than the other latecomers but that ABSOLUTELY DOES NOT MEAN WE KNOW IT ALL! Sorry…I also tend to shout with excitement when faced with a good iron question. Yes, run for cover, I do have an even higher volume setting 🙉🙉
Just this month, I received this little ripper: I was wondering about the expected timeframe for iron supplementation to improve ferritin levels?
Yes of all the nutritional answers we can quickly ‘google scholar‘ our way towards, actual realistic expectations for response to treatment, is rarely an easy find! And yet, this critical clinical detail seems to be the thing that can leave so many of us stranded at sea with our patient prescriptions. Did I give up too soon? Or should it have worked already by now? Some of the best naturopathic approaches are easy to execute…but when those patients come back after maybe a few repeats & perhaps minimal change you realise, you have a major piece of information MIA: what to expect. Rapid relief or a cure by Christmas?! Aka, it won’t happen overnight but it will happen. So, great, let’s talk ironing out our expectations around responses to iron repletion!!!
First – We need know where iron goes First!
So if your iron deficient individual is actually suffering from iron deficiency anaemia, no guesses who the VIP (very important priority) is during repletion! Consequently, you can throw lots of iron at somebody (oral or even IV) and find there’s limited increase in their ferritin initially, a rather ‘disappointing’ show actually but if you keep your other eye (Jack Sparrow style) on their FBE, you’ll see the iron is being funnelled into producing haemoglobin and red blood cells. Sneaky! And if sensible can ever be associated with sexy…this is it! Ferritin is for iron surpluses only and right now, we ain’t got none! Medical texts advise that in these scenarios, confirmation of efficacy equals an increase in Hb levels of approx 10g/L a week. In reality, no one wants to turn patients into pin cushions (esp when we’re trying to build iron back up not keep springing leaks!) so we might retest in a month or more. But an increase in Haemoglobin of 40g/L per month sounds rather aspirational with oral iron, doesn’t it!!
If we bring in the personalised perspective here, we recognise that most of our anaemic patients may only be just on the wrong side of the line, with values at 110g/L and tbh we would be shocked and a little worried if this grew in a month to 150 in a woman! Erythropoiesis is not the result of iron alone! But the point is, if the iron replacement is working well enough, you should be moving out of anaemia within a month not a millennium!
And only once this job is done will the ferritin start to build.
So what if your patient isn’t anaemic – just low in ferritin? Well then, if you’ve a) fixed the leaks (unintended or excessive blood loss anywhere Rectal, Renal, Repro) and b) buoyed bioavailability (HCl & prebiotics while minimising iron-blocking issues like excess Ca, tannins etc) and c) corrected for low intake via a sound supplemental approach (daily dosing for those not consuming much dietary iron and alternate days for the rest) you should be seeing ferritin increase within the month of at least 10mcg/L, but hopefully more. And if it’s not? Go back to the beginning of this little to-do list…because it means we’ve missed something. Doh!
Yes it’s true the learning doesn’t ever end and as I’ve continued to learn about new iron research I’ve added to our one-stop-iron-resource-shop..the Iron Package. Earlier this year we added a new clinical cheat sheet with some other important numbers on there you want to have at your fingertips whenever you read iron studies. So if you’ve already purchased and have access to the Iron Package…SURPRISE! 🤩 Go back and look again and if the iron package is not already on your ‘bookshelf’ there’s no time to waste!
You’ll never look at iron studies or your iron-challenged patients the same way.
Now find a comfy spot everyone & I’ll tell you a story…’Once upon a time, a long long time ago, we lived our days out in the dark, regarding potential calcium dysregulation!’But ever since serum Calcium has become a standard lab included in most routine screening tests (General Chemistry aka ELFTs) abnormal calcium handling is no longer an ambush for patients of ‘stones, moans and abdominal groans’, as the saying goes in hyperaparthyroidism. A diagnosis historically only mad, when someone presented with this constellation of rather advanced symptoms. But actually being able to identify your patients’ typical blood calcium levels offer us so much more than just a heads-up re parathyroid disease
It may tell us something about their Magnesium status, cardio cautions, be a bit of ‘bone barometer’ and probably most immediately important, flag their suitability for calcium supplementation!
Yep…rather than the current-criminally-crude-calcium-checklist: 1. Patient is female 2. Patient probably doesn’t consume enough calcium 3. Patient may be at risk of osteoporosis (yup…that accounts for practically every woman, right there!)
But seriously, if you just do a full review of the vast literature on this topic, what?! Not enough time?! How about then, just skim read a couple of key papers? Still baulking at that?…maybe just a wafer-thing editorial (??!) will tell you that, consuming elemental amounts of calcium (> 250mg), that are beyond even the biggest Dairy Diva’s Diet Diary, may be deeply problematic for many. And guess what…this doesn’t pertain to supplements alone…even calcium fortified foods are not free from concern! But let’s not let yet throw all our calcium fortified foods in the same bin as the folate ones we did a while ago!! Let’s step out of the dark and into the light that shines upon us, care of fasting serum Calcium measurements, to help us recognise whether Calcium is the cause, the consequence, a cure or a curse for person sitting in front of you 🧐
The Calcium ConspiracyControversy Continued
The Calcium Conspiracy arises primarily from misperceptions about it being ‘the boss of bones’ but becomes more of a controversy when in spite of ongoing advice for broad-scale use we review the evidence and have to acknowledge that the recommendation to supplement post-menopausal women with large doses of Calcium, not only lacks strong evidence but may cause harm to some. In this detailed discussion of the two schools of thought – Rachel finds a position somewhere in between. Reinforcing the need for an individualised approach and personalised risk benefit analysis while teaching you how to undertake this in every client.
The latest Update in Under 30 has landed!!!
You can purchase The Calcium Conspiracy Continued here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
You can become an Update in Under 30 Subscriber to access this episode and the entire library of Update in Under 30 audio’s and resources here.
Trends in mineral supplements are like music genres, you can pick which ‘decade’ they were formulated very quickly. But instead of going by clothes, hairstyles or even the style of accompanying music video, it’s all about the form – the ‘thing’ the mineral is bound to, that gives the game away. While mineral carbonates , sulphates and oxides seem to many of us contemporary clinicians, pre even MTV, amino acid chelates take me back to a time when I was wearing shoulder pads in everything, even my pyjamas. It was called power-dressing and needed to be adhered to 24/7, you see. Then along came fancy forms like orotates, aspartates, hydroxyapatites as we moved confidently into the 90s…well, as confidently as you can, when the Y2K bug may ‘end life as we know it’ come NYE. The dawn of the new millennium saw us embracing picolinates and bis-glycinates in a big way and for the last little while, citrates have really been having their time in the sun. But you know what…here’s a few things you MUST know…
These are trends, not truths
Every mineral has its Mrs Rights and Mrs Wrongs, in terms of chelates and ligands, and these are not the same from one mineral to the next e.g. Zn sulphate is a decent form of available Zn, Mg sulphate, an over-priced laxative
In almost every case, there is simply NO strong consistent body of evidence that one form of a mineral is superior in terms of bioavailability, regardless of what companies tell you..go on I dare you…check their references and then do your own quick literature search away from the cherry picker
Nor is there one mineral form that is above adverse effects in everyone
Brutal. Welcome back to ‘tough talkin’ Tuesday’ 😉 But we have to state these facts because we need effective supplements for our patients and not understanding the different forms that are better (but not ‘best’) compared with those that are inferior (this we do have some evidence of) threatens the integrity and efficacy of an otherwise well thought out prescription. So here’s where you might want to move into a room away from everyone and lock the door…because you’re likely to scream. One of, if not the most commonly used single nutrient supplement almost across the world, is calcium. After almost 30 years of studying supplemental forms side by side, can we conclude which form is best? No. How about ‘better’….hmmmmm yes…maybe…citrates look good going by some markers but not all and vice versa for other commonly seen forms. I can say this, because I have followed the research over the decades, reading the primary papers, like this excellent one by Bristow et al from 2015 that should burst quite a few people’s ‘best!’ bubbles. Have you screamed yet?
I scream. Often.
Because I am frustrated by the lack of research that we need, to be more certain of our preferred forms and then even more frustrated by companies’ claims that the evidence is already in, and guess what, theirs wins!
But it comes back to the same call to action for us – know your nutrients and specifically, where possible, get familiar with the Mrs Right and Wrong for each mineral! Know that the supplemental forms that work for zinc will not necessarily be a good match with iron, that any company that formulates their minerals in the vain of ‘one form for all’, be that glycinates, citrates, picolinates…well they’ve probably got a good fit for some of those minerals and a shocker for others. And as always truly check efficacy with follow up bloods, if you had baseline deficiencies evident in lab tests. I know, that’s not everyone’s model of practice right, or ideal but not always ‘real’, so alternatively, if you are prescribing based on clinical signs of mineral deficiencies that should respond quickly to repletion e.g. white spots on nails in the case of Zn deficiency, then ensure that they do!! If they don’t and your patient is compliant then consider switching form! When I see good practitioners’ prescriptions let down by poor choices of nutrient forms, well, that’s when I need to go into that separate room once more….can you hear me? Ooh that reminds me of something else dated by Mike and the Mechanics: Silent running “Can you hear me?!”😂
Let’s make sense of the over-arching nutrition principles, that will profoundly change your understanding and application of this modality Truly understanding the ‘big’ concepts, so often overlooked, or incorrectly taught, ensures you get the critical ‘small’ detail in your nutritional prescriptions right. In this 4 hour recording, together with key clinical tools, we talk about the tough stuff: dose-response curves, active versus passive stores and excretory pathways and ooh lah lah…the myth of taking ‘activated vitamins’. And yes we even mention Mrs Right/Wrong forms for minerals. Even those who feel satisfied with their original training – will find a lot in this critical review that is new, insightful and truly practise-changing!
I don’t know about you but I don’t count myself among the conspiracy theorists. While I may have been partial to the occasional one over my lifetime, you have my word, I never inhaled. Or at least not since I learned the practise of scientific enquiry and the application of critical thinking to all evidence. The two together tend to put a dampener on the whole: earth is flat & the moon-landing was a hoax…kind of notions. But there is one conspiracy I think all of us in nutritional medicine have been the victim of: The Calcium Conspiracy.
Not in the vein of speculations regarding excessive lobbying & undue influence of the Dairy Corporation on dietary guidelines. Nor even arguments that this has gone so far as to inflate the RDIs for this nutrient. Nope, I am actually good with the RDIs for this mineral. High level evidence confirms that our intake of Calcium was enormous even before the Agricultural Revolution, and therefore BD (Before Dairy) 😂
Man, those roots and tubers and other bushfoods sure were nutrient dense, not like the stuff we consume these days!
No, the Calcium Conspiracy we’ve all been lead to believe is that it is the boss. The boss of bones. The boss of the parathyroid. The boss of the other minerals. And especially the boss of Magnesium. While you might have heard me describe Calcium as a ‘bully’ in the GIT (let’s call this the slide 😅) and I stand by that, it is far from being the boss of the rest of the playground! In fact its regulation is largely at the hands of other nutrients..not naming any names…[Magnesium😳] So while, all of us trained in nutrition have had the significance of the Calcium-Magnesium relationship & the mantra “2:1, 2:1, 2:1” drilled into us, which we repeat at night to get ourselves to sleep (or did they mean to take not just ‘talk’ these minerals, to help with sleep?!) Our teaching created this conspiracy – a misperception that Calcium is the boss and Magnesium its long-forgotten lackey. Well guess who’s really calling the shots and on whom?!
Have you ever heard the saying, ‘It can take Magnesium to fix a Calcium problem”? I’ve not just heard it but seen it many, many times in my patients.
But how do you tell which patients need both and which ones, just one? It comes down to understanding the exquisitely sophisticated way Magnesium lords it over Calcium – via the parathyroid and Vitamin D metabolism and how we can see this patently in the pathology (regular screening labs) of your clients. I think there is a bias in integrative nutrition – we favour Magnesium – it goes into our supplement recommendations for so many of our patients and while the rationale for this is valid – all dietary surveys show magnesium under-consumption to be rampant in the SAD – I don’t actually think all of us know 1) how much we should be giving (yes there is a limit) 2) how to discern who needs what, in spite of a lack of a good Magnesium assay and 3) the true potency in the prescription when we get these things right or wrong! This study by Sahota et al is so far my favourite for 2020..it’s 14 years old and the sample size is small but its methodology and examination of when Magnesium can fix a Calcium issue and when it can’t, is superb. Together with about 50 other papers I’ve just imbibed…they’ve refined my thinking, tremendously. There’s a Calcium Conspiracy, alright, but just throwing Magnesium at everyone in arbitrary doses is not the solution…. “2:1, 2:1, 2:1…..”😴
There’s a conspiracy going on regarding Calcium but it’s probably not the one you imagine. We have been lead to believe that Calcium is the boss: the boss of the bones, of the other minerals and certainly of its often over-looked lackey, Magnesium. But the truth is, we have it all the wrong way round. There is a sophisticated synergism between these two minerals but the brains and the brawn in this relationship are held by the latter and we need to understand how to recognise when Magnesium is ‘pulling the strings’, to produce low calcium, in our patients and how to find the sweet spot of their synergy. This recording comes with a great resource to use in your clinic, with explicit redefinition of ‘what healthy looks like’.
Have you been told somewhere by someone that the ‘perfect’ TSH is 1.5 mIU/L? This is a wonderful, terrible & wonderfully terrible example of ‘magical numbers medicine’. As a push-back against the published reference ranges we’re given, that are so wide you could drive a truck through them, there has been an over-correction by some, leading to the myth of ‘magic numbers’. We can narrow the reference range substantially for many parameters with good rationale, make no mistake about that but once we start setting ‘aspirational goals’ that are explicitly rigid…well we’ve done 2 things 1) forgotten about the patient to whom this result belongs and 2) disregarded viewing each result as part of a ‘pattern’, that we must piece together and make sense of.
Back to TSH then… if my obese patient had a value of 1.5 mIU/L this in fact would be woefully inadequate.
Also too low for any patient, no matter their size, if their T4 is low and we’d like a higher value as well for risk minimisation in our elderly clients too.
But the same result would be excessively & worringly high in my patient who’s undergone thyroidectomy.
Being given a list of ‘magic numbers’ will never replace learning labs correctly. When we do this, we come to truly know that meaning can only be made of the markers when you can answer the following questions:
What is this (metabolite, analyte, binding agent, plasma protein etc)?
What do I know about its physiological and biochemical context – what is its role and regulation in the blood, what moves it and to what magnitude?
How have the reference ranges been determined for this lab – who am I comparing my patient to?
Therefore, what is the significance of a result that is: ‘normal’, ‘low normal’, ‘high normal’, below or above the range?
Does this value ‘fit’ with my patient?
What else could explain an unexpected result?
How strong is my level of evidence?
What do I need to do from here to confirm or refute this?
And a few more 😉
Realising the full value of any test result in terms of what it reveals about the person sitting in front of you, requires these skills. Unfortunately, in contrast a list of magic numbers will often lead you astray. And building your scientific knowledge about labs will not only help you avoid the pitfalls of pathology but will strengthen your pathophysiology prowess in surprising ways, saving your patients a packet in terms of additional extraneous testing and help you truly personalise your prescriptions…because the ‘invisible (biochemical individuality, oxidative stress, genetic probabilities, subclinical states, imbalanced or burdened processes etc) just became visible’. I started requesting lab results early in my career and years later was lucky enough to be taken under the wing of Dr. Tini Gruner. I found some of our shared notes, from 10 years ago, scribbled all over patient results recently and I was struck by just how lucky I was to have her encouragement to really pursue my interest and how she was a guiding force about learning to recognise pathology patterns over single parameters. A decade on I can confess, much of clinical and educative success has come off the back of this foundational skill-set and I know, this is true for so many I’ve taught too.
“The guidance I’ve received over the years from Rachel in relation to pathology interpretation has been one of the most valuable (and fascinating) investments I’ve made as a clinician. Her teachings have filled gaps in my knowledge base I never knew needed filling and have significantly enhanced my understanding of the inner workings of the body! Rachel has an incredible ability to make the numbers that patient’s so often present us with, both understandable and clinically meaningful. The knowledge I’ve gained by investing in this skillset has paid off in dividends and I’m certain will continue to do so into the future.”
Stacey Curcio – Cultivating Wellness
I hope you’ll join me for the most exciting up-skilling opportunity in learning labs yet. Oh…and all this talk about thyroid testing..that’s just a serving suggestion 😉 this year my MasterCourse is focused on the most routine labs of all: ELFTs, FBE, WCC, Lipid and Glucose Panels…an absolute treasure trove of free integrative health information about your patient!
This skillset has been found by many to be biggest ‘game-changer’ in Integrative Medicine!
There are limited places. To sign up for the MasterCourse: Comprehensive Diagnostics click here. For more information about the program click here.
Listen to me, I’m sounding all sporty 😂. I’m not though, just in case you suffer misguided visions of my virtues! But it’s not just the self-declared serious athletes that we need to have on our radar in relation to optimising their oxygen carrying capacity (aka window to winning). Our clinics are full of people, regularly running, doing triathlons for fun (!), riding vast distances clad in Lycra to drink coffee in other town’s cafes etc. etc. whose FBE might be feeling the pinch! That’s right! All these individuals, depending on the frequency and intensity of their exercise, could have the so-called, anaemia of an athlete.
Long gone is the idea that exercise-induced changes to your haemoglobin and red blood cells and perhaps even your iron, would only affect the ultra-marathon runners among us. It’s the swimmers, the cyclists, the Roller Derbyists, the CrossFitters, the basketballers, the Gym Junkies, the lawn bowlers..ok I may have gone too far now…they all are at increased risk.
Why? Isn’t exercise good for you? You know I so want to say, ‘Surprise! It’s not!’ but alas. Of course it is good for us BUT there are some fascinating challenges regular exercise can throw at your dear old blood and its bestie, iron. These challenges are incredibly dynamic – having one effect during exercise, a different one immediately following, and yet another in the days of rest in between. And sometimes, in fact, often, our patients can end up on the wrong side of these seismic shifts. Here’s how the story usually goes
“Oh yeah..I’ve had anaemia for ages! You know and it doesn’t matter how much Iron I take or how I take it – it never budges. But I’ve been told to stay on the Ferrograd anyway”
Typically, being told it’s ‘Athlete’s Anaemia’ is the first, in a series, of many many errors to follow. Because in fact, there is no such thing. That’s right. Anaemia is a symptom not a disease and exercise induced anaemia comes in 4 common flavours: Dilutional, Heamolytic, Iron Deficient & Acute Anaemia of Exercise, and knowing the difference is critical to correct management. Only 1 of them will reliably improve with iron and it needs to be prescribed in a totally novel way. Others will get worse with more iron. Yep. And one is a complete illusion. So when we don’t make the right diagnosis, which of the 4 types your patient actually has, we fail to find the fix. And while all of our patients may not be overly obsessed with improving their performance or even winning, let’s face it, they all want to achieve their PB, that’s why they came to see you. So can you tell the difference?
WARNING: I got so enthused about this topic that I went over. The current ‘Update in Under 30’ is a ‘serving suggestion’ only! And you may need to speed up your playback to squeeze in another bonus 10 min, if you can only afford your usual 30 min car trip to listen!
Outrunning ‘Athlete’s’ Anaemia
Persistent ‘hard-to-resolve’ anaemia is a common presentation for anyone participating routinely in sport and that can be at any level, not just among the professionals. From our lovely ladies who take up running or CrossFit in their middle-age, to our MIL (men in Lycra) and ‘weekend warriors’, they may love it but their haemoglobin and their iron doesn’t! Anaemia equals reduced oxygen carrying capacity, a concern for anyone interested in optimising their performance but equally relevant to patients just trying to manage their energy throughout the day. In this important episode we identify 4 different types of anaemia seen in patients as a result of exercise, incorrectly lumped together as ‘Athlete’s Anaemia’. Each type is easy to recognise once you know how and effective treatment of each is remarkably different. This summary and the super handy clinical resource that accompanies it will help you and your patients absolutely outrun it, at last.
For all Update in Under 30 Subscribers, you will find it waiting for you in your online account and don’t forget the **EXTRA BONUS LIVE CALL WITH RACHEL.
**This live Zoom call with Rachel is for current Update in Under 30 Subscribers ONLY. A Q&A session for subscribers on the UU30 episodes released in 2020. Contact the RAN Team to reserve your spot!
Sometimes I think I must be psychic..or is that psychotic? Don’t answer that, it’s a bad Byron Bay in-joke. I had literally just recorded my Update in Under 30 Copper in Kids and this excellent new study was published that same week, assessing and comparing trace minerals in age-matched ADHD and neurotypical kids. Snap! ✨ First, a moment of panic…because believe it or not, there are very few rigorous studies that have looked into this and so I had already read them all cover to cover and could confidently say, I had a grip on the literature. Gasp…’ will it have a different finding and challenge the much broader story about the excessive demonising of this mineral in kids health?’ Everyone take a big breath out…no.
But if you’re someone who thinks you’re seeing Copper toxicity in kids, you can keep taking a big breath in and while you’re at it a huge bit of new information:
Copper Excess is Normal in Children.
Every investigation of blood Copper levels in kids has reached the same conclusion and this latest one by a Russian group of researchers renowned for their work in Copper agrees. So the ideas that we have about optimal in terms of mineral balance for adults may stand, but can not and should not be applied to children. The elusive 1:1 relationship between Cu and Zn, for example, considered aspirational in optimising the mental health of big people, is absolutely not desirable or even healthy, in little ones. Why is it so? I hear you ask (…because you loved those old Cadbury chocolate ads with the crazy Professor as much as I did) Well, essentially because kids need more Copper than us, as a simple result of their increased growth requirements: blood vessels, bones, brains…Cu is a critical player in them all and more. And while we (and when I say ‘we’ I mean ‘I’) may be passionately passionate about Zinc’s importance, turns out, in paediatrics, it really does play second fiddle to Cu and should.
This new contribution to the Cu & Zn in ADHD kids debate did find that compared with neurotypical kids, their Cu:Zn was higher BUT – **and this is the really important bit **- as has been shown in a similar cohort before, the shift in relationship between the two was due in fact to lower Zinc levels NOT higher Copper.
So, I guess when you think about it…Zinc perhaps really does still deserve all our loving attention we give it 😂…we just need to rethink the whole negative attention we tend to mistakenly give Copper!
Copper, as a kingpin in angiogenesis, brain & bone building & iron regulation is a critical mineral during paediatric development. So much so, the kind of blood levels we see in a primary schooler might cause alarm if we saw them in an adult. So too their Zn:Cu. But higher blood Copper and more Copper than Zinc are not just healthy but perhaps necessary during certain paediatric periods. This recording redefines normal, low and high with a great clinical desktop tool to help you better interpret these labs, as well as reviewing the top causes and consequences of both types of Copper imbalance in kids.
The latest Update in Under 30 has landed. You can purchase January’s episode, Copper in Kids here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
-Your RAN Online Account has a NEW LOOK!!-
Next time your log in, you will experience a more user friendly way to search, view, listen and download your resources. Find out what’s new here.
Copper deficiency happens in kids, so does copper toxicity and both are serious concerns, but do we know when to accurately call either? First, we have to know ‘normal’. If we know what normal Serum Copper values look like in children, then we can easily spot those falling below or above this, right? That’s the first hurdle we tend to knock over and break a toe on! Being a mineral whose levels vary widely in soil from country to country, globally, the differences in reference ranges are breathtaking & absurd. Add to that, that copper is a key mineral in kids, driving huge demand for it during key periods of development, so the range for pre-schoolers isn’t the same as the primary or high schoolers – not that your lab is flagging that. Unhelpful? Yes. Dangerous, even? Potentially.
To diagnose ‘Copper Excess’ in a child is a big call to make.
One, because most practitioners are unaware just how much Copper a child really needs at each age & two, high copper is often a messenger for something else going on and then three, the primary objective based on this diagnosis becomes to lower their Copper but we could be either shooting the messenger or missing the mark all together…right?
Copper excess does happen but not nearly as often as practitioners believe it does. And in kids, the fall-out from such misdiagnosis is bigger. And missing a Copper deficiency? (because we’re not as well-trained to recognise it and because Copper has been sadly demonised) Likely to have myriad negative impacts at this vulnerable age…almost none of which generate symptoms or a distinct clinical picture e.g. secondary iron deficiency, low neutrophils without necessarily compromised immunity. But what about the holy grail get-out of jail adjective: ‘relative’. You know, ‘this is at least a Copper excess relative to their Zinc?’
Well, to form this opinion you’re likely calculating the Zn:Cu ratio and applying an ideal adult value of 1:1 but show me the primary evidence that supports this for kids…anywhere? The Zn & Cu relationship shifts as we move through life-stages and in fact Copper is supposed to dominate through a lot of our childhood so…ummmmm…no.
HTMA Copper side-steps all of this?..double no.
I used to make the same mistake re Zn:Cu, I may have even taught you this?!🤦♀️ But as so often happens, a week spent in all the original scientific data and I’ve emerged a changed practitioner! Having been part of perpetuating this problematic premise in the past, I am determined to get the correct message out there to as many practitioners as possible. So help me spread the word on Copper in Kids – by telling others that this mineral is so critical to kids compared with adults, they will often have higher levels than ‘us’ and that until you’ve applied the right age-appropriate reference range and ruled out confounders you can’t possibly make a call on Copper. I mean, we kind of knew this all along, with healthy pregnancy Copper values being exponentially higher being a giant clue. Turns out kids’ ‘Copper Age’ extends way beyond the womb.
Copper, as a kingpin in angiogenesis, brain & bone building & iron regulation is a critical mineral during paediatric development. So much so, the kind of blood levels we see in a primary schooler might cause alarm if we saw them in an adult. So too their Zn:Cu. But higher blood Copper and more Copper than Zinc are not just healthy but perhaps necessary during certain paediatric periods. This recording redefines normal, low and high with a great clinical desktop tool to help you better interpret these labs, as well as reviewing the top causes and consequences of both types of Copper imbalance in kids.
The latest Update in Under 30 has landed. You can purchase January’s episode, Copper in Kids here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
-Your RAN Online Account has a NEW LOOK!!-
Next time your log in, you will experience a more user friendly way to search, view, listen and download your resources. Find out what’s new here.
It’s like that split-second you close the door and realise you’ve locked the car with the keys still inside, or the whole reason you rang someone pops back into your head just after you put the phone down. Yes after the opportunity to draw breath over the break I went, ‘Doh! …I forgot to mention manganese!!’ So some of you may already know I am not a super fan of manganese. Well actually, that’s not accurate, I am perhaps just less of a fan than the people who are formulating a lot of our supplements! A place for everything and everything in its place. While this saying is completely foreign to my office, my house, my domestics and the rest of my life, it is a mantra I abide by with all micronutrients. Having enough of each micronutrient is good, having optimal (if we know what that is, which often we don’t) is wonderful but an excess is bad news.
And as I’ve spoken to before, with our increasing use of multi-nutritional formulas and the frequent inclusion of significant amounts Mn somewhere towards the bottom of those long ingredient lists…we very much run this risk with patients who are taking multiple supplements, at which point Manganese can become a serious meddler.
There’s a short list of patients for whom I am particularly conservative regarding their Manganese exposure and near the top of that list is those with Gilbert’s Syndrome. Do you get my ‘Doh!’ moment now? Because at the end of last year I released the Gilbert’s Syndrome: New Goals & Good News Update in Under 30…only to realise after ‘I’d put the phone down’ that I’d left this important one out of the dos and don’ts of managing these patients. So why am I saying no to chronic routine use of Manganese in those with GS? Well here’s the deal…
That’s why we need to be clear to cap the Mn for these patients as part of being across the cumulative subtotals of all micronutrients. While there is no established Upper Tolerable Limit (UL) set for Mn, adequate intake has been determined as 5mg/d for an adult. I agree, this is probably inadequate for some but I’ve seem individual patient prescriptions with cumulative Mn totals over 20 and 30mg per day! In spite of being generally regarded as having a low acute toxicity profile there is increasing research documenting Mn as a meddler when it comes to thyroid function in particular. So who else is on my watch and wait list for Mn excess? You’ve probably got some ideas…
The latest Update in Under 30 has landed: Gilbert’s – New Goals and Good News and my team has gone all out in producing a brilliant desktop reference to go with this recording that aids better understanding and clear treatment aims for your GS patients.
You can purchase Gilbert’s: New Goals & Good News here.
If you are an Update in Under 30 Subscriber, you will find it waiting for you in your online account.
**But if you’re just joining us & this important conversation now,
ideally get the basics and backstory first and purchase all 3 key episodes in ‘A Guide to Gilbert’s Package’